Title: An instrument to evaluate patient counseling provision on herbs and dietary supplements
Authors: Hsiang-Wen Lin, Ph.D.a,b,c A. Simon Pickard, Ph.D.c,d,e Gail B. Mahady, Ph.D.d,f George Karabatsos, Ph.D.g Stephanie Y. Crawford, Ph.D.c Nicholas G. Popovich, Ph.D.c
a. School of Pharmacy and Graduate Institute, China Medical University (CMU), Taichung, Taiwan, ROC
b.Department of Pharmacy, CMU Hospital, Taichung, Taiwan, ROC
c. Department of Pharmacy Administration, College of Pharmacy, University of Illinois at Chicago (UIC)
d.Department of Pharmacy Practice, College of Pharmacy, UIC
e. Center for Pharmacoeconomic Research, College of Pharmacy, UIC
f. UIC/NIH Center for Botanical Dietary Supplements Research, College of Pharmacy, UIC
g.Department of Educational Psychology, UIC
Hsiang-Wen (Margaret) Lin, Ph.D. (corresponding author) Assistant Professor, Graduate Institute and School of Pharmacy College of Pharmacy, China Medical University
[email protected], [email protected] No. 91 Hsueh-Shih road, Taichung, Taiwan 40402, R.O.C. Tel: 886-4-22053366 ext 5151
Keywords: patient counseling, instrument, herbal and dietary supplements, pharmacist,
student
Acknowledgements:
The authors express their gratitude to Robert Bennett, Carla Denise Clemmons, Maria Charisse De Leon Santos, John Hessian, Illinois Pharmacists Association executive staff, Swu-Jane Lin, Alexandra Perez, Vikrant Vats, Caitlyn Wilke, Robert Wittenberg,
Margareta S. Zwolenik, and the study participants.
These results were presented at 2008 Annual Meeting of American Association of College of Pharmacy during July 19-23, 2008 at Sheraton hotel, Chicago, IL Chicago, and 2008 Annual Meeting of Taiwan Society of Health-System Pharmacists, on November 11, 2008 at Taipei, Taiwan.
At the time of this study, Dr. Hsiang-Wen Lin was a doctoral candidate in the Department of Pharmacy Administration (PMAD), College of Pharmacy, at the University of Illinois at Chicago (UIC). Currently, she is an assistant professor in School of Pharmacy and Graduate Institute, China Medical University, and adjunct assistant professor in the PMAD, UIC.
Abstract: (135 words)
Objective: To develop a measure of pharmacists’ provision of herbs and dietary
supplements (HDS)-related patient counseling.
Design: A systematic process for item generation, testing, and validation of a measure
was employed. Because the pharmacist-patient encounter may involve a potential indication for HDS that does not necessarily result in the recommendation of an HDS product and vice versa, the instrument was bifurcated into two distinct components: (1) patient counseling in general (PC-G); and (2) HDS-related counseling (PC-HDS).
Assessment: The instrument demonstrated high reliability and desirable construct
validity. After adjusting for item difficulty, it appeared that participant pharmacists tended to provided more counseling related to the PC-G than on the PC-HDS.
Conclusion: This instrument can be applied to assess the quality of counseling provided
by pharmacists and pharmacy students, and the outcomes of educational outreach on HDS.
INTRODUCTION (word count: 2862)
Use of herbs and dietary supplements (HDS) has been on the rise in the United States.1,2 Compared to prescription and nonprescription drugs, HDS products have less stringent regulations and looser manufacturing oversight in the U.S.3 and are readily available at many retail outlets, including community pharmacies, grocery stores, health food stores, as well as on the Internet. Consumers often obtain information on HDS from their family, friends, magazines, books, or infomercials 4,5 rather than from healthcare professionals. Because the evidence on HDS products is often lacking or conflicting, it can be a challenge for healthcare professionals to make informed and consistent recommendations of HDS to their patients using evidenced-based approaches.6
An estimated 16 to 42% of patients used prescription drugs concomitantly with HDS,7-9 and 22 to 50% of patients took HDS products prior to surgeries and/or during preoperative care.10-12 The extensive use of HDS among higher-risk patients poses a potential safety concern that could be mitigated by pharmacist counseling on the appropriate use of HDS products. Pharmacists have been encouraged to integrate professional HDS counseling and education services into their daily practice,13,14 yet counseling services on the appropriate use of HDS from pharmacists are often
lacking.15-20 Possible explanations for insufficient counseling on HDS by pharmacists include an insufficient education and knowledge on HDS, unfavorable attitude towards HDS products, a limited evidence-base in the literature on HDS, and a lack of time dedicated to patient counseling.
been expressed by pharmacy educators, individual pharmacists, pharmacy managers, patients and other health professionals.14-15,22 The educational provisions associated with HDS toward pharmacy students in schools and pharmacy practitioners through postgraduate continuing education programs is not commensurate with the widespread use of HDS in the United States. As of 2005, some colleges/schools of pharmacy still did not offer course instruction in natural products or herbal supplements.14,16,23-26 Shah and colleagues (2005) recommended the establishment of guidelines for curricular content on herbal supplements in pharmacy education,24 and revised Accreditation Council for Pharmacy Education (ACPE) guidelines for evaluating and improving pharmacy curricula include topics regarding knowledge and expected competencies on complementary and alternative medicine, including HDS.27 A systematic review reported a majority of practicing pharmacists perceived they were not satisfactorily educated about herbal products and other types of alternative medicines during pharmacy school.28
Several instruments that assess patient counseling related to medication-related issues are available, with varying evidence to support the validity of the scales. 29-32 The focus of these instruments is on the performance of medication-related counseling or on counseling for specific self-care products. Of these studies, few describe a conceptual framework to guide instrument development and item generation, or they generate a checklist rather than an instrument with a meaningful metric.
