Applying HFMEA to Prevent Chemotherapy Errors
1Chia-Hui Cheng, MS; 2Chia-Jen Chou, PhD; 3–5Pa-Chun Wang, MD, MSc; 6Hsi-Yen
Lin, MS; 6Chi-Lan Kao, BA; 2Chao-Ton Su, PhD
1Quality Management Center, Cathay General Hospital, Taipei, Taiwan
2Department of Industrial Engineering and Engineering Management, National Tsing
Hua University, Hsinchu, Taiwan
3Department of Otolaryngology, Cathay General Hospital, Taipei, Taiwan
4School of Medicine, Fu Jen Catholic University, Taipei County, Taiwan
5Department of Public Health, College of Public Health, China Medical University,
Taichung, Taiwan
6Department of Pharmacy, Cathay General Hospital, Taipei, Taiwan
Word Count: 1,677
Correspondence:
Chao-Ton Su, PhD
Department of Industrial Engineering and Engineering Management, National Tsing Hua University
Address: 820 Room, Engineering Building I, 101, Section 2, Kuang-Fu Road, Hsinchu 300, Taiwan
Telephone: 8863-5742936 FAX: 8863-5722204
ABSTRACT
Background: To evaluate risk and vulnerability in the chemotherapy process using a
proactive risk analysis method.
Methods: Healthcare failure mode and effect analysis (HFMEA) was adopted to
identify potential chemotherapy process failures. A multidisciplinary team is formed to identify, evaluate, and prioritize potential failure modes based on a chemotherapy process flowchart. Subsequently, a decision tree is used to locate potential failure modes needing urgent improvement. Finally, some recommended actions are generated and executed to eliminate possible risks.
Results: A total of 11 failure modes were identified with high hazard scores.
Computerized physician order entry was adopted to eliminate potential risks in chemotherapy processes. Chemotherapy prescription errors significantly decreased from 3.34% to 0.40%.
Conclusion: Chemotherapy is regarded as a high-risk process. Multiple errors can
occur during ordering, preparing, compounding, dispensing, and administering medications and lead to serious consequences. HFMEA is a useful tool to evaluate potential risk in healthcare processes.
Keywords: healthcare failure mode and effect analysis (HFMEA), chemotherapy
INTRODUCTION
The chemotherapy process is regarded as potentially risky for patients because of complex processes, multiple drug uses, dangerous compounds, and high utilization rates in outpatient departments. Chemotherapy is commonly administered as an infusion of a potent and potentially toxic drug solution. Doses are computed based on body weight or other factors and are usually adapted to body surface area or renal function of patients. Errors in multiple-dose administration can result in catastrophic reaction or death.[1] Some chemotherapy errors occur because of understaffing, poor communication, human error, fatigue, or environmental factors.[2] Possible errors listed by Schulmeister [3] include underdosing and overdosing, scheduling and timing errors, administering incorrect drugs or hydration, improperly preparing drugs, and giving chemotherapy to the wrong patient. For patient safety, an effective risk analysis method to reduce error rates of the chemotherapy process should be prioritized in medical clinics and hospitals.
Chemotherapy errors affect patient health and should not be ignored. According to Greenall, [4] chemotherapy ordering, preparing, dispensing, and administering are highly connected and susceptible to errors. Hence, recognizing and preventing
potential failure modes in the chemotherapy process are priority missions. Our research hospital collected data from 22,550 inpatient and outpatient prescriptions (from 2007 to 2009) and found a chemotherapy prescription error rate of 3.34%. Although most adverse effects were near-miss events, the chemotherapy process is considered a high-alert medication process and requires an effective proactive risk analysis method to avoid errors. Failure mode and effect analysis (FMEA) is a systematic and prospective risk evaluation method initially adopted in the industrial field, and its administration outcomes are excellent. Recently, the concept of risk prevention was adopted in the healthcare arena (HFEMA) and is used to reduce medication errors.
