行政院國家科學委員會專題研究計畫 期中進度報告
胰島素抗阻與胖素在多囊性卵巢囊腫症候群致病機轉上的
角色(2/3)
期中進度報告(精簡版)
計 畫 類 別 : 個別型
計 畫 編 號 : NSC 95-2314-B-002-035-
執 行 期 間 : 95 年 08 月 01 日至 96 年 07 月 31 日
執 行 單 位 : 國立臺灣大學醫學院婦產科
計 畫 主 持 人 : 楊友仕
處 理 方 式 : 期中報告不提供公開查詢
中 華 民 國 96 年 05 月 21 日
行政院國家科學委員會補助專題研究計畫
□期中進 度 報 告(
胰島素抗阻與胖素在多囊性卵巢囊腫症候群致病
機轉上的角色(2/3)
)
計畫類別:□ 個別型計畫
□ 整合型計畫
計畫編號:NSC 95-2314-B-002-035-
執行期間:
2006 年 8 月 1 日至
2007 年 7 月 31 日
計畫主持人:楊友仕
共同主持人:陳美州
計畫參與人員: 黃惠玲
成果報告類型(依經費核定清單規定繳交):□精簡報告 □完整
報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究
計畫、列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公
開查詢
執行單位:台大醫院婦產部
中
華
民
國
96 年
5 月
21 日
Relationship between Androgen Levels and Blood Pressure in Young Women with Polycystic Ovary Syndrome
Mei-Jou Chen, M.D.,a,c Wei-Shiung Yang, M.D., Ph.D.,b,c,dJehn-HsiahnYang, M.D.,aChi-Ling Chen, Ph.D.,cHong-Nerng Ho, M.D.,aand Yu-Shih Yang, M.D., Ph.D.a
a
Departments of Obstetrics and Gynecology andbInternal Medicine, National Taiwan University Hospital,cGraduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, anddInstitute of Biomedical Science, Academia Sinica, Taipei, Taiwan.
Corresponding author and reprint requests: Yu-Shih Yang, M.D., Ph.D. Department of Obstetrics and Gynecology, National Taiwan University Hospital, No. 7 Chung-Shan South Road, 100, Taipei, Taiwan
TEL: +886-2-2356-5159; FAX: +886-2-2341-8557 E-mail: [email protected]
Running title: Testosterone and blood pressure in PCOS Word count of manuscript: 4610
Word count of abstract: 255 Total number of figures: 2
*此部分研究成果已經被 Hypertension 接受,預
計 6 月出版
Abstract
The role of testosterone on the development of hypertension is controversial, especially in women with polycystic ovary syndrome (PCOS) who have higher prevalence of obesity and insulin resistance than women without PCOS. Little is known about the association between serum testosterone level and blood pressure in young women with PCOS. In the 151 young Taiwanese women with PCOS enrolled in this cross-sectional study, we measured the body mass index (BMI), waist circumference, blood pressure, fasting glucose, fasting insulin, lipid profile, and hormone profiles. The free androgen index (FAI), total testosterone, and sex hormone binding globulin (SHBG), but not the level of
dehydroepiandrosterone sulfate, significantly correlated with both systolic blood pressure (SBP) and diastolic blood pressure (DBP). In multiple linear regression models adjusted for age, BMI, and other anthropometric, metabolic, and hormonal variables, the level of serum FAI or total testosterone, but not the SHBG, were independently related to SBP and DBP. The age- and BMI-adjusted least square mean of serum FAI levels were significantly different between the highest quartile and other quartiles of the SBP and DBP levels. The high bioavailable testosterone levels (FAI ≥19%) in PCOS women increased therisk ofelevated blood pressure(SBP ≥ 130 mmHg and/orDBP ≥ 85 mmHg)with an oddsratio of 3.817 (P = 0.029; 95% confidence interval = 1.14-12.74) after adjustment for age, anthropometric measures, and metabolic profiles. Our results suggest that the characteristic hyperandrogenemia in young PCOS women was associated with an elevated SBP and DBP independent of age, insulin resistance, obesity, or dyslipidemia.
