0066-4804/10/$12.00
doi:10.1128/AAC.01151-09
Copyright © 2010, American Society for Microbiology. All Rights Reserved.
Glycerol Monolaurate Inhibits Candida and
Gardnerella vaginalis In Vitro and
In Vivo but Not Lactobacillus
䌤
Kristi L. Strandberg,
1Marnie L. Peterson,
2Ying-Chi Lin,
2Melinda C. Pack,
3David J. Chase,
3and Patrick M. Schlievert
1*
Department of Microbiology, University of Minnesota Medical School, Minneapolis, Minnesota 55455
1; Department of
Experimental and Clinical Pharmacology, College of Pharmacy, University of Minnesota, Minneapolis, Minnesota 55455
2;
and Johnson & Johnson Consumer and Personal Products Worldwide, Skillman, New Jersey 08558
3Received 12 August 2009/Returned for modification 28 September 2009/Accepted 7 December 2009
We investigated the effects of glycerol monolaurate (GML) on Lactobacillus, Candida, and Gardnerella
vaginalis human vaginal microflora. Our previous work demonstrated that 6 months of GML treatment
vaginally does not alter lactobacillus counts in monkeys. Candida and G. vaginalis are commonly
associ-ated with vaginal infections in women, many becoming chronic or recurrent. In vitro growth inhibition
studies determined the effects of GML (0 to 500
g/ml) against multiple Candida species and G. vaginalis.
A randomized, double-blind study investigated the effects of GML on vaginal microflora Lactobacillus,
Candida, and G. vaginalis in colonized or infected women (n
ⴝ 36). Women self-administered intravaginal
gels containing 0% (n
ⴝ 14), 0.5% (n ⴝ 13), or 5% (n ⴝ 9) GML every 12 h for 2 days. Vaginal swabs were
collected before and immediately after the first gel administration and 12 h after the final gel
adminis-tration. Swabs were tested for Lactobacillus, Candida, G. vaginalis, and GML. In vitro GML concentrations
of 500
g/ml were candicidal for all species tested, while a concentration of 10 g/ml was bactericidal for
G. vaginalis. Control and GML gels applied vaginally in women did not alter vaginal pH or Lactobacillus
counts. Control gels reduced G. vaginalis counts but not Candida counts, whereas GML gels reduced both
Candida and G. vaginalis. No adverse events were reported by participating women. GML is antimicrobial
for Candida and G. vaginalis in vitro. Vaginal GML gels in women do not affect Lactobacillus negatively but
significantly reduce Candida and G. vaginalis.
The human vagina is colonized by microbes, and infections
occur when the balance is disturbed. Under healthy conditions,
vaginal flora is dominated by lactobacilli, which maintain acidic
pH through production of organic acids at times other than
menstruation (1, 8, 13, 30). Disruptions of vaginal pH or
lac-tobacilli may allow potentially pathogenic microorganisms to
grow and dominate.
Bacterial vaginosis (BV) is a common chronic infection
characterized by complex vaginal flora changes, which include
elevations of vaginal pH and, when symptomatic, malodorous
discharge and inflammation (2, 5, 11). BV is associated with
preterm delivery, increased risk of HIV transmission, and risk
of other infections (17). The prevalences of BV range from 4 to
40% of women, with the highest prevalence among patients at
sexually transmitted infection clinics (25). During BV
infec-tion, there are reductions in lactobacilli and increases in
bac-terial groups such as the Gram-negative bacterium Gardnerella
vaginalis (3, 10, 18, 25). Additional bacterial groups that are
associated with BV include Bacteroides fragilis and
Peptostrep-tococcus (12, 28). Current treatment recommendations for BV
include metronidazole and clindamycin (4).
Vulvovaginal candidiasis (VVC) is also a common infection.
VVC is caused by Candida species, most often Candida
albi-cans (7, 26). It is estimated that 70 to 75% of women
experi-ence VVC at least once during their reproductive years (14),
and 5 to 8% have recurrent VVC (9). C. albicans is isolated
from the vaginas of 85 to 95% of women (17, 27). Due to the
propensity of C. albicans to colonize, up to 30% of women
develop VVC as a posttreatment complication of BV (6).
Cur-rent recommendations for VVC treatment include topical
azole agents or oral fluconazole for uncomplicated vaginitis;
recurrent VVC should be managed with fluconazole (19). The
high recurrence rates of BV and VVC indicate the limitation of
current antimicrobial therapy and the need for better
thera-peutics.