FMEA has been widely used by engineers to improve reliability, quality, and safety of their products and to reduce potential risks.[5,6] The most important function of FMEA is to identify potential failure modes for each subsystem or component. A risk priority number (RPN) is determined by multiplying three risk parameters in the following formula: RPN = S × O × D, where S indicates severity rate; O, occurrence rating; and D, detection rating.
In 2000, the US Joint Commission on Accreditation of Healthcare Organizations (JCAHO) promoted HFMEA in their prospective analysis of healthcare processes to
prevent possible medication errors. Since 2002, the JCAHO has requested its
subordinate medical institutions to analyze at least one high-risk medical process per year. [7] Prospective risk analysis was subsequently popularized in medical
operations.[8,9] Risk evaluation indexes used in FMEA were substantially modified for HFMEA. Hazard scores are used in HFMEA to prioritize failure modes and to determine recommended actions based on decision tree analysis.
METHODS
Study Design
This study applied HFMEA to the chemotherapy process at Cathay General Hospital, a 600-bed university-affiliated medical center located in downtown Taipei, Taiwan. The research hospital expected significant reduction in chemotherapy prescription errors through adoption of preventive actions.
Duration
Implementation of HFMEA began in July 2007 with formation of the HFMEA team. Monthly meetings were conducted lasting approximately 1½ hours. The entire
project involved 12 meetings comprising more than 140 hours.
HFMEA Application
Team
An eight-member multidisciplinary team was formed to implement HFMEA. With a medical vice-superintendent as the project leader, the team comprised individuals from the quality management center, cancer prevention committee, and relevant departments, including information technology, nursing, and pharmacy. The team was supervised by two external process engineers from National Tsing Hua University, Hsinchu, Taiwan.
Procedure
HFMEA includes the following 5 key steps: (1) define the HFMEA topic, (2) assemble the team, (3) graphically describe the process, (4) conduct a hazard analysis, and (5) perform recommended actions and outcome measures.
Process Map
A process map (Figure 1) split the chemotherapy process into inpatient and outpatient components, and only one difference was found to exist. In the outpatient setting, prepared medication does not need to be transported to patients because the administration room is next to the preparation room.
Baseline HFMEA
The HFMEA team discussed the inpatient and outpatient chemotherapy
processes in detail and analyzed the severity and probability of each failure mode to determine recommended actions. Table 1 summarizes the decision tree used to determine whether recommended actions were necessary.
By brainstorming, the HFMEA team summarized 15 potential causes that could result in seven failure modes in the inpatient process. Similarly, the team identified 11 potential causes that could result in four failure modes in the outpatient process. Results of the decision tree showed nine potential causes that must be addressed. Figure 2 shows the potential causes that needed correction or prevention. The team submitted the following three recommended actions to hospital management for
approval: (1) to adopt an appropriate computerized physician order entry (CPOE) system, (2) to use radiofrequency identification (RFID) or bar codes in verifying patients and medications, and (3) to construct an automatic alert system for detecting medication exosmosis.
Top management selected CPOE as the initial improvement campaign. Because of finite resources and possible ward renovation, RFID and the automatic alert system will be considered in the future.
Recommended CPOE System
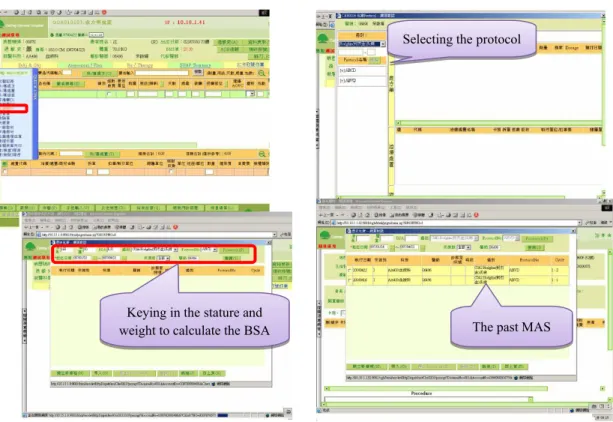
The CPOE system prototype was built in March 2008, with 1-month pilot testing. Based on end user requirements, the system had to perform the following: (1) check the past medication administration sheet, (2) calculate the dosage of
medications based on body surface area, (3) search the laboratory information system to provide liver or renal function insufficiency alerts, and (4) automatically show medication quantity (vial, ampule, or pill) on the basis of required dosages.
