經皮神經電刺激足三里穴對全身麻醉中改善胰島素阻抗之臨床評估; A Pilot Randomized Control Clinical Trial of Improving Insulin Resistance by Transcutaneous Electrical Nerve Stimulation (TENS) on Zusanli Acupoints (ST36) during General Anesthesia
56
0
0
全文
(2) Contents Contents……………………………………………………………..………..i Contents of Tables…………………………………………………………..iii Contents of Figures…..……………………………………………………..iv Abstract………………………………………………………………….......v Chapter 1. Introduction…………………………………………………........1 Section 1. Background…………………………………………………….1 Section 2. Aims of this study……………………………………………...8 Chapter 2. Materials and Methods…………………………………………...9 Section 1. Study design and patients………………..…………….………9 Section 2. Acupoints and methods of TENS…………………………….11 Section 3. Venous blood collection...…………………………………….13 Section 4. Assay of plasma glucose, insulin, and insulin resistance…….14 Section 5. General anesthesia and monitoring…………………………..16 Section 6. Statistical analysis…………………………………………….17 Chapter 3. Results…………………………………………………………..18 Chapter 4. Discussion…………………………………………………........30 Chapter 5. Conclusion……………………………………………………...34 Chapter 6. References…………………………………………………........35 中文摘要………………………………………………………………...…39 i.
(3) Appendix I…………………………………………………………….........40 Appendix II……………………………………………………………........42. ii.
(4) Contents of Table and Consort E-Flowchart Table 1. Demographic data and clinical variables of 52 intend to analyze patients of the placebo group and the TENS group……………………..….21 The Consort E-Flowchart Aug 2005……………………………………..22. iii.
(5) Contents of Figures and Photographs Figure 1. Plasma glucose lowering effect.……………………………........23 Figure 2. Hypoglycemic activity..…………………………………….........24 Figure 3. Comparing the plasma insulin level during general anesthesia……….………………………………….…………………..…...25 Figure 4. HOMA index represented insulin sensitivity of general anesthesia in a time course curve…………………………………………………........26 Photograph 1: The operating TENS stimulator….……….......……….......27 Photograph 2: The connection of HANS stimulator between acupoints………………………………...………………...28 Photograph 3: Lateral view of TENS at bilateral Zusanli acupoints and Sanyinjiao acupoints:………………………...……………29. iv.
(6) Abstract Transcutaneous complementary. electrical. therapy. to. nerve the. stimulation. pharmacological. (TENS). was. management. a of. postoperative pain for long time. However, the hypoglycemic effect and insulin resistance (IR) improvement by TENS on specific acupoints had not been investigated. We designed a single blind, randomized control clinical study of 60 female patients, scheduled for elective low abdominal surgery. The 52 patients consented to enrollment and were assigned to receive either TENS (n = 26) on bilateral Zusanli (ST36) acupoints with continuous mode at a frequency of 15 Hz and the intensity of 10 mA synchronously for 30 minutes or non-stimulation (placebo group, n = 26) during general anesthesia to examine the effects on lowering plasma glucose and improving IR. Statistically significant lowering plasma glucose level, hypoglycemic activity, and lower homeostasis model assessment (HOMA-IR) index were obtained in the TENS group (p 0.05) than the placebo group. We recommend TENS at bilateral Zusanli acupoints as an alternative management for diabetic patients to control plasma glucose level and to improve IR perioperatively. Key words:TENS; Zusanli acupoint; plasma glucose; insulin resistance. v.
(7) Chapter 1. Introduction Section 1. Background Diabetes mellitus Diabetes mellitus is a common endocrine disease that is characterized by long-term complications involving the blood vessels, kidneys, nerves, and eyes.1 Subsequently, for diabetic patients undergoing major surgery more frequently than those without diabetes,2 the major risk factors are heart disease, stroke, kidney disease, blindness, and nontraumatic amputation.1 Of importance to the anesthesiologist is preoperative treatment of patients with such complications. Some of the chronic complications of diabetes may be prevented or improved by chronic “tight” control of Type I diabetes, to a certain degree.3 However, the benefits associated with tight control of blood glucose are debatable when considering the benefit-to-risk ratio. For example, tight control of blood glucose benefits diabetics that are undergoing cardiopulmonary bypass, and those undergoing global central nerve system ischemia, but as there is little evidence of benefit to other groups, the benefit-to-risk ratio of tight glucose control has not been assessed.3 The diabetic population is not homogeneous and several diabetic. 1.
(8) syndromes exist. Hyperglycemia is a major phenotype of diabetes mellitus. The criteria for the diagnosis of diabetes mellitus is one of the following:4 1. Symptoms of diabetes plus random blood glucose concentration 11.1 mmol/L (200 mg/dL) since the last meal. 2. Fasting at least 8 hours plasma glucose 7.0 mmol/L (126 mg/dL). 3. Two-hour plasma glucose 11.1 mmol/L (200 mg/dL) during an oral glucose tolerance test. Depending on the etiology of the diabetes mellitus, factors contributing to hyperglycemia may include reduced insulin secretion, decreased glucose utilization, increased insulin resistance (IR), and increased glucose production.4 Etiologic classification of diabetes mellitus:4 I.. Type I diabetes (insulin dependent diabetes mellitus, IDDM): Causes of -cell destruction that leading to absolute insulin deficiency. 1. Immune-mediated 2. Idiopathic. II.. Type II (non-insulin dependent diabetes mellitus, NIDDM): Range from IR with relative insulin deficiency to an insulin secretory defect with IR.. 2.
(9) III.. Other specific types of diabetes 1. Genetic defects of -cell function of pancrease characterized by mutations in: i.. Hepatocyte nuclear transcription factor (HNF) 4 (MODY 1). ii.. Glucokinase (MODY 2). iii.. HNF-1 (MODY 3). iv.. Insulin promoter factor (IPF) 1 (MODY 4). v.. HNF-1 (MODY 5). vi.. NeuroD1 (MODY 6). vii.. Mitochondrial DNA. viii. Proinsulin or insulin conversion 2. Genetic defects in insulin action: i.. Type A IR. ii.. Leperchaunism. iii.. Rabson-Mendenhall syndrome. iv.. Lipodystrophy syndromes. 3. Disease of the exocrine pancreas 4. Endocrinopathies. 3.
(10) 5. Drug or chemical-induced 6. Infections 7. Uncommon forms of immune-mediated diabetes 8. Other genetic syndromes sometimes associated with diabetes IV.. Gestational diabetes mellitus.. The. multifactorial. causes. of. diabetic. complications. include. glycosylation of proteins and glucose reduction to sorbital (which functions as a tissue toxin).5 In addition, glycosylation of the atlanto-occipital joint may limit joint mobility and cause difficulty with airway management (“stiff-neck” syndrome).6 Otherwise hyperglycemia is the major factor in the development of diabetic complications.7 The Somogyi effect also describes the rebound hyperglycemia following a hypoglycemic reaction.8 Careful monitoring ensures successful management of blood glucose perioperatively. Patients with NIDDM may develop metabolic disorder, coronary artery disease, nephropathy, neuropathy, nontraumatic lower extremity amputations, and adult blindness. With an increasing incidence worldwide, diabetes mellitus will be a leading cause of morbidity and mortality for the foreseeable future.9 In Taiwan, diabetes has become the fourth among the top ten causes of death.10-12. 4.