The aim of this study is to describe the development of an instrument that assesses the extent to which HDS-related counseling activities are performed by pharmacists. This study was part of a broader study included in the development and implementation
of knowledge, attitude, and behavior (KAB) surveys to gather information, describe current practice, and potentially assess the effects of initiatives to refine the practice, education, and training of pharmacists with respect to HDS.
METHODS
Instrument development
The goal of the instrument was to quantify the provision of HDS-related patient counseling by pharmacists. Specifically, the performance of HDS patient counseling was the construct of interest, whereby “patient counseling” was defined as an individualized counseling process when the pharmacist helps the patient treat his/her HDS-related problems through providing appropriate guidance using a problem-solving approach.33 Upon conducting a literature review, several relevant measures were identified: Kemper’s communication practice scale,30 USP Medication Counseling Behavior Guideline29,34 and other measures.31-32 Upon further evaluation, these instruments did not satisfy our measurement goals. Specifically, the pharmacist-patient encounter may begin with an HDS inquiry but may not result in an HDS-related recommendation, and vice versa. As a consequence, the performance of drug/HDS counseling was
conceptualized as two measures: a general patient counseling [PC-G] measure and a HDS-specific counseling [PC-HDS] measure.
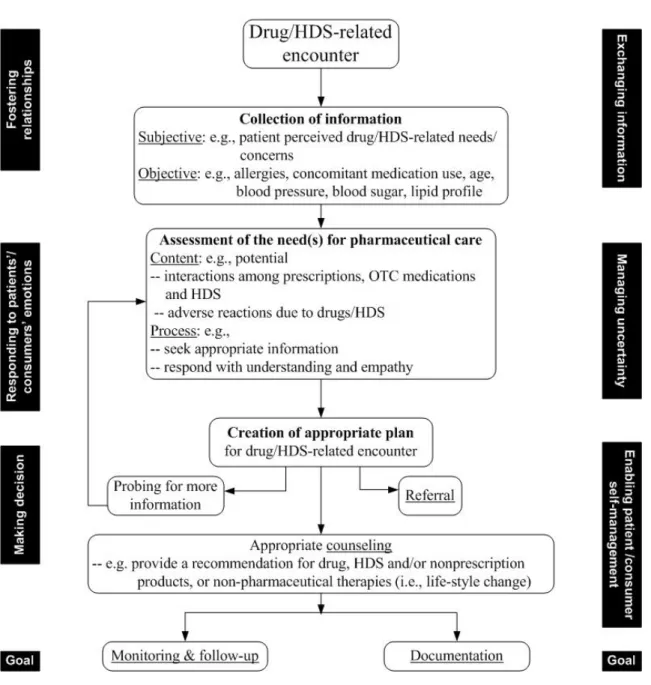
When considering HDS for an individual patient, the American Dietetic Association /American Pharmacists Association recommends health professionals use the SOAP format (i.e., Subjective, Objective, Assessment, Plan).35,36 This approach was followed in conceptualizing the patient-pharmacist consultation process37 for a drug/HDS-related
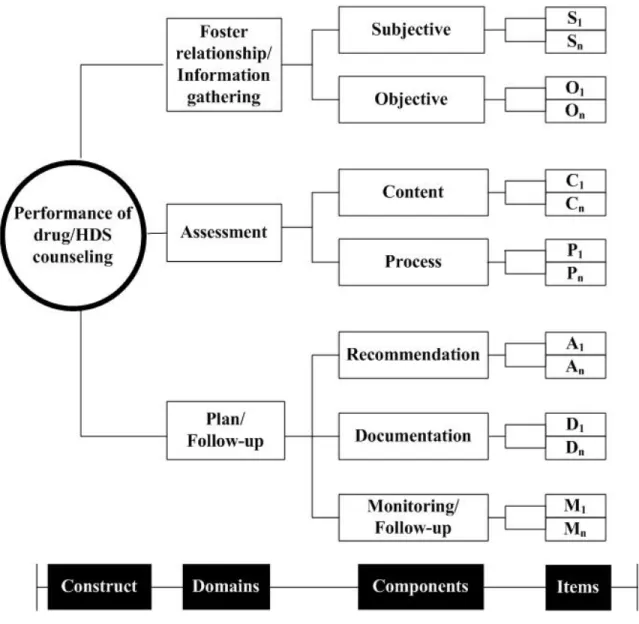
encounter (Figure 1). The counseling process includes six factors that characterize effective patient-centered communication (e.g., fostering relationships, exchanging information, responding to patients’/consumers’ emotions, managing uncertainty, making a decision, enabling patient/consumer self-management).38. When operationalized, the construct was conceptualized as having three main domains (i.e., foster
relationships/information gathering, assessment, and plan/follow-up), each with 2-3 components (Figure 2). Items were generated by the authors and from existing literature and measures.31-33, 36, 39-45
Instrument refinement and validation
Item pools were created with a sufficient number of items covering a broad
spectrum of pharmacists’ provision of HDS-related counseling. Once the item pool was generated, internal expert panel discussions were conducted to identify irrelevant,
redundant items, and items with bias towards different characteristic of respondents. Two lay persons without a pharmacy background reviewed the structure and wording of the instrument as a final check. An external reviewer accessed the created web-based survey draft and provided suggestions on each item and the survey administration process.
