中國醫藥大學機構典藏 China Medical University Repository, Taiwan:Item 310903500/2362
6
0
0
全文
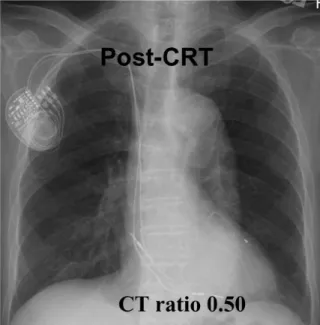
(2) Chung-Ho Hsu, et al.. 51. Patient 1. Patient 2. Fig. 1. Chest roentgenograms showing reduction in heart sizes after cardiac resynchronization therapy (CRT). CT = cardiothoracic.. the onset of AF. The baseline ECG showed left bundle branch block with a QRS duration of 174 ms. After excluding left atrial thrombus by transesophageal echocardiography, sinus rhythm was restored after successful electrical cardioversion of AF. A temporary pacemaker was implanted by successful AV junction ablation. The next day, a CRT pacemaker (Medtronic, InSync III, model 8042) was implanted. The left. ventricle was paced 20 ms earlier than the right ventricle, which produced the narrowest paced QRS complexes. The AV delay was adjusted according to Ritter's formula [10]. At 11-month follow-up, the NYHA functional class had improved from class IV to class II. Chest roentgenograms and echocardiography showed marked reduction in cardiac size (Fig. 1, upper panel; Table). Echocardiograms also showed improvement in.
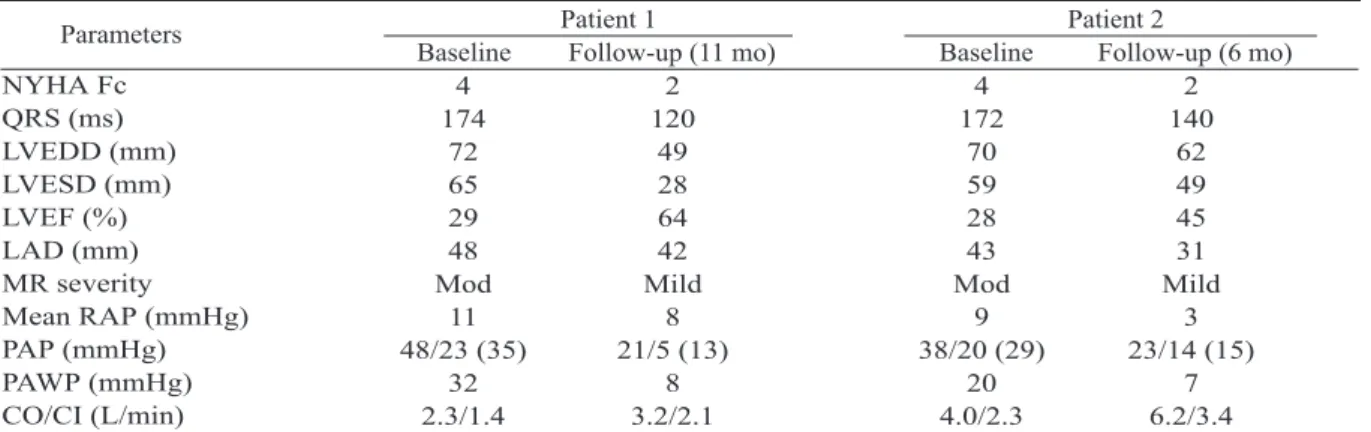
(3) 52. Cardiac Resynchronization and Rhythm Control of Atrial Fibrillation. Table. Functional class, QRS duration, echocardiographic and hemodynamic parameters at baseline and after intervention Patient 1 Patient 2 Parameters Baseline Follow-up (11 mo) Baseline Follow-up (6 mo) NYHA Fc 4 2 4 2 QRS (ms) 174 120 172 140 LVEDD (mm) 72 49 70 62 LVESD (mm) 65 28 59 49 LVEF (%) 29 64 28 45 LAD (mm) 48 42 43 31 MR severity Mod Mild Mod Mild Mean RAP (mmHg) 11 8 9 3 PAP (mmHg) 48/23 (35) 21/5 (13) 38/20 (29) 23/14 (15) PAWP (mmHg) 32 8 20 7 CO/CI (L/min) 2.3/1.4 3.2/2.1 4.0/2.3 6.2/3.4 Fc = functional class; LVEDD = left ventricular end-diastolic dimension; LVESD = left ventricular end-systolic dimension; LVEF = left ventricular ejection fraction; LAD = left atrial dimension; MR = mitral regurgitation; RAP = right atrium pressure; PAP = pulmonary artery pressure; PAWP = pulmonary artery wedge pressure; CO = cardiac output; CI = cardiac index; Mod = moderate.. A. B. Fig. 2. Stored algorithm recordings from the pacemaker show freedom of atrial fibrillation in patient 1 (panel A) and a decrease in atrial fibrillation frequency and duration in patient 2 (panel B).. left ventricular ejection fraction from 29% to 64% and decrease in the degree of mitral regurgitation. Hemodynamic study displayed normalization of pulmonary artery wedge pressure, pulmonary artery pressure and right atrium pressure (Table). The patient has been maintained in sinus rhythm and free of AF episodes since the operation, as documented by the stored data from the pacemaker (Fig. 2A), while on the same dose of amiodarone, which was previously ineffective for AF control. Patient 2. A 57-year-old man with dilated cardiomyopathy and persistent AF was admitted in April 2003 for CRT because of advanced CHF refractory to treatment with carvedilol, digoxin, captopril, losartan and furosemide. Paroxysmal. AF was detected in October 2001. Sinus rhythm had been maintained with amiodarone until AF became persistent in March 2002. The patient presented with AF, rapid ventricular rate and deteriorating CHF. The baseline ECG displayed left bundle branch block with a QRS duration of 172 ms. After excluding left atrial thrombus by transesophageal echocardiography, sinus rhythm was restored after successful electrical cardioversion of AF. A temporary pacemaker was inserted followed by successful AV junction ablation. The next day, a CRT pacemaker (Medtronic, In-Sync III, model 8042) was implanted. The left ventricle was paced 20 ms earlier than the right ventricle, which produced the narrowest QRS duration. The AV delay was.