The formal CPOE system was released in April 2008, when its accompanying user manual was delivered. All physicians were required to establish their
chemotherapy protocols. Handwritten prescriptions for chemotherapy were prohibited, and all chemotherapy orders had to go through the system. HFMEA hazard scores were reassessed 6 months after CPOE implementation. Because of limited CPOE approval by top management, the reassessment considered only potential causes of failure modes.
The CPOE system checks the past medication administration sheet, selects a protocol, and automatically calculates body surface area and dosages. Interfaces are shown in Figure 3. Also incorporated is a liver and renal alert system to remind prescribing physicians about patient functions and prevent overdosing.
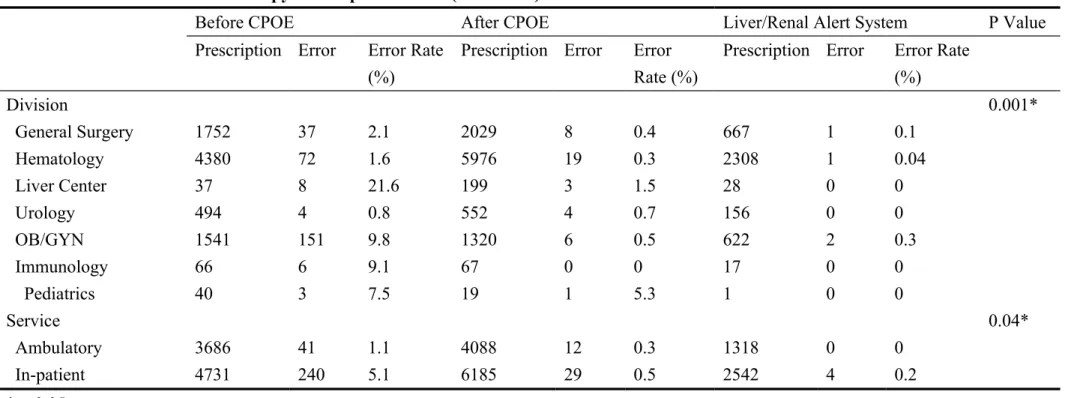
CPOE significantly decreased the chemotherapy error rate from 3.34% (95% confidence interval [CI], 2.91–3.69) to 0.40% (95% CI, 0.28–0.52) (p<0.05). The improvement affirms the effectiveness of the CPOE system in reducing medication errors. Table 2 summarizes the reduction in chemotherapy prescription errors.
DISCUSSION
The chemotherapy process starts with prescription, dispensation, and delivery and ends with administration, and each step sustains high risk of significant patient
harm, which can be lethal. Some studies[10–12] report chemotherapy error rates ranging from 0.45% to 15%, with a mean error rate of 3.34% for research hospitals before improvement is initiated. Introduction of a CPOE system decreased the error rate from 15% to 5% (compared with an error rate of 13.5% for handwritten
prescriptions) in one study.[10] In 2003, the Institute for Safe Medication Practices[13] reported that cancer chemotherapy tops the list of high-alert medications, outranking intravenous potassium chloride and insulin as potential threats to patient safety. The volume of patients with cancer and the repetition of chemotherapy-related adverse events prompted research hospitals to prioritize chemotherapy process safety and to adopt immediate amendment.
In the summer of 2001, the Veterans Affairs National Center for Patient Safety
[14] reviewed the FMEA system broadly used in engineering and modified it for
healthcare. HFMEA is a proactive analysis tool to systematically calculate potential process risks using a two-variable equation. Since then, the JCAHO Standard LD.5.2 requires facilities to select at least one high-risk process for proactive risk assessment each year. It is uniformly agreed that HFMEA is a useful tool for systematic analysis, prioritization of recommended actions, and identification of unrecognized errors.[15– 19] However, few effects of HFMEA were reported in those studies, with most
describing applications of the tool and not focusing on improvement actions generated.