Item performance assessment
Each item on the pharmacists’ HDS counseling measure used a five-point
Likert-type scale labeled as “none of the time,” “a little of the time,” “some of the time,” “most of the time,” and “all of the time.” Proportion scores were derived by dividing the maximum obtainable total scores into the total observed scores, where the expected
total score was equal to the number of items multiplied by 5 (five-point Likert type scale). The higher the score, the more frequently a pharmacist performed patient counseling tasks related to HDS.
The properties of each measure were evaluated using kernel regression-based nonparametric item response theory (KIRT) models46-47 to examine the properties of each measure (i.e., testing of items with monotonic response pattern, variant item ordering, sufficient number of functional category responses) along with classical test theory based approaches (i.e., internal consistency [Cronbach’s α], exploratory factor analysis
[EFA]).48 Items with poor psychometric properties were revised for content and/or eliminated, resulting in a final set of items related to each patient counseling instrument. At least two strata of difficulty (i.e., participant ability strata) were deemed necessary for the measure to have a sufficient span of ability to interpret the construct defined by the items.49 Only items contributing to an acceptable level of reliability (i.e.,α ≥ 0.7) were retained.50
Subject recruitment
Practicing pharmacists with various levels of HDS knowledge and practice
behaviors were asked to complete the instrument so the appropriateness and difficulty of items could be examined in the pilot study. In a subsequent larger scale validation study, pharmacists who were employed in healthcare settings and had regular patient contact were recruited. The studies were approved by the Institutional Review Board of the University of Illinois at Chicago (Protocol # 2007-0505).
Data analysis
The proportion score and the logit score for the two measures (PC-G and PC-HDS), were compared using an independent t test, or if not appropriate, the Mann-Whitney test, based on the results obtained from one sample Kolmogorov-Smironov test.51
Differences in participant characteristics across two administration stages of the study (i.e., pilot, large-scale) were examined using t tests to identify differential item
functioning (DIF). 95% confidence intervals were computed by employing the
bootstrap method.52 Person measure scores (i.e., in logit units) obtained in the validation study were used when conducting bivariate analyses, i.e., Pearson correlations. The corresponding nonparametric analyses were performed whenever the parametric assumption of normality was violated. These approaches were performed to examine the association between background information (e.g., including personal, workplace information, HDS information/ training resources) and logit scores of pharmacists’ performance of HDS-related patient counseling, respectively. A significance level of α < 0.05 was set a priori. All analyses were performed using SPSS 16.0 version and in using “R” software.
RESULTS
Of the 34 pilot study participants, 20 (58.8%) completed the KAB survey instrument in its entirety, whereas 179/330 participants (54.4%) completed the revised survey
instrument administered in the larger scale validation study.
Of 46 items constructed in the initial item pool, 17 items were revised and retained for the patient counseling - general measure (PC-G). Eleven items were generated for the measure of performance patient counseling on HDS (Table 1). The proportion of items measuring each component of patient counseling in the general construct (PC-G) was similar to the initial item pool. However, no items were retained which measured pharmacists’ tasks related to gathering subjective or objective information from patients within the HDS counseling construct (PC-HDS).
Instrument Validation
Table 2 and Table 3 present the psychometric properties of the two measures. Prior to refinement in the pilot study, the Cronbach’s α of PC-G was 0.91 (95% interval= 0.84, 0.95) for the 17-item measure. With the removal of poorly performing items, the
reliability of 10-item version was reduced to 0.86 (0.71, 0.93). In the larger validation study with sufficient sample size to apply the EFA, two factors were extracted for general counseling. Consequently, five items (i.e., PC-G2, PC-G4, PC-G5, PC-G7 and PC-G14) loaded on one factor (named as information gathering) and another five items (PC-G6, PC-G9, PC-G10, PC-G12, PC-G13) loaded onto a second factor (named as facilitating decision making). The two factors were strongly correlated (rf-f = 0.68), which inferred these items might account for only one construct. While the PC-G possessed a fairly good level of reliability, two items (PC-G2 and PC-G9) did not demonstrate monotonicity. Upon removal of these items, the eight remaining items were able to distinguish at least three groups of respondents’ performance behavior (participant strata = 3.09). The internal consistency of the PC-G was acceptable (α = 0.81).
