Contribution of Double Strand Break Repair Gene XRCC3
Genotypes to Nasopharyngeal Carcinoma Risk in Taiwan
Juhn-Cherng Liu
1,2,*, Chia-Wen Tsai
1,2,*, Chin-Mu Hsu
2,*, Wen-Shin
Chang
1,2, Chi-Yuan Li
1, Shih-Ping Liu
2, Wu-Chung Shen
2and Da-Tian
Bau
1,2,3,*1 Graduate Institute of Clinical Medical Science, China Medical University, Taichung,
Taiwan, R.O.C.;
2 Terry Fox Cancer Research Laboratory, China Medical University Hospital, Taichung,
Taiwan, R.O.C.;
3 Graduate Institute of Basic Medical Science, China Medical University, Taichung, Taiwan,
R.O.C.
* These authors contributed equally to this study.
Reprints and correspondence to: Da-Tian Bau, Terry Fox Cancer Research Laboratory,
China Medical University Hospital, 2 Yuh-Der Road, Taichung, 40458 Taiwan, R.O.C. Tel. +886 422052121 Ext. 7534, e-mail: [email protected]; [email protected]
Abstract.
The DNA double strand break repair protein XRCC3 plays a central role in removing double strand breaks from the genome and defects in cellular repair capacity is closely related to human cancer initiation. Therefore, we aimed to investigate the contribution of XRCC3 genotypes to individual nasopharyngeal carcinoma (NPC) susceptibility. In this hospital-based population research, the genotyping and analyzing of XRCC3 rs1799794, rs45603942, rs861530, rs3212057, rs1799796, rs861539, rs28903081 in a large Taiwanese population was performed. Totally, 176 NPC patients and 880 age- and gender-matched healthy controls were genotyped and analyzed by PCR-RFLP method. The results showed that there was differential distribution among NPC and control subjects in the genotypic (P=0.000488) and allelic (P=0.0002) frequencies of XRCC3 rs861539. As for the gene-environment interaction, we have firstly provided evidence showing that there is an obvious joint effect of XRCC3 rs861539 CT and TT genotypes with individual smoking habits on increased NPC risk. In conclusion, the T allele of XRCC3 rs861539, interacts with smoking habit in increasing NPC risk, may be an early detection marker for NPC.
Introduction
Nasopharyngeal carcinoma (NPC) is rare cancer which happened in most countries around the world with an incidence rate generally less than 1 per 100,000 person-years. However, in record the NPC incidence is extremely high in Southern China (25-30 per 100,000 person-years) (4, 6, 40). In Taiwan the annual incidence rates for males and females were 8.41 and 2.93 per 100,000 person-years, respectively*. Compared with Western countries, the incidence rate is significantly higher in Taiwan with a very high genetic conservation. Thus, the genetic studies for Taiwanese are very useful, especially for NPC susceptibility evaluation. In addition to Epstein-Barr virus (EBV) infection (27, 42), certain dietary factors (18) and genetic differences such as single nucleotide polymorphisms (SNPs) which may all contribute to NPC carcinogenesis (28, 31, 32), environmental factors such as smoking, may also play a role in the etiology of NPC (5, 19, 36, 37).
Environmental carcinogens such as tobacco smoke may induce double strand breaks (DSBs) in the cells. DSBs are a very severe type of DNA damage which should be repaired by the DNA DSB repair system as soon as possible (35, 41). Tobacco smoking accounts for 5% of cancer cases overall in the world, and several lines of evidence have linked tobacco smoking to NPC risk including those from case-control studies conducted in China, the United States, Southeast Asia, Europe, Singapore, China (Guangdong), and Taiwan (31, 37). Mechanically, if cells cannot remove them immediately by means of homologous recombination (HR) and non-homologous end-joining (NHEJ), those DNA DSBs may induce precancerous lesions and cancer itself as well (21, 38). Genetic polymorphisms in DNA DSB repair genes influence DNA repair capacity and confer predisposition to several cancers
including skin (15), breast (1, 2), liver (17), gastric (11), and oral cancer (3, 10). The X-ray repair cross-complementing group 3 (XRCC3; 14q32.3) is a member of the rad51 DNA repair family, which has been shown to interact directly with rad51 and is essential with respect to the proper accumulation of rad51 at sites of DNA DSBs in the nucleus (29).
The most commonly studied XRCC3 genetic polymorphic site is the rs861539 C/T polymorphism (also named Thr241Met, T241M, C18067T and C722T). However up to now no finding of any XRCC3 SNP about NPC was reported. To identify the contribution of
XRCC3 genotyping to NPC risk in Taiwan, we determined the genotypic frequencies of seven
polymorphisms of XRCC3 gene at promoter A-315G (rs1799794), promoter C-280T (rs45603942), intron5 (rs861530), exon6 (rs3212057), intron7 (rs1799796), exon8 (rs861539) and exon10 (rs28903081), and evaluate the gene-environment interaction.