In 1996, the American Society of Health-System Pharmacists [20]proposed the
following seven measures to prevent medication errors in cancer chemotherapy: educate healthcare providers, verify the dose, establish dosage limits, standardize the prescribing vocabulary, work with drug manufacturers, educate patients, and improve communication. In the past, verifying the dose, establishing dosage limits, and
standardizing the prescribing vocabulary depended on healthcare personnel (physicians, pharmacists, and nurses) to prevent error. With the advancement of healthcare information technology, hardware and software became available for healthcare organizations to facilitate a safe environment for patients. Studies have demonstrated the progress and effect of computerization in reducing chemotherapy error rates. According to Voeffray et al, [10] errors decreased from 15% (141 of 940) to 5% (75 of 1505) after implementation of CPOE, with a 13.1% error rate for
handwritten prescriptions (22-fold higher than the error rate for computerized
prescriptions). After CPOE deployment in pediatric oncology, Kim et al [21] reported a significant reduction the overall error rate, with fewer daily chemotherapy orders having improper dosing, incorrect dosage calculations, missing cumulative dose
calculations, and incomplete nursing checklists.
The chemotherapy process at our hospital used to comprise several risky procedures, including human key-in error, incorrect dosing calculation, and reliance on personnel to prevent errors. With application of HFMEA and a dedicated
multidisciplinary team, our hospital identified potential risks, although there were some difficulties in applying this tool. For example, a couple of months were required to complete the initial analysis and longer to implement the recommended actions. Moreover, consensus was sometimes difficult to reach among team leadership from different disciplines. Changing a work process (especially moving from handwritten to computerized orders) can elicit strong negativity from physicians and lead to increased errors during the learning curve. Despite these difficulties, HFMEA effectively reduced chemotherapy errors at our hospital.
In conclusion, the complexity of chemotherapy renders it vulnerable to error, and the consequences can be catastrophic. With introduction of HFMEA and CPOE, we reduced the chemotherapy prescription error rate at our hospital from 3.34% to 0.40%. HFMEA is a useful tool to evaluate potential risk in healthcare processes, and CPOE is an effective technology to prevent human error.
REFERENCES
1. Dizon, D. S., Sabbatini, P. J., Aghajanian, C., Hensley, M. L., Spriggs, D. R., Analysis of patients with epithelial ovarian cancer of fallopian tube carcinoma retreated with cisplatin after development of a carboplatin allergy. Gynecol Oncol 82:378–82, 2002.
2. Sheridan-Leos, N., Schulmeister, L., Hartranft, S., Failure mode and effect
analysis: a technique to prevent chemotherapy errors. Clin J Oncol Nurs 10:393–398, 2006.
3. Schulmeister, L., Chemotherapy medication errors: description, severity, and contributing factors. Oncol Nurs Forum 26:1033–1042,1999.
4. Greenall, J., Failure modes and effects analysis: a tool for identifying risk in community pharmacies. Can Pharm J 140:191–193, 2007.
5. Roland, H. E., Moriarity, B., System Safety Engineering and Management. Hoboken, NJ: John Wiley & Sons Inc, 1990.
6. Teoh, P. C., Case, K., An evaluation of failure modes and effect analysis generating method for conceptual design. Int J Comput Integr Manuf 18:279–93, 2005.
7. Joint Commission on Accreditation on Healthcare Organization. Revisions to Joint Commission Standards in Support of Patient Safety and Medical/Health Care Error Reduction. Oakbrook Terrace, IL: Joint Commission on Accreditation on Healthcare Organization, 2002.
8. Hambleton, M., Applying root cause analysis and failure mode and effect analysis to our compliance programs. J Health Care Compliance 7:5–13, 2005.
