Kaohsiung J Med Sci January 2010 • Vol 26 • No 1 21
Coronary artery disease (CAD) is a major cause of morbidity and mortality worldwide. Conventional invasive coronary angiography is currently the clini-cal gold standard for the detection of CAD. However,
the risk of potentially serious adverse complications and the associated cost have prompted intensive searches for noninvasive alternatives. Advances in multi-detector-computed tomography (MDCT) have improved imaging quality and simplified the im-plementation of contrast-enhanced MDCT in non-invasive cardiovascular imaging programs [1–5]. The improved imaging quality has increased the accuracy of MDCT imaging for the diagnosis of coronary artery stenosis when compared with conventional invasive coronary angiography. A recent meta-analysis [6]
Received: Aug 20, 2009 Accepted: Sep 9, 2009 Address correspondence and reprint requests to: Dr Jui-Sheng Hsu, Department of Medical Imaging, Kaohsiung Municipal Hsiao-Kang Hospital, 482 San-Ming Road, Hsiao-Kang District, 812 Kaohsiung City, Taiwan.
E-mail: [email protected]
Q
UANTITATIVE
A
SSESSMENT OF
I
MAGE
Q
UALITY IN
64-
SLICE
-
COMPUTED
T
OMOGRAPHY OF
C
ORONARY
A
RTERIES IN
S
UBJECTS
U
NDERGOING
S
CREENING
FOR
C
ORONARY
A
RTERY
D
ISEASE
Li-Hwa Yang,1Ding-Kwo Wu,1,2Chiao-Yun Chen,1,2Gin-Chung Liu,1,2Tsyh-Jyi Hsieh,1,2 Twei-Shiun Jaw,1,2Shu-Yuan Huang,1Chien-Chung Lin,1and Jui-Sheng Hsu3,4
1Department of Medical Imaging, Kaohsiung Medical University Hospital; 2Department of Radiology,
Faculty of Medicine, 3Graduate Institute of Medicine College of Medicine, and 4Department of Medical
Imaging, Kaohsiung Municipal Hsiao-Kang Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
Accurate and consistent visualization of the entire coronary system with high-grade imaging qual-ity is crucial for routine applications of multi-detector-computed tomography (MDCT) coronary angiography. To determine the imaging quality of 64-slice-MDCT coronary angiography, we respec-tively explored the quantitative parameters of imaging quality in 105 consecutive subjects (71 men, 34 women; aged 58.66± 10.62 years) who underwent 64-slice-MDCT coronary angiography to screen for coronary disease. The interobserver agreement for semi-quantitative image quality, visible length, signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) of the coronary arter-ies was good. The SNR and CNR of the proximal segments of the coronary arterarter-ies were superior to that of the distal segments of coronary arteries (p<0.001). The visible length of the stenosed right coronary artery was significantly shorter than that of the non-stenosed right coronary artery (p= 0.03). The SNR and CNR of the stenosed and non-stenosed coronary arteries revealed no sig-nificant difference (p> 0.05). Body weight and body mass index were inversely related to the SNR and CNR of the aorta (p< 0.001). In conclusion, 64-slice-MDCT coronary angiography can provide excellent imaging quality of coronary arteries in subjects undergoing screening for coronary disease, although the SNR and CNR were relatively low at the distal segments of coronary arteries.
Key Words:computed tomography, coronary artery (Kaohsiung J Med Sci 2010;26:21–9)
showed a clear increase in diagnostic accuracy as tech-nology improved from 4-slice-MDCT to 16-slice- and 64-slice-MDCT, with a pooled sensitivity of 95% and specificity of 93% for 64-slice-MDCT on a per-vessel basis. On a per-patient analysis, the pooled sensitivity for 64-slice-MDCT was 99% and the specificity was 93%. Nevertheless, 29% of the coronary arteries could not be evaluated because of insufficient imaging qual-ity with 4-slice-MDCT, 22–29% with 16-slice-MDCT, and 3–11% with 64-slice-MDCT [7–15]. High heart rate and greater body mass index (BMI) have been impli-cated as the major factors that degrade the imaging quality of MDCT coronary angiography [7,12,16–19]. Stenosis of coronary arteries might impede the enhancement of the post-stenosed coronary arteries. To our knowledge, the influence of stenosed coro-nary arteries on imaging quality of MDCT corocoro-nary angiography has not been reported. Accurate and consistent visualization of the entire coronary system with high-grade imaging quality is crucial for routine applications of MDCT coronary angiography. The purpose of our study was to quantitatively assess the imaging quality of coronary arteries in subjects undergoing 64-slice-MDCT coronary angiography to screen for CAD.