study after removing four items. Two items related to the tasks of subjective
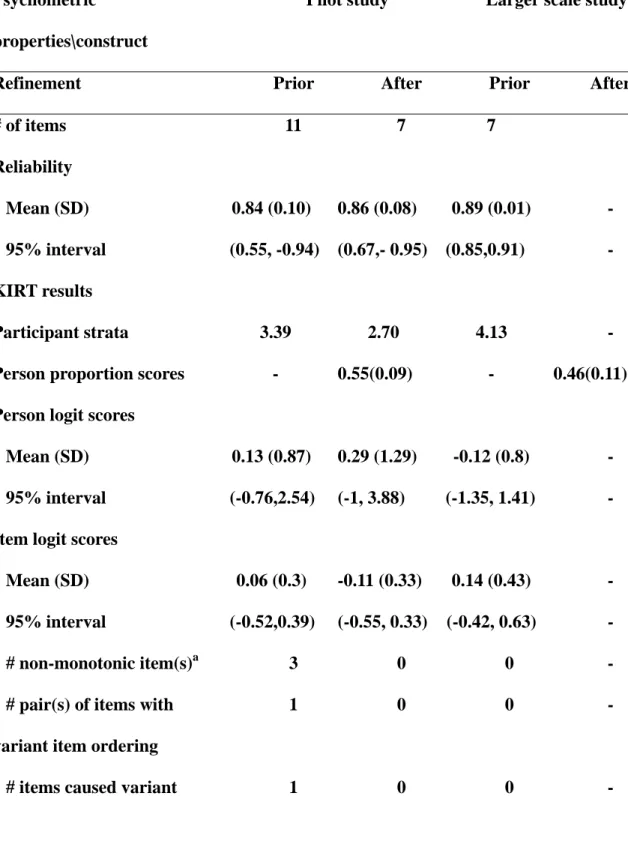
information gathering and recommendations were removed from the PC-HDS. In the larger validation study, the remaining seven items possessed a good level of reliability (α = 0.89 [SD = 0.01]) and satisfied other psychometric criteria, and were able to stratify HDS patient counseling into more than 4 ability groups (participant strata = 4.13). Upon the EFA, two items indicating the monitoring (i.e., PC-HDS10, PC-HDS11) were loaded in one stand alone factor and the remaining five items (i.e., PC-HDS1, PC-HDS3, PC-HDS6, PC-HDS7, PC-HDS8) assessing pharmacists’ performance on the tasks
associated with assessment and plan of HDS counseling were loaded into another factor. These two factors were strongly correlated (rf-f = 0.93) and could be recognized as one construct, which corresponded to one of the KIRT assumptions, “unidimensionality”.
Quantifying pharmacists’ provision of HDS-related counseling
The proportion scores of two measures (i.e., PC-G, PC-HDS), which quantify pharmacists’ provision of HDS-related counseling, were significantly higher in the pilot study than in the larger scale study (p<0.05). After adjusting for item difficulty, the person logit scores on the PC-G and PC-HDS were significantly higher in the pilot study than in the larger scale study (p<0.05), which indicated that respondents seemed more likely to perform more activities in the pilot study than in the large-scale study.
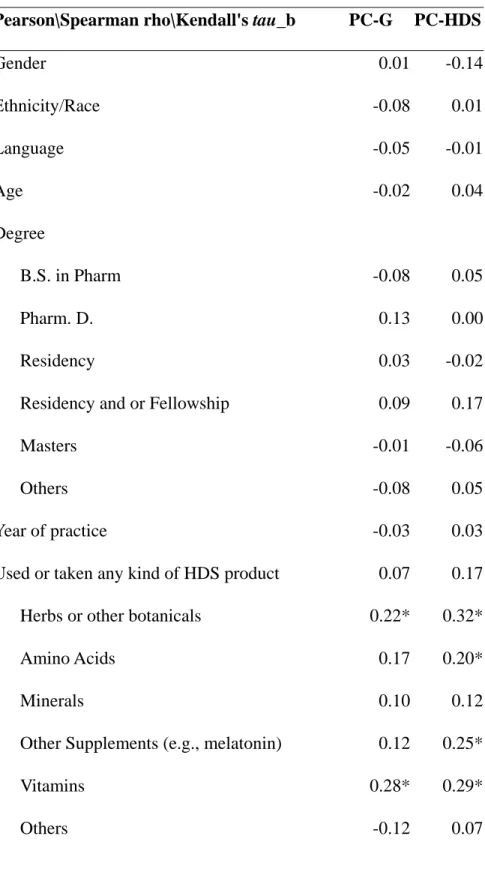
Table 4 presents the strength of correlations between the pharmacists’ background information and their person scores for each measure based on the correlation coefficients. There were zero to weak correlation values (r ranged from |0.001 | to <| 0.2|) between the majority of pharmacists’ demographic information and their person logit scores, even if
there were some exceptions. Experience with disease state management was positively correlated with the PC-G (rs≥0.2). Performance of HDS counseling was positively correlated, e.g. r = 0.20 to 0.35 with pharmacists’ own experience taking herbs and other supplements, practicing in community pharmacy, counseling OTC/ self-care, offering HDS and offering HDS information with the PC-HDS (rs≥ +0.2 ).
In addition, strong correlations existed between pharmacists’ person scores of PC-G and PC-HDS (mean of r [95% Interval] =0.53 [0.40, 0.64] for logit unit and
0.55[0.45,0.73] for proportion score, respectively).
DISCUSSION
Pharmacists and other clinicians are expected to help consumers by evaluating the effectiveness and safety evidence for HDS products and sharing this information with consumers.14 In this study, a newly developed instrument for assessing the performance of counseling by pharmacists was supported by the evidence of validity and reliability. We propose that the well-validated instrument can be used for self-assessment by
pharmacists, evaluation of student competencies by pharmacy faculty and preceptors, and quality improvement initiatives by pharmacy managers. This instrument fills a gap in the assessment of quality of care associated with HDS-related professional services.