(11) Hyperglycemic response to stress during general anesthesia It is commonly known that an increased secretion of endogenous catecholamines is found in a neurohormonal response to stress during general anesthesia with subsequent increase of plasma cortisol, glucagon, and glucose, along with hemodynamic changes of increased heart rate, blood pressure, and cardiac output.13 An increased plasma glucose level is associated with poor clinical outcome or cell death during critical illness.14 Surgical mortality rates are on average five times higher for the diabetic population than for the non-diabetic population.3 Hyperglycemia is a common result of stress signals caused by pain and surgical procedure.14 As we know in many reports, volatile anesthetics directly manipulate glucose homeostasis by affecting pancreatic insulin release15-17 and induce hyperglycemia without surgical stress.15,. 18-22. The. hyperglycemic response is also observed during isoflurane anesthesia that is a consequence of both impaired glucose clearance and increased production of glucose.18 Both sevoflurane and isoflurane anesthesia also impair glucose tolerance to the same degree and is independent of agent and dosage up to 1.5 minimum alveolar concentration (MAC).22. 5.
(12) Methods to increase insulin sensitivity There is a hope for controlling blood glucose in insulin dependent diabetic patient since the discovery of insulin. However, the IR, especially patients with NIDDM has been become another medical issue to be solved. Thus, methods to increase insulin sensitivity have become importance. In Chinese medicine, “Chi” (Qi) is a metaphysical concept of supposed body energy that runs through 365 designated acupuncture points within the hypothesized meridians which can be stimulated by the needles or “moxibustion” (lighted punks of artemis vulgaris) to balance “Yin and Yang” by relieving blockage in the flow of “Chi”.23 The regulation of Chi is also similar to the change in the kinetic effects of insulin.24 Opioid analgesics have become the treatment of choice for the management of pain control. Furthermore, opioid participates in the regulation of endocrine processes, including glucose metabolism.25 Activation of -opioid receptors on the insulin-targeted organs seems to be an important role for lowering plasma glucose and increasing insulin sensitivity, although the direct role of -opioid receptors for the improving insulin resistance has not been completely investigated.7 Transcutaneous electrical nerve stimulation (TENS) is a complementary therapy to the. 6.
(13) pharmacological management of pain.26 Many clinical studies have reported that TENS also is an adjunct method for the management of postoperative pain.27, 28 It has been shown that postoperative treatment with TENS results in decreased analgesic consumption and lower incidence of postoperative complications.27 Importantly, a study showed that stimulation of the Zusanli (ST36) acupoint was effective in decreasing both the postoperative opioid analgesic needed and opioid-related side effects.29 The implication of this finding is that the location of the stimulating electrodes is significant in determining the efficacy of TENS in reducing postoperative pain. Besides treatment for postoperative pain, TENS has been applied to acupoints to increase muscle strength after acute stroke.30 Of the non-pharmacological methods to manage pain, TENS is the most non-invasive method. Conversely, needle acupuncture is an invasive, skill-based procedure and the possible risks of broken needles, infection and transient hypotension have been reported.31 A significant animal study using acupuncture found that rats had enhanced hypoglycemic activity and insulin sensitivity when electroacupuncture was applied on bilateral Zusanli acupoints.24 There have been few studies that evaluated the effects of TENS on the specific acupoints, and as such, this clinical investigation is a pioneer study in its field also.32, 33. 7.
(14) Section 2. Aims of this study Based on findings from previous research, we hypothesized that preoperative application of TENS to the classical Chinese acupoints Zusanli would lower the plasma glucose and increase the sensitivity of insulin during general anesthesia. We designed a single blind, randomized control clinical trial to test our hypotheses that TENS has hypoglycemic activity and improve IR.. 8.
(15) Chapter 2. Materials and Methods Section 1. Study design and patients This study was designed in a single blind, randomized control trial, and 60 American Society of Anesthesiologists (ASA) physical status I or II female patients, scheduled for elective abdominal total hysterectomy or laparoscopic assisted vaginal hysterectomy procedures, were enrolled in this study after written and informed consent. The Tungs’ General Hospital Institutional Review Board approved this study protocol (IRB97006-1). According to the following inclusion and exclusion criteria, the patients were grouped randomly. Inclusion criteria: 1. 35-75 year old non-diabetic female patients. 2. Body weight: 50-80 kg. 3. ASA class I-II. 4. Elective for lower abdominal surgery. Exclusion criteria: 1. Heart disease, arrhythmia, inserted pace maker. 2. Cerebral vascular disease. 3. Hepatic disease (GOT, GPT 40 IU/L).. 9.
(16) 4. Renal disease (BUN 22 mg/dL, Creatinine 1.5 mg/dL). 5. Coagulation dysfunction. 6. Pregnant women. 7. Pre-operative and/or intra-operative blood transfusion. 8. Fisevoflurane > 2.5 % during general anesthesia.. 10.
(17) Section 2. Acupoints and methods of TENS According to the theory of traditional Chinese medicine, Zusanli acupoint is within stomach meridian of Foot-Yang-Ming, (ST). The location of Zusanli acupoint is inside the anterior tibia muscle three cun below knee laterally. And the location of Sanyinjiao (SP6) acupoint is at the medial side of the leg, three cun above the tip of the medial malleolus posterior to the medial border of the tibia. Identification of these acupoints, attachment of the electrodes on skin, and operation of the TENS stimulator were be performed by the same anesthesiologist. Due to three patients refusing to joint our clinical trial during the preoperative visit, 57 patients were randomly assigned to receive either transcutaneous electrical nerve stimulation (TENS group, n = 28) with continuous mode at a frequency of 15 Hz and the intensity of 10 mA on both Zusanli acupoints synchronously for 30 minutes or non-electrical nerve stimulation (placebo group, n = 29) before the induction of general anesthesia (Photograph 1, 2). During the preoperative visit, both the placebo group and the TENS group were informed that an electrode was to be placed on the Zusanli acupoint and Sanyinjiao acupoint prior to the induction of anesthesia. The. 11.
(18) electrodes placed for the TENS group were connected to the TENS stimulator (HANS LY257; Healthronics, Singapore). By contrast, the electrodes placed for the placebo group were not connected to the TENS stimulator. The positive electrodes and the negative electrodes were connected to bilateral Zusanli (ST36) and Sanyinjiao (SP6) acupoints respectively. The TENS group was informed that the electrodes needed to be connected to the TENS stimulator to be effective, but the placebo group was told that the electrodes on Zusanli acupoint and Sanyinjiao acupoint were sufficient for the treatment (Photograph 2, 3).. 12.
