Title: Concurrent use of antiplatelets, anticoagulants, or digoxin with Chinese medications: a
population-based cohort study
Names of authors: Hsin-Hui Tsai · Hsiang-Wen Lin · Chun-Ru Chien · Tsai-Chung Li Hsin-Hui Tsai
Graduate Institute and School of Pharmacy, College of Pharmacy, China Medical University, Taichung, Taiwan
Department of Pharmacy, China Medical University Hospital, Taichung, Taiwan
Hsiang-Wen Lin (Corresponding author)
Graduate Institute and School of Pharmacy, College of Pharmacy, China Medical University, Taichung, Taiwan
Department of Pharmacy, China Medical University Hospital, Taichung, Taiwan No. 91 Hsueh-Shih road, Taichung, Taiwan 40402, R.O.C.
Tel: 886-4-22053366 ext 5151 Mobil: 886-4-963149906
[email protected], [email protected] Chun-Ru Chien
Department of Radiation Oncology, China Medical University Hospital, Taichung, Taiwan School of Medicine, China Medical University, Taichung, Taiwan
Tsai-Chung Li
Institute of Health Care Administration, College of Public Health, China Medical University, Taichung, Taiwan
Abstracts:
Purpose: To examine the extent of concurrent use of antiplatelets, anticoagulants, or digoxin with
Chinese medications (CM) and to identify its associated factors.
Methods: A retrospective cohort study was conducted using one million random samples of
Longitudinal Health Insurance Database 2005 in Taiwan. High-risk Western medications (HRWM) included antiplatelets (aspirin, clopidogrel, dipyridamole, ticlopidine), anticoagulants (heparin, warfarin), and digoxin. Concurrent use was described as having overlapping use period of HRWM with CM any time in 2005. Baseline demographics, comorbidities, and health services utilizations between patients with and without concurrent HRWM-CM use were compared. Logistic regression analyses were performed to identify factors associated with incident concurrent use.
Results: Of the 70,698 eligible HRWM users, 13.2% used CM concurrently for an average
durations of 26.7±43 days. The incidence of concurrent HRWM-CM use, which excluded prior CM use within six months preceding the first CM use, was 6.3%. Warfarin or ticlopidine users were more likely to be prescribed with CM than the other HRWM users. Factors associated with an increasing incidence of concurrent HRWM-CM use included female sex, age 45-54 years, middle monthly income, higher number of outpatient visits or distinct medications prescribed, and a previous diagnosis of heart diseases, stroke or hypertension. In contrast, age ≥65 years and higher medical expenditure were associated with a lower incidence of concurrent use.
Conclusions: Approximately one in eight HRWM users were concomitantly prescribed with CM
among Taiwanese population. Whether such concurrent use is associated with the adverse clinical outcomes warrants further investigations.
Introduction
The use of complementary and alternative medicine (CAM) has increased during the last few decades in Asia, the United States, and Europe . The estimated prevalence of CAM use varied across populations, ranging from 30-40% in the United States or Europe and to 60-70% in East Asia . Patients with chronic diseases, including cardiovascular diseases, were more likely to use CAM . The most resent systematic review indicated that 4 to 61% ever used CAM and 2% to 46% used herbal medicine among patients with cardiovascular diseases . Of various types of CAM, Chinese medicine is the most dominant form in many Asian countries . In particular, Chinese medicine is not only popular among Chinese population (including Chinese immigrants in the Western countries) but also among the other racial and ethnic groups such as Indians and Malays . As a result, both Western medicine and Chinese medicine are the common medical therapies in many parts of Asia .
Of various therapies of Traditional Chinese medicine (TCM), the concentrated Chinese medications, acupuncture, and traumatology manipulative therapies, which are prescribed by TCM physicians, are almost all covered by Taiwan’s National Health Insurance (NHI) since the program was incepted in 1995. Concentrated Chinese medications (CMs) are the extracts of a single CM or the combined CM remedy. All of these CM products are provided as the powder dosage form and its quality is regulated by Department of Health in Taiwan. Thus, these CM products are required to be manufactured by the companies that comply with the current good manufacture practice , and the detailed information about its ingredients, manufacturers and registration is provided transparently on the website ofCommittee on Chinese Medicine and Pharmacy, Department of Health, Executive Yuan, Taiwan using Traditional Chinese language .
In recent years, the utilization of concentrated CM products has increased in Taiwan . For instance, nearly 86% of patients seeking for reimbursed TCM therapies were prescribed with concentrated CM in 1996-2001 . However, concomitant use of Western medications and CM might result in unintended consequences, especially for those who took medications with a narrow
with warfarin would increase the bleeding risks, while use of danshen and ginseng might interfere the digoxin fluorescence polarization immunoassay, in which the digoxin levels might be
misinterpreted .