Key terms: Polycystic ovary syndrome, testosterone, systolic blood pressure, diastolic blood pressure, hypertension
Introduction
Women with polycystic ovary syndrome (PCOS) are characterized by clinical and/or biochemical hyperandrogenism, oligomenorrhea, and the presence of polycystic ovaries.1 PCOS is a heterogenous medical condition. Since large individual variation is present with respect to hyperandrogenism in terms of clinical manifestations and biochemistry, not all women with PCOS have elevated testosterone levels. Indeed, some women with PCOS without elevated testosterone levels may have acne, hirsutism, and/or androgenic alopecia that may arise as a result of the elevated androgens secreted by adipose tissue and the adrenal glands rather than the testosterone secreted from the ovaries.
Although the increased risk of atherosclerotic cardiovascular disease and hypertension in women with PCOS remains controversial,2, 3a variety of intriguing metabolic disturbances related to the risk for cardiovascular disease and hypertension are commonly found in a large proportion of women with PCOS, such as obesity, insulin resistance, dyslipidemia, and the metabolic syndrome.4 Women with PCOS have been reported to have reduced vascular compliance,5vascular endothelial dysfunction,6and a higher mean arterial blood pressure7in comparison to women without PCOS. Furthermore, the degree of impairment in vascular compliance and endothelial function, as well as the increased blood pressure, persists after adjusting for obesity and insulin resistance.5-7 Therefore, it is reasonable to speculate that the increased cardiovascular risk and hypertension in women with PCOS may be partially attributed to the characteristic state of hyperandrogenism.
Although there is little evidence to substantiate the association between hyperandrogenism and cardiovascular events,3, 8the role of gender differences in hypertension has been well-reviewed.9, 10 Blood pressure is higher in males than age-adjusted pre-menopausal women, beginning as early as puberty and persisting for life.10, 11In male rats, hypertension can be prevented by orchitectomy and can be reproduced by treatment with testosterone in castrated males or females,9suggesting the essential role of testosterone in blood pressure regulation. On the other hand, this facilitated effect of
testosterone on hypertension is not supported by several epidemiological studies performed in elderly men12and post-menopausal women.8 The age- and gender-specific effects may conceivably overshadow the effects of testosterone on hypertension.11
In the current study, we investigated the role of testosterone as a possible determining factor, other than obesity and other known metabolic risk factors, in affecting the blood pressure of young women with PCOS.
Material and Methods Subjects
One hundred fifty-one females with PCOS were included in this study. They had not been prescribed any medication prior to enrollment and were presented to our reproductive endocrinology clinic with a chief complaint of irregular menstrual cycles and/or clinical hyperandrogenism. The study was approved by the Institutional Review Board of the National Taiwan University Hospital and informed consent was obtained from all patients and/or their parents. We defined the clinical diagnosis of diabetes mellitus as a fasting plasma glucose≥ 126 mg/dL and an elevated blood pressureasa systolicblood pressure(SBP)≥ 130 mmHg and/oradiastolicblood pressure(DBP)≥ 85 mmHg.The diagnosis of PCOS was made when at least include 2 of the following 3 criteria existed, as proposed at the Rotterdam Consensus Meeting: oligomenorrhea or amenorrhea, clinical hyperandrogenism and/or hyperandrogenemia, and polycystic ovaries. Women with clinical hyperandrogenism, but without hyperandrogenemia, and either oligomenorrhea or polycystic ovaries, were not enrolled in this study. Oligomenorrhea was defined as less than eight spontaneous menstrual cycles per year in the three years prior to enrollment. Hyperandrogenemia was defined as a serum total testosterone level > 0.8 ng/mL, with or without persistent acne, hirsutism (i.e., a Ferriman-Gallwey score > 8), and androgenic alopecia. The criteria for polycystic ovaries required visualization of at least 12 follicles, 2-9 mm in diameter, per ovary by transvaginal ultrasonography or an ovarian volume exceeding 10 cm3by transabdominal ultrasonography with a distended bladder for virginal women. Exclusion criteria included:
hyperprolactinemia,thyroid dysfunction,Cushing’ssyndrome,congenitaladrenalhyperplasia,adrenal tumors, ovarian tumors, current or previous pregnancy within one year of enrollment, autoimmune disease, malignancy, central nervous system disease, current or previous use of oral contraceptives within six months of enrollment, or use of medications known to have an effect on the
hypothalamic-pituitary-ovarian axis, such as antiandrogens, ovulation induction agents, antidiabetic medications, antiobesity medications, or glucocorticoids. All subjects were non-smokers and did not consume alcoholic beverages on a regular basis. No subjects in the study had restricted physical activity due to handicap or other reasons, and no subjects were encouraged to exercise or engaged in work requiring physical labor.