Materials and Methods
Study Population and Sample Collection
One hundred and seventy-six NPC patients were diagnosed and recruited at the outpatient clinics of general surgery between 2003-2009 at the China Medical University Hospital, Taichung, Taiwan. The clinical characteristics of patients including histological details were all graded and defined by expert surgeons. All patients voluntarily participated, completed a self-administered questionnaire and provided peripheral blood samples. At the same time 880 (five-fold of the cases) healthy volunteers as controls were selected by matching for age, gender and habits after initial random sampling from the Health Examination Cohort of the hospital. The exclusion criteria of the control group included previous malignancy, metastasized cancer from other or unknown origin, and any familial or genetic diseases. Both
groups completed a short questionnaire which included personal habits. Smokers were defined as daily or almost daily smokers who had smoked at least five packs of cigarettes in their lifetime. Smokers were recorded for their age of smoking initiation, whether they were currently smoking or had already quit, and if so, when they had quit, and on average, how many cigarettes they smoked or had smoked daily. As for the 880 non-cancer healthy people, the ratio of male versus female was both 75% versus 25% in each group. The mean age of the NPC patients and the controls were 48.2 (SD = 11.1) and 51.3 (SD = 8.8) years, respectively (see Table I for more details). Our continuous study was approved by the Institutional Review Board of the China Medical University Hospital and written-informed consents were obtained from all participants.
Genotyping Conditions
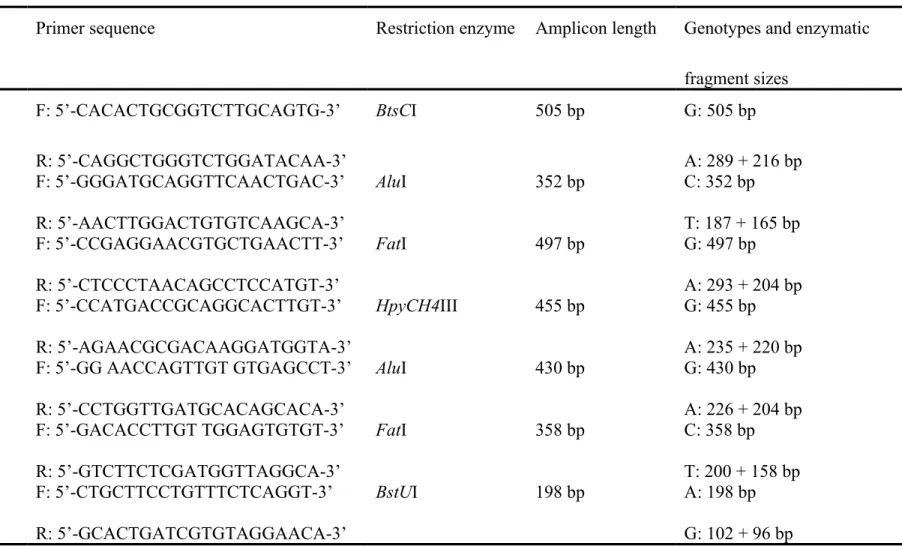
Genomic DNA was prepared from peripheral blood leucocytes using a QIAamp Blood Mini Kit (Blossom, Taipei, Taiwan) and kept as previous literature (9, 30). A total of seven polymorphic sites were analyzed in all the subjects in control and case groups. Briefly, all of the seven polymorphic sites were genotyped by means of a PCR-restriction fragment length polymorphism (PCR-RFLP), and further processed as previous genotyping publications (7, 8, 23). PCR was performed on BioRad’s Mycycler (BioRad, Hercules, CA, USA) following the normal manufacturer’s instructions. Each PCR reaction consisted of 5 min initial cycle at 94oC
for 5 min; 40 cycles of 94oC for 30 s, 55oC for 30 s, and 72oC for 30 s; and a final extension at
72oC for 10 min. Then the SNP-containing DNA amplicons were subjected to individual
overnight digestion by restriction endonucleases following the manufacturer’s instructions (see Table II for more details). Following digestion, each sample was immediately analyzed
by 2% agarose gel electrophoresis. Details such as the primer sequences, and enzymatic digestion conditions for each SNP analyzed in this study were summarized in Table II.