Glycerol monolaurate (GML) is a naturally occurring
mono-glyceride that is generally recognized as safe for oral use by the
FDA (Title 21, Code of Federal Regulations [CFR], Part 184)
and has been used extensively in the food and cosmetic
indus-tries. GML has bactericidal properties for Gram-positive
or-ganisms (22, 23) and inhibits signal transduction at microbial
plasma membranes, thereby inhibiting transcription of
Gram-positive exotoxins (20, 22, 29). A critical exception is that
lactobacilli are insensitive to GML. Long-term in vivo studies
of monkeys show that 50 mg/ml of GML in intravaginal gels
does not inhibit lactobacilli and is not proinflammatory (24).
Gram-negative bacteria, such as Enterobacteriaceae, with intact
lipopolysaccharide (LPS) are not susceptible to GML (23).
* Corresponding author. Mailing address: Department of
Microbi-ology, University of Minnesota Medical School, 420 Delaware Street
SE, Minneapolis, MN 55455. Phone: (612) 624-1484. Fax: (612)
626-0623. E-mail: [email protected].
䌤
Published ahead of print on 14 December 2009.
We conducted this study to assess the effect of GML on
Candida and G. vaginalis, associated with VVC and BV,
respectively. GML was microbicidal for both organisms in
vitro. GML gels (0.5% and 5%) applied vaginally in women
reduced both organisms but did not reduce vaginal
lactoba-cilli.
MATERIALS AND METHODS
Microorganisms.A clinical isolate of G. vaginalis was provided by Fairview University Medical Center Microbiology. Four clinical isolates of C. albicans, the laboratory C. albicans strain SC5314, and one isolate each of Candida glabrata, C. krusei, C. parapsilosis, C. tropicalis, and C. pseudotropicalis (kefyr) were gen-erously provided by Judith Berman, University of Minnesota (UMN).
In vitro experiments.Growth inhibition studies investigated the effects of GML on Candida (C. albicans, C. glabrata, C. pseudotropicalis [kefyr], C. parapsilosis, C. tropicalis, and C. krusei) and G. vaginalis. The organisms were grown for 24 h in the presence of GML (0, 10, 50, 100, and 500g/ml) in Todd Hewitt (TH) broth at 37°C with shaking (200 rpm; Becton, Dickinson and Co., Sparks, MD) in 25 ml of medium in 125-ml Erlenmeyer flasks. Numbers of microbial CFU at various time points were determined by serial dilutions and plate counts.
Human study design.We conducted a single-center, double-blind, randomized study, approved by the UMN Institutional Review Board (IRB), to determine the effects of an intravaginal gel containing GML on Lactobacillus, Candida, and G. vaginalis.
Women were recruited by flyers posted at the UMN, Twin Cities, campus. Written informed consent was obtained prior to participation. Women between the ages of 18 and 50 who suspected they might have VVC and/or BV were eligible. Women with acute systemic infection or those using vaginal or perineal antimicrobial, immunosuppressant, antihistamine, or anti-inflammatory medica-tion (except oral nonsteroidal anti-inflammatory medicamedica-tion) within 2 weeks prior to participating were excluded. Women were not allowed to participate during menstruation. Pregnant women were excluded. Women were asked to refrain from sexual intercourse during participation. When CFU counts of Lac-tobacillus, Candida, and G. vaginalis were analyzed individually, subjects were omitted from analysis if they did not have the microbe being analyzed during at least at one of the two visits (⬍100 CFU/ml). Study participants were examined by a gynecologist (June LaValleur), who also confirmed the presence of yeast and/or BV before the women received intravaginal gels (except the first dose) and upon study completion. Participants maintained a diary of their experiences with the gels.
Thirty-nine women were randomized in that they used intravaginal GML gels (0.5% or 5%) or no GML for 2 days (total of 4 applications; 1 application every 12 h). Swabs of each woman’s vaginal secretions were collected at the initial visit (visit 1) (before gel insertion) and at the final visit (visit 2, 12 h after the final gel application) and were analyzed for microbes. Our studies have shown that vag-inal swabs consistently absorb 0.1 ml of fluid, thus allowing quantification of microorganisms. Briefly, during each clinical visit, vaginal swabs were collected and placed directly into 1 ml of TH broth. These were then serially diluted, plated onto chocolate agar plates, and allowed to grow at 37°C in 7% CO2for up
to 3 days. Plates were analyzed for quantities of Lactobacillus, Candida, and G. vaginalis on the basis of expected microbial characteristics. Numbers of CFU per milliliter of vaginal secretions were determined, and numbers from visit 1 versus those from visit 2 were compared. The minimum level of detection of microbes in our analyses was 102CFU/ml.
