Title Page Title
Emergency Medical Service in Rural Mountain Areas in Taiwan - A Nantou Mountain Areas Based Study
Running Title
Emergency Medical Service in Mountain Areas Authors
Shih-Chang Hung1,2,5, Ya-Hsin Li3, Ming-Chin Chen4, Shi-Wei Lai7,8, Fung-Chang Sung1,
Lin-Lin Liu6
1Department of Public Health and 7School of Medicine, China Medical University, Taichung,
Taiwan
2Emergency and Rescue Section, Fire Department of Nantou County, Taiwan
3Department of Health Policy and Management, Chung Shan Medical University and
Hospital, Taichung, Taiwan
4Department of Surgery, 5Department of Emergency, 6Department of Nursing, Nantou
Hospital, Nantou city, Taiwan
8Department of Family Medicine, China Medical University Hospital, Taichung, Taiwan
Correspondence to
Fung-Chang Sung, PhD, MPH
Department of Public Health, China Medical University, Taichung, Taiwan Telephone number: 886-4-22054070
E-mail: [email protected]
Words count: 248 in abstract; 2946 in text; 5 tables; 1 figures; 18 references
Background The purpose of this This study explored the emergency medical service (EMS) in rural mountain areas in Taiwan for helping the government to establish the public health policies in rural mountain areas in the future.
Methods This was a retrospective study. Based on all branches EMS missions in Ren-Ai and Sinyi of Nantou County, the dispatched status, the patients’ status, and the pre-hospital emergency managements were extracted from each mission records.
Results From January to June in 2011, a total of 765 EMS were dispatched from these 3 mountain branches. Each dispatched EMS team was consisted of only one official emergency medical technicians (EMT) with EMT II certificate (100%) and additional with one (88.0%) or two (11.2%) volunteers as EMT I personnel. Most of the missions were conducted in the daytime and peaked during 10AM to 12PM. The mountain EMS served patients were characterized with the elderly (23.0%) and non-traumatic medical complains services predominantly (64.4%). Approximately 38.7% EMS patients required the risk to be the advanced life support needed. Of the mountain EMS branches, the mean response time was 15.3±16.9 minutes, the mean management time on site was 6.1±6.9 minutes and the mean transport time was 38.0±15.9 minutes. The response time and transportation time of EMS in rural mountain areas was relatively longer than that in urban towns in Taiwan.
Conclusion The rural quality of EMS is under the challenges of providing appropriate and adequate medical care. Each EMS team should be equipped with adequate emergency care facilities and well trained personnel. in rural areas not good enough and is distinctive in the rural mountain area in Taiwan. Patients might be cared by only one EMT I personnel for hours on the long way to the hospital. The result of this study could be the references for the further policies making and EMTs training.
Introduction
Pre-hospital emergency medical service (EMS) is the extension of emergency treatment at hospitals. According to the statistics by up to July of 2011 on Emergency Medical Service published by National Fire Agency of Ministry of the Interior, the total EMS cases in Taiwan nation-wide had raised for 2.2-fold from 367,011 in 2002 to 818,825 in 2011., that increased by 2.2 times.1 Though there are three equally important assignments of The fire departments
in Taiwan are responsible for 3 missions equally important: fire preventing, disaster rescue and emergency medical service. The emergency medical service has become the most regularly and also the most important daily work for the fire branches.
In the past ten plus years, the studies on emergency medicine service system are
getting thriving while most of them are based on urban areas and relatively less on rural areas, no mention the pre-hospital emergency medical service in mountain areas. The EMS quality was also straggly behind in rural areas.2 However, for being relatively shortage of health care
resources, the effect of EMS in rural mountain areas may be more crucial. Even though there were only 545,032 (2.3%) population in 2012 end, the 30 official defined mountain counties totally occupied 15,814 km² (43.7%) of Taiwan island. The purpose of this study is to explore the EMS in rural mountain areas in Taiwan.