Statistical Analyses
The subjects matched with all SNPs data and clinical (case/control =176/880) were taken into final analyzing. To ensure that the controls used were representative of the general population and to exclude the possibility of genotyping error, the deviation of the genotype frequencies of
XRCC3 SNPs in the control subjects from those expected under the Hardy-Weinberg
equilibrium was assessed using the goodness-of-fit test. Pearson’s Chi-square test or Fisher’s exact test (when the expected number in any cell was less than five) was used to compare the distribution of the XRCC3 genotypes between cases and controls. Cancer risk associated with the genotypes was estimated as odds ratio (ORs) and 95% confidence intervals (CIs) using unconditional logistic regression. Data was recognized as significant when the statistical P-value was less than 0.05. All statistical tests were performed using SAS, Version 9.1.3 (SAS Institute Inc., Cary, NC, USA) on two-sided probabilities.
Results
The basic characteristics of recruited 176 NPC patients and 880 non-cancer controls are shown in Table I. Since the controls are age-, gender-matched with the cases, there was no significant difference between the two groups as in their age and gender (Table I). As for the individual habit status, there was a significant difference that the case group seemed to have more cigarette smokers (P=0.0001), but not alcohol drinkers or betel quid chewers (Table I). The frequency distributions of the genotypes for the seven XRCC3 polymorphic sites between
controls and NPC patients are shown in Table III. Among them, the genotypic distribution pattern of XRCC3 rs861539 was significantly different between NPC and control groups (P=0.000488), while those for rs1799794, rs45603942, rs861530, rs3212057, rs1799796 and rs28903081 were not significant (P>0.05) (Table III). In detail, distributions of XRCC3 rs861539 CC homozygote/heterozygote/TT homozygote in controls and oral cancer patients were 91.9/7.6/0.5% and 86.8/11.7/1.5%, respectively (Table III). The ORs for CT and TT genotypes versus CC wild-type were 1.85 (95%CI=1.10-3.09) and 5.47 (95%CI=1.74-17.18), respectively. There was no heterozygote or homozygote variant for XRCC3 rs3212057 and rs28903081 among Taiwanese subjects (Table III). To sum up, the genotype of XRCC3 rs861539, not rs1799794, rs45603942, rs861530, rs3212057, rs1799796 or rs28903081, is associated with NPC risk and may be a biomarker for the early detection and prediction of NPC.
The frequencies of the alleles for the XRCC3 rs1799794, rs45603942, rs861530, rs3212057, rs1799796, rs861539 and rs28903081 of all the recruited subjects are shown in Table IV. Among them, the carriers of XRCC3 rs861539 allele T were of higher risk for NPC (P=0.0002), while genotypes of XRCC3 rs1799794, rs45603942, rs861530, rs3212057, rs1799796 and rs28903081 were not associated with individual NPC susceptibility (Table IV).
In Taiwan, the habit of cigarette smoking is a risky factor for increased NPC risk. Therefore, the risk of NPC related to XRCC3 genotypes was further examined with stratification by personal smoking status. Table V showed the interaction of XRCC3 genotype and smoking status on personal NPC susceptibility (Table V). The results showed that compared with C/C
genotype, the C/T plus T/T significantly enhanced the risk only in the smoker group (P=0.0015, OR=3.30, 95%CI=1.63-6.69), not in the non-smoker group (P>0.05, OR=1.41, 95%CI=0.71-2.81) (Table V).
Discussion
In recent years, there were a few papers investigated the contribution of genetic variations on DSB repair genes to head and neck risk (3, 10, 12, 13, 16, 22, 24-26, 33, 34, 38, 39). However, those investigated the contribution of genetic variations on DSB repair genes to NPC risk were very few. The present study is to investigate the role of XRCC3 gene polymorphisms in NPC risk in Taiwan, where the NPC prevalence density in high due to an over-exposure to environmental factors such as betel quid, smoke and alcohol. Among these polymorphisms of
XRCC3 we investigated, the rs861539 located in the exon region and the T allele on it was
associated with increased NPC risk in Taiwan (Table III and IV), while the other polymorphisms were not associated. The rs861539 genetic variation direct results in an amino acid coding alteration from Thr to Met which may indicate XRCC3 rs861539 genetic polymorphism also result in functional alteration and predisposing to NPC cancer progression.
Physiologically speaking, the cells with risky TT or CT genotypes may of less DNA repair capacity than those with CC wild-type genotype. Exposed to the same dose of exogenous or endogenous DNA damage, these cells with risky genotypes would leave more DNA adducts induced by the DNA damaging agents in the genome of these people. Years by years, these
people with TT or CT genotypes at XRCC3 rs861539 would accumulated more genomic
instability and be attacked by all types of cancer. Thus, the effects of variant genotypes would be stronger in the smoker group than in the non-smoker group since the genome of smokers
are exposed to higher exogenous DNA damaging agents, especially those carcinogens in cigarette components (Table V).
In 2012, XRCC3 rs3212057 was reported to be associated with head and neck cancer in Poland (14). There were some groups reporting negative association between XRCC3 genotype and oral cancer in Brazil (12), Belgium (33), and India (24). Consistent with ours,
XRCC3 rs861539 was reported to be associated with oral cancer risk in Thailand. However the
sample size of the report was rather small with only 112 oral cancer cases and 119 controls (22).