By IRB requirements, one subject was not allowed to complete the study, due to the presence of Trichomonas vaginalis in the sample collected before the first administration of gel; this subject was enrolled in the study and received her first gel treatment (determined to be 0.5% GML gel after the blind was broken). The subject was advised to seek treatment from her regular physician; she later called the investigators to report that she showed no further evidence T. vaginalis infection, as determined by her physician, even though she had received no additional therapy. Data from two subjects, one in the control group and one in the 5% GML group, were excluded from analyses because of unknown material present vaginally during the visit 2 examination.
Swabs were also collected at the initial visit after gel insertion and at the final visit for determination of GML content through use of gas chromatography-mass spectrometry (GC-MS) at the UMN, College of Pharmacy. The lower limit of GML detection was 0.7g/ml.
Gel formulation.GML (Cognis, Cincinnati, OH) was dissolved in gels made at the Fairview Compounding Pharmacy, Minneapolis, MN, by a pharmacist (M. L. Peterson) to mimic K-Y warming gel to achieve final concentrations of 0.5% or
5% and pHs of 4 to 4.5 (16, 24). Vaginal applicators (Exacta-Med vaginal dispensers; Baxa Corporation, Englewood, CO) were filled with 5 ml of gels. Applicators containing gels were given to the Fairview Investigational Drug Studies Pharmacy, which distributed filled applicators to study participants so that treatment and data analyses remained blinded to the investigators during experimentation.
The vehicle control for preparing GML gels, mimicking K-Y warming, was chosen because the intravaginal gel is an approved class II medical device for use in women, and GML is highly soluble in the gel. The combination of the intravaginal gel and GML is also regarded as a class II medical device, as determined by the UMN IRB. Medical devices are subject not to Investigational New Drug (IND) exemptions for clinical studies but rather to Investigational Device Exemption (IDE) procedures. In the case of a device that is considered to be a “nonsignificant risk” device, as this one is, the IDE is an “abbreviated IDE,” involving review by an IRB rather than by the FDA itself. This device and the research study were reviewed and approved by the UMN IRB, and this approval can be considered to be the “abbreviated IDE.”
Data analyses.Differences in number of CFU/ml of vaginal Lactobacillus, Candida, and G. vaginalis were calculated for the initial samples (visit 1), col-lected prior to the use of intravaginal gels, and the final samples (visit 2), collected upon study completion. Significant differences (P⬍ 0.05) by the paired Student’s t test or trends toward significance (P⬍ 0.2) in number of CFU/ml were regarded as evidence of GML effects. McNemar’s test was used to com-pare the prevalences of microorganisms in visit 1 and visit 2. The analyses were performed using GraphPad Prism version 5.01 (GraphPad software, La Jolla, CA).
RESULTS
In vitro studies.
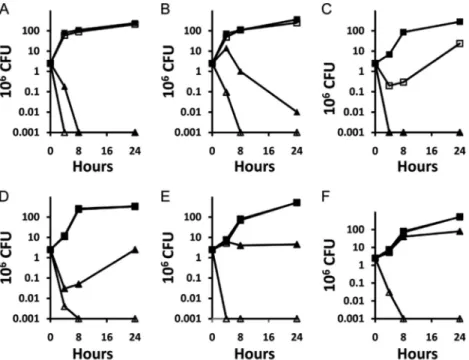
Dose-related effects of GML on C. albicans
strain SC5314 and five other species of Candida in vitro are
shown in Fig. 1A to F. GML was fungicidal, as defined by a
ⱖ3-log drop in number of CFU/ml for 24 h, for all Candida
species at GML concentrations of 500
g/ml GML within 4 to
8 h and for C. albicans and C. pseudotropicalis (kefyr) also at
100
g/ml. Four additional clinical isolates of C. albicans
showed susceptibilities to GML similar to those observed for
the laboratory strain. GML (10
g/ml) was bactericidal, as
defined by a
ⱖ3-log drop in number of CFU/ml for 24 h, for G.
vaginalis (Fig. 2).
In vivo studies.