Data collection
Blood samples were collected from females with spontaneous menstrual cycles between the third and seventh day of a spontaneous menstrual cycle, and between 0800 and 1000 after an overnight fast. For those subjects in whom amenorrhea exceeded three months, blood samples were collected without hormone-induced withdrawal bleeding, based on the results of pelvic sonography and a serum
progesterone level. Specifically, if a dominant follicle was present and the serum estradiol level exceeded 150 pg/mL, or the serum progesterone was greater than 2 ng/mL, the blood sample was discarded. The subject was then asked to measure her basal body temperature and a blood sample was collected during the next cycle following the menstruation after spontaneous ovulation. Blood was processed within 30 minutes of collection. Blood glucose and insulin sampleswerestored at4˚C and
analyzed the day of sampling. Serum and plasma were aliquoted and frozen at -70˚C untilassayed. Anthropometric measurements, pelvic sonography, and the measurement of blood pressure were done on the day of, and before, venipuncture. For those women who were unable to undergo transvaginal sonography, venipuncture was performed before transabdominal sonography. Blood pressure was measured by the same trained physician using a standard mercury sphygmomanometer with an appropriate cuff size. Measurements were made on the right arm of the subjects while in a seated position and after a resting period of > 30 minutes. Two readings were taken at 5 minute intervals and the results were averaged.12, 13If the first blood pressure measurement differed significantly from the second blood pressure measurement (> 10 mmHg systolic and/or diastolic), we then measured the blood pressure a third time after an additional 5 minutes rest and recorded the second and third blood pressure measurements as the result in an effort to reduce the so-called “white-coat effect.”Except for body weight and waist circumference, the blood pressure observer was blind to other measurements and the hypothesis. The body mass index (BMI) was calculated as the weight in kg divided by the height in m2.
Assay methods
The concentration of plasma glucose and the serum levels of low density lipoprotein-cholesterol (LDL-C), high density lipoprotein-cholesterol (HDL-C), triglycerides, and insulin were measured as previously described.14 The homeostasis model assessment was applied to estimate the degree of insulin resistance [HOMA-IR = (glucose × 0.05551) × insulin / 22.5], where insulin is expressed in μU/mL and glucoseisexpressed in mg/dL.Serum hormoneprofilessuch asFSH,LH,estradiol, progesterone, and serum hormone binding globulin (SHBG), were measured as previously described.14 Serum total testosterone and dehydroepiandrosterone sulfate (DHEA-S) were measured by
radioimmunoassay (RIA; Diagnostic Systems Laboratories, Webster, TX, USA). The free androgen index (FAI)15was calculated according to the equation, FAI (%) = testosterone (ng/mL) × 3.47 × 100 / SHBG (nmol/L). The intraassay and interassay coefficients of variation of the aforementioned assays were all < 10%.
Statistical analyses
The numeric variables are presented as the untransformed mean ± SD, unless indicated otherwise. The Shapiro-Wilk W test was used to identify whether all the variables were normally distributed or not. Log transformation was performed on variables with significant deviation from a normal distribution before further analysis. Pearson correlation coefficients were calculated to determine the correlations between the clinical characteristics and SBP or DBP. Multiple linear regression models were performed using SBP or DBP as the dependent variable, and anthropometric, metabolic, and hormonal factors as the independent variables. In these models, BMI or waist circumference was chosen to represent weight and HOMA-IR was selected to represent fasting glucose and insulin, to avoid collinearity. Logistic regression analysis was performed to assess the association between elevated blood pressure and the categorical data of the FAI (with a cutoff value at 19%, the highest quartile of FAI in this study) after adjustment for age, anthropometric measures, and metabolic factors. The least square (LS) means
of the FAI levels were calculated after adjustment for age and BMI among the subjects in different SBP and DBP quartiles by using ANOVA. A P value < 0.05 was considered statistically significant. All statistical analyses were performed using the PC version of the Statistical Analysis System (SAS, edition 9.1, SAS Institute Inc., Cary, NC, USA).