9. Kunac, D. L., Reith, D. M., Identification of priority for medication safety in neonatal intensive care. Drug Saf 28:251–261, 2005.
10. Voeffray, M., Pannatier, A., Stupp, R., Fucina, N., Leyvraz, S., Wasserfallen, J. B.,
Effect of computerisation on the quality and safety of chemotherapy prescription. Qual Saf Health Care 15:418–421, 2006.
11. Markert A, Thierry V, Kleber M, et al. Chemotherapy safety and severe adverse events in cancer patients: strategies to efficiently avoid chemotherapy errors in in- and outpatient treatment. Int J Cancer 2009;124:722–820.
12. Bonnabry, P., Cingria, L., Ackermann, M., Behrens, M., Engelhardt,M.,Use of a
prospective risk analysis method to improve the safety of the cancer chemotherapy process. Int J Qual Health Care 18:9–16, 2006.
13. American Society of Health-System Pharmacists. ASHP guidelines on preventing medication errors with antineoplastic agents. Am J Health Syst Pharm 59:1648–1668, 2002.
14. DeRosier, J., Stalhandske, E., Bagian, J. P., Nudell, T., Using health care failure mode and effect analysis: the VA national center for patient safety’s prospective risk analysis system. Jt Comm J Qual Improv 28:248–267, 2002.
15. Habraken MM, Van der Schaaf TW, Leistikow IP, et al. Prospective risk analysis of health care processes: a systematic evaluation of the use of HFMEA in Dutch health care. Ergonomics 2009;52:809–819.
16. Kimehi-Woods, J., Shultz, J. P.,Leistikow, I. P., Reijnders-Thijssen, P. M., Using
HFMEA to assess potential for patient harm from tubing misconnections. Jt Comm J Qual Patient Saf 32:373–381,2006.
17. van Tilburg, C. M., Leistikow, I. P., Rademaker, C. M., Bierings, M. B., van Dijk,
A.T., Health care failure mode and effect analysis: a useful proactive risk analysis in a
pediatric oncology ward. Qual Saf Health Care 15:58–63, 2006.
18. Esmail, R., Cummings, C., Dersch, D., Duchscherer, G., Glowa, J., Liggett, G.,
Patient Safety and Adverse Events Team. Using health care failure mode and effect
analysis tool to review the process of ordering and administrating potassium chloride and potassium phosphate. Healthc Q 8:73–80, 2005.
19. Linkin DR, Sausman C, Santos L, Lyons, C., Fox, C., Aumiller, L., Applicability
of health care failure mode and effect analysis to healthcare epidemiology: evaluation of the sterilization and use of surgical instruments. Clin Infect Dis 41:1014–1019, 2005.
20. Cohen, M. R., Anderson, R. W., Attilio, R. M., Green, L., Muller, R.J., Pruemer JM. Preventing medication errors in cancer chemotherapy. Am J Health Syst Pharm 53:737–746, 1996.
21. Kim, G. R., Chen, A. R., Arceci, R. J., Mitchell, S. H., Kokoszka, K. M., Daniel, D., Error reduction in pediatric chemotherapy computerized order entry and failure modes and effects analysis. Arch Pediatr Adolesc Med 160:495–498, 2006.