S
UBJECTS ANDM
ETHODSStudy population
This study was approved by our institutional human research committee. We retrospectively studied 105 consecutive patients (74 men and 34 women) referred for CAD screening between January 1 and October 31, 2007. Standard exclusion criteria for contrast-enhanced MDCT coronary angiography were applied, and included previous allergic reaction to iodinated contrast, atrial fibrillation or other arrhythmias, or renal disease with serum creatinine level > 1.5 mg/dL.
MDCT coronary protocol
All patients were assessed 60–90 minutes before their scheduled scan appointment to determine if they were clinically and hemodynamically stable. Heart rate and blood pressure were recorded. If the heart rate exceeded 65 beats per minute with a sys-tolic blood pressure above 100 mmHg, and the pa-tient was without contraindications for β-blockers, an oral dose of 5 mg of bisoprolol (Concor, Merck,
Darmstadt, Germany) was administered to reduce the heart rate to improve image quality. In addition, in the absence of contraindications, patients received a sublingual dose of nitrate (0.6 mg of nitroglycerin; Nitrostat, Pfizer, USA) to dilate the coronary arteries.
MDCT scans were performed on a 64-slice-MDCT (Brilliance 64; Philips Medical Systems, Haifa, Israel). Patients were examined in the supine position, and all image acquisitions were performed during an inspiratory breath-hold. The breath-hold time was between 10–20 seconds, depending on the scanning volume. A bolus of 60–80 mL of Iohexol (Omnipaque 350; GE Healthcare, Cork, Ireland) was injected into an antecubital vein at a flow rate of 4–5 mL/s, fol-lowed by a 50-mL saline chasing bolus. The start delay was defined by bolus tracking in the ascending aorta and the scan was automatically started 10 sec-onds after reaching the threshold (150 Hounsfield units). Scanning was performed from the tracheal carina to the diaphragm using the following parame-ters: X-ray tube potential= 120 kV, effective tube cur-rent= 800 mAs, detector collimation = 64 × 0.625 mm, rotation time= 420 ms, and pitch = 0.2.
For image reconstruction, we processed the source images on a separate workstation (Brilliance 2.0; Philips Medical Systems). We used retrospective electrocardiographic gating for optimal heart phase selection. The images were reconstructed and syn-chronized to electrocardiography during the late dias-tole phase at 70–80% of the RR interval. Slices with a thickness of 1 mm (increment= 0.6mm) and a medium soft-tissue reconstruction kernel were used to evaluate the coronary arteries. Evaluation of vessel visibility was performed on each edited data set by two expe-rienced radiologists (Dr D.K. Wu and Dr C.Y. Chen) to select the best phase for further vessel segment analysis using a combination of axial, multi-planar reformation and maximum intensity projection views on an image post-processing workstation (Brilliance 2.0; Philips Medical Systems).
MDCT image analysis
Two experienced radiologists, acting independently, performed a semi-quantitative assessment of the overall image quality using a four-point scale, as reported previously [20], where 4= excellent, no arti-fact; 3= good, mild artifact; 2 = acceptable, moderate artifact present but images still interpretable; and
1= unmeasurable, severe artifact renders interpreta-tion not possible. For any disagreement in data analysis between the two observers, consensus agreement was achieved. Stenosis of the coronary artery was defined as at least one segment of the coronary artery with a ≥50% reduction in diameter based on cross-sectional image analysis [2].
The overall visible length of each coronary artery was determined by manually measuring the center-line length from the ostium to the most distal point at which the enhanced vessel lumen was still clearly visible in the curved multi-planar reformatted images by two independent, experienced observers (Dr L.H. Yang and Dr T.J. Hsieh). We measured the length of the left main coronary artery (LM), left anterior descend-ing coronary artery (LAD), left circumflex coronary artery (LCX) and right coronary artery (RCA). The length of the LCX was defined as the length of the entire LCX or the length of the proximal LCX and the first obtuse marginal branch, if this branch had a larger diameter [12].