Results
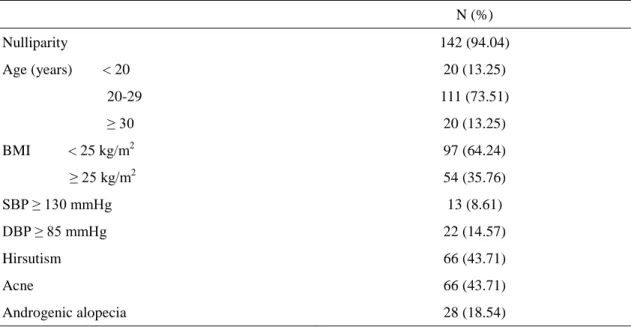
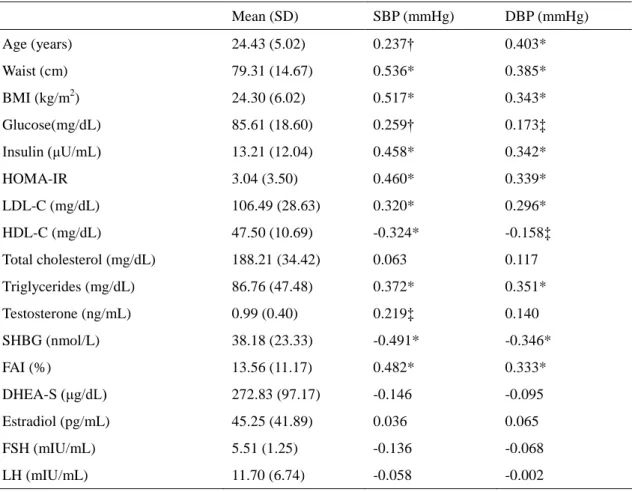
The clinical features of the subjects are summarized in Table 1. The majority of the subjects were young (87% of the subjects were < 30 years of age, with a mean age of 24.43 ± 5.02 years and a range of 14-37 years) and 94% were nulligravidas. There were only five subjects who met the diagnostic criteria for diabetes mellitus. As expected, the blood pressures, both SBP and DBP, significantly correlated with most metabolic variables related to the metabolic syndrome and insulin resistance (Table 2). The SBP and DBP positively correlated with age, waist circumference, BMI, HOMA-IR, fasting insulin, fasting glucose, LDL-C, triglycerides, and the FAI (Table2, Figure 1). The SBP and DBP negatively correlated with HDL-C and SHBG. No association existed between blood pressure and the hormonal profile, total cholesterol, or DHEA-S (Table 2).
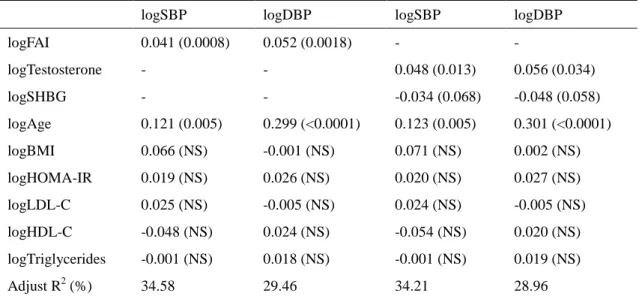
Based on multiple linear regression analyses, the SBP and DBP were significantly related to the FAI (P = 0.0008 and P = 0.0018, respectively) as well as age (P = 0.005 and P < 0.0001, respectively) after adjustment for BMI, HOMA-IR, LDL-C, HDL-C, and triglycerides (Table 3). No parameters were shown to have modifying effect on the FAI in the models tested. When waist circumference was used instead of BMI in the same multi-variables analyses as indicated in Table 3, the SBP and DBP were still significantly related to theFAI(β = 0.040, P = 0.001 and β = 0.048, P = 0.004, respectively). To evaluate the impact of total testosterone and the SHBG level on blood pressure in place of the FAI, we used SBP or DBP as the dependent variable, and the total testosterone level, SHBG, age, BMI, HOMA-IR, LDL-C, HDL-C, and triglycerides as independent variables for multivariate analysis. Serum total testosterone levels remained independently and positively associated with SBP (P = 0.013) and DBP (P = 0.034) after adjustment for SHBG, age, BMI, HOMA-IR, LDL-C, HDL-C, and
triglycerides (Table 3).