The instrument for the assessment pharmacists’ provision of counseling was bifurcated into two measures: general counseling and HDS-specific counseling. This was necessary because the pharmacist-patient encounter may or may not begin with an HDS inquiry. It may, however, result in an HDS-related recommendation, and vice versa. This instrument implicitly captures the quality of patient counseling encounters
which they are conducted. Although not all tasks performed by the pharmacist related to a counseling encounter are captured, the instrument quantifies key elements involved in patient counseling associated with HDS.
Previous measures related to counseling have demonstrated evidence of validity and reliability using primarily classical test theory based approaches which assume for instance, that scores are normally distributed and that the measure is
unidimensionality.30-34 In contrast, the KIRT used in the present study does not invoke assumptions of normality, and the results demonstrated good construct validity and internal consistency for each measure. Additional convergent validity of the patient counseling measures was presented based on significant relationships with related factors.
In this study, pharmacists were requested to indicate their frequency of HDS provision in the context of statements to describe different activities related to HDS patient counseling. In contrast, previous studies used different approaches to operationalizing item responses related to specific or general activities about HDS counseling. Some studies used one or more dichotomous questions.16,18-19,24,53-55 For instance, pharmacists were asked whether they had received inquiries from patients about natural products on a weekly or monthly basis in Dolder’s study.19 Some studies inquired about the length of pharmacists’ encounters 15,18 or asked pharmacists to rate the frequency using a Likert-type scale. For example, Brown’s study demonstrated
pharmacists rated (1=never, 5= always), on average, 2.5± 0.9, they inquired about the patients’ use of CAM.53
In the current study, the average person proportion score of PC-G of 0.65 would be analogous to endorsing 26/40 points, or alternatively respondents endorsing “some of
the time” to all eight items. The average person proportion score of PC-HDS of 0.46 would be equivalent to endorsing 16/35 points, which would indicate that pharmacists responded, on average, with at least “a little of the time” to all seven items. This implies respondent pharmacists tended to spend at least “a little of the time” on either patient counseling, in general, or HDS specifically in their daily practice. After adjusting for item difficulty, the average person logit score on the PC-G was dramatically higher than the scores on the PC-HDS. Given the strong correlation between pharmacists’ person scores of PC-G and PC-HDS, these results imply pharmacists who provided more general counseling tended to provide more HDS- specific counseling and vice versa. Moreover, pharmacists who personally use herbs, amino acid, vitamins, other supplements, and who worked in the community settings, and who worked in the settings which offered the HDS and provided HDS related information tended to spend more time on counseling patients about HDS-related matters. These results intuitively mimic current pharmacy practice behaviors.
In fact, many patients tend not to disclose HDS product use experience to their primary health care professionals.1,56-57 With these findings, the results in this study can help to guide the development of interventions, specifically for pharmacy managers and preceptors, which target pharmacists’ awareness and pharmacy students’ professional performance regarding patient care with respect to the appropriate use of HDS products. The 15-item patient counseling measure could be used for quality and performance assessment in pharmacy practice, experiential training (e.g., IPPE, APPE), postgraduate continuing education, and for allied health clinicians. The 8-item PC-G scale could be used as a stand-alone measure for general patient counseling of medication, while the
7-item PC-HDS could be modified for use in patient counseling concerning other
self-care OTC products as well. Nevertheless, the authors encourage further validation and application of the instrument to evaluate educational outreach, experiential training and quality assurance in diverse settings. Regardless, these results were exploratory in nature and further use of the instrument in other samples of pharmacists, pharmacy trainees or clinicians would greatly enhance its generalizability.
CONCLUSION
Although it is known there exists no single, standardized patient counseling measure or instrument applicable for all pharmacy practice or experiential training scenarios, the psychometric properties of this newly developed measure support its use in assessing pharmacists' counseling behaviors on HDS products. Findings suggest the instrument can be used as a tool for quality assurance and training assessment to ensure a standard level of HDS-related patient counseling is being provided.
ACKNOWLEDGEMENTS:
The authors express their gratitude to Robert Bennett, Carla Denise Clemmons, Maria Charisse De Leon Santos, John Hessian, the Illinois Pharmacists Association executive staff, Swu-Jane Lin, Alexandra Perez, Vikrant Vats, Caitlyn Wilke, Robert Wittenberg, Margareta S. Zwolenik, and the study participants.
References
1. Eisenberg DM, Davis RB, Ettner SL. Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA 1998; 280:1569-75. 2. National Center for Complementary and Alternative Medicine. The use of
complementary and alternative medicine in the United States, 2004. Available at www.nccam.nih.gov/news/camsurvey_fs1.htm#use. Accessed October 6, 2005.
3. Crawford SY, Leventis C. Herbal product claims: boundaries of marketing and science. J Consum Marketing 2005;22(7):432-6.
4. Johnston BA. One-Third of Nation's Adults use Herbal Remedies: Market Estimated at $ 3.24 Billions. Herbalgram 1997; 40:52.
5. Lam A, Bradley G. Use of self-prescribed nonprescription medications and dietary supplements among assisted living facility residents. J Am Pharm Assoc (Wash DC) 2006; 46:574-581.
6. Mechanick JI. The rational use of dietary supplements and nutraceuticals in clinical medicine. Mt Sinai J Med 2005;72(3):161-65.
7. Kaufman, DW, Kelly JP, Rosenberg L et al. Recent patterns of medication use in the ambulatory adult population of the United States: the Slone Survey. JAMA 2002; 287: 337-344.