As in other developed countries, cardiovascular and cerebrovascular diseases are the two major diseases to be treated or prevented using antiplatelets, anticoagulants, or digoxin, while these two diseases are the top second and third causes of death in Taiwan (i.e., 10.9 and 7.1% of all deaths, respectively) . These two leading causes of death directly correspond to the chronic conditions experienced by many patients, who might have lived with these conditions that are typically controlled with medications for several years. Thus, patients with these diseases are very likely to seek CAM therapies, including herbs, concomitantly to prevent arterial or venous thrombosis,
strokes as well as to manage the discomfort due to heart problems .
However, it is not easy for the clinicians to outweigh the risks of potential complications on bleedings and possibility of misinterpreting the digoxin levels against the benefits of concurrent use between prescribed medications with CAM therapies to prevent possible cardiovascular risks. Concerning of the potential occurrences of serious interactions and its undesired consequences, the patterns of concomitant use of CM and western medications should be continuously assessed . However, up to now, there is very limited documented information about potential prescription drug interactions with Chinese medications and it actual use. The aim of this study was to examine the extent of concurrent use of the antiplatelets, anticoagulants, or digoxin with CM in Taiwan and to identify the factors
associated with such concurrent use.
Methods
The box 1 is the illustration for the major acronyms, including CAM, TCM, CM and HRWM, which are frequently used in this study
Data source
The National Health Insurance Research Database (NHIRD) in Taiwan, which contains the
enrollment and medical claims data from more than 99% of the Taiwanese population, was used in this study . The source population of this study was comprised of a random sample of one million NHI beneficiaries enrolled in 2005 (i.e., Longitudinal Health Insurance Database 2005, LHID2005). The distribution of the gender between the patients in the LHID2005 and the primary NHIRD was not significantly different. For our knowledge, this is one of formal population databases with complete information about prescription data of covered, concentrated CMs, which are commonly used in TCM practice in Taiwan. The analyses using NHIRD are exempt from the Institutional Review Board. That is because the NHIRD databases contain the identified person and de-identified institution information and are publicly available through the proper application process. All researchers who apply to use the NHIRD are required to sign a written agreement, which needs to declare that they have no intention to obtain information that could potentially violate the privacy of patients or care providers.
Study population
In this study, those antiplatelet drugs (aspirin, clopidogrel, dipyridamole, ticlopidine), anticoagulants (heparin, warfarin), and digoxin were considered as high-risk Western medications (HRWM), which might be prone to adverse drug reactions (i.e., bleeding, imbalance of electrolytes, influence digoxin immunoassay) or result in ineffective treatments due to drug-interactions.
Outpatients with at least one prescribed or dispensed HRWM at any time in 2005 were identified as HRWM users. Those HRWM users were grouped into either concurrent HRWM-CM users (i.e., with a concomitant use of CM during 2005) or HRWM-only users (i.e., without a concomitant use of CM during 2005). Concurrent HRWM-CM users were defined as those patients whose use of HRWM and CM overlapped for at least one day in 2005 based on the records of
prescribing/dispensing dates and their supplied days.
patients who had no prescription of CM for at least six months prior to the date of first CM prescription in 2005 (i.e., index date). For each incident HRWM-CM user, we randomly selected one counterpart of HRWM-only users in the same month of the index date and those who had the same duration of the HRWM use. Therefore, the index date of the selected HRWM-only users was the same as their counterpart of concurrent HRWM-CM users.
Potential factors associated with concurrent HRWM-CM use
The following variables as the potential factors of incident concurrent HRWM-CM use were identified based upon the literature and were used for further analyses : patients’ age, gender, monthly income, and region of NHI enrollment, as well as their comorbidities (based on ICD-9-CM codes) and health services utilizations ( e.g., outpatient visits, distinct medications, hospitalization) during the 6-month period prior to the index date. The “distinct medications” in this study refers all types of distinct medications, which had ever prescribed by physicians during observation period.
Statistical analyses
The prevalence and incidence of concurrent CM use among all identified HRWM users was estimated. The prevalence was calculated using the number of concurrent HRWM-CM users as the numerator and the number of all HRWM users as the denominator, whereas the number of incident HRWM-CM users was used as the numerator to calculate the incidence. The duration of concurrent use (in days) was expressed using the mean, standard deviation (SD), median, and interquartile range (IQR) to express the spread of distributions.
To identify the factors associated with the incidence of concurrent HRWM-CM use, the patients’ characteristics were compared between the incident HRWM-CM users and the randomly selected HRWM-only users using Chi-square tests. Then, univariate logistic regression model was used to estimate the crude association between each of the potential factors with the incidence of current HRWM-CM use. Lastly, a multivariate logistic regression model was fitted with the
from the univariate logistic regression analyses (i.e., criterion for selection was the p value < 0.05 except for cancer, stroke, and diabetes which were included according to literature ) were used as the independent variables. The crude and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were presented for all potential factors. All analyses were conducted using SAS version 9.1.