Materials and Methods Study population
This was a retrospective study. Nantou County, total 4,106 km², is the 2nd largest county
of Taiwan. Ren-Ai and Sinyi townships, totally 2,696 km² with 32,513 populations, are two main mountain areas in Nantou County. There was no any hospital in these two districts. The nearest local community hospitals from the Ren-Ai and Sinyi townships government office were around 25-30 km² via mountainous roadways. There was no regular helicopter service
except in particular mountain accidents or natural disasters in rural mountain areas in Taiwan. There were three emergency medical branches in these two mountain districts. For
administering the emergency medical data system, Nantou County government had set up the regulation of pre-hospital EMS mission report sheets, and also launched the guidance on the writing format. Every time when the Emergency Medical Technicians (EMTs) were
dispatched, they had to record the whole emergency medical service process according to the regulation. The EMS missions report sheet contained the dispatched status, the patients’ status, and the pre-hospital emergency management for each EMS patient. The dispatched status included the date, the unit receiving the case, the time to get the dispatch informed, the time arriving and leaving the scene, the time arriving and leaving the hospital, also the time to return back to unit and get ready. The patients’ status contained name, identification number, gender, age, and also the contact address. The pre-hospital EMS missions were classified into non-trauma rescue missions and trauma rescue missions. The pre-hospital emergency
management record patients’ situation, the chief complaint, the past history, and the history of anaphylaxis, and all the emergent procedures provided to the patients. Also the pre-hospital care and in-hospital information, which contains the vital signs such as consciousness status, respiration pattern, pulse, blood pressure, and the injured status for the trauma rescue
missions, were all recorded in the report sheet. The dispatched technicians had to sign the sheet and double-checked by the medical staffs in the ED that received the patients. Time definition
The definition of time period of EMS included, “response time”, the time length on the recorded from departing the unit to arrival the scene; “on-scene time” was the time length from the time arrival the scene to depart the scene; “transport time” meant the actual time length on the way to hospital, which would be from departing the scene to arrival to hospital; “in-hospital interval” was the time length staying in the hospital; “return time” meant the time
length that the EMS team leaves the hospital, returns to the unit and gets ready again. In this study, we tried to group patients as “high probability of Advanced Life Support (ALS) cases” and “less probability of ALS cases” according to the judgment of three emergency experts, an emergency physician, a surgeon and a senior head nurses in emergency department, based on the “Emergency Medical Technicians II operation Manual in Nantou”, and the patients’ clinical condition recorded on the mission reports.3 According to these rules, patients who
were with altered consciousness (GCS, Glasgow Coma Scale < 14), tachypnea (respiratory rate > 30/min), bradypnea (respiratory rate < 10/min), tachycardia (heart beat > 140/min), bradycardia (heart beat < 50/min), very high blood pressure (systolic blood pressure > 220mmHg), low blood pressure (systolic blood pressure < 60mmHg), poor distal circulation (finger reperfusion test > 2 seconds), hyperthermia (body temperature > 40℃), hypothermia (body temperature < 32℃), suspected stroke events, ischemia chest pain, status seizure, life-threating or unknown intoxication, snakebite, chocking events, cyanosis, severe burning injury (more than 18% second degree or third degree body surface burning, or facial or genital burning ), subcutaneous emphysema, above ankle amputation, above wrist amputation, deep and large open wounds, penetrating wounds over face, head, or trunk, flair chest, brain tissue or internal organ tissue exposure, spinal cord injury, long bone open fractures, pelvis
fractures, falling from high (more than 5 meters high), and other major trauma. If there were disagreement, three experts wound meet and discuss to make the final decisions about groupings.