A total of 36 women were analyzed in this
study. Most women exhibited vaginal discharge during visit 1,
prior to receiving vaginal gel. A few also showed vulvar
ery-thema and edema. One woman was determined to have BV
associated with anaerobic streptococci (presumed to be
Pep-tostreptococcus) but not G. vaginalis; this woman also had a
documented Candida infection and was included in the study.
A Gram stain of this participant’s vaginal discharge collected at
visit 1 revealed yeasts and high numbers of Gram-positive
anaerobic cocci; these organisms were absent in visit 2. This
subject was in the 0.5% GML treatment group. After the blind
was broken, 9 analyzable subjects received 5% (50 mg/ml)
GML gel, 13 received 0.5% (5 mg/ml) GML gel, and 14
ceived control gel without GML. No adverse events were
re-ported by any of the women.
GML was detected vaginally in the women immediately
after initial application of the GML gels (data not shown);
GML was not detected (
⬍0.7 g/ml) in women who received
control gels. GML was undetectable in women during the
second visit, regardless of gel treatment, indicating that
GML did not persist in vaginal secretions for the 12 h
between treatments.
Table 1 summarizes the prevalences of the three study
mi-croorganisms, comparing visit 1 to visit 2. Because of the small
numbers of study participants, data for GML (0.5% and 5%)
were evaluated individually but also pooled for determination
of significant differences between visits. The prevalences of
Lactobacillus between visit 1 and visit 2 for all treatment
groups were not significantly different, consistent with the idea
that the gels with or without GML have no effect on lactobacilli
(24). Candida prevalences between visit 1 and visit 2 were not
different in women given control gels (P
⫽ 0.45) but were
significantly reduced by treatment with GML gels (P
⫽ 0.003).
G. vaginalis prevalences between visit 1 and visit 2 were also
not significantly different in women given control gels but were
significantly lower at visit 2 than at visit 1 for the combined
GML treatment groups.
Table 2 summarizes quantitative colony count data for the
three microorganisms in the treatment groups. The control and
GML gels did not inhibit Lactobacillus between visit 1 and visit
2. Three study participants had significant increases in
Lacto-bacillus counts, from 10
2to 10
8CFU/ml (P
⫽ 0.007). Since
Lactobacillus is important for establishing acidic pH in the
vagina, pH was measured at visits 1 and 2. No significant
difference was seen in vaginal pH between visits 1 and 2,
suggesting that none of the gels altered vaginal pH (data not
shown).
No significant differences in Candida counts were seen
be-tween visits 1 and 2 in women who received control gels (Table
2). In contrast, women who received the 0.5% GML gels
showed significant reductions in Candida CFU at visit 2 in
comparison to the level for visit 1 (P
⫽ 0.001). Women who
received the 5% GML gel treatment also showed reductions in
Candida CFU from visit 1 to visit 2, but this reduction was not
statistically significant (P
⫽ 0.15). When the Candida counts
for subjects who received either of the GML-containing gels
were combined for analysis, thereby increasing the sample size,
highly significant reductions from visit 1 to visit 2 were found
(P
⫽ 0.001) (Table 2). The reduction of Candida in the GML
gel-treated women who showed reductions between visits 1
and 2 was nearly at the minimum level of detection in our
analyses (10
2CFU).
Significant reductions were seen in G. vaginalis counts
between visits 1 and 2 for women who received the control
FIG. 1. In vitro effect of GML on the growth of Candida species: C. albicans (A), C. glabrata (B), C. pseudotropicalis (kefyr) (C), C. parapsilosis
(D), C. tropicalis (E), and C. krusei (F). Candida strains were incubated for 24 h in the presence of various concentrations of GML at 37°C. Samples
were removed at the indicated times for determination of CFU counts. The GML concentrations were 0
g/ml (f), 50 g/ml (䡺), 100 g/ml (Œ),
and 500
g/ml (‚).
FIG. 2. In vitro effect of GML on the growth of G. vaginalis. G.
vaginalis was cultured for 24 h in the presence of various
concentra-tions of GML at 37°C. Samples were removed at the indicated times
for determination of CFU counts. The GML concentrations included
0
g/ml (f), 1 g/ml (䡺), 5 g/ml (Œ), and 10 g/ml (‚).
gel (P
⫽ 0.006) (Table 2). Women who received the 0.5%
and 5% GML gel treatments did not individually show
sig-nificant reductions in G. vaginalis levels between visit 1 and
visit 2 (P
⫽ 0.13 and P ⫽ 0.07, respectively). When data
from the 0.5% and 5% GML gel treatment groups were
combined and analyzed, the counts of G. vaginalis at visit 2
were found to be significantly lower than those observed at
visit 1 (P
⫽ 0.015) (Table 2).