8. Wong RS, Cheng G, Chan TY. Use of herbal medicines by patients receiving Warfarin. Drug Saf 2003; 26(8):585-88.
9. Qato DM, Alexander GC, Conti RM et al. Use of Prescription and Over-the-counter Medications and Dietary Supplements among Older Adults in the United States. JAMA. 2008; 300(24):2867-2878
10. Collins SC, Dufresne RG. Dietary supplements in the setting of Mohs Surgery. Dermatol Surg 2002; 28:447-52.
11. Tsen LC, Segal S, Pothier M, Bader AM. Alternative medicine use in presurgical patients. Anesthesiology. 2000;93:148-151.
12. Kaye AD, Clarke RC, Sabar R, et al. Herbal medications: current trends in anesthesiology practice–a hospital survey. J Clin Anesth. 2000;12:468-471. 13. American Society of Health-System Pharmacists. ASHP statement on the use of
dietary supplements. Am J Health Syst Pharm 2004; 61(16):1707-11.
14. Miller LG, Harris HA, Jackson EA, Kanmaz TJ, Cauffield JS, Chin TW, et al. White paper on herbal products. American College of Clinical Pharmacy. Pharmacotherapy 2000; 20(7):877-91.
15. Bouldin AS, Smith MC, Garner DD, Szeinbach SL, Frate DA, Croom EM. Pharmacy and herbal medicine in the US. Soc Sci Med 1999; 49:279-89.
16. Howard N, Tsourounis C, Kapusnik-uner J. Dietary supplement survey of pharmacists: personal and professional practices. J Altern Complement Med 2001; 7(6):667-80.
17. National Council on Patient Information and Education (NCPIE). Attitudes and beliefs about the use of over-the-counter medicines: a dose of reality: HarrisInterative, January 2002. Available at http://www.bemedwise.org/survey/final_survey.pdf. Accessed October 2, 2005
18. Welna EM, Hadsall S, Schommer JC. Pharmacists' personal use, professional practice behaviors, and perceptions regarding herbal and other natural products. J Am Pharm Assoc (2003) 2003; 43(5):602-11.
19. Dolder C, Lacro J, Dolder N, Gregory P. Pharmacist's use of and attitudes and beliefs about alternative medications. Am J Health Syst Pharm 2003; 60(1):1352-57.
20. Maglion M, Miotto K, Iguchi M., Jungvig L, Morton SC, ShekellePG. Psychiatric effects of ephedra use: an analysis of food and drug administration reports of adverse events. American Journal of Psychiatry, 2005; 162, 189-191.
21. Popovich NG Nonprescription medications and self-care: nonprescription medication therapy and self-care instruction. Am J Pharm Educ , 2006; 70(6), Article 136.
22. Chang ZG, Kenney DT, Holdford D A, Small R E. (2000). Pharmacists' knowledge and attitudes toward herbal medicine. Ann Pharmacother,2000; 34, 710-715.
23. Shields KM, McQueen CE, Bryant PJ. Natural product education in schools of pharmacy in the United States. Am J Pharm Educ. 2003;67(1):Article 10.
24. Shah B, Siganga W, Mallya U, Shah S. Pharmacy student perspectives on classroom education about herbal supplements. Am J Pharm Educ. 2005;69(5):Article 102. 25. Mackowiak ED, Parikh A, Freely J. Herbal product evaluation in United States
pharmacy schools: core or elective program? Am J Pharm Educ. 2001;65(1):1-6. 26. Clauson KA, McQueen CE, Shield KM, Bryant PJ. Knowledge and attitudes of
pharmacists in Missouri regarding natural products. Am J Pharm Educ 2003; 67(2): Article 41.
27. Accreditation Council for Pharmacy Education (ACPE). Accreditation standards and guidelines for the professional program in pharmacy leading to the Doctor of Pharmacy degree. 2007.
http://www.acpe-accredit.org/pdf/ACPE_Revised_PharmD_Standards_Adopted_Jan1520 06.pdf. Accessed June 23, 2010.
28. Kwan, D., Hirchkorn, K., & Boon, H. U.S. and Canadian pharmacists' attitudes, knowledge, and professional practice behaviors toward dietary supplements: a systematic review. BMC Complement Altern Med, 2006; 6(31).
29. Puumalainen I. Development of instruments to measure the quality of patient counseling. Helsinki, Finland: Department of Social Pharmacy, Faculty of pharmacy, University of Kuopio, 2005.
30. Kemper KJ, Gardiner P, Gobble J, Woods C. Expertise about herbs and dietary supplements among diverse health professionals. BMC Complement Altern Med 2006;6(15):1-9
31. Gupchup GV, Wolfgang AP, Thomas J, III. Development of a scale to measure directive guidance by pharmacists. Ann Pharmacother 1996; 30(12):1369-75.
32. Ward PR, Bissell P, Noyce PR. Criteria for assessing the appropriateness of patient counseling in community pharmacies. Ann Pharmacother 2000; 34(2):170-75. 33. Bartlett EE. At last, a definition. Patient Educ Couns 1985; 7(4):323-24.
34. Puumalainen, II, Kause JM, Airaksinen MS. Quality assurance instrument focusing on patient counseling. Ann Pharmacother 2005; 39(7-8):1220-26.