The age- and BMI-adjusted LS means of the FAI level among the subjects categorized according to SBP or DBP quartiles are shown in Figure 2. The age- and BMI-adjusted LS means of the FAIlevelsofwomen with PCOS in thehighestSBP quartile(SBP ≥ 119 mmHg)were significantly higher than the FAI levels of women that in the lowest and the second lowest SBP quartiles (P = 0.019 and P = 0.0006, respectively; Figure 2A). The age- and BMI-adjusted LS means of the FAI levels of women with PCOS in the highest DBP quartile were also significantly higher than the FAI levels of women in the lowest and the third DBP quartiles (P = 0.017 and P = 0.007, respectively; Figure 2B). It is noteworthy that the serum FAI level had a positive association with the SBP and DBP levels after adjustment for age and obesity. Utilizing logistic regression analysis with an adjustment for age, BMI, HOMA-IR, HDL-C, LDL-C,and triglyceridelevels,thehigh bioavailableandrogen level(i.e.,aFAI≥ 19%)wasassociated with ahigherprobability ofan elevated blood pressure(i.e.,aSBP ≥ 130 mmHg and/oraDBP ≥ 85 mmHg),with an oddsratio of3.817 (95% confidence interval = 1.14, 12.74; P = 0.029). If waist circumference was used instead of BMI in the model with the same adjustments, the high androgen level was still significantly associated with the occurrence of elevated blood pressure with an odds ratio of 3.758 (95% confidence interval = 1.08-13.14; P = 0.038).
Discussion
The effects of androgen on blood pressure are controversial.3, 11-13, 16 Because elevated androgens, such as DHEAS and testosterone (free and total), have been reported to associate with insulin resistance,17obesity,18and lipid metabolism,19therefore elevated androgens may raise the risk for cardiovascular disease. The present study demonstrated that the serum bioavailable and total testosterone levels were significantly and positively correlated with both SBP and DBP in young women with PCOS, independent of insulin resistance, obesity, and dyslipidemia. The observed associations in this specific population suggest that the characteristic hyperandrogenemia in young women with PCOS is associated with the level of the blood pressure and may possibly contribute to the risks of hypertension and cardiovascular disease that may occur in middle age.
The mechanisms by which androgens initiate and/or mediate cardiovascular disease and hypertension have not been clearly elucidated. In all major genetically hypertensive rat models, blood pressure has been reported to be higher in male than in female rats of similar ages.9, 11 Removal of the gonads reduces blood pressure in both genetic and non-genetic hypertensive male rats, but not in females, and the administration of testosterone increases the blood pressure in both genders.20, 21 Testosterone replacement can restore and increase the blood pressure, plasma renin, and renal and hepatic angiotensinogen, in both male and female gonadectomized rats.20 A recent study utilizing in
vivo microperfusion reported that androgen may directly upregulate the proximal tubule
renin-angiotensin system and increase the volume reabsorptive rate, thereby increasing extracellular volume and blood pressure.22 In humans, endothelial dysfunction has been reported to be associated not only with insulin resistance, but also with elevated free testosterone levels in post-menopausal women.6 In addition, serum androgen concentrations were reported to be an important predictor of blood pressure in young healthy women without PCOS.13
Contrariwise, there are some studies that have led investigators to presume that androgens may not be responsible for initiating and/or mediating cardiovascular disease and hypertension. For example, epidemiologic studies have demonstrated an inverse association between blood pressure and
testosterone in elderly men.12, 23Several studies involving post-menopausal populations suggested that circulating endogenous testosterone levels did not correlate with peripheral arterial disease and cardiovascular events.8, 24 In addition, iatrogenic hyperandrogenism in female-to-male transsexuals did not result in increased hypertensive morbidity.16 Such observations may be due to the
overshadowing effect of aging since testosterone levels decline with age.25, 26 It is also possible that the downregulation of androgen synthesis is a protective compensatory mechanism that occurs once the disease processes are initiated.21
A decline in testosterone levels with increasing age has been reported in pre-menopausal women and the testosterone levels in women in their fifth decade of life are approximately 50% of those in women in their third decade.25, 26 This phenomenon, the decline in testosterone with aging, was also reported specifically in women with PCOS.27 In addition, the source of androgen also changes with age. Peripheral conversion and adrenal gland production, instead of gonadal synthesis, is the main
source of circulating testosterone after menopause and oophorectomy.25 In fact, we found a significant and independent correlation between SBP and DBP and circulating testosterone levels in PCOS women at a young age, consistent with reports in other young healthy women without PCOS.13 A prospective, longitudinal study will be necessary to clarify whether the high circulating testosterone levels in women with PCOS at a young age actually contribute to hypertension later in life.