Results
Prevalence and incidence of concurrent HRWM-CM use
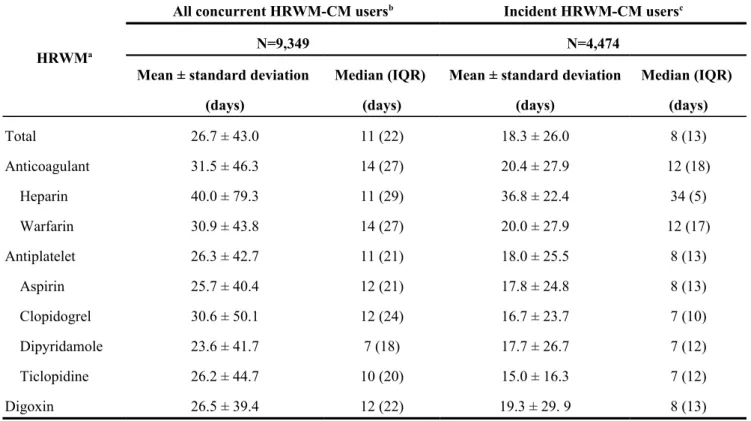
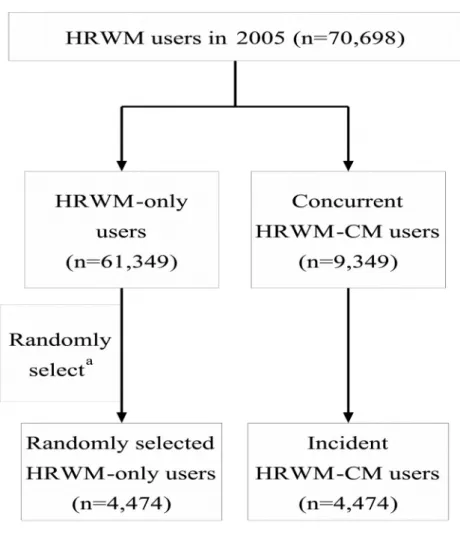
Of the one million NHI beneficiaries randomly sampled in 2005, a total of 70,698 patients ever used at least one of HRWMs. The majority of patients (80.0%) used only one HRWM, and 17.0% received two HRWMs. Among all identified HRWM users, 9,349 (13.2%) used CM simultaneously for at least one day in 2005, and 4,474 (6.3% of the total HRWM users) were incident concurrent users. The average duration of concomitant use was 26.7±43.0 days among all concurrent HRWM-CM users and 18.3±26.0 days among incident HRWM-CM users (Table 1).
Concomitant CM use among warfarin, ticlopidine and aspirin users were more prevalent than the other drugs of HRWM users (Fig. 1). The incidence was 7.7% among warfarin users, 6.8% among ticlopidine users, and 6.5% among aspirin users.
Factors associated with incidence of concurrent HRWM-CM use
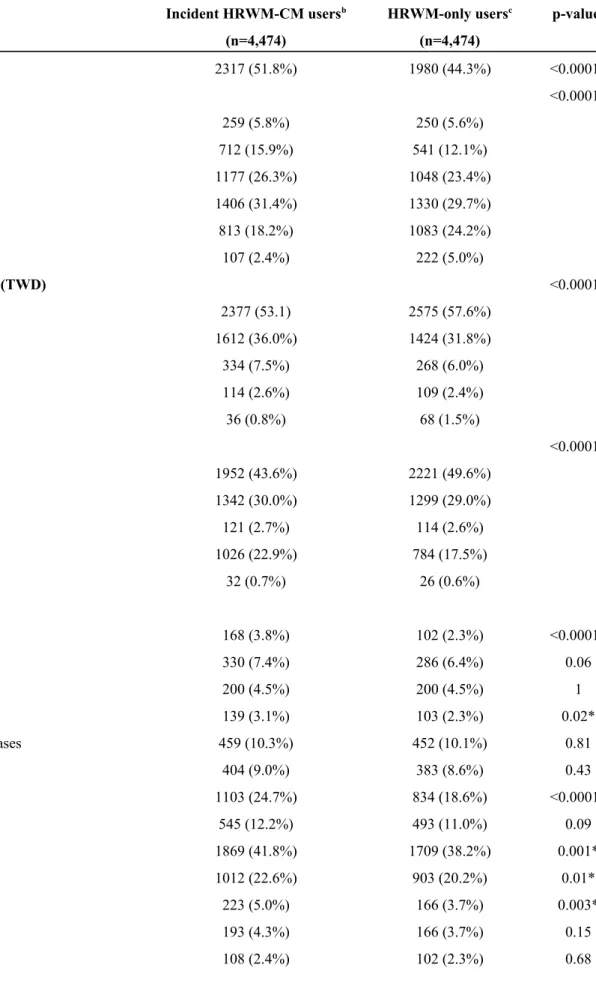
Of the 61,349 HRWM-only users, 4,474 patients were randomly selected (Fig. 2.) as the control group. All these selected patients had the same duration of use in the same month of index date as their corresponding, identified CM concurrent users. Compared with the HRWM-only users, the incident HRWM-CM users were younger, more likely to be female, have middle monthly income, or be enrolled in the NHI program from Central Taiwan. Also, they had a higher prevalence of certain comorbidities (i.e., menopausal symptoms, asthma, arthritis, heart diseases, hyperlipidemia, osteoporosis, schizophrenia, chronic nasal diseases, primary hypertension, and acute respiratory infection, all ps<0.05), and more health service utilization (i.e., outpatient clinic
ps<0.05) (Table 2).