Statistical analysis
In statistical analysis, we adopted SPSS version 12.0 in Chinese Traditional as the main analysis tool. The result was judged to be statistically significant when p = 0.05 or less. Apart from descriptive statistics, this study also used ANOVA and the chi-square test. Furthermore, according to the determination on “high probability of Advanced Life Support (ALS) cases” or “less probability of ALS cases”, all the EMS mission report sheets from 3 branches would
be re-grouped and statistically exanimated by t-test for further understanding if the EMS efficacy would be different according to the patients’ critical situation.
Results
EMS in branches of Ren-Ai and Sinyi in Nantou County
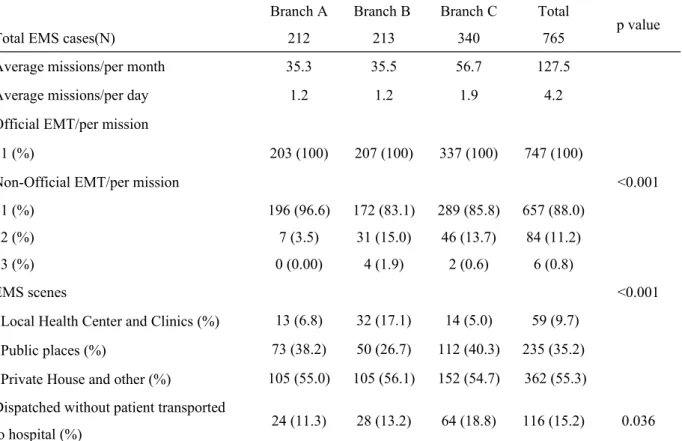
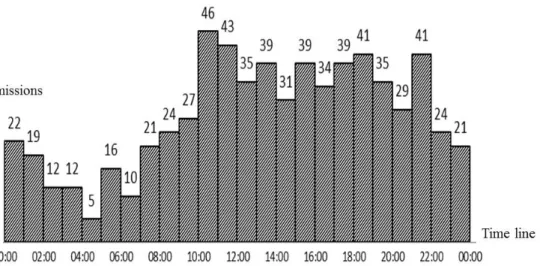
From January to June in 2011, total of 765 EMS were dispatched from these 3 mountain branches. The dispatched EMS team was leaded by only one official emergency medical technicians (EMT) with EMT II board (100%), and additional with one (88.0%) or two (11.2%) volunteers EMT I personnel (see table 1). In all dispatch missions, there were 116 (15.2%) cases without patients being transport via the dispatched ambulance. As for the scene, there were 9.7% of EMS cases were from the clinics, and 35.2% cases were from the public places or non-residence registered address. The average dispatched mission was 42.5 for each branch in each month, and most of the cases happened in the daytime from 10AM to 10PM, and peaked during 10AM to 12PM. The different dispatch status of each branches and the time received the cases were shown in table 1 and figure 1.
The Characteristic of EMS Patients
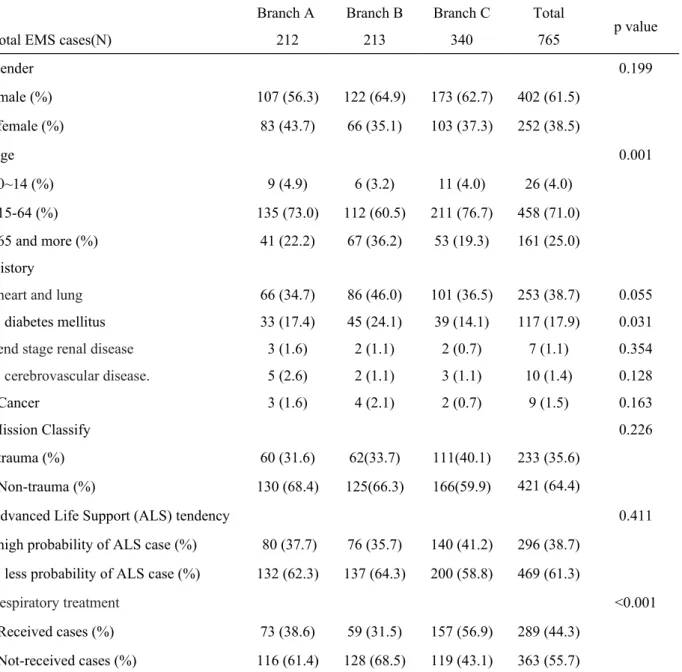