Asian women with PCOS have been reported to be less obese and have less apparent
hyperandrogenic phenotypes than women of other ethnicities, but the prevalence of androgen excess, insulin resistance, and polycystic ovaries appears to be similar in comparison with other populations.28 Since the phenotype of clinical hyperandrogenism is not distinct in our population and the diagnosis is very subjective, we chose more strict criteria for the definition of hyperandrogenism in our study. Therefore, it may be possible to restrict the applicability for the generalized PCOS in this study.
Additionally, it was difficult to collect an adequate non-biased representative control group in our study, therefore, we could not show if the association between androgen and blood pressure was specific for women with PCOS per se. However, a previous study13demonstrated this association in young women without PCOS. Since the young women with PCOS in this study were less obese than most PCOS study populations,4, 6, 29the importance of androgens rather than insulin resistance in our multiple linear regression models may emerge. Nevertheless, it should also be noted that our study did not identify a relationship between testosterone and either an increased incidence of hypertension, defined as a blood pressure > 140/90 mmHg, or an increased incidence of cardiovascular disease. In addition, this study did not prove the cause-and-effect relationship between testosterone and blood pressure and the relationship observed in these females with PCOS may not apply to males.
Perspectives
Our results are consistent with the hypothesis that elevated testosterone levels at a young age in women with PCOS is correlated with SBP and DBP independent of age, insulin resistance, obesity, and dyslipidemia. These findings suggest that in order to prevent the future onset of cardiovascular disease and hypertension, control of the metabolic variables in women with PCOS, as well as their
hyperandrogenism, might be considered. Further longitudinal follow-up research is needed to elucidate how the extent and the duration of testosterone exposure may impact the incidence of hypertension and cardiovascular disease in women with PCOS.
Sources of Founding
This study was supported by grants NSC94-2314-B002-195 and NSC95-2314-B002-035 from the National Science Council of Taiwan.
References
1. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004; 19:41-47.
2. Wild RA. Long-term health consequences of PCOS. Hum Reprod Update. 2002; 8:231-241. 3. Legro RS. Polycystic ovary syndrome and cardiovascular disease: a premature association?
Endocr Rev. 2003; 24:302-312.
4. Ehrmann DA, Liljenquist DR, Kasza K, Azziz R, Legro RS, Ghazzi MN. Prevalence and predictors of the metabolic syndrome in women with polycystic ovary syndrome. J Clin
Endocrinol Metab. 2006; 91:48-53.
5. Kelly CJ, Speirs A, Gould GW, Petrie JR, Lyall H, Connell JM. Altered vascular function in young women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2002; 87:742-746. 6. Paradisi G, Steinberg HO, Hempfling A, Cronin J, Hook G, Shepard MK, Baron AD.
Polycystic ovary syndrome is associated with endothelial dysfunction. Circulation. 2001; 103:1410-1415.
7. Holte J, Gennarelli G, Berne C, Bergh T, Lithell H. Elevated ambulatory day-time blood pressure in women with polycystic ovary syndrome: a sign of a pre-hypertensive state? Hum
Reprod. 1996; 11:23-28.
8. Barrett-Connor E, Goodman-Gruen D. Prospective study of endogenous sex hormones and fatal cardiovascular disease in postmenopausal women. BMJ. 1995; 311:1193-1196. 9. Reckelhoff JF. Gender differences in the regulation of blood pressure. Hypertension. 2001;
37:1199-1208.
10. Dubey RK, Oparil S, Imthurn B, Jackson EK. Sex hormones and hypertension. Cardiovasc
Res. 2002; 53:688-708.
11. Liu PY, Death AK, Handelsman DJ. Androgens and cardiovascular disease. Endocr Rev. 2003; 24:313-340.
12. Fogari R, Preti P, Zoppi A, Fogari E, Rinaldi A, Corradi L, Mugellini A. Serum testosterone levels and arterial blood pressure in the elderly. Hypertens Res. 2005; 28:625-630.
13. Mantzoros CS, Georgiadis EI, Young R, Evagelopoulou C, Khoury S, Katsilambros N, Sowers JR. Relative androgenicity, blood pressure levels, and cardiovascular risk factors in young healthy women. Am J Hypertens. 1995; 8:606-614.