(4) Chung-Ho Hsu, et al.. adjusted according to Ritter's formula. Six months after the procedure, the NYHA functional class had improved from class IV to II. Chest roentgenograms showed reduction of cardiothoracic ratio (Fig. 1, lower panel). Echocardiograms revealed an increase in left ventricular ejection fraction from 28% to 45%, a reduction in the severity of mitral regurgitation and a decrease in left atrial and left ventricular dimensions (Table). Hemodynamic study displayed normalization of pulmonary artery wedge pressure, pulmonary artery pressure and right atrium pressure (Table). Stored data from the pacemaker showed marked reduction of paroxysmal AF episodes (Fig. 2B). DISCUSSION. CRT with atrial-synchronized biventricular pacing in patients with refractory heart failure and left bundle branch block improves symptoms, quality of life, exercise capacity and left ventricular function [1-8]. AF is a common arrhythmia associated with moderate-to-severe CHF [9]. Previous studies have demonstrated that the effects of CRT on CHF are comparable between patients with stable sinus rhythm and those with chronic AF [11]; however, whether CRT provides additional beneficial effects for rhythm control of AF in patients with CHF is not well documented in the literature. Malinowski [12] described a spontaneous recovery of permanent AF to sinus rhythm 17 months after biventricular pacing in a 68-year-old man with refractory CHF without AV nodal ablation and cardioversion. The outcome in our two patients also provides anecdotal evidence which suggests that CRT, in addition to improving refractory heart failure, may improve rhythm control of AF. Animal models have demonstrated that chronic atrial enlargement may increase vulnerability to atrial arrhythmias caused by atrial electrical remodeling in response to chronic atrial stretch [13-15]. Thus, we speculate that CRT in CHF improves rhythm control of AF by reversing atrial enlargement and diminishing the atrial pressure. In our patients, electrical cardioversion. 53. was performed to restore sinus rhythm prior to biventricular pacing, and amiodarone was maintained after the interventions. This therapeutic approach resulted in complete elimination of AF in one patient and diminished frequency of paroxysmal AF in the other during a follow-up period of 11 months and 6 months respectively. In both patients, echocardiographic studies demonstrated reduction in the left atrial and left ventricular dimensions and mitral regurgitation severity, as well as improvement in the left ventricular ejection fraction. Hemodynamic studies displayed normalization of the pulmonary artery wedge, pulmonary artery and right atrial pressures as well as improvement in cardiac output. The beneficial effect of rhythm control of AF correlated with the favorable changes in echocardiographic and hemodynamic parameters during follow-up. The reduction of left ventricular dimension and improvement in the left ventricular ejection fraction, decreased left atrial dimension and stretch, hence improved rhythm control of AF. Melenovsky [16] et al concluded that in heart failure patients with AF, RR-interval irregularity worsens cardiac function at elevated but not at normal range heart rate. Overall rate control is most important in these patients while rate regularization of rapid AF may impart additional benefits. Ozcan et al [17] demonstrated that in patients with drug-refractory AF and left ventricular dysfunction, control of ventricular rate by AV junction ablation and implantation of a conventional single or dual-chamber pacemaker is associated with improved left ventricular function. They found near normalization of left ventricular ejection fraction in 29% of study patients, in whom the observed survival was comparable to that of the normal subjects. In a similar study [18], the improvement in left ventricular systolic function had been found to be due to reduction of the end-systolic left ventricular diameter with no appreciable change in the end-diastolic diameter. Therefore, based on the above evidence, we believed that adequate control of ventricular rate after AV junction ablation might have exerted a synergistic effect.