(19) Section 3. Venous blood collection For both groups, 3 mL venous blood was drawn as the baseline before the placement of electrodes on the bilateral Zusanli acupoints, and thus before the commencement of TENS stimulation for the TENS group. The continuous TENS stimulation was then started at the bilateral Zusanli acupoints and Sanyinjiao acupoints synchronously for the TENS group only, and TENS stimulation was automatically stopped after 30 minutes. At this point for both groups, anesthesia was induced with intravenous anesthetics, followed by the drawing of venous blood. General anesthesia was maintained for the duration of the surgery with 2.0 0.5% sevoflurane for all patients. During 60 minutes of general anesthesia, skin incision commenced for all patients in both groups, and blood was subsequently drawn. At the 90-minute and 120-minute time points after the induction of anesthesia, blood was collected for both groups.. 13.
(20) Section 4. Assay of plasma glucose, insulin, and insulin resistance All the blood samples were analyzed for the plasma concentration of glucose by automatic analyzer (HITACHI 7170A, Tokyo, Japan). And the plasma concentration of insulin was analyzed by the human enzyme-linked immunosorbent. assays. (ELISA,. DSL-10-1600,. Diagnostic. System. Laboratories. INC; Webster, Texas, USA) in both groups. The procedures are as below: 1. Mark the microtitration strips to be used. 2. Add 25 L serum to standard samples into the appropriate wells. 3. Add 100 L of the Insulin Antibody-Enzyme Conjugate Solution into each well. 4. Incubate the wells, shaking at a fast speed (500-700 rpm) on an orbital shaker, at room temperature of 25C for one hour. 5. Aspirate and wash each well 5 times for 30 seconds with 200 L washing buffer. Blot and dry by inverting plate on absorbent material. 6. Add 100 L of the TMB Chromogen solution to each well. 7. Incubate the wells, shaking at a fast speed (500-700 rpm) on an orbital shaker, at room temperature of 25C for 10 minutes and avoid exposure to direct sunlight.. 14.
(21) 8. Add 100 L of 0.2 M sulfuric acidic stopping solution to each well. 9. Read the absorbance of the solution in the well within 30 minutes by wavelength at 450 nm. Insulin resistance (IR) was assessed by using the homeostasis model assessment (HOMA) index.34 HOMA-IR = FG (mg/dL) FI (IU/mL) / 22.5. Where FG and FI represented as fasting plasma glucose and fasting plasma insulin, respectively.. 15.
(22) Section 5. General anesthesia and monitoring General anesthesia was induced with intravenous fentanyl (2 g/kg), thiamylal sodium (4-5 mg/kg), 2% lidocaine (1 mg/kg), and esmeron (0.8-1 mg/kg) for facilitating tracheal intubation. The anesthesia was maintained by 2.0 0.5% sevoflurane in 100% oxygen. No additional opioid analgesics were given intraoperatively. Intravenous route was setup with 0.9% normal saline for all patients in this clinical trail preoperatively and intraoperatively. During general anesthesia, heart rate, non-invasive blood pressure, pulse oximetry, body temperature, FiO2, End-tidal CO2, Fisevo, and End-tidalsevo were monitored completely. The room temperature of operation room is set within the standard range of 18-25C.. 16.
(23) Section 6. Statistical analysis The demographic data for all the patients were expressed as mean SEM using Student’s t-test in Table 1. All values were expressed as mean SEM in the figures. “n” was represented as number of patients in each group. The One-way ANOVA method was applied to compare the values of the plasma glucose levels in each group. A self-paired t-test was applied in the dependent samples to compare levels before and after TENS in TENS group or same conditions as TENS group without stimulation in placebo group. For all comparisons, p 0.05 was considered statistically significant. The hypoglycemic activity (HA) (%) was calculated: HA = (PG1-PG0) PG0 100%. Where PG1 and PG0 represented as plasma glucose level of one time point and plasma glucose level at the beginning, respectively.. 17.
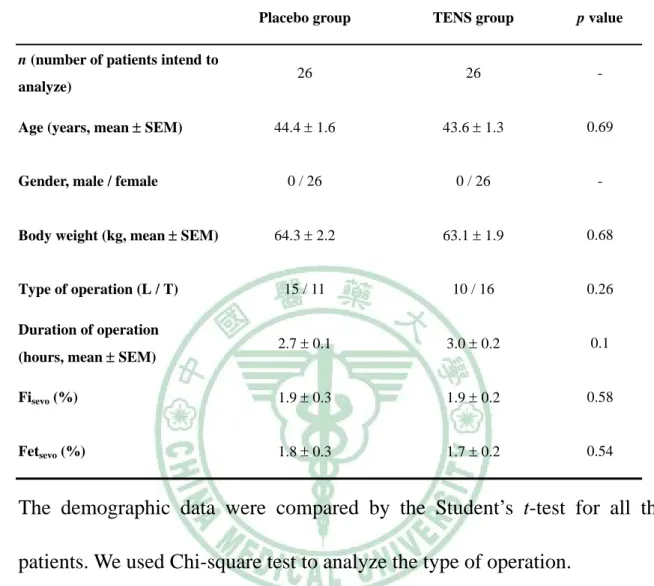
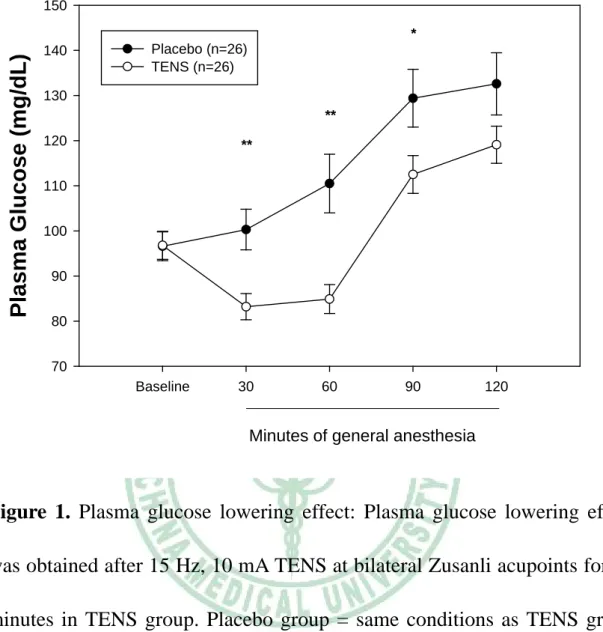
(24) Chapter 3. Results Both the demographic and clinical variables of 52 intend to analyze patients were comparable between these two groups. There were no significant differences in the patients’ age, weight, surgical time, and type of operation between TENS group and placebo group (Table 1). The concentration of supplied sevoflurane and end-tidal sevoflurane in percentage was not significantly different between TENS group and placebo group statistically (Table 1). Initially, there was no significant difference between TENS group and the placebo group in the plasma glucose level (Figure 1). Statistically significant plasma glucose lowering effects were obtained after 15 Hz, 10 mA, and 30 minutes of TENS on bilateral Zusanli acupoints during the period of general anesthesia induction and surgical incision in TENS group (**p 0.005) (Figure1). On the other hand, the levels of plasma glucose in TENS group were significant different from placebo group at 30 and 60 minutes under general anesthesia statistically (**p < 0.005). In addition, plasma glucose levels were also found statistically significant difference at 60 minutes and 90 minutes of general anesthesia between TENS group and placebo group (**p < 0.005 and *p < 0.05, respectively) (Figure 1).. 18.