14. Chen MJ, Yang WS, Yang JH, Hsiao CK, Yang YS, Ho HN. Low sex hormone-binding globulin is associated with low high-density lipoprotein cholesterol and metabolic syndrome in women with PCOS. Hum Reprod. 2006; 21:2266-2271.
15. Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab. 1999; 84:3666-3672. 16. van Kesteren PJ, Asscheman H, Megens JA, Gooren LJ. Mortality and morbidity in
transsexual subjects treated with cross-sex hormones. Clin Endocrinol (Oxf). 1997; 47:337-342.
17. Doi SA, Al-Zaid M, Towers PA, Scott CJ, Al-Shoumer KA. Steroidogenic alterations and adrenal androgen excess in PCOS. Steroids. 2006; 71:751-759
18. Pasquali R. Obesity and androgens: facts and perspectives. Fertil Steril. 2006; 85:1319-1340. 19. Moverare-Skrtic S, Venken K, Andersson N, Lindberg MK, Svensson J, Swanson C,
Vanderschueren D, Oscarsson J, Gustafsson JA, Ohlsson C. Dihydrotestosterone treatment results in obesity and altered lipid metabolism in orchidectomized mice. Obesity (Silver
Spring). 2006; 14:662-672.
20. Chen YF, Naftilan AJ, Oparil S. Androgen-dependent angiotensinogen and renin messenger RNA expression in hypertensive rats. Hypertension. 1992; 19:456-463.
21. Reckelhoff JF. Sex steroids, cardiovascular disease, and hypertension: unanswered questions and some speculations. Hypertension. 2005; 45:170-174.
22. Quan A, Chakravarty S, Chen JK, Chen JC, Loleh S, Saini N, Harris RC, Capdevila J, Quigley R. Androgens augment proximal tubule transport. Am J Physiol Renal Physiol. 2004;
287:F452-459.
23. Hak AE, Witteman JC, de Jong FH, Geerlings MI, Hofman A, Pols HA. Low levels of
endogenous androgens increase the risk of atherosclerosis in elderly men: the Rotterdam study.
J Clin Endocrinol Metab. 2002; 87:3632-3639.
24. Price JF, Lee AJ, Fowkes FG. Steroid sex hormones and peripheral arterial disease in the Edinburgh Artery Study. Steroids. 1997; 62:789-794.
25. Davis SR, Burger HG. Clinical review 82: Androgens and the postmenopausal woman. J Clin
Endocrinol Metab. 1996; 81:2759-2763.
26. Zumoff B, Strain GW, Miller LK, Rosner W. Twenty-four-hour mean plasma testosterone concentration declines with age in normal premenopausal women. J Clin Endocrinol Metab. 1995; 80:1429-1430.
27. Winters SJ, Talbott E, Guzick DS, Zborowski J, McHugh KP. Serum testosterone levels decrease in middle age in women with the polycystic ovary syndrome. Fertil Steril. 2000; 73:724-729.
28. Carmina E, Koyama T, Chang L, Stanczyk FZ, Lobo RA. Does ethnicity influence the prevalence of adrenal hyperandrogenism and insulin resistance in polycystic ovary syndrome?
Am J Obstet Gynecol. 1992; 167:1807-1812.
29. Orio F, Jr., Palomba S, Spinelli L, Cascella T, Tauchmanova L, Zullo F, Lombardi G, Colao A. The cardiovascular risk of young women with polycystic ovary syndrome: an observational, analytical, prospective case-control study. J Clin Endocrinol Metab. 2004; 89:3696-3701.
Figure Legend Figure 1:
Correlation between serum FAI levels and SBP (A), and DBP (B). Unadjusted Pearson correlation coefficients are shown.
Figure 2:
A: The serum free androgen index (FAI) levels (LS mean ± SE) after adjustment for age and body mass index (BMI) among the PCOS women in different SBP quartiles. *** P=0.019; ** P=0.0006; and *
P=0.084 by ANOVA. The SBP quartiles were as follows: 1) < 103 mmHg, 2) 103-108 mmHg, 3)
109-118 mmHg,and 4)≥ 119 mmHg.B:Theageand BMIadjusted FAIlevels(LS mean ± SE)in different DBP quartiles. ## P=0.017 and # P=0.007 by ANOVA. The DBP quartiles were as follows: 1) < 65 mmHg, 2) 65-70 mmHg, 3) 71-76 mmHg,and 4)≥ 77 mmHg.