To determine the signal-to-noise ratio (SNR) and the contrast-to-noise ratio (CNR), a region-of-interest (ROI) cursor (3–4 mm2) was placed within the contrast-enhanced lumen of the coronary artery and the con-nective tissue adjacent to the vessel, and the signal intensity (SI; i.e. CT attenuation) was recorded by the two experienced observers. The ROIs were posi-tioned by carefully avoiding calcifications, plaques, and vessel walls. The mean SI of both observations was calculated for further evaluation. We measured nine locations: LM, proximal LAD, distal LAD (distal portion), proximal first diagonal branch, proximal LCX, distal LCX (distal portion), first obtuse mar-ginal branch (proximal part), proximal RCA, and dis-tal RCA (disdis-tal portion of the posterior descending coronary artery). Image noise was defined as the standard deviation (SD) of SI in a ROI cursor (1 cm2)
placed in the aortic root at the level of the origin of the LM. SNR, CNR, SNR of the proximal–distal dif-ference and CNR of the proximal–distal difdif-ference were calculated using the following equations:
SNR= SIlumen/imaging noise;
CNR= (SIlumen– SIconnective tissue)/imaging noise;
SNR of the proximal–distal difference = (SNRproximal– SNRdistal);
CNR of the proximal–distal difference = (CNRproximal– CNRdistal);
where SIlumenis the mean SI of the coronary artery,
SIconnective tissueis the mean SI of the connective tissue
adjacent to the vessel, image noise is the SD of SI in the aortic root, SNRproximal is the SNR of the proximal
segment of coronary artery, SNRdistalis the SNR of the
distal segment of coronary artery, CNRproximalis the
CNR of the proximal segment of coronary artery, and CNRdistal is the CNR of the distal segment of
coro-nary artery.
Statistical analysis
All data are expressed as means± SD. The results are reported as the mean of the measurements by two observers. Wilcoxon signed-rank test and κ statistics were applied for interobserver agreement of semi-quantitatively imaging quality assessment. Pearson’s correlation coefficient and Student’s paired t test were used to determine the interobserver agreement for the visible length, SNR and CNR of the coronary arteries. Linear regression analysis was preformed to plot the effects of heart rate on semi-quantitative imaging quality. Differences among arteries (SNR and CNR) were examined using one-way analysis of variance. Differences between individual pairs were then analyzed using Bonferroni’s multiple compari-son test. Student’s t test was used to determine the difference between the stenosed and non-stenosed coronary arteries. Linear regression analysis was per-formed to explore the influence of heart rate, body weight, BMI and SNR of the aortic root on the CNR of the aortic root and coronary arteries.
R
ESULTSPatient characteristics
The mean age of the 105 subjects in the study was 58.66± 10.62 years (range, 30–85 years). The mean heart rate during the scan was 59± 8 beats/min. The mean body weight was 68.36± 10.76kg and mean BMI was 24.98±3.13kg/m2. Results showed stenosis at the
RCA in 26 subjects, LAD in 39 subjects and LCX in 16 subjects. Stenosis of the RCA (n= 5), LAD (n = 6) and LCX (n= 5) was confirmed by conventional coronary angiography in 11 subjects.
The semi-quantitative imaging quality for each coronary artery is summarized in Table 1. In 105 sub-jects, a total of 360 vessels were evaluated. The overall interobserver agreement for the semi-quantitative
imaging quality rating was good (κ = 0.67, p = 0.56). All coronary segments were of diagnostic imaging quality (score 2–4; Figure 1), with 551 segments (87.5%) were rated to have excellent imaging quality (score=4), 49 (8.8%) had mild artifacts (score= 3) and 30 (5.8%) had moderate artifacts (score= 2). No coronary seg-ments were rated as non-diagnostic coronary segseg-ments (score= 1).