Univariate logistic regression analyses indicated no statistical difference for the following variables between the two groups: liver diseases, renal diseases, chronic respiratory diseases, gout, gastrointestinal ulcers, eczema, other skin diseases, cancer, stroke, diabetes and history of
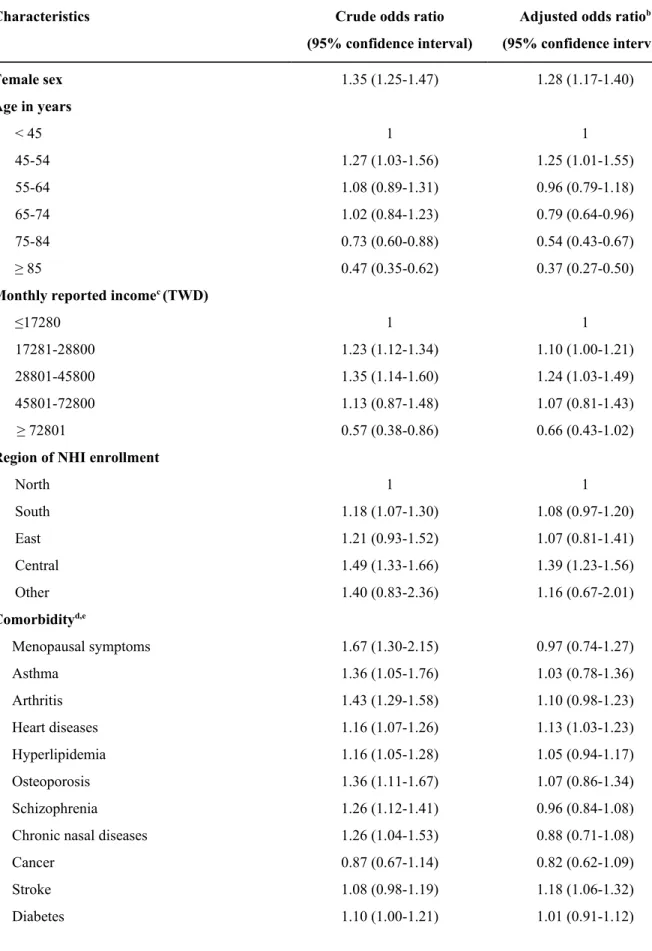
hospitalization. Thus, these variables were not included in the final multivariate model except for those variables represent cancer, stroke, and diabetes. After controlling for the other factors, the following factors were statistically significant, associated with the increasing adjusted ORs of incident HRWM-CM use : female sex, age 45-54 years (compared with age <45 years), middle monthly income (i.e., $17281-45800 New Taiwan dollars (TWD), compared with monthly income $17,280 TWD which was the minimum wage according to the labor regulation), enrollment in Central Taiwan (compared with those enrollment in Northern Taiwan), number of outpatient visits ≥2 times per month (compared with number <2 times per month), number of distinct medications ≥20 (compared with number <20), and a diagnosis of heart diseases, stroke and hypertension (Table 3). As for the extent of these adjusted ORs, for instance, the HRWM users who made two and more outpatient visits per month had 1.66 to 2.66 times of odds to use CM concurrently than those who made less than two outpatient visits, after controlling for the other potential factors. Moreover, those HRWM users with heart diseases, stroke and hypertension had 1.13, 1.18, and 1.11 times of odds, respectively, to use CM concurrently than those who didn’t have these three diseases. In contrast, the factors associated with the lower adjusted ORs of incident HRWM-CM use included: age ≥65 years or total medical expenditure >$50,000 TWD during the 6-month period prior to the index date (compared with expenditure less than $10,000 TWD) (The exchange rate of TWD to USD was 30.86 to 1 on December 31, 2005).
Discussion
In this retrospective population-based cohort study, we found that the prevalence of concurrent HRWM-CM use was approximately 13%, while the incidence was 6% in 2005. Warfarin, ticlopidine or aspirin users were prone to be prescribed with concentrated CM
concurrently. While the factors that statistically significant associated with the incremental incidence of HRWM-CM concurrent use were female, age 45-54 years old, middle monthly income, higher number of outpatient visits or distinct medications prescribed, and previous diagnosis of heart diseases, stroke or hypertension, in contrast, age ≥65 years and medical expenditure higher than $50,000 TWD were associated with a lower incidence of concurrent HRWM-CM use.
The results of this study revealed that approximately one in eight patients using anticoagulants, antiplatelets, or digoxin received concentrated CM concurrently in 2005. This was less than the findings (61.5%) obtained in Chen’s study in 2002 in Taiwan . While current study looks at the prescription and/or refills of specific HRWM and concentrated CM, Chen et al focused on those patients using any kind of Western medication with either prescription or non-prescription CM (including folk herbs). We used the sampling national health insurance database while Chen relied on the self-reported questionnaires in only one medical institute . Further, our study examined those drugs of HRWMs that are commonly used for cardiovascular diseases, including for atrial fibrillation, myocardial infarction, heart failure, and stroke.