(5) 54. Cardiac Resynchronization and Rhythm Control of Atrial Fibrillation. on the left ventricular systolic function in our patients. Nonetheless, CRT was responsible for the improvement of left ventricular function as significant reduction of the end-diastolic along with the end-systolic left ventricular dimension was observed in our patients. In summary, our report demonstrates that CRT in CHF patients can facilitate rhythm control of AF, possibly by reversing chronic atrial stretch and diminishing atrial pressure by reversing the atrial anatomical-electrical remodeling process. REFERENCES. 1. Leclercq C, Cazeau S, Le Breton H, et al. Acute hemodynamic effects of biventricular DDD pacing in patients with end-stage heart failure. J Am Coll Cardiol 1998;32:1825-31. 2. Kass DA, Chen CH, Curry C, et al. Improved left ventricular mechanics from acute VDD pacing in patients with dilated cardiomyopathy and ventricular conduction delay. Circulation 1999;99:1567-73. 3. Auricchio A, Stellbrink C, Block M, et al. Effect of pacing chamber and atrioventricular delay on acute systolic function of paced patients with congestive heart failure. Circulation 1999;99:2993-3001. 4. Leclercq C, Cazeau S, Ritter P, et al. A pilot experience with permanent biventricular pacing to treat advanced heart failure. Am Heart J 2000; 140:862-70. 5. Etienne Y, Mansourati J, Touiza A, et al. Evaluation of left ventricular function and mitral regurgitation during left ventricular-based pacing in patients with heart failure. Eur J Heart Fail 2001;3:441-7. 6. Cazeau S, Leclercq C, Lavergne T, et al. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med 2001;344:873-80. 7. Gras D, Leclercq C, Tang AS, et al. Cardiac resynchronization therapy in advanced heart failure the multicenter InSync clinical study. Eur J Heart Fail 2002;4:311-20. 8. St John Sutton MG, Plappert T, Abraham WT, et al. Effect of cardiac resynchronization therapy on left ventricular size and function in chronic heart failure. Circulation 2003;107:1985-90.. 9. Stellbrink C, Auricchio A, Diem B, et al. Potential benefit of biventricular pacing in patients with congestive heart failure and ventricular tachyarrhythmia. Am J Cardiol 1999;83:143-50. 10.Ritter P, Padeletti L, Gillio-Meina L, et al. Determination of the optimal atrioventricular delay in DDD pacing. Comparison between echo and peak endocardial acceleration measurements. Europace 1999;1:126-30. 11. Leclercq C, Victor F, Alonso C, et al. Comparative effects of permanent biventricular pacing for refractory heart failure in patients with stable sinus rhythm or chronic atrial fibrillation. Am J Cardiol 2000;85:1154-6,A9. 12. Malinowski K. Spontaneous conversion of permanent atrial fibrillation into stable sinus rhythm after 17 months of biventricular pacing. Pacing Clin Electrophysiol 2003;26:1554-5. 13.Boyden PA, Hoffman BF. The effects on atrial electrophysiology and structure of surgically induced right atrial enlargement in dogs. Circ Res 1981;49: 1319-31. 14. Li D, Fareh S, Leung TK, et al. Promotion of atrial fibrillation by heart failure in dogs: atrial remodeling of a different sort. Circulation 1999;100:87-95. 15. Kalman JM, Sparks PB. Electrical remodeling of the atria as a consequence of atrial stretch. J Cardiovasc Electrophysiol 2001;12:51-5. 16. Melenovsky V, Hay I, Fetics BJ, et al. Functional impact of rate irregularity in patients with heart failure and atrial fibrillation receiving cardiac resynchronization therapy. Euro Heart J 2005;26:70511. 17. Ozcan C, Jahangir A, Friedman PA, et al. Significant effects of atrioventricular node ablation and pacemaker implantation on left ventricular function and long-term survival in patients with atrial fibrillation and left ventricular dysfunction. Am J Cardiol 2003;92:33-7. 18. Heinz G, Siostrzonek P, Kreiner G, et al. Improvement in left ventricular systolic function after successful radiofrequency His bundle ablation for drug refractory, chronic atrial fibrillation and recurrent atrial flutter. Am J Cardiol 1992;69:489-92..
(6) 55. 11 6 2006;11:50-5. 403. 2. 2005. 3. 2005. 12. 24 30. 2005. 11. 29.
(7)
數據
相關文件
Effectiveness of robot-assisted upper limb training on spasticity, function and muscle activity in chronic stroke patients treated with botulinum toxin: A randomized single-
Even though in this case the patient was treated for AML after the age of 5, the long-term side effects of the chemo and/or radiotherapy caused anomalies in all his permanent
The chairman/representative director, and at least 2/3 of the board of directors of a limited company or a company limited by shares providing the above services shall be the Republic
Buttermilk, curdled milk and cream, Yogurt, kephir and other fermented or acidified milk and cream, whether or not concentrated or containing added sugar or other sweetening matter
Milk and cream, in powder, granule or other solid form, of a fat content, by weight, exceeding 1.5%, not containing added sugar or other sweetening matter.
Center for Faculty Development, Department of Medical Education, Taichung Veterans General Hospital 1 Department of Nursing, Hungkuang University, Taichung, Taiwan 2. Section
Center for Faculty Development, Department of Medical Education, Taichung Veterans General Hospital 2 School of Medicine, National Yang-Ming University, Taipei, Taiwan 3.
A discussion of the Dapagli flozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) trial, the Effect of Sotagli flozin on Car- diovascular Events in Patients