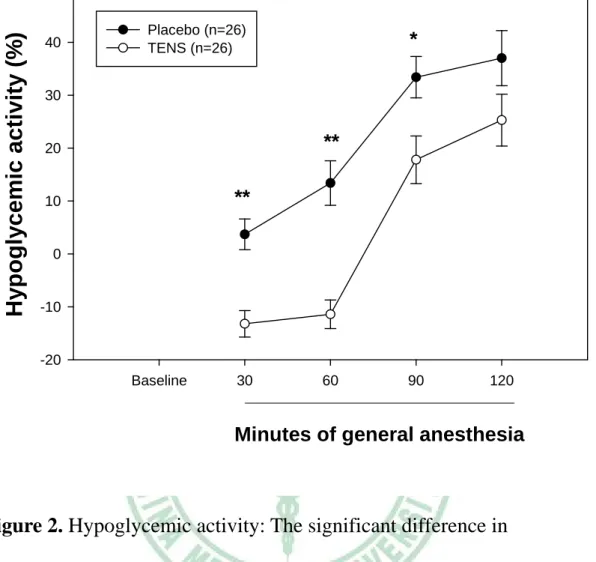
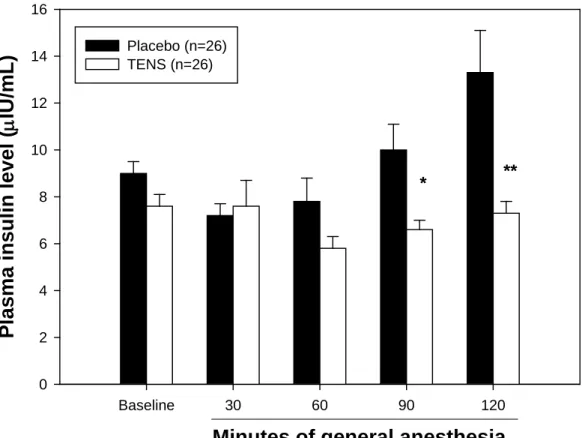
(25) The results of HA were shown in Figure 2. In TENS group, the hypoglycemic effect was obtained 13.2 2.5% and 11.4 2.7% after 30 minutes and 60 minutes of TENS respectively. No further hypoglycemic activities were noted after 90 and 120 minutes of TENS in TENS group. Furthermore, there were statistically significant differences of the hypoglycemic effect after 30, 60, and 90 minutes TENS between TENS group and placebo group (Figure 2). Although the level of plasma glucose was increased in 90 and 120 minutes after TENS in TENS group, the percentage of hypoglycemic activity was still lower than the placebo group at the same points of time (Figure 2). In the placebo group, the plasma glucose increased during induction of general anesthesia, surgical incision, and throughout the operation (Figure 1). Although there was no statistically significant difference in the level of plasma insulin between TENS group and placebo group during the period of induction of general anesthesia and/or the time of surgical incision (Figure 3), the significant difference in hypoglycemic effect was found at the same point of time in TENS group than in placebo group. As well, the plasma insulin levels were statistically significant lower in TENS group (90 and 120 minutes after TENS, p < 0.01 and p < 0.005, respectively) than in placebo. 19.
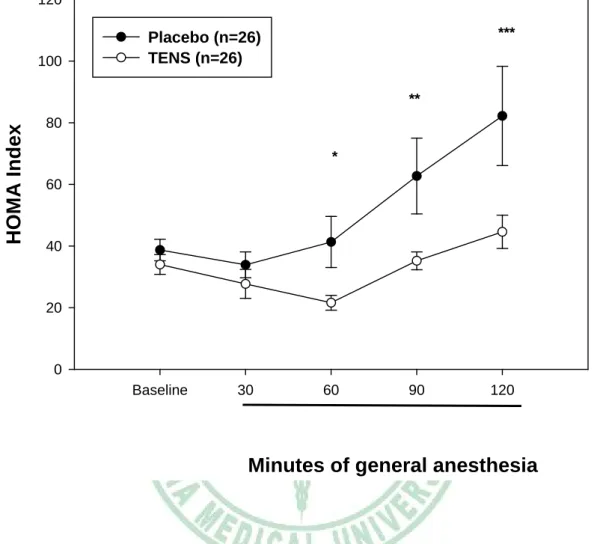
(26) group during surgical procedure (Figure 3). These results indicated that the sensitivity of plasma insulin was increased in TENS group compared to the placebo group. On the other hand, the IR increased during general anesthesia by using the inhalation of sevoflurane. The HOMA index of the TENS group was also statistically significant lower in TENS group than placebo group (Figure 4).. 20.
(27) Table 1. Demographic data and clinical variables of 52 intend to analyze patients of the placebo group and the TENS group. Placebo group. TENS group. p value. 26. 26. -. 44.4 1.6. 43.6 1.3. 0.69. 0 / 26. 0 / 26. -. 64.3 2.2. 63.1 1.9. 0.68. 15 / 11. 10 / 16. 0.26. 2.7 0.1. 3.0 0.2. 0.1. Fisevo (%). 1.9 0.3. 1.9 0.2. 0.58. Fetsevo (%). 1.8 0.3. 1.7 0.2. 0.54. n (number of patients intend to analyze) Age (years, mean SEM). Gender, male / female Body weight (kg, mean SEM). Type of operation (L / T) Duration of operation (hours, mean SEM). The demographic data were compared by the Student’s t-test for all the patients. We used Chi-square test to analyze the type of operation. L= Laparoscopic assisted vaginal hysterectomy T = Total abdominal hysterectomy. 21.
(28) The Consort E-Flowchart Aug. 2005 Assessed for eligibility (n = 60 ). Enrollment. Randomized (n = 57). Allocated to placebo group (n = 29) Received allocated intervention (n = 29). Lost to follow-up (n = 0) Excluded from analysis (n = 3) Give reasons: Sevoflurane > 2.5 %. Analyzed (n = 26). Allocation. Follow-Up. 22 Analysis. Excluded (n = 3) Refused to participate (n = 3). Allocated to TENS group (n = 28) Received allocated intervention (n = 28). Lost to follow-up (n = 0) Excluded from analysis (n = 2) Give reasons: Sevoflurane > 2.5 %. Analyzed (n= 26).