Concurrent use of concentrated CM was more prevalent among patients using warfarin than those using other drugs of HRWMs. Some evidence has suggested that using warfarin
concomitantly with certain CAM (e.g., herbal remedies or CM) might increase the risks of adverse events . A cohort study showed that frequent consumption of herbs was associated with suboptimal anticoagulant effects of warfarin in patients with atrial fibrillation . Several clinical case reports have documented the occurrence of bleeding due to the potential interactions between warfarin and CM (i.e., quilinggao, and lycium barbarum) . Nevertheless, the benefits of using anticoagulants and antiplatelets with those blood-activating and stasis-resolving CM (e.g., danshen, dong quai, and turmeric) should be balanced against the potential harms arising from HRWM-CM interactions.
In this study, we found that HRWM users with heart disease, hypertension or stroke were more likely to be prescribed with concentrated CM concomitantly. More specifically, it was found that HRWM users with heart diseases, stroke and hypertension had 1.11 to 1.18 times the risks of using
concentrated CM compared to those who didn’t have these diseases, controlling for other factors. This phenomenon was not observed among patients with other chronic diseases and symptoms (including cancers and diabetes). Although we randomly selected the corresponding HRWM-only users based upon the same duration of HRWM use as incident HRWM-CM concurrent users, more proportion of incident HRWM-CM users had certain types of chronic diseases (including arthritis, hyperlipidemia,osteoporosis, schizophrenia, chronic nasal diseases, acute respiratory infection), other than having heart diseases, stroke and hypertension in the baseline. This phenomenon might infer the possibility to encounter the selection bias while identifying the incident HRWM-CM users. However, the adjusted ORs of using CM were statistically significant bigger only on those HRWM patients with heart diseases, stroke and hypertension, but not for the other comorbidities, after adjusting for other factors. In other words, the findings revealed that those HRWM users with these three comorbidities were more likely to use concentrated CM concurrently, which occurs beyond due to by chance.
In fact, such findings are consistent with previous studies that examined the use of herbal medicine among patients with cardiovascular diseases (prevalence ranging from 7% to 21%) . Several studies have shown that patients with chronic conditions were more likely to use Western medicine with CAM for their illness and ailments . Our findings were partially concordant with the other studies, which found that patients with stroke, hypertension, diabetics, and/or cancer were more frequent users of CAM . In Asia, approximately one-third to half of stroke patients had ever used CAM therapies, including herbal medicine despite limited evidence supporting the benefit of CM (including herbal medicine) among stroke patients .
In addition, age, gender, and geographical locations were associated with a higher incidence of HRWM-CM use in this study. This is consistent with other studies that found that female patients were more likely to use CAM, including dietary supplements and CM . As in other studies , NHI beneficiaries enrolled in the Central Taiwan region were more likely to use concentrated CM concurrently with HRWM. This could be due to the higher density of medical institutes providing both Western medicine and Chinese medicine services located in this region . Our results are also
consistent with the other population-based studies conducted in Taiwan , suggesting that there was a higher incidence of concomitant Western medicine and CM use among the middle-aged population but not among the elderly patients. However, it is still inconclusive about the benefit and risk ratios of using HRWM-CM concurrently among the elderly. In particular, the incidence of concurrent HRWM-CM use among the elderly might be underestimated because those elderly with
cardiovascular diseases might use other complementary and alternative therapies that are not covered by NHI (including non-prescription raw CM products and folk therapies) .
While the earlier study showed that around 86% of patients seeking for the reimbursed TCM therapies were prescribed with concentrated CM in 1996-2001 , another study showed that there was a 15% increasing TCM use in 2003 compared to 1997 using NHIRD . There are many types of folk therapies available in Taiwan, including folk herbs, raw CM products, massage/knead, and spine alignment, other than the reimbursed TCM therapies. However, one national survey revealed that the utilization rate of NHI covered-TCM and non-covered-TCM (i.e., folk therapy) was 10.4% and 7.9%, respectively, among all survey participants . This study also revealed that the
combination rate of Western medications with covered-TCM was 4.3%, while of Western medications with folk therapy was 2.7% . Further, another study using Taiwan’s National Health Interview Survey (NHIS) with NHIRD found that the prevalence of covered-CM and non-covered folk remedies was only 4.95% and 2.16%, respectively, among all survey participants . Therefore, the extent of concurrent use varies from studies to studies due to the different data resources, study designs and focuses of western medications and CM. While the previous studies based on NHIRD only focused on the use of TCM, (ref) some other studies regarding concurrent use were survey study with small samples of participants. (ref) To our knowledge, this is the first study to comprehensively investigate the concurrent use of antiplatelets, anticoagulants and digoxin with concentrated CM in general population. Our study explored the actual prescription patterns of HRWM and CM under one single payer insurance system.