35. American Dietetic Association, American Pharmaceutical Association. A healthcare professional? Guide to evaluating dietary supplements, 2000. Available at
http://www.pharmacist.com/pdf/dietary_supplements.pdf. Accessed August 16, 2006 36. Rosenbloom C, Storile J. A nutritionist's guide to evaluating ergogenic aids. Am.
37. Isetts BJ, Brown LM. Patient assessment and consultation In: Handbook of
Nonprescription Drugs, 15th Ed, Berardi R, Senior Editor. Washington, DC: American Pharmacists Association 2006:17-35.
38. Epstein RE, Street JRL. Patient-centered communication in cancer care: promoting healing and reducing suffering. Bethesda, MD: National Cancer Institute, 2007.
Available at http://outcomes.cancer.gov/areas/pcc/communication/monograph.html. Accessed Jun 10, 2006
39. Briss PA, Zaza S, Pappaioanou M, Fielding J, Wright-De Aguero L, Truman BI, et al. Developing an evidence-based Guide to Community Preventive Services--methods. The Task Force on Community Preventive Services. Am J Prev Med 2000; 18(1 Suppl):35-43.
40. Briss PA, Brownson RC, Fielding JE, Zaza S. Developing and using the Guide to Community Preventive Services: lessons learned about evidence-based public health. Annu Rev Public Health 2004; 25:281-302.
41. Farris KB, Kirking DM. Assessing the quality of pharmaceutical care. II. Application of concepts of quality assessment from medical care. Ann Pharmacother 1993;
27(2):215-23.
42. Farris KB, Kirking DM. Assessing the quality of pharmaceutical care. I. One perspective of quality. Ann Pharmacother 1993;27(1):68-73.
43. Hudmon KS, Prokhorov AV, Corelli RL. Tobacco cessation counseling: pharmacists' opinions and practices. Patient Educ Couns 2006;61(1):152-60.
44. Truman BI, Smith-Akin CK, Hinman AR, Gebbie KM, Brownson R, Novick LF, et al. Developing the Guide to Community Preventive Services--overview and rationale. The
Task Force on Community Preventive Services. Am J Prev Med 2000;18(1 Suppl):18-26.
45. Zaza S, Wright-De Aguero LK, Briss PA, Truman BI, Hopkins DP, Hennessy MH, et al. Data collection instrument and procedure for systematic reviews in the Guide to Community Preventive Services. Task Force on Community Preventive Services. Am J Prev Med 2000;18(1 Suppl):44-74.
46. Karabatsos, G. (2006). An R computer program for the kernel regression approach to Nonparametric IRT. University of Illinois-Chicago.
47. Ramsay, J.O. (1991). Kernel smoothing approaches to nonparametric item characteristic curve estimation. Psychometrika, 56(4), 611-630.
48. Lin HW. Pharmacists’ knowledge, attitudes, self-efficacy and counseling on herbs and dietary supplements. Chicago IL, United States: Department of Pharmacy Administration, Graduate College of the University of Illinois at Chicago, 2008. 49. Smith EV. Evidence for the Reliability of Measures and Validity of Measure
Interpretation: A Rasch Measurement Perspective. In: Smith EV, Smith RM, editor. Introduction of Rasch Measurement. Maple Grove, MN: JAM Press, 2004.
50. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika 1951; 16:297-334.
51. Massey FJ. The Kolmogorov-Smirnov Test for goodness of fit. J Am Statist Assoc1951; 46:68-78.
52. Efron B. Bootstrapping method: another look at Jackknife. Ann Statist 1979; 7(1):1-26.
53. Brown CM, Barner JC, Shah S. Community pharmacists' actions when patients use complementary and alternative therapies with medications. J Am Pharm Assoc (Wash DC) 2005;45(1):41-47.
54. Clauson KA, McQueen CE, Shield KM, Bryant PJ. Knowledge and attitudes of pharmacists in Missouri regarding natural products. Am J Pharm Educ 2003; 67(2): Article 41.
55. Dunn JD, Cannon E, Lewis T, Shane-McWhorter L. Development of a
complementary and alternative medicine (CAM) pharmacy and therapeutics (P&T) subcommittee and CAM guide for providers. J Manag Care Pharm 2005;
11(3):252-258.
56. Blendon R J, DesRoches CM, Benson JM, Brodie M, & Altman DE. American's views on the use and regulation of dietary supplements. Arch Intern Med, 2001; 161: 805-810.
57. Hensrud DD, EngleDD, & ScheitelS. M. Underreporting the use of dietary
supplements and nonprescription medications among patients undergoing a periodic health examination. Mayo Clin Proc 1999; 74(5), 443-447.
Figure 1: Effective patient/consumer-pharmacist consultation process for a clinical encounter related to HDS in a community pharmacy
Table 1: Item content included in patient counseling measures in the pilot study Domain
(N)
Component (N)
Item content to be examined Item IDb
Patient counseling - general (N= 17 items)
Subjective Patient’s self-care needs PC-G1 (3 items) Patient’s feeling PC-G2 a
Patient’s health concerns PC-G3 Objective Patient’s relevant medical history PC-G4 a Foster
relationship/ Information gathering
(5 items) (2 items) Patient’s current medication use PC-G5 a Content Identify potential solutions PC-G7 a (2 items) Consider the benefits/risks of options PC-G8 Identify patient’s preference of options PC-G9 a
Process Seeking literature PC-G6 a
Assessment (5 items)
(2 items) Decide the need of referral PC-G13 a Recommendation Advise about self-care PC-G10 a (4 items) Advise in lay terms PC-G11
Offer general management approaches PC-G12 a Suggest consult physicians PC-G17 Documentation
(1 item)
Document the inquiry PC-G14 a
Monitoring Follow-up on treatment effectiveness PC-G15 Plan/
Follow-up (7 items )
(2 items) Follow-up on undesired effects PC-G16
Assessment Content Explain effectiveness PC-HDS2 (4 items ) (2 items) Explain the pros and cons of HDS use PC-HDS3 a
Process Ensure product quality. PC-HDS1 a (2 items) Identify undesired/adverse effects PC-HDS8 a Plan/
Follow-up
Recommendation Refer patient for medical care as a result of HDS misuse.