DISCUSSION
Our studies demonstrate that Candida and the
Gram-negative bacterium G. vaginalis are killed by GML in vitro
and in women by intravaginal GML gels; however, G.
vagi-nalis in vivo is also killed by gels lacking GML. Both
Pep-tostreptococcus and T. vaginalis may be killed in vivo by GML
gels.
Previous studies demonstrate that GML inhibits growth and
production of exotoxins of various Gram-positive bacterial
groups but does not inhibit the growth or metabolism of
lac-tobacilli (23, 24). GML does not inhibit Enterobacteriaceae
unless LPS mutants, such as Re, are present (23). G. vaginalis
is a Gram-negative bacterium that contains a
lipooligosaccha-ride in its outer membrane and, like Re mutants, is sensitive to
growth inhibition by GML (23). We confirmed, and
signifi-cantly extended, previous reports that GML inhibits Candida
(15). These yeasts are killed in vitro by GML (100 to 500
g/ml).
Our in vivo studies investigated the effects of GML gel on
the vaginal microflora in 36 women with VVC and/or BV
organisms. In blinded fashion, we evaluated gels containing
0%, 0.5% (5,000
g/ml), or 5% (50,000 g/ml) GML for effects
on Lactobacillus, Candida, and G. vaginalis over 2 days; both of
the GML concentrations are in excess of the in vitro
concen-trations necessary to exert microbicidal activity against
Can-dida and Gardnerella. When the Lactobacillus levels in the
women were monitored, we observed that neither the 0.5% nor
the 5% GML gels reduced Lactobacillus counts or altered
vaginal pH; in three instances, Lactobacillus counts increased
dramatically. In contrast, GML inhibited the growth of
Can-dida, in many cases below the limit of our detection. When the
data from both the 0.5% and the 5% GML treatment groups
were analyzed together, the reduction in Candida counts was
found to be highly significant compared to the level for the
control group. Both control and GML gels inhibited the
growth of G. vaginalis.
Collectively, our studies show that GML gels simultaneously
inhibit the growth of both VVC and BV organisms. (Although
not presented, GML in vitro inhibits Bacteroides fragilis,
an-other Gram-negative bacterium associated with BV.) GML
gels may be the first agents that allow simultaneous
manage-ment of both VVC and BV.
GML may be considered a dual-acting agent for
interfer-ence with vaginal microorganisms. GML directly kills both
Candida and Gardnerella. However, we recently
demon-strated that 5% GML gels, applied vaginally to monkeys,
prevented simian immunodeficiency virus (SIV)
transmis-sion (16, 24) by interference with epithelial cell production
of proinflammatory cytokines that attract CD4 T cells into
cervical/vaginal tissues. These data agree with prior studies
that demonstrate that GML exerts membrane-stabilizing
anti-inflammatory effects (21). In our study, GML
anti-in-flammatory effects are also likely to contribute to
interfer-ence with VVC and BV.
It is important to note that this is a small pilot study of
GML effects on vaginal microflora. Clinical studies are
re-quired to confirm and extend our findings, particularly to
assess the effectiveness of GML gel in treating vaginal
in-fections.
TABLE 1. Prevalences of vaginal Lactobacillus, Candida, and G. vaginalis during clinic visits 1 and 2
GML treatment (no. of subjects)
Lactobacillus Candida G. vaginalis No. of women (%) positive Pa No. of women (%) positive Pa No. of women (%) positive Pa
Visit 1 Visit 2 Visit 1 Visit 2 Visit 1 Visit 2
0% (14)
8 (57)
8 (57)
1
9 (64)
6 (43)
0.45
10 (71)
5 (36)
0.07
0.5% (13)
9 (69)
11 (85)
0.48
10 (77)
3 (23)
0.02
7 (54)
4 (31)
0.25
5% (9)
6 (67)
7 (78)
1
6 (67)
2 (22)
0.13
6 (67)
3 (33)
0.25
0.5% and 5% combined (22)
15 (68)
18 (82)
0.25
16 (73)
5 (23)
0.003
13 (59)
7 (32)
0.04
aP values determined by McNemar’s test.