The present study has several advantages. First is its large enough sample size. Although the case is limited to 176, we have recruited 5-fold (n=880) age- and gender-matched controls and the overall analyzing power is satisfying. Second, all the analysis without adjustment strengthen the accuracy and reliability of our findings. Third, the frequencies of XRCC3 polymorphisms variant alleles were similar to those reported in the NCBI website in the Asian population studies, for example the T minor allele frequencies of XRCC3 rs861539 is 4.4% (Table IV) in our 880 controls, a little smaller than 4.7 to 11.0% for Asian population recorded on NCBI website. In 2005, Jin and his colleagues9study reported that the T minor allele frequencies of XRCC3 rs861539 was 0.36% in 280 controls and 0.71% in 140 colorectal cancer patients in Taiwan (20). All of the above data suggested that no selection bias for the subject enrolments in our work, and the verifying of our findings in further larger studies is not so urgently necessary in the same issue. The paper has several disadvantages such as the limited sample size. Since NPC only was responsible for the prevalence of less than 1/100,000 per year all over the world and in Taiwan the annual incidence rates for males and females
were 8.41 and 2.93 per 100,000 person-years, it is not easily to collect a large sample size within a single hospital. To fulfill this, the authors boosted the analyzing power by increasing the number of control to 880, and the total sample size is up to more than 1,000 and very representative.
The Table I suggested that the cigarette smoking is a risky factor for NPC in Taiwan (Table I). Also, the results in this study have shown that there was positive interaction of variant DNA double strand break gene XRCC3 rs861539 genotypes with individual smoking habits in NPC risk (Table V). People with smoking habit and carrying the T allele of XRCC3 rs861539 have an increased risk of NPC among our stratified subgroups (Table V). These findings strengthened the theory of NPC carcinogenesis that genetic variants in DNA double strand break repairing system may enhance the genomic vulnerability to smoking-related DNA attacks, leading to NPC cancer progression.
To sum up, we found the genotype of XRCC3 rs861539, but not those of rs1799794, rs45603942, rs861530, rs3212057, rs1799796 or rs28903081, was associated with increased NPC risk. In addition, the elevated NPC risk by variant genotypes of XRCC3 rs861539 was more obviously enhanced among smokers, but not among none-smokers. Individual betel quid chewing and alcohol drinking habits could not enhance the risky genotype in increasing NPC susceptibility (data not shown). The Taiwanese are of conserved genetic background, combined Eastern-Western lifestyle and diet, and specific environmental risk factors, such as betel quid chewing for (oral) cancer progression. To realize the personalized medicine and therapy, the biomarkers for Taiwanese are in urgent need since NPC is much prevalent in
Taiwan and south Asia. Up to now, there is early screening methodology for oral cancer, colorectal cancer, breast cancer, hepatoma, but not NPC. The XRCC3 rs861539 CT or TT risk genotype found in this paper might serve as a useful biomarker for early detection and prediction of NPC in Taiwan.
Acknowledgements
We thank Tsai-Ping Ho, Chieh-Lun Hsiao, Tzu-Chia Wang, Yun-Ru Syu, Lin-Lin Hou, Chia-En Miao and Tissue-bank of China Medical University Hospital for technical assistance. This study was supported by research grants from Terry Fox Cancer Research Foundation of China Medical University and the National Science Council (NSC101-2320-B-039-045 and NSC102-2320-B-039-045).
References
1. Bau, D.T., Fu, Y.P., Chen, S.T., Cheng, T.C., Yu, J.C., Wu, P.E. and Shen, C.Y. Breast cancer risk and the DNA double-strand break joining capacity of nonhomologous end-joining genes are affected by BRCA1. Cancer Res. 64: 5013-5019, 2004.
2. Bau, D.T., Mau, Y.C., Ding, S.L., Wu, P.E. and Shen, C.Y. DNA double-strand break repair capacity and risk of breast cancer. Carcinogenesis 28: 1726-1730, 2007.
3. Bau, D.T., Tseng, H.C., Wang, C.H., Chiu, C.F., Hua, C.H., Wu, C.N., Liang, S.Y., Wang, C.L., Tsai, C.W. and Tsai, M.H. Oral cancer and genetic polymorphism of DNA double strand break gene Ku70 in Taiwan. Oral Oncol. 44: 1047-1051, 2008.
4. Cao, S.M., Simons, M.J. and Qian, C.N. The prevalence and prevention of nasopharyngeal carcinoma in China. Chin. J. Cancer 30: 114-119, 2011.