The EMS patients’ characters in mountain area were male predominant (61.5%). There were more elderly (25.0% of 65 years old and above) with less young children (4.8% of 0-14 years old). There were 38.7% patients with past medical history of cardiovascular diseases such as hypertension, cardiomyopathy, arrhythmias and chronic obstructive pulmonary disease etc. There were 17.9% with the history of diabetes mellitus, 1.1% with the history of end-stage renal disease, 1.4% with cerebrovascular diseases, and 1.5% with history of cancer. On the classification of trauma or non-trauma rescue missions, the non-traumatic rescue missions were predominant (64.4%), and according to the classification on “high or less probability of ALS cases”, there were 38.7% EMS patients have the risk to be the advanced life support needed. 44.3% patients (31.8% trauma patients and 50.9% non-trauma patients) were treated
with airway management and breathing care before arrival to the hospitals (table 2). The time of EMS branches of Ren-Ai and Sinyi of Nantou County
Table 3 showed each time period spent in each mission. The average response time of each branches is was 15.3±16.9 minutes, the average on-scene time was 6.1±6.9 minutes, the average transport time was 38.0±16.0 minutes, in-hospital interval of average was 12.9±6.9 minutes and the return time of average was 46.4±25.5 minutes. The branch C has significant differences on response time, transport time, and return time.
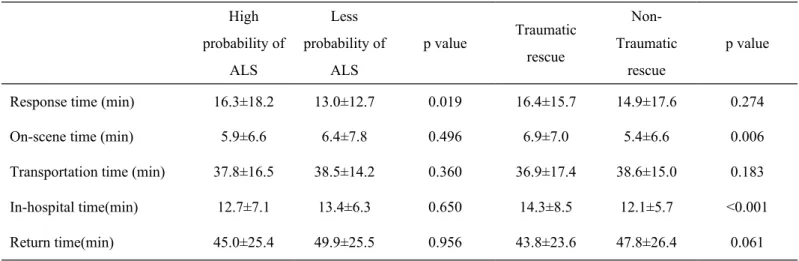
This study also compared “high probability of Advanced Life Support (ALS) cases” and “less probability of ALS cases” in each time period (table 4), and only found the significance difference on response time. In response time, the average time of non-ALS cases (16.3 minutes) was obviously longer than of the ALS cases (13.0 minutes).
When reviewing the difference on time of EMS between the trauma and non-trauma rescue missions, there were significant difference on on-scene time (p=0.006) and in-hospital time (p<0.001). In on-scene time, the average 6.9 minutes of trauma cases was obviously longer than 5.4 minutes of non-trauma cases, and also 14.3 minutes of trauma cases over 12.1 minutes of non-trauma cases on in-hospital interval.