(29) 150. Plasma Glucose (mg/dL). * 140. Placebo (n=26) TENS (n=26). 130 ** 120. **. 110 100 90 80 70 Baseline. 30. 60. 90. 120. Minutes of general anesthesia. Figure 1. Plasma glucose lowering effect: Plasma glucose lowering effect was obtained after 15 Hz, 10 mA TENS at bilateral Zusanli acupoints for 30 minutes in TENS group. Placebo group = same conditions as TENS group without stimulation. 30 minutes = period of general anesthesia induction. 60 minutes = surgical incision under general anesthesia. * p < 0.05, ** p < 0.005 vs. the placebo group at the same time.. 23.
(30) Hypoglycemic activity (%). 50. 40. Placebo (n=26) TENS (n=26). *. 30. **. 20. **. 10. 0. -10. -20 Baseline. 30. 60. 90. 120. Minutes of general anesthesia. Figure 2. Hypoglycemic activity: The significant difference in hypoglycemic activity (%) showed between placebo group and TENS group. * p < 0.01, ** p < 0.001.. 24.
(31) Plasma insulin level (IU/mL). 16 14. Placebo (n=26) TENS (n=26). 12 10. *. 8. **. 6 4 2 0 Baseline. 30. 60. 90. 120. Minutes of general anesthesia. Figure 3. Comparing the plasma insulin level during general anesthesia: Comparing the plasma insulin level during general anesthesia between TENS group and placebo group. Baseline = plasma insulin level before general anesthesia. TENS = 15 Hz, 10 mA TENS at bilateral Zusanli acupoints for 30 minutes. Placebo group = the same conditions as TENS group without TENS * p < 0.01, ** p < 0.005 vs. the placebo group at the same time.. 25.
(32) 120. 100. ***. Placebo (n=26) TENS (n=26). HOMA Index. ** 80 * 60. 40. 20. 0 Baseline. 30. 60. 90. 120. Minutes of general anesthesia. Figure 4. HOMA index represented insulin sensitivity of general anesthesia in a time course curve. TENS = 15 Hz, 10 mA TENS at bilateral Zusanli acupoints for 30 minutes in TENS group. Placebo = same conditions as TENS group without stimulation. * p 0.03, ** p < 0.02, *** p < 0.01.. 26.
(33) Photograph 1: The operating TENS stimulator: TENS at bilateral Zusanli acupoints and Sanyinjiao acupoint with continuous mode at the frequency of 15 Hz and the intensity of 10 mA synchronously for 30 minutes by HANS stimulator.. 27.
(34) Photograph 2: The connection of HANS stimulator between acupoints: By means of HANS stimulator, the positive (red) electrodes and the negative electrodes (black) were connected to bilateral Zusanli and Sanyinjiao acupoints respectively.. 28.
(35) Photograph 3: Lateral view of TENS at bilateral Zusanli acupoints and Sanyinjiao acupoints.. 29.
(36) Chapter 4. Discussion Our study is a pioneer in the investigation of a complementary non-pharmacologic treatment as an adjunct for lowering hyperglycemia during general anesthesia. The findings of this study suggest that TENS on Zusanli acupoints with the frequency of 15 Hz and the intensity of 10 mA has both effects of lowering plasma glucose and increasing insulin sensitivity. According to the theory of traditional Chinese medicine, acupuncture regulates “Chi” which runs through all the meridians of whole body.24, 35 Manipulation of a needle in an acupoint produces a slow increase of the skin pain threshold, which reaches the peak within 30 minutes, followed by an exponential decay after the removal of the needle.36 Furthermore, electrical stimulation via skin patch electrodes is as effective as electroacupuncture than manual acupuncture.36 Thus, we performed an interval of 30 minutes TENS stimulation in TENS group. However, we have not yet clarify the efficiency of lowering plasma glucose and improving insulin resistance at different frequencies and/or different intensities of TENS stimulation at the. 30.
(37) specific acupoints. In addition, the dense and disperse mode of action with alternating 2 and 100 Hz can be applied two different ways to produced a maximized analgesic effect in electroacupuncture practice.36 In our clinical investigation, we applied the continuous mode on bilateral Zusanli acupoints synchronously to determine the hypoglycemic effect and to improve insulin resistance by TENS. Previous animal studies showed that continuous mode of electroacupuncture with 15 Hz, 10 mA for 30 minutes was an effective method to decrease plasma glucose level and increase insulin sensitivity simultaneously.24 Thus, an interesting topic arose from further comparison of the effectiveness of lowering plasma glucose and increasing insulin sensitivity between electroacupuncture and TENS during general anesthesia. In the placebo group, both plasma glucose levels at 90 minutes and 120 minutes of general anesthesia, using sevoflurane, were statistically significantly higher than baseline level (p < 0.001). At the same time, the level of secretory endogenous insulin was elevated (Figure 3). All the above data indicates that insulin resistance increased as represented by a statistically elevation of HOMA index during general anesthesia. As another issue, IR results in a defined decreased physiological response, compared to the response for normal quality and quantity of. 31.
(38) insulin, as represented by the problem of glucose utilization in peripheral tissues such as muscle and adipose tissue. In addition, hyperglycemia, elevated free fatty acid, and IR are the main mechanisms involved in the accelerated atherosclerotic process and coronary artery disease observed in type II diabetes mellitus. Moreover, the elevated concentration of plasma free fatty acid that decreased IRS-1-associated phosphatidylinositol 3-kinase (PI 3-kinase) activity and inhibited of translocation of intracellular vesicles containing GLUT4 glucose transporter to the plasma membrane resulting in the diminution of glucose transport or phosphorylation activity in human skeletal muscle, is considered to be an important factor of increasing insulin resistance.37 Although TENS can lower HOMA index in our clinical study, we have found that there are no statistically significant difference in the plasma level of free fatty acid between TENS group and placebo group during this short period time of general anesthesia. Activating the peripheral -opioid receptor plays an important role for lowering plasma glucose and improving insulin resistance.25 However, opiates may have pharmacological central side effects or may lead to drug addiction. In an animal study, electroacupuncture is also an effective method to activate -endorphin that act on -opioid receptor to lower plasma. 32.
(39) glucose level and improve insulin sensitivity.24, 38-40 Additionally, different types of endogenous opioid peptide can be activated by different frequencies of electroacupuncture.36 The previous study showed 2 Hz electroacupuncture produced a 7-fold increase in met-enkephalin that acts on and opioid receptors while 100 Hz electroacupuncture produced a 2-fold increase in the release of dynorphin A that act on receptor.36 In a chart with a log scale, 15 Hz is in the middle point between 2 and 100 Hz, which can partially activate both sides.36 This is the best as it activates the release of enkephalin and -endorphin, mixed and opioid receptor agonists.36 Moreover, TENS is also as effective as electroacupuncture.23 However, electroacupuncture requires skill, needles may break, and it is not convenient to use electroacupuncture in a busy operation room. There is a limitation to clarify the mechanism of -endorphin involved in the hypoglycemic effect and IR improvement in clinical practice of anesthesiology. This is another issue for further investigation.. 33.