5. Cao, Y., Miao, X.P., Huang, M.Y., Deng, L., Liang, X.M., Lin, D.X., Zeng, Y.X. and Shao, J.Y. Polymorphisms of methylenetetrahydrofolate reductase are associated with a high risk of nasopharyngeal carcinoma in a smoking population from Southern China. Mol. Carcinog. 49: 928-934, 2010.
6. Chan, A.T., Teo, P.M. and Johnson, P.J. Nasopharyngeal carcinoma. Ann. Oncol. 13: 1007-1015, 2002.
7. Chang, C.H., Wu, H.C., Ke, H.L., Lin, H.H., Shen, W.C., Sun, S.S., Tsai, C.W., Tsai, R.Y. and Bau, D.T. The genetic role of cyclooxygenase 2 in ureter cancer in Taiwan. Adapt. Med. 3: 99-105, 2011.
8. Chang, W.S., Tsai, C.W., Cheng, K.H., Lien, C.S., Huang, C.P., Liao, W.L., Lee, M.H., Wu, H.C., Chang, C.H., Lin, C.C. and Bau, D.T. The Role of APEX1/Ref-1 (apurinic/apyrimidic endonuclease DNA-repair gene) in Renal Cell Carcinoma. Adapt. Med. 4: 216-223, 2012.
9. Chang, W.S., Yang, M.D., Tsai, C.W., Cheng, L.H., Jeng, L.B., Lo, W.C., Lin, C.H., Huang, C.Y. and Bau, D.T. Association of cyclooxygenase 2 single-nucleotide polymorphisms and hepatocellular carcinoma in Taiwan. Chin. J. Physiol. 55: 1-7, 2012.
10. Chiu, C.F., Tsai, M.H., Tseng, H.C., Wang, C.L., Wang, C.H., Wu, C.N., Lin, C.C. and Bau, D.T. A novel single nucleotide polymorphism in XRCC4 gene is associated with oral cancer susceptibility in Taiwanese patients. Oral. Oncol. 44: 898-902, 2008.
11. Chiu, C.F., Wang, C.H., Wang, C.L., Lin, C.C., Hsu, N.Y., Weng, J.R. and Bau, D.T. A novel single nucleotide polymorphism in XRCC4 gene is associated with gastric cancer susceptibility in Taiwan. Ann. Surg. Oncol. 15: 514-518, 2008.
12. Dos Reis, M.B., Losi-Guembarovski, R., de Souza Fonseca Ribeiro, E.M., Cavalli, I.J., Morita, M.C., Ramos, G.H., de Oliveira, B.V., Mizuno, L.T., Rogatto, S.R. and de Syllos Colus, I.M. Allelic variants of XRCC1 and XRCC3 repair genes and susceptibility of oral cancer in Brazilian patients. J. Oral Pathol. Med. 42: 180-185, 2013.
13. Gal, T.J., Huang, W.Y., Chen, C., Hayes, R.B. and Schwartz, S.M. DNA repair gene polymorphisms and risk of second primary neoplasms and mortality in oral cancer patients.
Laryngoscope 115: 2221-2231, 2005.
14. Gresner, P., Gromadzinska, J., Polanska, K., Twardowska, E., Jurewicz, J. and Wasowicz, W. Genetic variability of Xrcc3 and Rad51 modulates the risk of head and neck cancer. Gene 504: 166-174, 2012.
15. Han, J., Colditz, G.A., Samson, L.D. and Hunter, D.J. Polymorphisms in DNA double-strand break repair genes and skin cancer risk. Cancer Res. 64: 3009-3013, 2004.
16. Hsu, C.F., Tseng, H.C., Chiu, C.F., Liang, S.Y., Tsai, C.W., Tsai, M.H. and Bau, D.T. Association between DNA double strand break gene Ku80 polymorphisms and oral cancer susceptibility. Oral Oncol. 45: 789-793, 2009.
17. Hsu, C.M., Yang, M.D., Chang, W.S., Jeng, L.B., Lee, M.H., Lu, M.C., Chang, S.C., Tsai, C.W., Tsai, Y., Tsai, F.J. and Bau, D.T. The contribution of XRCC6/Ku70 to hepatocellular carcinoma in Taiwan. Anticancer Res. 33: 529-535, 2013.
18. Hsu, W.L., Pan, W.H., Chien, Y.C., Yu, K.J., Cheng, Y.J., Chen, J.Y., Liu, M.Y., Hsu, M.M., Lou, P.J., Chen, I.H., Yang, C.S., Hildesheim, A. and Chen, C.J. Lowered risk of nasopharyngeal carcinoma and intake of plant vitamin, fresh fish, green tea and coffee: a case-control study in Taiwan. PLoS One 7: e41779, 2012.
19. Ji, X., Zhang, W., Xie, C., Wang, B., Zhang, G. and Zhou, F. Nasopharyngeal carcinoma risk by histologic type in central China: impact of smoking, alcohol and family history. Int. J.