The interobserver agreement for the visible length of the coronary arteries was good. The visible length (and correlation coefficients) of the coronary arteries was: LM, 10.2± 4.6 mm (r = 0.99, p = 0.77); LAD, 140.6± 26.2 mm (r = 0.96, p = 0.26); LCX, 94.3 ± 30.4 mm
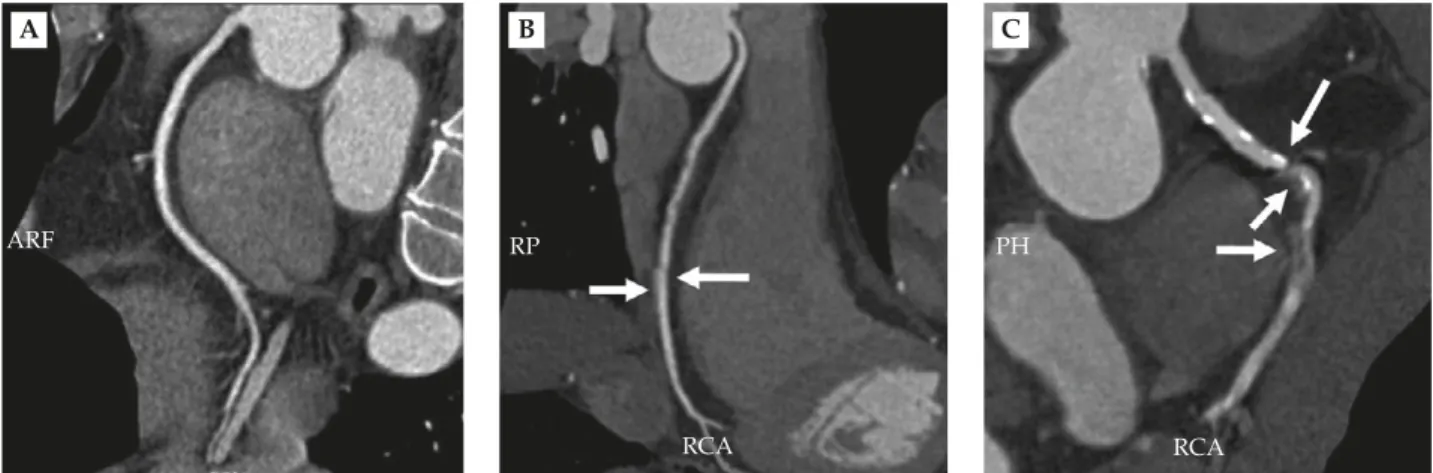
Figure 1.Curved multiplanar reformatted images of the right coronary arteries (A) for an excellent image with no artifacts; (B) a good image with mild motion artifacts and step artifacts (arrows); and (C) an acceptable image with moderate motion artifacts and step arti-facts (arrows). RCA= right coronary artery.
A B C
ARF RP PH
RCA RCA
Table 1.Semi-quantitative scores of image quality and interobserver agreement for the coronary arteries of 105 subjects*
Semi-quantitative imaging quality Variable Mean± SD κ coefficient p LM 3.99± 0.10 0.99 0.99 LAD 3.74± 0.56 0.59 0.58 D1 3.90± 0.37 0.79 0.58 LCX 3.80± 0.48 0.61 0.34 OM1 3.72± 0.63 0.92 0.99 RCA 3.75± 0.54 0.78 0.42 Total coronary 3.82± 0.49 0.67 0.56 arteries
*The interobserver agreement for semi-quantitative rating of image quality of coronary arteries was good. SD= standard deviation; LM= left main coronary artery; LAD = left anterior descending coronary artery; D1= first diagonal branch; LCX = left circumflex coronary artery; OM1= first obtuse marginal branch; RCA= right coronary artery.
(r= 0.99, p = 0.32); and RCA, 158.2 ± 34.7 mm (r = 0.78, p= 0.12). The visible length of the stenosed RCA was significantly shorter than that of the non-stenosed RCA (145.9± 31.1 vs. 162.2 ± 35.1 mm, p = 0.03). Assess-ment of the visible length of the coronary arteries revealed no significant difference between stenosed and non-stenosed groups of LAD (135.3± 24.0 mm vs. 143.7± 27.1 mm, p = 0.10) and LCX (104.8 ± 22.7 mm vs. 92.4± 31.4 mm, p = 0.07).