PC-HDS4
(7 items) (4 items) Make an evidence-based recommendation
PC-HDS5
Ensure appropriate HDS dosage PC-HDS6 a Provide written information PC-HDS7 a Documentation (1 item) Document the use PC-HDS9 Monitoring Follow-up on treatment effectiveness PC-HDS10 a (2 items) Follow-up undesired effects PC-HDS11 a a
: Items were retained in the instrument prepared for the larger scale validation study b
Table 2: Psychometric properties of patient counseling - general measure (PC-G) in
two stages of validation studies Psychometric
properties\construct
Pilot study Larger scale study
Refinement Prior After Prior After
# of items 17 10 10 8 Reliability Mean (sd) 0.91 (0.03) 0.86 (0.06) 0.85 (0.02) 0.81 (0.02) 95% interval (0.84, 0.95) (0.71, 0.93) (0.82, 0.88) (0.76, 0.85) KIRT results Participant strata 4.57 2.70 3.51 3.09
Person proportion scores - 0.73(0.09) - 0.65(0.08)
Person logit scores
Mean (sd) 1.27 (0.98) 0.58 (1.48) 0.69 (0.64) 0.67 (0.68)
95% interval (0.08, 3.43) (-2.76, 2.18) (-0.4, 1.99) (-0.4, 2.21)
Item logit scores
Mean (sd) -1.15 (0.59) -0.72 (0.98) -0.65 (0.34) 0.61 (0.36)
95% interval (-2.23, -0.23) (-2.54, 0.75) (-0.97, 0.04) (-0.93, 0.07)
# non-monotonic item(s)a 0 0 2 0
# pair(s) of items with variant item ordering
17 0 0 0
item ordering
# items with less than n-2 functional category responses (n= # of category responses)
3 0 0 0
a
:proportion respondents endorsing higher item levels not increasing as the latent trait level increases
Table 3: Psychometric properties of patient counseling – HDS measure (PC-HDS) in
two stages of validation studies Psychometric
properties\construct
Pilot study Larger scale study
Refinement Prior After Prior After
# of items 11 7 7 Reliability Mean (SD) 0.84 (0.10) 0.86 (0.08) 0.89 (0.01) - 95% interval (0.55, -0.94) (0.67,- 0.95) (0.85,0.91) - KIRT results Participant strata 3.39 2.70 4.13 -
Person proportion scores - 0.55(0.09) - 0.46(0.11)
Person logit scores
Mean (SD) 0.13 (0.87) 0.29 (1.29) -0.12 (0.8) -
95% interval (-0.76,2.54) (-1, 3.88) (-1.35, 1.41) -
Item logit scores
Mean (SD) 0.06 (0.3) -0.11 (0.33) 0.14 (0.43) -
95% interval (-0.52,0.39) (-0.55, 0.33) (-0.42, 0.63) -
# non-monotonic item(s)a 3 0 0 -
# pair(s) of items with variant item ordering
1 0 0 -
item ordering
# items with less than n-2 functional category responses (n= # of category responses) 1 0 0 - a
:proportion respondents endorsing higher item levels not increasing as the latent trait level increases
Table 4: The strength of correlations between the performance of HDS counseling and the pharmacists’ background information
Pearson\Spearman rho\Kendall's tau_b PC-G PC-HDS
Gender 0.01 -0.14 Ethnicity/Race -0.08 0.01 Language -0.05 -0.01 Age -0.02 0.04 Degree B.S. in Pharm -0.08 0.05 Pharm. D. 0.13 0.00 Residency 0.03 -0.02
Residency and or Fellowship 0.09 0.17
Masters -0.01 -0.06
Others -0.08 0.05
Year of practice -0.03 0.03
Used or taken any kind of HDS product 0.07 0.17 Herbs or other botanicals 0.22* 0.32*
Amino Acids 0.17 0.20*
Minerals 0.10 0.12
Other Supplements (e.g., melatonin) 0.12 0.25*
Vitamins 0.28* 0.29*
Pearson\Spearman rho\Kendall's tau_b PC-G PC-HDS
Practice in community pharmacy or not 0.00 0.24* Current position (yr) -0.03 0.07 Health food store nearby 0.02 0.01
Average daily Rx -0.04 -0.07
Practice activity
Counseling pt about Rx 0.17 0.11 Counseling pt about OTC/self-care 0.10 0.21* Disease state management 0.23* 0.06 Management functions 0.02 0.11 Receiving/dispensing prescriptions -0.20 -0.06 Others 0.04 0.04 Employer-sponsored training of HDS 0.08 0.14 Offer HDS 0.05 0.21* Offer HDS information 0.06 0.27* *: the correlation coefficient was greater than |±0.2|