Cancer 129: 724-732, 2011.
20. Jin, M.J., Chen, K., Song, L., Fan, C.H., Chen, Q., Zhu, Y.M., Ma, X.Y. and Yao, K.Y. The association of the DNA repair gene XRCC3 Thr241Met polymorphism with susceptibility to colorectal cancer in a Chinese population. Cancer Genet. Cytogenet. 163: 38-43, 2005.
21. Khanna, K.K. and Jackson, S.P. DNA double-strand breaks: signaling, repair and the cancer connection. Nat. Genet. 27: 247-254, 2001.
22. Kietthubthew, S., Sriplung, H., Au, W.W. and Ishida, T. Polymorphism in DNA repair genes and oral squamous cell carcinoma in Thailand. Int. J. Hyg. Environ. Health 209: 21-29, 2006. 23. Lin, C.H., Ho, C.Y., Liu, C.S., Lin, W.Y., Li, C.I., Yang, C.W., Bau, D.T., Li, T.C. and Lin, C.C.
resistance index in taiwanese metabolic syndrome patients. Chin. J. Physiol. 55: 405-411, 2012.
24. Majumder, M., Sikdar, N., Paul, R.R. and Roy, B. Increased risk of oral leukoplakia and cancer among mixed tobacco users carrying XRCC1 variant haplotypes and cancer among smokers carrying two risk genotypes: one on each of two loci, GSTM3 and XRCC1 (Codon 280). Cancer Epidemiol. Biomarkers Prev. 14: 2106-2112, 2005.
25. Matullo, G., Dunning, A.M., Guarrera, S., Baynes, C., Polidoro, S., Garte, S., Autrup, H., Malaveille, C., Peluso, M., Airoldi, L., Veglia, F., Gormally, E., Hoek, G., Krzyzanowski, M., Overvad, K., Raaschou-Nielsen, O., Clavel-Chapelon, F., Linseisen, J., Boeing, H., Trichopoulou, A., Palli, D., Krogh, V., Tumino, R., Panico, S., Bueno-De-Mesquita, H.B., Peeters, P.H., Lund, E., Pera, G., Martinez, C., Dorronsoro, M., Barricarte, A., Tormo, M.J., Quiros, J.R., Day, N.E., Key, T.J., Saracci, R., Kaaks, R., Riboli, E. and Vineis, P. DNA repair polymorphisms and cancer risk in non-smokers in a cohort study. Carcinogenesis 27: 997-1007, 2006.
26. Mondal, P., Datta, S., Maiti, G.P., Baral, A., Jha, G.N., Panda, C.K., Chowdhury, S., Ghosh, S., Roy, B. and Roychoudhury, S. Comprehensive SNP scan of DNA repair and DNA damage response genes reveal multiple susceptibility loci conferring risk to tobacco associated leukoplakia and oral cancer. PLoS One 8: e56952, 2013.
27. Niedobitek, G., Hansmann, M.L., Herbst, H., Young, L.S., Dienemann, D., Hartmann, C.A., Finn, T., Pitteroff, S., Welt, A., Anagnostopoulos, I., Friedrich, R., Friedrich, H., Sam, C.K., Araujo, I., Rickinson , A.B., and Stein, H. Epstein-Barr virus and carcinomas: undifferentiated carcinomas but not squamous cell carcinomas of the nasopharynx are regularly associated with the virus. J. Pathol. 165: 17-24, 1991.
28. Shih, L.C., Tsai, C.W., Tsai, M.H., Tsou, Y.A., Chang, W.S., Li, F.J., Lee, M.H. and Bau, D.T. Association of cyclin D1 genotypes with nasopharyngeal carcinoma risk. Anticancer
Res. 32: 1093-1098, 2012.
29. Thacker, J. The RAD51 gene family, genetic instability and cancer. Cancer Lett. 219: 125-135, 2005.
30. Tsai, C.W., Ho, C.Y., Shih, L.C., Ying, T.H., Hsieh, Y.H., Chen, Y.C., Chang, W.S., Huang, C.Y., Pan, S.B., Shui, H.A., Chen, C.P., Wang, P.S. and Bau, D.T. The Joint Effect of hOGG1 Genotype and Smoking Habit on Endometriosis in Taiwan. Chin. J. Physiol. 56: 263-268, 2013.
31. Tsai, C.W., Tsai, M.H., Shih, L.C., Chang, W.S., Lin, C.C. and Bau, D.T. Association of interleukin-10 (IL10) promoter genotypes with nasopharyngeal carcinoma risk in Taiwan.
Anticancer Res. 33: 3391-3396, 2013.