FIGURE LEGENDS
Figure 1. Inpatient Chemotherapy Process
Figure 2. Potential Causes of Failure Modes in the Inpatient Chemotherapy Process Figure 3. CPOE System Interfaces
Prescription Dispensing
1 2
Subprocesses:
A. Checking the patient’s medical record
a. Checking the patient’s hypersensitivity history b. Checking the chemotherapy schedule
B. Patient’s regular examination
a. Measuring weight and stature (to calculate the BSA)
b. Drawing blood for inspecting (CBC, LFT) c. Examining Hepatitis B surface Antigen
(HBsAg) and antibody to the hepatitis C virus (Anti-HCV) of the first-time receiving chemotherapy patient
C. Creating a bipartite prescription (medicine type, dosage, administration way, time, lacquer thinner)
D. Keying the computerized prescription
a. Keying the bed number, patient’s ID, medicine name, dosage, time
b. Checking if the prescription matches doctor’s order
E. Sending the prescription to the pharmacy a. The pharmacist signs after receiving the
prescription
Subprocesses:
A. Checking the medication administration sheet (MAS) of patient
B. Reconfirming the prescription
a. Checking if the prescription is complete b. Checking the patient’s basic information (bed
number, date, doctor’s autograph, medicine, quantity)
c. Attaching the standard operation process of chemotherapy prescription
d. Noting the administration date, medicine name, dosage, administration days, and administration frequency, and writing these details in the blank space of the doctor’s order
e. Keying the prescription into the computer and printing out the label
C. Preparing the medicine
a. Sticking the label on the prescription bag b. Preparing the correct medicine (withdraw
packing) and cartridge
c. Checking if a warning is advanced (No IV push) d. Checking if the Non-PVC set & filter are required e. Filling-in the consumption materials sheet
D. Drawing the medicine
a. Checking if the patient name, prescription, medicine, cartridge, solubility fluid, and label correspond with the original prescription b. Confirming the medicine dosage, volume, and
administration date
c. Examining the standard asepsis operation process d. Checking that medicine fluid in cartridge is pure
and without any foreign matter
e. Sticking the label and pack into prescription bag E. Reconfirming the medicine
a. Checking the patient’s basic information including administration date, bed number, medicine, dosage, volume, foreign matter, an warning labels (No IV push)
b. Checking if the inside label corresponds with the outside label, then closing the protecting cover and ensuring the absence of leakage
F. Packing the medicine a. Sealing the prescription bag
b. Writing down the date and bed number on the box and filling-in the signature sheet
Transportion Adminstration
3 4
Subprocesses:
A. Placing transport requirement by phone B. Receiving the medicine
a. Signing after receiving medicine C. Transport
Subprocesses:
A. Checking the doctor’s order
a. Writing on the administration record, medicine plate, and intravenous injection plate; double checking by another nurse; those two nurses will sign on the record
b. Understanding the administration process and matters that need attention
B. Preparing the medicine
a. Preparing the require items: general set, precise set, IV pump, and others
b. Pre-C/T: drawing medicine after checking c. Intravenous drip: preparing on the basis of the
doctor’s order