There are a number of limitations in our study. First, this study only focuses on those
but not for all medications with narrow therapeutic ranges. The other types of HRWM, including antiepileptics, antimicrobial agents and immunosuppresives, also have the narrow therapeutic ranges and might be likely to incur undesired effects due to use with CM. We do not take into account these medications in this study due to its relatively less prevalent use among patients with chronic diseases. However, further study to examine the concurrent use patterns of using different types of HRWM with concentrated CM and its consequence is recommended. Second, there is a lack of information about relevant clinical consequences of the concurrent use of concentrated CM with HRWM in current study. In fact, the other study to investigate the consequence of current use of HRWM-CM using the more up-to-date databases is ongoing. Nevertheless, the findings in this study are limited to the exploration but not to examine the causality of concurrent use.
Third, only concentrated CM products prescribed by the TCM physicians are reimbursed by the NHI program and also listed in the available databases. Those concentrated CM products in this study were powder preparations with extracted and concentrated, single CM or mixed CM
formulae. The raw CM products are not covered by NHI and were not included in databases of NHIRD. While only 6.1% of adults had ever used non-covered CAM (including raw CM products) in a national survey and 86% of reimbursed TCM users were prescribed with concentrated CM (i.e., the remaining 14% were treated with covered acupuncture and traumatology manipulative therapies ) , it implies this study described the majority phenomena of TCM use with HRWM among Taiwanese population. Fourth, the duration of concurrent HRWM-CM use should be
interpreted with caution because we did not have information about patients’ compliance, actual use of CM for chronic conditions, or paid out-of-pocket of CM products. Lastly, our findings did not include the other potential factors, e.g., lifestyle factors, which might be also associated with the concurrent use. However, NHIRD is one of the few databases in the world that contain the information on the prescriptions of HRWM and concentrated CM. The findings could reflect the actual prescription patterns in Taiwan and provide evidence for further exploration.
In conclusion, approximately one in eight antiplatelets, anticoagulants, or digoxin users were prescribed with concentrated Chinese medications concurrently among Taiwanese population.
Further research to investigate the clinical outcomes associated with potential interactions between different types of HRWM and different types of CM is needed.
Acknowledgements
The authors express their gratitude to Kathy R. Fox and Sengwee Toh for their insights and comments for the manuscript. This study was supported by the Committee on Chinese medicine and Pharmacy, Department of Health, Executive Yuan, Taiwan, R.O.C. (grant number CCMP99-RD-016) and partially supported by National Science Council (NSC 99-2320-B-039-031-MY3). The research database was based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
Conflict of interest
Box 1 Illustration for the acronyms commonly used in this study
Acronym Term Definition
CAM Complementary
and alternative medicine
“A group of diverse medical and health care systems, practices, and products that are not generally considered part of conventional medicine, which including natural products, mind and body medicine, and manipulative and body-based practices.” . In particular, those terms of Traditional Chinese medicine, Chinese medications, and herbal medicine used in this study are part of natural products as in Complementary and Alternative Medicine.
TCM Traditional
Chinese medicine
“Traditional Chinese medicine (TCM) practitioners use herbs, acupuncture, and other methods to treat a wide range of conditions” for their patients . In this study, TCM include those therapies which are covered by National Health Insurance in Taiwan (e.g., Concentrated CM products, acupuncture, and traumatology manipulative therapies, etc.) and non-covered therapies (e.g., crude herbal medicine, massage/knead, and spine alignment, etc.).
CM Chinese
medications
Medications derived from the TCM theories and used to treat ailments or maintain the health status. The Chinese medication is known as an ancient form of medication. Those CM products could be concentrated powder, raw herbs, dry animal or mineral for decoction.
HRWM High-risk Western
medications
High-risk Western medications (HRWM), which might be those medications prone to adverse drug reactions or result in ineffective treatments due to their narrow therapeutic ranges or drug-interactions. In this study, we only focus on antiplatelet drugs (aspirin, clopidogrel, dipyridamole, ticlopidine), anticoagulants (heparin, warfarin), and digoxin.
Table 1 Duration of concurrent use in days of high-risk Western medications and Chinese
Medications
HRWMa
All concurrent HRWM-CM usersb Incident HRWM-CM usersc
N=9,349 N=4,474
Mean ± standard deviation (days)
Median (IQR) (days)
Mean ± standard deviation (days) Median (IQR) (days) Total 26.7 ± 43.0 11 (22) 18.3 ± 26.0 8 (13) Anticoagulant 31.5 ± 46.3 14 (27) 20.4 ± 27.9 12 (18) Heparin 40.0 ± 79.3 11 (29) 36.8 ± 22.4 34 (5) Warfarin 30.9 ± 43.8 14 (27) 20.0 ± 27.9 12 (17) Antiplatelet 26.3 ± 42.7 11 (21) 18.0 ± 25.5 8 (13) Aspirin 25.7 ± 40.4 12 (21) 17.8 ± 24.8 8 (13) Clopidogrel 30.6 ± 50.1 12 (24) 16.7 ± 23.7 7 (10) Dipyridamole 23.6 ± 41.7 7 (18) 17.7 ± 26.7 7 (12) Ticlopidine 26.2 ± 44.7 10 (20) 15.0 ± 16.3 7 (12) Digoxin 26.5 ± 39.4 12 (22) 19.3 ± 29. 9 8 (13)
HRWM: high-risk Western medications; CM: Chinese Medications; IQR: interquartile range.