The interobserver agreement for SNR and CNR of each coronary artery showed excellent agreement (Table 2). No significant differences in SNR and CNR were observed among LM and the proximal segments of the RCA, LAD and LCX (SNR, p= 0.25; CNR, p= 0.44). The SNR of the distal segments of the RCA and LCX was superior to that of the distal segments of the LAD (p< 0.001). No significant difference was observed for the CNR among the distal segments of the RCA, LAD and LCX (p= 0.24). The SNR of the proximal segments of the coronary arteries was superior to that of the distal fragments of coronary arteries in the RCA, LAD and LCX (p< 0.001). The CNR of the proximal segments of the coronary arter-ies was higher than that of the distal fragments of the coronary arteries in the RCA, LAD and LCX (p<0.001). The SNR and CNR were significantly higher in the proximal LAD than in the proximal first diagonal branch of the LAD (p<0.001). The SNR and CNR of the proximal LCX were higher than those of the first obtuse marginal branch of LCX (p< 0.001).
The SNR and CNR of the stenosed and non-stenosed coronary arteries are summarized in Table 3. The SNR and CNR showed no significant difference
between the stenosed and non-stenosed groups for the proximal segments, distal segments and the proximal– distal difference of the coronary arteries (p> 0.05). The SNR and CNR of the proximal segments of coronary arteries were superior to that of the distal fragments of coronary arteries in both the stenosed and non-stenosed groups (p< 0.001).
The SNR of the aorta was proportional to the CNR of the aorta (p< 0.001; Figure 2). Body weight and BMI were inversely proportional to the SNR and CNR of the aorta (p< 0.001; Figure 2). The SNR and CNR of the aortic root did not significantly affect the visible length of the coronary arteries (p> 0.05). Heart rate
did not significantly affect semi-quantitative imaging quality, CNR or SNR of the coronary arteries (p> 0.05).
D
ISCUSSIONThe study was designed to semi-quantitatively assess the image quality of 64-slice-MDCT coronary angiog-raphy in subjects undergoing screening for CAD. We showed that 64-slice-MDCT coronary angiography provided excellent image quality for these subjects. As a result of the technical developments that have improved the spatial resolution through thinner slice Table 3.The signal-to-noise ratio and contrast-to-noise ratio of stenosed and non-stenosed coronary arteries*
Stenosed Non-stenosed p Variables n SNR CNR n SNR CNR SNR CNR RCA Proximal 26 13.9± 3.9 16.7± 3.5 79 14.7± 4.6 17.5± 4.9 0.35 0.34 Distal 26 4.4± 2.7 6.6± 2.7 79 4.4± 2.3 6.7± 2.1 0.96 0.88 Difference 26 9.5± 3.1 10.1± 3.0 79 10.3± 4.3 10.9± 4.6 0.31 0.34 LAD Proximal 39 13.6± 3.2 16.3± 3.2 66 14.7± 4.4 17.5± 4.7 0.15 0.14 Distal 39 2.6± 1.8 6.2± 1.5 66 3.2± 2.1 6.3± 1.7 0.12 0.62 Difference† 39 11.0± 3.2 10.2± 2.9 66 11.5± 4.3 11.2± 4.3 0.51 0.16 LCX Proximal 16 13.6± 2.9 16.5± 3.0 89 14.9± 4.2 18.0± 4.8 0.14 0.11 Distal 16 3.7± 2.3 6.0± 2.7 89 4.2± 2.4 6.2± 2.5 0.49 0.75 Difference† 16 9.9± 2.5 10.5± 2.6 89 10.8± 4.0 11.8± 4.4 0.26 0.13
*Data presented as n or mean± standard deviation; †proximal–distal difference of the coronary arteries. SNR= signal-to-noise ratio;
CNR= contrast-to-noise ratio; RCA = right coronary artery; LAD = left anterior descending coronary artery; LCX = left circumflex coronary artery.