d. Chemotherapeutic medicine: chemotherapy team compounding the medicine based on standard operation process and returning to the administration unit
C. Staff protection measures
a. Using the isolation suit, active carbon respirator, goggles, and gloves
D. Administration
a. Before adding another chemotherapy medicine, it is require inspecting for blood backflow, red and swollen, and exosmosis occurring in port-A or IV cath
b. Two nurses go to patient unit and administer the medicine after confirming patient ID
c. If the administration is by intravenous drip, reconfirm whether the chemotherapy medicine is already added or not
E. Observing and recording
a. For patients who are in keep line’s, check for blood backflow, red and swollen, and exosmosis occurring in port-A or IV cath; checking
frequency is on the basis of a three-shift working system; results must be marked on the nursing record
b. Reinforcing attention to the patient receiving chemotherapy medication
Dispensing g
1 2 3 4
Prescription Transportion Adminstration
1CI- The handwriting of prescription is blurred
1DI- There are versions of computerized
prescriptions and each version is different
1DII- The previous data was not deleted and was easily confused with the newest data 1DIII- Personal key in
error
2BeI- The decimal point key in error
2BeII- When calculating the required dosage, the staff fills in wrong data 2BeIII- The mistake of
seeing the wrong decimal point
2BeIV- The staff is getting the incorrect total amount of medicines
3BaI- The transporter takes multiple medicines simultaneously and allots them to the incorrect sickroom
4DbI- The process is complicate and difficult to execute 4DbII- Because of too many
affairs, the staff forgets to verify vital information before administrating medication 4EI- The staff leaves immediately
after injecting medicine and does not monitor the condition of patient
4EII- Over the span of time of injecting medicine, exosmosis occurred
4EIII-Exosmosis occurred because the patient turned around
Figure 3. CPOE System Interfaces
Selecting the protocol Selecting the protocol
Keying in the stature and weight to calculate the BSA
Keying in the stature and
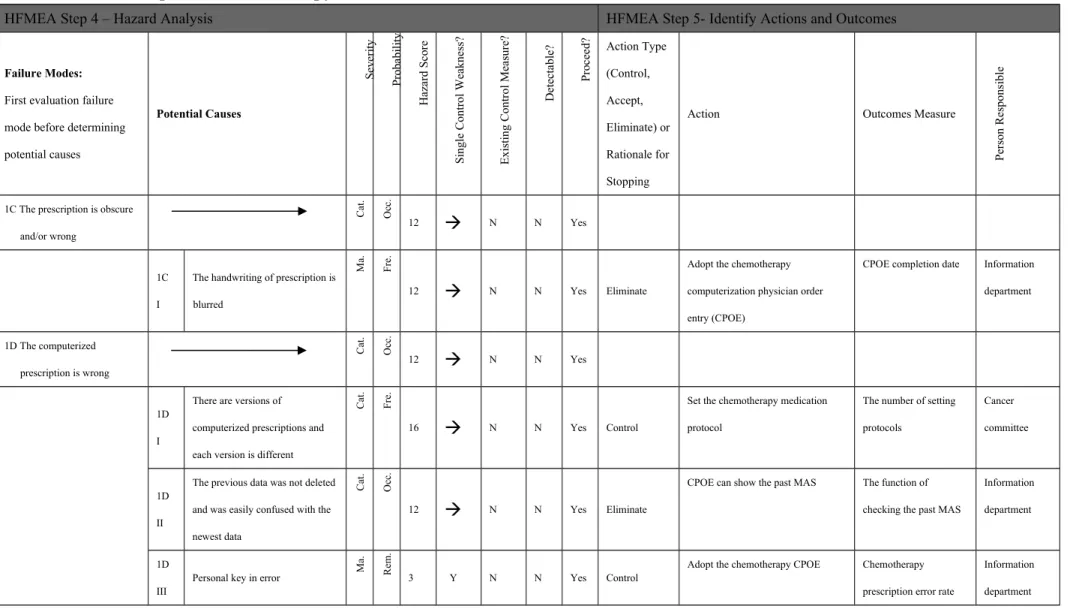
Table 1. HFMEA Inpatient Chemotherapy Process Decision Tree
HFMEA Step 4 – Hazard Analysis HFMEA Step 5- Identify Actions and Outcomes
Failure Modes:
First evaluation failure mode before determining potential causes Potential Causes Se ve ri ty Pr ob ab il ity H az ar d Sc or e Si ng le C on tr ol W ea kn es s? E xi st in g C on tr ol M ea su re ? D et ec ta bl e? Pr oc ee d? Action Type (Control, Accept, Eliminate) or Rationale for Stopping
Action Outcomes Measure
Pe rs on R es po ns ib le
1C The prescription is obscure and/or wrong C at . O cc . 12 N N Yes 1C I
The handwriting of prescription is blurred M a. F re . 12 N N Yes Eliminate
Adopt the chemotherapy computerization physician order entry (CPOE)
CPOE completion date Information department 1D The computerized prescription is wrong C at . O cc . 12 N N Yes 1D I
There are versions of computerized prescriptions and each version is different
C at . F re . 16 N N Yes Control
Set the chemotherapy medication protocol
The number of setting protocols
Cancer committee
1D II
The previous data was not deleted and was easily confused with the newest data C at . O cc . 12 N N Yes Eliminate
CPOE can show the past MAS The function of checking the past MAS
Information department
1D III
Personal key in error M
a.
R
em
.