Table 1. Basic demographic data of 151 women with PCOS. N (%) Nulliparity 142 (94.04) Age (years) < 20 20 (13.25) 20-29 111 (73.51) ≥ 30 20 (13.25) BMI < 25 kg/m2 97 (64.24) ≥ 25 kg/m2 54 (35.76) SBP ≥ 130 mmHg 13 (8.61) DBP ≥ 85 mmHg 22 (14.57) Hirsutism 66 (43.71) Acne 66 (43.71) Androgenic alopecia 28 (18.54)
Table 2. Basic characteristics of subjects and the Pearson correlation coefficient between blood pressure, anthropometric, hormonal, and metabolic variables.
Mean (SD) SBP (mmHg) DBP (mmHg) Age (years) 24.43 (5.02) 0.237† 0.403* Waist (cm) 79.31 (14.67) 0.536* 0.385* BMI (kg/m2) 24.30 (6.02) 0.517* 0.343* Glucose(mg/dL) 85.61 (18.60) 0.259† 0.173‡ Insulin (μU/mL) 13.21 (12.04) 0.458* 0.342* HOMA-IR 3.04 (3.50) 0.460* 0.339* LDL-C (mg/dL) 106.49 (28.63) 0.320* 0.296* HDL-C (mg/dL) 47.50 (10.69) -0.324* -0.158‡ Total cholesterol (mg/dL) 188.21 (34.42) 0.063 0.117 Triglycerides (mg/dL) 86.76 (47.48) 0.372* 0.351* Testosterone (ng/mL) 0.99 (0.40) 0.219‡ 0.140 SHBG (nmol/L) 38.18 (23.33) -0.491* -0.346* FAI (%) 13.56 (11.17) 0.482* 0.333* DHEA-S (μg/dL) 272.83 (97.17) -0.146 -0.095 Estradiol (pg/mL) 45.25 (41.89) 0.036 0.065 FSH (mIU/mL) 5.51 (1.25) -0.136 -0.068 LH (mIU/mL) 11.70 (6.74) -0.058 -0.002 *P <0.0001,†P <0.005,‡P <0.05.
BMI = body mass index; HOMA-IR = homeostasis model assessment of insulin resistance; LDL-C= low density lipoprotein cholesterol; HDL-C= high density lipoprotein cholesterol; DHEA-S = dehydroepiandrosterone sulfate; FAI = free androgen index; SBP = systolic blood pressure; DBP = diastolic blood pressure; E2 = estradiol; FSH = follicle stimulating hormone; LH = luteinizing hormone. Conversion factors:glucose(mg/dL)=18 × (mmol/L);insulin (μU/mL)× 7.175 = (pmol/L);
triglycerides (mg/dL) = 88.6 × (mmol/L); testosterone (ng/mL) × 3.47 = (nmol/L); DHEA-S (μg/dL )× 27.1 = (nmol/L); SHBG (nmol/L)× 0.095 = (μg/mL);fortotalcholesterol,HDL-C, and LDL-C (mg/dL) = 40 × (mmol/L).
Table 3. Multivariate analysis for the association between SBP and DBP with FAI or total testosterone. logSBP logDBP logSBP logDBP
logFAI 0.041 (0.0008) 0.052 (0.0018) - -logTestosterone - - 0.048 (0.013) 0.056 (0.034) logSHBG - - -0.034 (0.068) -0.048 (0.058) logAge 0.121 (0.005) 0.299 (<0.0001) 0.123 (0.005) 0.301 (<0.0001) logBMI 0.066 (NS) -0.001 (NS) 0.071 (NS) 0.002 (NS) logHOMA-IR 0.019 (NS) 0.026 (NS) 0.020 (NS) 0.027 (NS) logLDL-C 0.025 (NS) -0.005 (NS) 0.024 (NS) -0.005 (NS) logHDL-C -0.048 (NS) 0.024 (NS) -0.054 (NS) 0.020 (NS) logTriglycerides -0.001 (NS) 0.018 (NS) -0.001 (NS) 0.019 (NS) Adjust R2(%) 34.58 29.46 34.21 28.96 Values are expressed asregression coefficient(β);P values are indicated in parentheses; NS, Not