(40) Chapter 5. Conclusion We concluded that using the continuous mode with frequency of 15 Hz and intensity of 10 mA for 30 minutes synchronously on bilateral Zusanli acupoints made TENS a safe and reliable therapeutic procedure for lowering plasma glucose level, improving insulin resistance, and increasing hypoglycemic activity without any complications and adverse effects during general. anesthesia.. TENS. also. represents. a. cost-efficient,. operation-convenient, and efficacious treatment modality that could be readily applied to patients during general anesthesia. We suggest that TENS of the Zusanli acupoint can be used as a complementary method for controlling plasma glucose and improving IR perioperatively.. 34.
(41) Chapter 6. References 1. Kaye AD. Fluid and Electrolyte Physiology; In Ronald D. Miller editor: Anesthesia. Fifth ed. Philadelphia: Churchill Livingstone; 2000 volume I pp1596-1599. 2. Gavin LA. Management of diabetes mellitus during surgery. West J Med 1989;151:525-9. 3. Roizen MF. Anesthetic Implications of Concurrent Diseases; In Ronald D. Miller editor: Anesthesia. Fifth ed. Philadelphia: Churchill Livingstone; 2000 Volume I pp905-912. 4. Powers AC. Diabetes Mellitus;In Kasper, Braunwald, Fauci, Hauser, Longo, and Jameson editors: Harrison's Principles of Internal Medicine. NewYork: McGraw-Hill, 16 edition, 2005, Volume II, pp2152-2158. 5. Ahmed N. Advanced glycation endproducts--role in pathology of diabetic complications. Diabetes Res Clin Pract 2005;67:3-21. 6. Reissell E, Orko R, Maunuksela EL, Lindgren L. Predictability of difficult laryngoscopy in patients with long-term diabetes mellitus. Anaesthesia 1990;45:1024-7. 7. Eldridge AJ, Sear JW. Peri-operative management of diabetic patients. Any changes for the better since 1985? Anaesthesia 1996;51:45-51. 8. Gale EA, Kurtz AB, Tattersall RB. In search of the Somogyi effect. Lancet 1980;2:279-82. 9. Closing the gap: the problem of diabetes mellitus in the United States. The Carter Center of Emory University. Diabetes Care 1985;8:391-406. 10. Lu TH, Hsu PY, Anderson RN, Huang CN. Mortality and causes of death in a national sample of diabetic patients in Taiwan: response to Tseng. Diabetes Care 2005;28:1266-7; author reply 7-8. 11. Lu TH, Hsu PY, Bjorkenstam C, Anderson RN. Certifying diabetes-related cause-of-death: a comparison of inappropriate certification statements in Sweden, Taiwan and the USA. Diabetologia 2006;49:2878-81. 12. Tseng CH, Chong CK, Tseng CP, Cheng JC, Wong MK, Tai TY. Mortality, causes of death and associated risk factors in a cohort of diabetic patients after lower-extremity amputation: a 6.5-year follow-up study in Taiwan. Atherosclerosis 2008;197:111-7. 13. Cucchiaro G, Markowitz SD, Kaye R, Stanley CA, Watcha MF. Blood glucose control during selective arterial stimulation and venous sampling for localization of focal hyperinsulinism lesions in anesthetized children. 35.
(42) Anesth Analg 2004;99:1044-8, table of contents. 14. Zuurbier CJ, Keijzers PJ, Koeman A, Van Wezel HB, Hollmann MW. Anesthesia's effects on plasma glucose and insulin and cardiac hexokinase at similar hemodynamics and without major surgical stress in fed rats. Anesth Analg 2008;106:135-42, table of contents. 15. Desborough JP, Knowles MG, Hall GM. Effects of isoflurane-nitrous oxide anaesthesia on insulin secretion in female patients. Br J Anaesth 1998;80:250-2. 16. Ewart RB, Rusy BF, Bradford MW. Effects of enflurane on release of insulin by pancreatic islets in vitro. Anesth Analg 1981;60:878-84. 17. Saha JK, Xia J, Grondin JM, Engle SK, Jakubowski JA. Acute hyperglycemia induced by ketamine/xylazine anesthesia in rats: mechanisms and implications for preclinical models. Exp Biol Med (Maywood) 2005;230:777-84. 18. Lattermann R, Schricker T, Wachter U, Georgieff M, Goertz A. Understanding the mechanisms by which isoflurane modifies the hyperglycemic response to surgery. Anesth Analg 2001;93:121-7. 19. Brown ET, Umino Y, Loi T, Solessio E, Barlow R. Anesthesia can cause sustained hyperglycemia in C57/BL6J mice. Vis Neurosci 2005;22:615-8. 20. Nishiyama T, Yamashita K, Yokoyama T. Stress hormone changes in general anesthesia of long duration: isoflurane-nitrous oxide vs sevoflurane-nitrous oxide anesthesia. J Clin Anesth 2005;17:586-91. 21. Saho S, Kadota Y, Sameshima T, Miyao J, Tsurumaru T, Yoshimura N. The effects of sevoflurane anesthesia on insulin secretion and glucose metabolism in pigs. Anesth Analg 1997;84:1359-65. 22. Tanaka T, Nabatame H, Tanifuji Y. Insulin secretion and glucose utilization are impaired under general anesthesia with sevoflurane as well as isoflurane in a concentration-independent manner. J Anesth 2005;19:277-81. 23. Ulett GA, Han S, Han JS. Electroacupuncture: mechanisms and clinical application. Biol Psychiatry 1998;44:129-38. 24. Chang SL, Lin KJ, Lin RT, Hung PH, Lin JG, Cheng JT. Enhanced insulin sensitivity using electroacupuncture on bilateral Zusanli acupoints (ST 36) in rats. Life Sci 2006;79:967-71. 25. Tzeng TF, Lo CY, Cheng JT, Liu IM. Activation of mu-opioid receptors improves insulin sensitivity in obese Zucker rats. Life Sci 2007;80:1508-16. 36.
(43) 26. Han JS, Chen XH, Sun SL, Xu XJ, Hao JX, Terenius L. Effect of lowand high-frequency TENS on Met-enkephalin-Arg-Phe and dynorphin A immunoreactivity in human lumbar CSF. Pain 1991;47:295-8. 27. Chen L, Tang J, White PF, Naruse R, Kariger R. The effect of location of transcutaneous electrical nerve stimulation on postoperative opioid analgesic requirement: acupoint versus nonacupoint stimulation. Anesth Analg 1998;87:1129-34. 28. Ernst E, Pittler MH. The effectiveness of acupuncture in treating acute dental pain: a systematic review. Br Dent J 1998;184:443-7. 29. Chen L, Tang J, White PF, et al. The effect of location of transcutaneous electrical nerve stimulation on postoperative opioid analgesic requirement: acupoint versus nonacupoint stimulation. Anesth Analg 1998;87:1129-34. 30. Yan T, Hui-Chan CW. Transcutaneous electrical stimulation on acupuncture points improves muscle function in subjects after acute stroke: a randomized controlled trial. J Rehabil Med 2009;41:312-6. 31. White A. A cumulative review of the range and incidence of significant adverse events associated with acupuncture. Acupunct Med 2004;22:122-33. 32. Chang CS, Ko CW, Wu CY, Chen GH. Effect of electrical stimulation on acupuncture points in diabetic patients with gastric dysrhythmia: a pilot study. Digestion 2001;64:184-90. 33. Kim YS, Hong JW, Na BJ, Bae HS. The effect of low versus high frequency electrical acupoint stimulation on motor recovery after ischemic stroke by motor evoked potentials study. Am J Chin Med 2008;36:45-54. 34. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412-9. 35. Liao TJ, Urata S, Nishikawa H. Transient decrease in skin resistance response and level at the deh-chi stage caused by manual acupuncture. Tohoku J Exp Med 1998;186:19-25. 36. Han JS. Acupuncture and endorphins. Neurosci Lett 2004;361:258-61. 37. Dresner A, Laurent D, Marcucci M. Effects of free fatty acids on glucose transport and IRS-1-associated phosphatidylinositol 3-kinase activity. J Clin Invest 1999;103:253-9. 38. Chang SL, Lin JG, Chi TC, Liu IM, Cheng JT. An insulin-dependent 37.