3 Y N N Yes Control
Adopt the chemotherapy CPOE Chemotherapy prescription error rate
Information department
2Be While inputting data, the dosage of medicine was erroneously keyed C at . O cc . 12 N N Yes 2Be I
The decimal point key in error M
in . O cc . 3 Y N N Yes Eliminate
CPOE can automatically calculate required medicines on the basis of patient’s features (stature, weight, etc.)
The function of automatically calculating the required medicines 1. Pharmacy department 2. Information department 2Be II
When calculating the required dosage, the staff fills in wrong data C at . O cc . 12 N N Yes Eliminate 2Be III
The mistake of seeing the wrong decimal point C at . R em . 4 Y N N Yes Eliminate 2Be IV
The staff is getting the incorrect total amount of medicines
C at . R em . 4 Y N N Yes Control
Employ the bar code taking required medicines
The frequency of taking incorrect medicines
3Ba The transporter take back the wrong box when the medicine is empty M od . O cc . 6 N N 3Ba I
The transporter does not know if the cartridge is empty or not
M od . U nc . 4 N N
HFMEA Step 4 – Hazard Analysis HFMEA Step 5- Identify Actions and Outcomes Failure Modes:
First evaluation failure mode before determining potential causes Potential Causes Se ve ri ty Pr ob ab il ity H az ar d Sc or e Si ng le C on tr ol W ea kn es s? E xi st in g C on tr ol M ea su re ? D et ec ta bl e? Pr oc ee d? Action Type (Control, Accept, Eliminate) or Rationale for Stopping
Action Outcomes Measure
Pe rs on R es po ns ib le
3Ba The medicine is allotted to the wrong sickroom
C at . U nc . 8 N N Yes 3Ba I
The transporter takes multiple medicines simultaneously and allots them to the incorrect sickroom M od . U nc . 4 Y N N Yes Control
Enforce training for transporter The frequency of allotting incorrect medicines
Nursing department
4Db Vital information are not verified C at . O cc . 12 N N Yes 4Db I
The process is complicate and difficult to execute M a. U nc . 6 Y N N Yes Control
Adopt RFID or bar code system System completion date 1. Nursing department 2. Information technology department 4Db II
Because of too many affairs, the staff forgets to verify vital
M
a.
U
nc
.
6 Y N N Yes Accept Enforce training and education of staff
The number of unverified the patient
Nursing department
information before administrating medication
information
4E After injecting medicine into patient, the staff does not notice that exosmosis has occurred C at . O cc . 12 N N Yes 4E I
The staff leaves immediately after injecting medicine and does not monitor the condition of patient
C at . U nc . 8 N N Yes Accept
Enforce training and education of staff
The rate of medicine exosmosis
Nursing department
4E II
Over the span of time of injecting medicine, exosmosis occurred
C at . U nc . 6 Y N N Yes Control
Add an automatic alert system to prevent the exosmosis situations
The rate of medicine exosmosis that occurred after staff leaves
4E III
Exosmosis occurred because the patient turned around
C at . O cc . 12 N N Yes Control
The rate of medicine exosmosis caused by the patient turning
Table 2. Reduction in Chemotherapy Prescription Errors (2007-2009)
Before CPOE After CPOE Liver/Renal Alert System P Value
Prescription Error Error Rate
(%)
Prescription Error Error
Rate (%)
Prescription Error Error Rate
(%) Division 0.001* General Surgery 1752 37 2.1 2029 8 0.4 667 1 0.1 Hematology 4380 72 1.6 5976 19 0.3 2308 1 0.04 Liver Center 37 8 21.6 199 3 1.5 28 0 0 Urology 494 4 0.8 552 4 0.7 156 0 0 OB/GYN 1541 151 9.8 1320 6 0.5 622 2 0.3 Immunology 66 6 9.1 67 0 0 17 0 0 Pediatrics 40 3 7.5 19 1 5.3 1 0 0 Service 0.04* Ambulatory 3686 41 1.1 4088 12 0.3 1318 0 0 In-patient 4731 240 5.1 6185 29 0.5 2542 4 0.2 *p<0.05.