TABLE 2. Average log numbers of CFU/ml of Lactobacillus, Candida, and G. vaginalis during clinic visits 1 and 2
GML treatment group
Lactobacillus Candida G. vaginalis
Avg⫾ SD
Pa Avg⫾ SD
P
Avg⫾ SD
P
Visit 1 Visit 2 Visit 1 Visit 2 Visit 1 Visit 2
0%
5.3
⫾ 3.2
5.3
⫾ 3.2
0.45
3.4
⫾ 1.7
3.0
⫾ 1.6
0.16
4.5
⫾ 1.9
3.1
⫾ 1.9
0.006
0.5%
6.1
⫾ 2.8
6.9
⫾ 2.3
0.24
4.6
⫾ 1.9
2.5
⫾ 1.2
0.001
3.9
⫾ 2.1
3.1
⫾ 2.0
0.13
5%
5.5
⫾ 3.0
6.1
⫾ 2.8
0.32
2.9
⫾ 1.2
2.3
⫾ 0.6
0.15
4.1
⫾ 2.1
2.7
⫾ 1.3
0.07
0.5% and 5% combined
5.8
⫾ 2.9
6.6
⫾ 2.5
0.12
3.9
⫾ 1.8
2.4
⫾ 1.0
0.001
4.0
⫾ 2.0
2.9
⫾ 1.7
0.015
a
ACKNOWLEDGMENTS
This research was supported by grants from both Johnson &
John-son (to the University of Minnesota) and the Academic Health Center,
University of Minnesota (to P.M.S. and M.L.P.).
June LaValleur, who recently retired from the University of
Min-nesota, Department of Obstetrics and Gynecology, is gratefully
ac-knowledged for clinical evaluation of study participants.
REFERENCES
1. Alvarez-Olmos, M. I., M. M. Barousse, L. Rajan, B. J. Van Der Pol, D. Fortenberry, D. Orr, and P. L. Fidel, Jr.2004. Vaginal lactobacilli in ado-lescents: presence and relationship to local and systemic immunity, and to bacterial vaginosis. Sex. Transm. Dis. 31:393–400.
2. Amsel, R., P. A. Totten, C. A. Spiegel, K. C. Chen, D. Eschenbach, and K. K. Holmes.1983. Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am. J. Med. 74:14–22.
3. Catlin, B. W. 1992. Gardnerella vaginalis: characteristics, clinical consider-ations, and controversies. Clin. Microbiol. Rev. 5:213–237.
4. Centers for Disease Control and Prevention. 2006. Sexually transmitted disease treatment guidelines, 2006. MMWR Recommend. Rep. 55(RR11): 1–94.
5. Eschenbach, D. A., P. R. Davick, B. L. Williams, S. J. Klebanoff, K. Young-Smith, C. M. Critchlow, and K. K. Holmes.1989. Prevalence of hydrogen peroxide-producing Lactobacillus species in normal women and women with bacterial vaginosis. J. Clin. Microbiol. 27:251–256.
6. Ferris, D. G., M. S. Litaker, L. Woodward, D. Mathis, and J. Hendrich. 1995. Treatment of bacterial vaginosis: a comparison of oral metronidazole, metronidazole vaginal gel, and clindamycin vaginal cream. J. Fam. Pract. 41:443–449.
7. Fleury, F. J. 1981. Adult vaginitis. Clin. Obstet. Gynecol. 24:407–438. 8. Forsum, U., E. Holst, P. G. Larsson, A. Vasquez, T. Jakobsson, and I.
Mattsby-Baltzer.2005. Bacterial vaginosis—a microbiological and immuno-logical enigma. APMIS 113:81–90.
9. Foxman, B., J. V. Marsh, B. Gillespie, and J. D. Sobel. 1998. Frequency and response to vaginal symptoms among white and African American women: results of a random digit dialing survey. J. Womens Health 7:1167–1174. 10. Gutman, R. E., J. F. Peipert, S. Weitzen, and J. Blume. 2005. Evaluation of
clinical methods for diagnosing bacterial vaginosis. Obstet. Gynecol. 105: 551–556.
11. Hawes, S. E., S. L. Hillier, J. Benedetti, C. E. Stevens, L. A. Koutsky, P. Wolner-Hanssen, and K. K. Holmes.1996. Hydrogen peroxide-producing lactobacilli and acquisition of vaginal infections. J. Infect. Dis. 174:1058– 1063.