32. Tsou, Y.A., Tsai, C.W., Tsai, M.H., Chang, W.S., Li, F.J., Liu, Y.F., Chiu, C.F., Lin, C.C. and Bau, D.T. Association of caveolin-1 genotypes with nasopharyngeal carcinoma susceptibility in Taiwan. Anticancer Res. 31: 3629-3632, 2011.
33. Werbrouck, J., De Ruyck, K., Duprez, F., Van Eijkeren, M., Rietzschel, E., Bekaert, S., Vral, A., De Neve, W. and Thierens, H. Single-nucleotide polymorphisms in DNA double-strand break repair genes: association with head and neck cancer and interaction with tobacco use and alcohol consumption. Mutat. Res. 656: 74-81, 2008.
34. Werbrouck, J., De Ruyck, K., Duprez, F., Veldeman, L., Claes, K., Van Eijkeren, M., Boterberg, T., Willems, P., Vral, A., De Neve, W. and Thierens, H. Acute normal tissue reactions in head-and-neck cancer patients treated with IMRT: influence of dose and
association with genetic polymorphisms in DNA DSB repair genes. Int. J. Radiat. Oncol.
Biol. Phys. 73: 1187-1195, 2009.
35. Wood, R.D., Mitchell, M., Sgouros, J. and Lindahl, T. Human DNA repair genes. Science 291: 1284-1289, 2001.
36. Xu, F.H., Xiong, D., Xu, Y.F., Cao, S.M., Xue, W.Q., Qin, H.D., Liu, W.S., Cao, J.Y., Zhang, Y., Feng, Q.S., Chen, L.Z., Li, M.Z., Liu, Z.W., Liu, Q., Hong, M.H., Shugart, Y.Y., Zeng, Y.X., Zeng, M.S. and Jia, W.H. An epidemiological and molecular study of the relationship between smoking, risk of nasopharyngeal carcinoma, and Epstein-Barr virus activation. J.
Natl. Cancer Inst. 104: 1396-1410, 2012.
37. Xue, W.Q., Qin, H.D., Ruan, H.L., Shugart, Y.Y. and Jia, W.H. Quantitative association of tobacco smoking with the risk of nasopharyngeal carcinoma: a comprehensive meta-analysis of studies conducted between 1979 and 2011. Am. J. Epidemiol. 178: 325-338, 2013.
38. Yang, H., Lippman, S.M., Huang, M., Jack Lee, J., Wang, W., Spitz, M.R. and Wu, X. Genetic polymorphisms in double-strand break DNA repair genes associated with risk of oral premalignant lesions. Eur. J. Cancer 44: 1603-1611, 2008.
39. Yen, C.Y., Liu, S.Y., Chen, C.H., Tseng, H.F., Chuang, L.Y., Yang, C.H., Lin, Y.C., Wen, C.H., Chiang, W.F., Ho, C.H., Chen, H.C., Wang, S.T., Lin, C.W. and Chang, H.W. Combinational polymorphisms of four DNA repair genes XRCC1, XRCC2, XRCC3, and XRCC4 and their association with oral cancer in Taiwan. J. Oral Pathol. Med. 37: 271-277, 2008.
40. Yu, M.C. and Yuan, J.M. Epidemiology of nasopharyngeal carcinoma. Semin. Cancer Biol. 12: 421-429, 2002.
41. Yu, Z., Chen, J., Ford, B.N., Brackley, M.E. and Glickman, B.W. Human DNA repair systems: an overview. Environ. Mol. Mutagen. 33: 3-20, 1999.
42. Zong, Y.S., Sham, J.S., Ng, M.H., Ou, X.T., Guo, Y.Q., Zheng, S.A., Liang, J.S. and Qiu, H. Immunoglobulin A against viral capsid antigen of Epstein-Barr virus and indirect mirror examination of the nasopharynx in the detection of asymptomatic nasopharyngeal carcinoma.
Table I. The demographic and clinical characteristics of nasopharyngeal carcinoma
patients and controls.