Discussion
The pre-hospital EMS could partially cover the shortage of medical resources in rural areas.4 In Taiwan, the quality control and data analysis of EMS were mostly on densely
populated urban areas, and the previous researches on EMS system in mountain areas were mainly related to tourism enterprise. The difference of EMS in rural and urban area needs further and more accurate evaluations.5,6 This study focused on the EMS in mountain areas
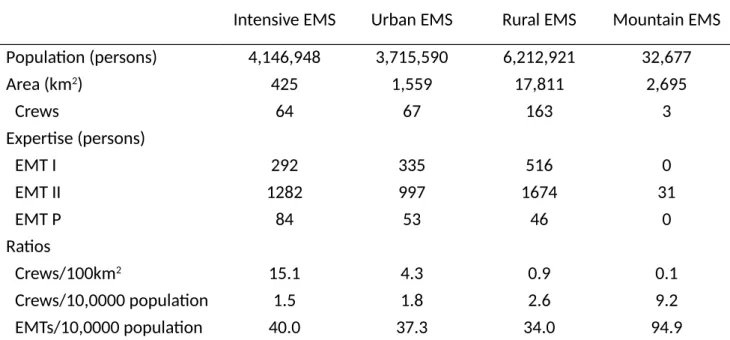
and tried to be the reference especially on EMS system planning and EMS quality promoting in the future. The discussion was mainly constructed in tree sections: the EMS manpower in rural mountain area, the EMS patients’ characteristics and the EMS efficiency (table 5).2
First, the manpower of EMS in the rural mountain area is shortage, and depended on volunteers. In each mission the EMS team could only be composed by one official emergency medical technician with EMT-II board with one (88.0%) or two EMT- I board personnel from volunteers or Substitute Military Service personnel. Though most official emergency medical technicians were certificated in EMT-II, the supported personnel from volunteers or
Substitute Military Service were merely certificated with EMT-I. Restrained by the rule of Enforcement Statute for Substitute Services published in 2000 in Taiwan and its interpretative letter in 2001, the Substitute Military Service personnel could not as the driver in the mission. In this situation, in most missions, the EMT-II might only serve as the driver for ambulances and on-scene treatment, and offer the verbal consulting and technical guidance while the EMT-I mainly take charge of the management and monitor the patients in the transportation to hospital. These EMS team might have some impact to the quality of EMS in rural mountain areas.
Comparing to the densely populated urban areas, the mission quantity is much lower in rural mountain areas. The lower quantity would influence the proficiency on EMS clinic judgments and techniques especially of the junior EMTs.7 How to use the continuous
education training in the consideration of the characteristics in rural mountain areas will be one of the main issues in the future,8 such as arrange the EMTs from high duty quantity
branches to exchange the experience for improvement on the low duty quantity branches. In rural mountain areas the demands were mainly in daytime from 10 AM to 10 PM, and peaked during 10 AM to 12 PM. This distribution pattern could be related to the lifestyle and work nature of people in rural mountain areas.6 The workload distribution of Ren-Ai and
Sinyi in Nantou County was similar to the workload distribution in Tainan County, and was different from the workload distribution in Tainan City. In city regions, there would be a second peak just after the midnight.6
Second, the EMS served more non-trauma patients than traumatic patients. According to the 2011 official report, the overall population in Taiwan was11% older than 65 years old, 74% between 15-64 years old, and 15% younger than 14 years old; in rural mountain areas, there was 9% elderly, 74% between 15-64 years old and 17% younger than 14 years old. There was less elderly population in rural mountain areas in Taiwan. In our study, male have relatively high usage rate on EMS, which is compatible to the results from long-term surveys show that male in different age levels have higher usage rate on emergency services, transfers, and emergency medical resources.9,10 Lots of patients served by EMS have the past history of
heart and lung diseases, and diabetes mellitus. The possible reason could be the EMS served more non-traumatic elderly patients. The study conducted in Tainan City in 1997 revealed more than 50% EMS missions were traumatic and related to traffic accidents.6 The nationwide
official report revealed 46.6% EMS missions were trauma related in 2011. Add the educational training programs on disease peculiar to the elderly could promote the pre-hospital EMS quality of the elderly in rural mountain areas.11,12
In this study, 30-40% of patients were classified as “high probability of ALS cases”. At the same time, there were also high to 30-40% of patients received respiratory treatments.