Table 2.Mean signal-to-noise ratio, contrast-to-noise ratio and interobserver agreement in the coronary arteries of 105 subjects*
Signal-to-noise ratio Contrast-to-noise ratio Variable Mean± SD r p Mean± SD r p Aorta 15.44± 4.15 0.90 0.71 18.10± 4.36 0.93 0.3 LM 15.31± 4.04 0.92 0.11 17.93± 4.20 0.91 0.2 Proximal LAD 14.44± 3.94 0.93 0.38 17.21± 4.15 0.9 0.97 Distal LAD 2.97± 1.99 0.98 0.84 6.26± 1.63 0.93 0.13 Proximal D1 10.98± 3.90 0.97 0.14 14.16± 4.29 0.94 0.92 Proximal LCX 14.72± 4.06 0.98 0.27 17.74± 4.61 0.89 0.65 Distal LCX 4.14± 2.31 0.98 0.82 6.22± 2.41 0.89 0.3 Proximal OM1 11.45± 3.67 0.96 0.36 14.44± 4.10 0.93 0.77 Proximal RCA 14.53± 4.36 0.95 0.15 17.34± 4.62 0.88 0.81 Distal RCA 4.41± 2.36 0.99 0.52 6.67± 2.25 0.93 0.13
*The interobserver agreement for the signal-to-noise ratio and contrast-to-noise ratio of the coronary arteries was excellent. SD=standard deviation; r=Pearson’s correlation coefficient; LM=left main coronary artery; LAD=left anterior descending coronary artery; D1 = first diagonal branch; LCX= left circumflex coronary artery; OM1 = first obtuse marginal branch; RCA = right coronary artery.
collimation and increased the temporal resolution through faster gantry rotation, 64-slice-MDCT has become a robust technology for non-invasive coro-nary imaging [12]. Premedication with β-blockers for subjects with heart rate exceeding 65 beats/min, administration of nitroglycerin, and optimization of the contrast injection protocols further improved the image quality of 64-slice-MDCT coronary angiography.
The mean visible length of the coronary arteries was similar to the previously reported values deter-mined by 16-slice-MDCT and 64-slice-MDCT [12,21]. These results most likely reflect the fact that 64-slice-MDCT scanners provide only stable improvements in spatial resolution, as compared with the 16-slice-MDCT scanner [12]. However, our study showed that the visible length of the stenosed RCA was signifi-cantly shorter than that of the non-stenosed RCA. These findings suggest that stenosis of the coronary arteries might reduce the visible length of the post-stenosed coronary arteries.
The best criterion for objectively assessing image quality is the determination of SNR and CNR [22]. We found excellent SNR and CNR in most of the sub-jects studied. High SNR and CNR were maintained
throughout the coronary tree, although the SNR and CNR were lower at the distal segments of the nary arteries than at the proximal segments of coro-nary arteries. The ROI measurements of the proximal segment of coronary arteries plus a point at the distal segment provided initial insight into the gradient of contrast enhancement. Although the ROI measure-ments were difficult and potentially less accurate for small caliber arteries, the 64-slice-MDCT imaging envi-ronment yielded excellent interobserver agreement.
Our results indicate that the SNR and CNR of the proximal segments of the coronary arteries were supe-rior to those of the distal fragments of coronary arter-ies. Our results were different to those in the study by Ferencik et al [12], who showed no significant differ-ence in CNR between the proximal and distal segments of the RCA, although the CNR was significantly higher in the proximal segments of the LAD and LCX than in the distal fragments of the LAD and LCX [12]. In addition, we found no significant difference in the proximal–distal difference of the coronary arteries between the stenosed and non-stenosed coronary arteries. A potentially decreased SNR or CNR of the distal coronary segments might reduce the diagnostic Figure 2.Linear regression analysis of the correlation between (A) the signal-to-noise ratio and the contrast-to-noise ratio of the aorta, (B) body weight and contrast-to-noise ratio of the aorta, and (C) body mass index and contrast-to-noise ratio of the aorta. 0 10 20 30 40 SNR of aorta Contrast-to-noise ratio of aorta y = 2.79 + 0.99x R2 = 0.89 0 10 20 30 40 10 20 30 40
Body mass index
Contrast-to-noise ratio of aorta y = 38.20 – 0.81x R2 = 0.37 15 20 25 0 30 35 40 A C y = 32.23 – 0.21x R2 = 0.29 Body weight 40 50 60 70 80 90 100 0 10 20 30 40 Contrast-to-noise ratio of aorta B
performance of MDCT coronary angiography. Inade-quate contrast administration (e.g. inadeInade-quate volume, injection speed or timing), inadequate selection of the field of view or ROI placement for bolus tracking, or inadequate breath-holds can result in low SNR and low CNR, resulting in poorly visualized coronary arteries. Contrast media with higher iodine concen-trations provide substantially higher attenuation val-ues in the coronary arteries [23] although the added value of these higher iodine concentration media on diagnostic accuracy in assessing CAD has not yet been established. However, as described by Fleischmann et al [24], arterial enhancement is dependent on the iodine administration rate and injection duration. At a constant iodine load, the injection duration of more concentrated contrast agents is shorter. Although we followed the rule “injection duration equals scanning duration”, shorter injection time might reduce image quality because the enhancement is non-uniform over time, with the brightest enhancement occurring out of the imaging acquisition [24]. Faster coronary angiog-raphy acquisition using MDCT with 64 or more detec-tors will possibly benefit from higher concentrations of contrast agents [12].