a Outpatients who were prescribed or dispensed the designated anticoagulants, antiplatelets, or
digoxin at least once in 2005.
b HRWM users who were prescribed CM concurrently in the year of 2005.
c HRWM-CM users without prior CM prescription during the 6-month period prior to the date of the
Table 2 Comparison of patient characteristics between incident HRWMa-CM users and
HRWM-only users
Characteristics Incident HRWM-CM usersb
(n=4,474) HRWM-only usersc (n=4,474) p-valued Female 2317 (51.8%) 1980 (44.3%) <0.0001* Age in years < 45 45-54 55-64 65-74 75-84 ≥ 85 259 (5.8%) 712 (15.9%) 1177 (26.3%) 1406 (31.4%) 813 (18.2%) 107 (2.4%) 250 (5.6%) 541 (12.1%) 1048 (23.4%) 1330 (29.7%) 1083 (24.2%) 222 (5.0%) <0.0001*
Monthly reported incomee (TWD)
≤17280 17281-28800 28801-45800 45801-72800 ≥ 72801 2377 (53.1) 1612 (36.0%) 334 (7.5%) 114 (2.6%) 36 (0.8%) 2575 (57.6%) 1424 (31.8%) 268 (6.0%) 109 (2.4%) 68 (1.5%) <0.0001*
Region of NHI enrollment
North South East Central Other 1952 (43.6%) 1342 (30.0%) 121 (2.7%) 1026 (22.9%) 32 (0.7%) 2221 (49.6%) 1299 (29.0%) 114 (2.6%) 784 (17.5%) 26 (0.6%) <0.0001* Comorbidityf Menopausal symptoms Liver diseases Renal diseases Asthma
Chronic respiratory diseases Gout Arthritis Gastrointestinal ulcers Heart diseases Hyperlipidemia Osteoporosis Eczema
Other skin diseases
168 (3.8%) 330 (7.4%) 200 (4.5%) 139 (3.1%) 459 (10.3%) 404 (9.0%) 1103 (24.7%) 545 (12.2%) 1869 (41.8%) 1012 (22.6%) 223 (5.0%) 193 (4.3%) 108 (2.4%) 102 (2.3%) 286 (6.4%) 200 (4.5%) 103 (2.3%) 452 (10.1%) 383 (8.6%) 834 (18.6%) 493 (11.0%) 1709 (38.2%) 903 (20.2%) 166 (3.7%) 166 (3.7%) 102 (2.3%) <0.0001* 0.06 1 0.02* 0.81 0.43 <0.0001* 0.09 0.001* 0.01* 0.003* 0.15 0.68
Schizophrenia Chronic nasal diseases Cancer
Stroke Diabetes
Primary hypertension Acute respiratory infection
771 (17.2%) 246 (5.5%) 107 (2.4%) 1083 (24.2%) 1224 (27.4%) 1937 (43.3%) 2850 (63.7%) 635 (14.2%) 197 (4.4%) 122 (2.7%) 1023 (22.9%) 1143 (25.6%) 1719 (38.4%) 2264 (50.6%) <0.0001* 0.02* 0.32 0.13 0.05 <0.0001* <0.0001*
Outpatient clinic visits per monthf
< 2 2-<3 3-<4 4-<5 5-<6 ≥ 6 597 (13.3%) 1365 (30.5%) 1018 (22.8%) 568 (12.7%) 403 (9.0%) 523 (11.7%) 1252 (28.0%) 1424 (31.8%) 854 (19.1%) 414 (9.3%) 237 (5.3%) 293 (6.6%) <0.0001*
Number of prescribed, distinct medicationsf
< 20 20-39 40-59 60-79 ≥ 80 625 (14.0%) 1145 (25.6%) 1336 (29.9%) 916 (20.5%) 452 (10.1%) 1142 (25.5%) 1660 (37.1%) 1078 (24.1%) 456 (10.19%) 138 (3.1%) <0.0001* History of hospitalizationf 700 (15.7%) 691 (15.4%) 0.79
Total medical expendituref (TWD)
< 10000 10001-29999 30000-49999 ≥ 50000 880 (19.7%) 2222 (49.7%) 691 (15.4%) 681 (15.2%) 1173 (26.2%) 2072 (46.3%) 583 (13.0%) 646 (14.4%) <0.0001*
HRWM: high-risk Western medications; CM: Chinese Medications; SD: standard deviation; IQR: interquartile range; NHI: National Health Insurance; TWD: New Taiwan dollar (Exchange rate of TWD to USD was 30.86 to 1 on December 31, 2005).
a Outpatients who were prescribed or dispensed the designated antiplatelets, anticoagulants, or
digoxin at least once in 2005.
b Concurrent high-risk Western medications and Chinese Medications users without prior CM
prescription during the 6-month period prior to the date of the first CM use.
selected one HRWM-only user from the month of the index date who had the same duration of HRWM use.
d We used chi-square tests to compare the differences between incident HRWM-CM users and
HRWM-only users.
e We identified monthly reported income based on patients’ monthly insurance and categorized it
upon NHI registration and enrollment records.