12. Hill, G. B. 1993. The microbiology of bacterial vaginosis. Am. J. Obstet. Gynecol. 169:450–454.
13. Hillier, S. L. 1998. The vaginal microbial ecosystem and resistance to HIV. AIDS Res. Hum. Retrovir. 14(Suppl. 1):S17–S21.
14. Hurley, R., and J. De Louvois. 1979. Candida vaginitis. Postgrad. Med. J. 55:645–647.
15. Kabara, J. J. (ed.). 1984. Cosmetic and drug preservation: principles and practice, vol. 1. Marcel Dekker, Inc., New York, NY.
16. Li, Q., J. D. Estes, P. M. Schlievert, L. Duan, A. J. Brosnahan, P. J. Southern, C. S. Reilly, M. L. Peterson, N. Schultz-Darken, K. G. Brunner, K. R. Nephew, S. Pambuccian, J. D. Lifson, J. V. Carlis, and A. T. Haase. 2009. Glycerol monolaurate prevents mucosal SIV transmission. Nature 458:1034–1038.
17. Nyirjesy, P. 2008. Vulvovaginal candidiasis and bacterial vaginosis. Infect. Dis. Clin. North Am. 22:637–652.
18. O’Brien, R. F. 2005. Bacterial vaginosis: many questions—any answers? Curr. Opin. Pediatr. 17:473–479.
19. Pappas, P. G., C. A. Kauffman, D. Andes, D. K. Benjamin, Jr., T. F. Calandra, J. E. Edwards, Jr., S. G. Filler, J. F. Fisher, B. J. Kullberg, L. Ostrosky-Zeichner, A. C. Reboli, J. H. Rex, T. J. Walsh, and J. D. Sobel. 2009. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 48:503–535.
20. Pechous, R., N. Ledala, B. J. Wilkinson, and R. K. Jayaswal. 2004. Regulation of the expression of cell wall stress stimulon member gene msrA1 in methicillin-susceptible or -resistant Staphylococcus aureus. An-timicrob. Agents Chemother. 48:3057–3063.
21. Peterson, M. L., and P. M. Schlievert. 2006. Glycerol monolaurate inhibits the effects of Gram-positive select agents on eukaryotic cells. Biochemistry 45:2387–2397.
22. Projan, S. J., S. Brown-Skrobot, P. M. Schlievert, F. Vandenesch, and R. P. Novick.1994. Glycerol monolaurate inhibits the production of beta-lacta-mase, toxic shock toxin-1, and other staphylococcal exoproteins by interfer-ing with signal transduction. J. Bacteriol. 176:4204–4209.
23. Schlievert, P. M., J. R. Deringer, M. H. Kim, S. J. Projan, and R. P. Novick. 1992. Effect of glycerol monolaurate on bacterial growth and toxin produc-tion. Antimicrob. Agents Chemother. 36:626–631.
24. Schlievert, P. M., K. L. Strandberg, A. J. Brosnahan, M. L. Peterson, S. E. Pambuccian, K. R. Nephew, K. G. Brunner, N. J. Schultz-Darken, and A. T. Haase.2008. Glycerol monolaurate does not alter rhesus macaque (Macaca mulatta) vaginal lactobacilli and is safe for chronic use. Antimicrob. Agents Chemother. 52:4448–4454.
25. Sobel, J. D. 2000. Bacterial vaginosis. Annu. Rev. Med. 51:349–356. 26. Sobel, J. D. 1985. Epidemiology and pathogenesis of recurrent vulvovaginal
candidiasis. Am. J. Obstet. Gynecol. 152:924–935.
27. Sobel, J. D. 2007. Vulvovaginal candidosis. Lancet 369:1961–1971. 28. Thorsen, P., I. P. Jensen, B. Jeune, N. Ebbesen, M. Arpi, A. Bremmelgaard,
and B. R. Moller.1998. Few microorganisms associated with bacterial vagi-nosis may constitute the pathologic core: a population-based microbiologic study among 3596 pregnant women. Am. J. Obstet. Gynecol. 178:580–587. 29. Vetter, S. M., and P. M. Schlievert. 2005. Glycerol monolaurate inhibits
virulence factor production in Bacillus anthracis. Antimicrob. Agents Che-mother. 49:1302–1305.
30. Yamamoto, T., X. Zhou, C. J. Williams, A. Hochwalt, and L. J. Forney. 2009. Bacterial populations in the vaginas of healthy adolescent women. J. Pediatr. Adolesc. Gynecol. 22:11–18.