(44) hypoglycaemia induced by electroacupuncture at the Zhongwan (CV12) acupoint in diabetic rats. Diabetologia 1999;42:250-5. 39. Lin JG, Chang SL, Cheng JT. Release of beta-endorphin from adrenal gland to lower plasma glucose by the electroacupuncture at Zhongwan acupoint in rats. Neurosci Lett 2002;326:17-20. 40. Lin JG, Chen WC, Hsieh CL, Chang SL. Multiple sources of endogenous opioid peptide involved in the hypoglycemic response to 15 Hz electroacupuncture at the Zhongwan acupoint in rats. Neurosci Lett 2004;366:39-42.. 38.
(45) 中文摘要 經皮神經電刺激(TENS)是一應用於輔助手術後疼痛控制已經有很長 的時間。然而,甚少對中醫的典型穴位上作 TENS 以達到降血糖效果和 改善胰島素阻抗的研究。因此,我們設計一單盲、隨機控制、臨床研究。 52 位女性病患,進行非緊急下腹腔手術。經簽署同意書後隨機分為二 組。TENS 組於全身麻醉誘導前,在兩側足三里穴位上施以同步連續模 式、頻率 15 Hz、強度 10 mA、TENS 刺激 30 分鐘。對照組在兩側足三 里穴位上貼電極片但不通電刺激。實驗結果顯示 TENS 組手術中在統計 學上(p < 0.05)有明顯降血糖效果及減少胰島素阻抗作用。因此,我們 建議在兩側足三里穴位上 TENS 刺激,可應用於輔助糖尿病病患在手術 週期中控制血糖、改善胰島素阻抗。 關鍵詞:經皮神經電刺激;足三里穴;血糖;胰島素阻抗. 39.
(46) Appendix I. 40.
(47) 41.
(48) Appendix II China Medical University and Asia University Joint Conference on BioTechnology Poster 評估麻醉插管前兩側足三里經皮電刺激之血壓控制效果 The Control of Blood Pressure by Transcutaneous Electrical Nerve Stimulation of Bilateral Zusanli Acupoints (ST36) before Endotracheal Intubation during General Anesthesia 文寄銘 Kee-Ming Man1,2,#、張世良 Shih-Liang Chang3、陳永祥 Yung-Hsiang Chan1、林維勇 Wei-Yong Lin1、張錦新 Kam-Sun Cheung2 、馬振來 Chun-Lai Ma2 、李昭德 Chao-Te Lee1、陳汶吉 Wen-Chi Chen1,* Mar 16 2009. 1Graduate Institute of Integrated Medicine, College of Chinese Medicine, China Medical University, Taichung;. 2Department of Anesthesiology, Tungs’ Taichung MetroHarbor Hospital, Taichung; 3Department of Medicinal. Botany and Healthcare, Dayeh University, Changhua, Taiwan. 42.
(49) Introduction Acupuncture and transcutaneous electrical nerve stimulation (TENS) have been used as a complementary management of pain relief postoperatively. However, there have been few clinical studies that investigate the effects of TENS in autonomic nerve systems on the specific acupoints during general anesthesia. Sympathetic nerve system stimulation accompanied with high blood pressure and the tachycardia have been noted during intubation of tracheal even with the standard dosage of intravenous anesthetics to induce general anesthesia. Materials and Methods We designed a single blind clinical study to investigate the effect of transcutaneous electrical nerve stimulation (TENS) of bilateral Zusanli acupoints (ST36) preoperatively to diminish the elevation of blood pressure and heart rate during endotracheal intubation. After we obtained written, informed consent, 52 ASA physical status I or II women scheduled for elective total abdominal hysterectomy or laparoscopic assisted virginal hysterectomy procedures with a standardized general anesthesia were randomly assigned to one of two groups. Placebo group: sham TENS (no. 43.
(50) electrical current) (n = 26) at the bilateral Zusanli (ST36) acupoints; TENS group (n = 26): the frequency of TENS was set in the continue mode of 15 Hz synchronously on the bilateral Zusanli acupoints for 30 minutes. The intensity of stimulation was set at 10 mA for patients in TENS group. The TENS stimulator (HAN LY257; Healthtronics, Singapore) was applied to each patients in TENS group before 30 minutes of the pre-induction of general anesthesia. Patients with a previous experience of acupuncture therapy, as well as those with clinically significant cardiovascular, pulmonary, renal, hepatic, and neurologic diseases were excluded from participating in this study. The induction of general anesthesia was performed with intravenous fentanyl 2 mL and thiopental 5 mg/kg. Tracheal intubation was facilitated with intravenous rocuronii 1 mg/kg within 30 seconds by the same experienced anesthesiologist. We monitored all the patients with the same Dash 5000 monitor (GE) and printed out all the values of systolic, diastolic blood pressure and heart rates before and after intubation immediately.. 44.