Table 3 Factors associated with incident concurrent use of high-risk Western medicationsa
and Chinese Medications
Characteristics Crude odds ratio
(95% confidence interval)
Adjusted odds ratiob
(95% confidence interval) Female sex 1.35 (1.25-1.47) 1.28 (1.17-1.40) Age in years < 45 45-54 55-64 65-74 75-84 ≥ 85 1 1.27 (1.03-1.56) 1.08 (0.89-1.31) 1.02 (0.84-1.23) 0.73 (0.60-0.88) 0.47 (0.35-0.62) 1 1.25 (1.01-1.55) 0.96 (0.79-1.18) 0.79 (0.64-0.96) 0.54 (0.43-0.67) 0.37 (0.27-0.50)
Monthly reported incomec (TWD)
≤17280 17281-28800 28801-45800 45801-72800 ≥ 72801 1 1.23 (1.12-1.34) 1.35 (1.14-1.60) 1.13 (0.87-1.48) 0.57 (0.38-0.86) 1 1.10 (1.00-1.21) 1.24 (1.03-1.49) 1.07 (0.81-1.43) 0.66 (0.43-1.02)
Region of NHI enrollment
North South East Central Other 1 1.18 (1.07-1.30) 1.21 (0.93-1.52) 1.49 (1.33-1.66) 1.40 (0.83-2.36) 1 1.08 (0.97-1.20) 1.07 (0.81-1.41) 1.39 (1.23-1.56) 1.16 (0.67-2.01) Comorbidityd,e Menopausal symptoms Asthma Arthritis Heart diseases Hyperlipidemia Osteoporosis Schizophrenia Chronic nasal diseases Cancer Stroke Diabetes 1.67 (1.30-2.15) 1.36 (1.05-1.76) 1.43 (1.29-1.58) 1.16 (1.07-1.26) 1.16 (1.05-1.28) 1.36 (1.11-1.67) 1.26 (1.12-1.41) 1.26 (1.04-1.53) 0.87 (0.67-1.14) 1.08 (0.98-1.19) 1.10 (1.00-1.21) 0.97 (0.74-1.27) 1.03 (0.78-1.36) 1.10 (0.98-1.23) 1.13 (1.03-1.23) 1.05 (0.94-1.17) 1.07 (0.86-1.34) 0.96 (0.84-1.08) 0.88 (0.71-1.08) 0.82 (0.62-1.09) 1.18 (1.06-1.32) 1.01 (0.91-1.12)
Characteristics Crude odds ratio (95% confidence interval)
Adjusted odds ratiob
(95% confidence interval)
Primary hypertension Acute respiratory infection
1.22 (1.12-1.33) 1.71 (1.57-1.86)
1.11 (1.02-1.22) 1.07 (0.97-1.18)
Outpatient clinic visits per monthe
< 2 2-<3 3-<4 4-<5 5-<6 ≥ 6 1 2.01 (1.78-2.27) 2.50 (2.19-2.86) 2.88 (2.45-3.36) 3.57 (2.96-4.30) 3.74 (3.15-4.45) 1 1.66 (1.45-1.89) 1.91 (1.63-2.23) 2.27 (1.87-2.75) 2.86 (2.28-3.57) 2.66 (2.11-3.35)
Number of distinct medications prescribede
< 20 20-39 40-59 60-79 ≥ 80 1 1.26 (1.11-1.43) 2.27 (2.00-2.57) 3.67 (3.16-4.26) 5.99 (4.83-7.41) 1 1.41 (1.24-1.61) 2.23 (1.95-2.54) 3.22 (2.75-3.78) 4.06 (3.19-5.16)
Total medical expendituree (TWD)
< 10000 10001-29999 30000-49999 ≥ 50000 1 1.43 (1.29-1.59) 1.58 (1.37-1.82) 1.41 (1.22-1.61) 1 1.06 (0.94-1.19) 0.84 (0.71-1.00) 0.70 (0.59-0.84)
NHI: National Health Insurance; TWD: New Taiwan Dollar.
a Outpatients who were prescribed or dispensed the designated antiplatelets, anticoagulants, or
digoxin at least once in 2005.
b Adjusted for all other variables in the table.
c We identified monthly reported income based on patients’ monthly insurance and
categorized it upon NHI registration and enrollment records.
d For each comorbidity, not having the diagnosis was used as the reference.
e Ascertained during the 6-month period prior to the date of first Chinese medications
Fig. 1 Incidence and prevalence of concurrent use of high-risk Western medications
(HRWM)a and Chinese Medications
a Outpatients who were prescribed or dispensed the designated antiplatelets, anticoagulants, or
Fig. 2 Flow chart of study population
HRWM: high-risk Western medications; CM: Chinese Medications.
a For each incident HRWM-CM user, we randomly selected one HRWM-only user from the