Compared with a study conducted in Nantou City, the major township in Nantou County, there was only 16.3% missions were classified as ALS cases in this area in 2009.13 In this
situation, as earlier mentioned, the quality of EMS on the way to the hospitals provided by EMT-I personnel alone was worrisome. According to Emergency Medical Technician Regulation Rule in Taiwan, EMT II was authorized to check patients glucose status, intravenous line setup and fluid infusion, and inserted laryngeal mask airway to critical patients while EMT I was only authorized to check vital signs, using oral or oral airway, and simple mask oxygenation etc. Also in rural mountains, though there were around 20% patients has the history of diabetes mellitus, there was no any records of finger-stick glucose
testing for ALS cases (data not shown). According to the statement and the devices claim records of Fire Department of Nantou County, glucometer devices were available in each branch. However, to fit the different scenarios of EMS in mountain and non-mountain areas, the current “Emergency Medical Technicians II operation Manual in Nantou” not strongly worded the necessity of glucose level checking and glucose water injection. It might need prospective studies to realize if there are other consideration e.g. legal problems, medical devices, EMTs’ confidence about medical technicians, or there are truly no demands about finger-stick glucose testing from these cases.
Third, the response time and transportation time of EMS in rural mountain areas was relatively longer, due to the broadness of the mountain areas and the long distance from the hospitals. A study which enrolled data of all branches from five counties of Taiwan (Taoyuan county, Hsihchu county, Kaohsiung county, Taichung county and Nantou county) reported the average response time is 6.08 to 10.52 minutes, and average transportation time is 10.60 to 18.57 minutes. 14 The 119 help calling might be direct connected to the local branches, but
not via the county dispatch center in rural areas. However, this mechanism might not impact the response time.14 Another study conducted in Tainan City of Taiwan in 1997 reported that
the response time was less than 10 minutes in 92% missions, and 99% patients could be sent into hospital EDs in 40 minutes.6 There were many other studies trying to apply innovative
technologies to solve the problem on response time of EMs in rural areas,15 or to improve the
accessibility by employ the concept of telemedicine.16 The feasibility and demand of
air ambulance medical service is worth of consideration, nevertheless, the pros and cons, and also the economic effects requires further analysis17. A study conducted in Australia showed
that if the distance of EMS is in the range of 100km and also accessible by land traffic, there is no apparent ameliorate in the air ambulance transport to improve time to definite care.18 In
Our study showed high probability of ALS cases had longer response time than lower probability cases, and trauma patients required more on-scene and in-hospital time. That could be related to the injured patients needing more rescue equipment usage. In addition, the EMTs did not apply different policy on EMS efficiency according to different situation. For the limitation of EMS resource in rural mountain areas, there is only one EMS team in each branch. However, for each dispatch missions, it require around 3 hours for an EMS to go back ready for the next mission. The region will be shortage of EMS resources in this time period, and will rely on neighbor branches more far away.
Some limitations were also present in our study. First, we did not visit patients on scene, patients physical examination status and trauma mechanism were all depend on mission report sheets. Second, the judgment of probability of Advanced Life Support (ALS) cases depended on mission report sheets too. That is, over or under judgment could be possible. For example, patients with hyperventilation syndrome with tachypnea might be group into high probability of Advanced Life Support (ALS) cases.
The EMS in rural mountain areas has finite resource as it in urban regions. The quality of EMS is not good enough and is distinctive in the rural mountain area in Taiwan. The EMS patients’ characters in mountain area were non-traumatic predominant and higher risk to be the advanced life support needed. However, patients might be cared by only one EMT I personnel for hours on the long way to the hospital. The management and analysis on EMS in rural areas could be effective to improve the EMS resource distribution and future educational training programs.
Reference
1. National Fire Agency‚ Ministry of the Interior. The Statistics on the Emergency Medical Services. Taipei: National Fire Agency website.
2. Cheng SC, Liao CK, Guo HR, Lin HJ, Tsai MC, Chen JC, et al. Comparison of the Satisfaction among Varied Emergency Medical System District by Medical Personnel in Taiwan. Journal of Emergency Medicine 2010;12:s7-13. [In Chinese, English abstract] 3. Nantou County Government Fire Bureau. Emergency Medical Technicians Regulation.