It is well known that image noise correlates with biometric data such as body weight and BMI [16–18]. Greater body weight and BMI are associated with greater image noise, thus reducing SNR and CNR, and negatively affecting the quality of MDCT coronary angiography. Therefore, our results were in agreement with previous studies.
Heart rate is also a major predictor of MDCT coro-nary angiography image quality [7,12,19]. Patients with higher heart rates had significantly more motion artifacts. Our results revealed that the heart rate did not significantly influence the semi-quantitative assess-ment of imaging quality, or SNR or CNR of the coro-nary arteries. The systematic approach to heart rate control, as performed in this study, was probably one of the major contributors to improved image quality.
Our study has some limitations, which need to be addressed. First, the patient group only included a small number of cases with stenosis of the coronary artery. Second, our study was principally limited by its retrospective nature, which might have intro-duced selection bias. Third, we only included sub-jects undergoing screening, which might represent inclusion bias. Fourth, the semi-quantitative rating of image quality may have been biased by subjectivity;
however, the high κ coefficient indicated good inter-observer agreement and may argue against such a bias. Fifth, our study lacked direct comparison to previous generations of MDCT scanners in the same patient group. Thus the improved image quality could be partly attributed to different population variables (e.g. patient size and body weight, and heart rate). Sixth, we did not calculate the estimated radiation dose using the exposure parameters pro-vided by the CT scanner. In general, image noise is inversely proportional to the square root of the radia-tion dose. In other words, reducing the radiaradia-tion dose may increase image noise and decrease the SNR and CNR. Finally, the systematic approach to heart rate control, as performed in this study, might not be reasonable for routine CT coronary angiography. Faster coronary angiography acquisition using MDCT with 256 or more detectors will benefit from whole heart coverage and sub-second acquisition of the entire cardiac volume. Whole heart coverage might eliminate the “stair-step” artifacts inherent in 64-slice-MDCT, which images sub-volumes of the entire cardiac volume over multiple gantry rotations. Sub-second acquisition of the entire cardiac volume might enable imaging of the contrast bolus at a single time-point to reduce contrast opacification gradients of the coronary arteries.
In conclusion, we have demonstrated that body weight, BMI and the SNR of the aortic root might affect the image quality of 64-slice-MDCT coronary angiog-raphy. The 64-slice-MDCT coronary angiography can provide excellent imaging quality of coronary arter-ies in subjects undergoing screening for coronary dis-ease, although the SNR and CNR were relatively low in the distal segments of coronary arteries. In addition, no significant difference of imaging quality was found between the stenosed and non-stenosed coronary ar-teries, except that the visible length of the stenosed RCA was shorter than that of the non-stenosed RCA. Overall, 64-slice-MDCT coronary angiography could provide excellent image quality for non-invasive screening of CAD.
A
CKNOWLEDGMENTSWe are grateful to the Kaohsiung Medical University Hospital, Taiwan, for financial support (KMU-95-5N35).
R
EFERENCES1. Gershlick AH, de Belder M, Chambers J, et al. Role of non-invasive imaging in the management of coronary artery disease: an assessment of likely change over the next 10 years. A report from the British Cardiovascular Society Working Group. Heart 2007;93:423–31.
2. Hoe JW, Toh KH. A practical guide to reading CT coronary angiograms—how to avoid mistakes when assessing for coronary stenoses. Int J Cardiovasc Imaging 2007;23:617–33.
3. Limkakeng AT, Halpern E, Takakuwa KM. Sixty-four-slice multidetector computed tomography: the future of ED cardiac care. Am J Emerg Med 2007;25:450–8. 4. Ramos JJ, Williams M, Synetos A, et al. Clinical utility
of cardiac computed tomography. Am J Med Sci 2007; 334:350–5.
5. Baur LH. Cardiac imaging at the emergency department is a must! The role of cardiac computed tomography and magnetic resonance imaging in the evaluation of acute chest pain in the emergency department. Int J Cardiovasc Imaging 2008;24:343–4.