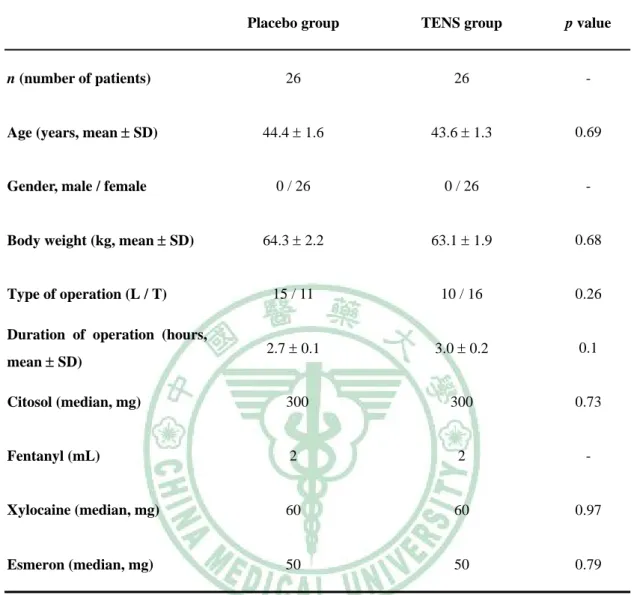
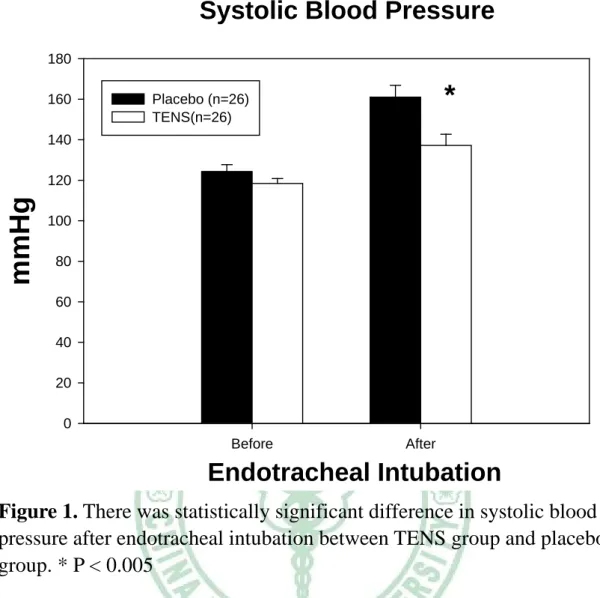
(51) Results These two groups were comparable with respect of both demographic and the dosage of intravenous anesthetics which had been given for the induction of general anesthesia. There were no statistically significant differences in the patients’ age, weight between these two groups of patients (Table 1). As the data showed, preoperative TENS of bilateral Zusanli acupoints diminished the elevation of blood pressure and heart rate during endotracheal intubation (p < 0.05 compared with the control group). Discussion This study shows the benefits of using a nonpharmacologic complimentary therapy to control blood pressure during endotracheal intubation. We do not know the mechanism between TENS and autonomic nerve system clearly. TENS application normalized the sympathovagal balance had been reported. In addition, the numbers of sample size must increase to a significant statistic to support our evidence-based clinical trial. When TENS was applied at the Zusanli acupoints, the immunoreactive metenkephalin-arg-phe was found increased in the lumbar cerebrospinal fluid in a human study, showed highly effective in relieving lower abdominal. 45.
(52) pain. Conclusion We concluded preoperative TENS on bilateral Zusanli acupoints offers an effective treatment in decreasing the elevation of blood pressure and heart rate in the period of endotracheal intubation during general anesthesia, but further study is necessary.. 46.
(53) Table 1. Demographic data and clinical variables for the placebo group and the TENS group Placebo group. TENS group. p value. n (number of patients). 26. 26. -. Age (years, mean SD). 44.4 1.6. 43.6 1.3. 0.69. 0 / 26. 0 / 26. -. 64.3 2.2. 63.1 1.9. 0.68. 15 / 11. 10 / 16. 0.26. 2.7 0.1. 3.0 0.2. 0.1. Citosol (median, mg). 300. 300. 0.73. Fentanyl (mL). 2. 2. -. Xylocaine (median, mg). 60. 60. 0.97. Esmeron (median, mg). 50. 50. 0.79. Gender, male / female Body weight (kg, mean SD). Type of operation (L / T) Duration of operation (hours, mean SD). The demographic data were compared by the Student’s t-test for all the patients. We used Chi-square test to analyze the type of operation. L = Laparoscopic assisted vaginal hysterectomy T = Total abdominal hysterectomy. 47.
(54) Systolic Blood Pressure 180 160. *. Placebo (n=26) TENS(n=26). 140. mmHg. 120 100 80 60 40 20 0 Before. After. Endotracheal Intubation Figure 1. There was statistically significant difference in systolic blood pressure after endotracheal intubation between TENS group and placebo group. * P < 0.005. 48.
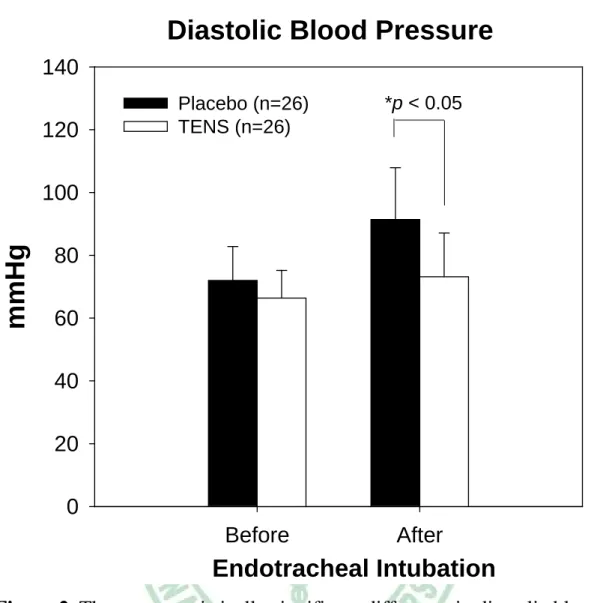
(55) Diastolic Blood Pressure 140 120. *p < 0.05. Placebo (n=26) TENS (n=26). mmHg. 100 80 60 40 20 0 Before. After. Endotracheal Intubation Figure 2. There was statistically significant difference in diastolic blood pressure after endotracheal intubation between TENS group and placebo group. * P < 0.05. 49.
(56) Heart Rate 120. Beats/min. 100. Placebo (n=26) TENS (n=26). 80. 60. 40. 20. 0 Before. After. Endotracheal Intubation Figure 3. The comparison of hear rate before and after endotracheal intubation between TENS group and placebo group. There have no statistically significant difference in elevation of heart rate after endotracheal intubation between these two groups.. 50.
(57)
數據

+7
Outline
相關文件
• The XYZ.com bonds are equivalent to a default-free zero-coupon bond with $X par value plus n written European puts on Merck at a strike price of $30. – By the
A function f is said to be continuous on an interval if it is continuous at each interior point of the interval and one-sidedly continuous at whatever endpoints the interval
A discussion of the Dapagli flozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) trial, the Effect of Sotagli flozin on Car- diovascular Events in Patients
• The XYZ.com bonds are equivalent to a default-free zero-coupon bond with $X par value plus n written European puts on Merck at a strike price of $30.. – By the
• The XYZ.com bonds are equivalent to a default-free zero-coupon bond with $X par value plus n written European puts on Merck at a strike price of $30.. – By the
• The XYZ.com bonds are equivalent to a default-free zero-coupon bond with $X par value plus n written European puts on Merck at a strike price of $30.. – By the
Then g is defined on [a, b], satifies (11), and is continuous on [a, b] by the Sequential Characterization of Limits.. Thus, f
• The XYZ.com bonds are equivalent to a default-free zero-coupon bond with $X par value plus n written European puts on Merck at a strike price of $30.. – By the