Characteristics Controls (n = 880) Patients (n = 176) P-Valuea
n % Mean (SD) n % Mean (SD) Age (y) 51.3 (8.8) 48.2 (11.1) 0.5104 Gender 0.5692 Male 660 75.0% 128 72.7% Female 220 25.0% 48 27.3% Indulgence Cigarette smoking 253 28.8% 77 43.8% 0.0001*
Betel quid chewing 238 27.0% 55 31.3% 0.2688
Alcohol drinking 331 37.6% 80 45.5% 0.0622
Table II. Summary of the rs numbers, primer sequences, restriction enzymes, amplicon lengths before and after
enzyme digestion, for the XRCC3
SNPs investigated in this study.XRCC3 SNP Primer sequence Restriction enzyme Amplicon length Genotypes and enzymatic
fragment sizes rs1799794 F: 5’-CACACTGCGGTCTTGCAGTG-3’ R: 5’-CAGGCTGGGTCTGGATACAA-3’ BtsCI 505 bp G: 505 bp A: 289 + 216 bp rs45603942 F: 5’-GGGATGCAGGTTCAACTGAC-3’ R: 5’-AACTTGGACTGTGTCAAGCA-3’ AluI 352 bp C: 352 bp T: 187 + 165 bp rs861530 F: 5’-CCGAGGAACGTGCTGAACTT-3’ R: 5’-CTCCCTAACAGCCTCCATGT-3’ FatI 497 bp G: 497 bp A: 293 + 204 bp rs3212057 F: 5’-CCATGACCGCAGGCACTTGT-3’ R: 5’-AGAACGCGACAAGGATGGTA-3’ HpyCH4III 455 bp G: 455 bp A: 235 + 220 bp rs1799796 F: 5’-GG AACCAGTTGT GTGAGCCT-3’ R: 5’-CCTGGTTGATGCACAGCACA-3’ AluI 430 bp G: 430 bp A: 226 + 204 bp rs861539 F: 5’-GACACCTTGT TGGAGTGTGT-3’ R: 5’-GTCTTCTCGATGGTTAGGCA-3’ FatI 358 bp C: 358 bp T: 200 + 158 bp rs28903081 F: 5’-CTGCTTCCTGTTTCTCAGGT-3’ R: 5’-GCACTGATCGTGTAGGAACA-3’ BstUI 198 bp A: 198 bp G: 102 + 96 bp
Table III. Distribution of XRCC3
genotypes among nasopharyngeal carcinoma patients and controlsGenotype Controls Patients P-valuea Odds ratio (95% CI)b
(n) % (n) % rs1799794 0.8838 GG 212 24.1% 44 25.0% 1.00 (Reference) AG 489 55.6% 99 56.3% 0.98 (0.66-1.44) AA 179 20.3% 33 18.7% 0.89 (0.54-1.45) rs45603942 0.7883 CC 818 93.0% 161 91.5% 1.00 (Reference) CT 54 6.1% 13 7.4% 1.22 (0.65-2.29) TT 8 0.9% 2 1.1% 1.27 (0.27-6.04) rs861530 0.7630 AA 264 30.0% 55 31.3% 1.00 (Reference) AG 477 54.2% 97 55.1% 0.98 (0.68-1.40) GG 139 15.8% 24 13.6% 0.83 (0.49-1.40) rs3212057 1.0000 GG 880 100.0% 176 100.0% 1.00 (Reference) AG 0 0.0% 0 0.0% AA 0 0.0% 0 0.0% rs1799796 0.8702 AA 399 45.3% 83 47.2% 1.00 (Reference) AG 435 49.5% 85 48.3% 0.94 (0.67-1.31) GG 46 5.2% 8 4.5% 0.84 (0.38-1.84) rs861539 0.000488* CC 809 91.9% 148 84.1% 1.00 (Reference) CT 65 7.4% 22 12.5% 1.85 (1.10-3.09)* TT 6 0.7% 6 3.4% 5.47 (1.74-17.18)* rs28903081 1.0000 GG 880 100.0% 176 100.0% 1.00 (Reference) AG 0 0.0% 0 0.0% AA 0 0.0% 0 0.0%
a P-value based on Chi-square test (Fisher’s Exact test when n<5). b CI: confidence interval;
Table IV. Distribution of XRCC3
alleles among nasopharyngeal carcinoma patients and controlsAllele Controls % Patients % P-valuea
rs1799794 0.6828 Allele G 913 51.9% 187 53.1% Allele A 847 48.1% 165 46.9% rs45603942 0.4627 Allele C 1690 96.0% 335 95.2% Allele T 70 4.0% 17 4.8% rs861530 0.5952 Allele A 1005 57.1% 207 58.8% Allele G 755 42.9% 145 41.2% rs1799796 0.6554 Allele A 1233 70.1% 251 71.3% Allele G 527 29.9% 101 28.7% rs861539 0.0002* Allele C 1683 95.6% 318 90.3% Allele T 77 4.4% 34 9.7%
a P based on Chi-square test.
Table V. Odds ratios for XRCC3
rs861539 genotype and nasopharyngeal carcinoma stratified by personal smoking statusGenotypes Non-smokers P-value OR (95% CI) a Smokers P-value OR (95% CI) a
Controls Patients Controls Patients
CC 576 88 0.3330 1.00 (Reference) 233 60 0.0015* 1.00 (Reference)
CT+TT 51 11 1.41 (0.71-2.81) 20 17 3.30 (1.63-6.69)*
Total 627 99 253 77
a OR: Odds ratio, CI: confidence interval; ORs were estimated with multivariate logistic regression analysis.