6. Vanhoenacker PK, Heijenbrok-Kal MH, Van Heste R, et al. Diagnostic performance of multidetector CT angi-ography for assessment of coronary artery disease: meta-analysis. Radiology 2007;244:419–28.
7. Kroft LJ, de Roos A, Geleijns J. Artifacts in ECG-synchronized MDCT coronary angiography. AJR Am J Roentgenol 2007;189:581–91.
8. Giesler T, Baum U, Ropers D, et al. Noninvasive visual-ization of coronary arteries using contrast-enhanced multidetector CT: influence of heart rate on image quality and stenosis detection. AJR Am J Roentgenol 2002;179:911–6.
9. Nikolaou K, Knez A, Rist C, et al. Accuracy of 64-MDCT in the diagnosis of ischemic heart disease. AJR Am J Roentgenol 2006;187:111–7.
10. Heuschmid M, Kuettner A, Schroeder S, et al. ECG-gated 16-MDCT of the coronary arteries: assessment of image quality and accuracy in detecting stenoses. AJR Am J Roentgenol 2005;184:1413–9.
11. Garcia MJ, Lessick J, Hoffmann MH. Accuracy of 16-row multidetector computed tomography for the assessment of coronary artery stenosis. JAMA 2006;296:403–11. 12. Ferencik M, Nomura CH, Maurovich-Horvat P, et al.
Quantitative parameters of image quality in 64-slice
computed tomography angiography of the coronary arteries. Eur J Radiol 2006;57:373–9.
13. Wintersperger BJ, Nikolaou K, von Ziegler F, et al. Image quality, motion artifacts, and reconstruction timing of 64-slice coronary computed tomography angiography with 0.33-second rotation speed. Invest Radiol 2006;41: 436–42.
14. Pannu HK, Jacobs JE, Lai S, et al. Coronary CT angiog-raphy with 64-MDCT: assessment of vessel visibility. AJR Am J Roentgenol 2006;187:119–26.
15. Leschka S, Husmann L, Desbiolles LM, et al. Optimal image reconstruction intervals for non-invasive coro-nary angiography with 64-slice CT. Eur Radiol 2006; 16:1964–72.
16. Horiguchi J, Kiguchi M, Fujioka C, et al. Radiation dose, image quality, stenosis measurement, and CT densitometry using ECG-triggered coronary 64-MDCT angiography: a phantom study. AJR Am J Roentgenol 2008;190:315–20.
17. Sun Z. Multislice CT angiography in aortic stent grafting: relationship between image noise and body mass index. Eur J Radiol 2007;61:534–40.
18. Yoshimura N, Sabir A, Kubo T, et al. Correlation between image noise and body weight in coronary CTA with 16-row MDCT. Acad Radiol 2006;13:324–8. 19. Jones CM, Athanasiou T, Dunne N, et al. Multi-slice
computed tomography in coronary artery disease. Eur J Cardiothorac Surg 2006;30:443–50.
20. Rybicki FJ, Otero HJ, Steigner ML, et al. Initial evaluation of coronary images from 320-detector row computed tomography. Int J Cardiovasc Imaging 2008;24:535–46. 21. Ferencik M, Moselewski F, Ropers D, et al. Quantitative
parameters of image quality in multidetector spiral computed tomographic coronary imaging with sub-millimeter collimation. Am J Cardiol 2003;92:1257–62. 22. Heyer CM, Mohr PS, Lemburg SP, et al. Image quality
and radiation exposure at pulmonary CT angiography with 100- or 120-kVp protocol: prospective randomized study. Radiology 2007;245:577–83.
23. Cademartiri F, Mollet NR, van der Lugt A, et al. Intravenous contrast material administration at helical 16-detector row CT coronary angiography: effect of iodine concentration on vascular attenuation. Radiology 2005;236:661–5.
24. Fleischmann D. Use of high-concentration contrast media in multiple-detector-row CT: principles and rationale. Eur Radiol 2003;13(Suppl 5):M14–20.
收文日期:98 年 8 月 20 日 接受刊載:98 年 9 月 9 日 通訊作者 : 許瑞昇醫師 高雄巿立小港醫院影像醫學科 高雄巿 812 小港區山明路 482 號