Nantou County Government Fire Bureau website. http://www.ntfd.gov.tw/news.asp? id=446&RedirURL1=%2Fnewslist.asp%3Fpage%3D12%26st%3D1. Accessed July 19, 2012.
4. Hwang KP, Wu CH. [Simulation and Evaluation of Emergency Medical Services Systems Resource Allocation and Performance]. Taiwan Journal of Public Health 2007;26:184-95. 5. Hu SC, Kao WF. [Emergency Medical Services in Mountain and Remote Recreational
Areas]. Tzu Chi Medical Journal 2002;14:301-9.
6. Chi CH, Tsai MC, Yen YL, Ye YJ, Lin, SM, Wu MH. [Ambulance Utilization in Tainan: Analysis of Emergency Ambulance Missions in Urban and Rural Areas]. Taiwan Journal
of Public Health 1997;16:177-84.
7. Stevens SL, Alexander JL. The impact of training and experience on EMS providers’ feelings toward pediatric emergencies in a rural state. Pediatr Emerg Care 2005;21:12-7. 8. Weichenthal L, Cabañas J, Spano S, Horan B, Schmitt E. EMS in rural and wilderness
areas. In: Tintinalli JE, Cameron P, Holliman J eidtors. EMS a practical global guidebook. Shelton: People’s Medical Publishing House; 2010, p. 575-85.
9. Chi CH, Tsai MC, Wu KW, Wu, MH. [119 Emergency Medical Transport of the Elderly].
The Kaohsiung Journal of Medical Sciences 1996;12:699-706.
10. Wofford JL, Moran WP, Heuser MD, Schwartz E, Velez R, Mittelmark MB. Emergency medical transport of the elderly: a population-based study. Am J Emerg Med 1995;13:297-300.
11. Keskinoglu P, Sofuoglu T, Ozmen O, Gündüz M, Ozkan M. Older people’s use of pre-hospital emergency medical services in Izmir, Turkey. Arch Gerontol Geriatr
2010;50:356-60.
12. Shah MN, Rajasekaran K, Sheahan WD 3rd, Wimbush T, Karuza J. The effect of the geriatrics education for emergency medical services training program in a rural community. J Am Geriatr Soc 2008;56:1134-9.
13. Hung JC. The Elderly Pre-Hospital Emergency Medical Service Study – in Nantou City. Nan Kai University of Technology Institutional Repository.
http://163.22.228.106:8080/ir/handle/987654321/555. [In Chinese, English abstract] 14. Hung SC, Xie FN, Lai SW, Chen WK,; Li YH. The Impact of Dispatch System on
Emergency Medical Service Time. Journal of Emergency Medicine, 2009;11:s1-6 15. Gonzalez RP, Cummings GR, Mulekar MS, Harlan SM, Rodning CB. Improving rural
emergency medical service response time with global positioning system navigation. J
Trauma 2009;67:899-902.
16. Blozik E, Wildeisen IE, Fueglistaler P, von Overbeck J. Telemedicine can help to ensure that patients receive timely medical care. J Telemed Telecare 2012;18:119-21.
17. Butler DP, Anwar I, Willett K. Is it the H or the EMS in HEMS that has an impact on trauma patient mortality? A systematic review of the evidence. Emerg Med J
2010;27:692-701.
18. Shepherd MV, Trethewy CE, Kennedy J, Davis L. Helicopter use in rural trauma. Emerg
Table 1. EMS in branches of Ren-Ai and Sinyi in Nantou County
Branch A Branch B Branch C Total
p value
Total EMS cases(N) 212 213 340 765
Average missions/per month 35.3 35.5 56.7 127.5
Average missions/per day 1.2 1.2 1.9 4.2
Official EMT/per mission
1 (%) 203 (100) 207 (100) 337 (100) 747 (100)
Non-Official EMT/per mission <0.001
1 (%) 196 (96.6) 172 (83.1) 289 (85.8) 657 (88.0)
2 (%) 7 (3.5) 31 (15.0) 46 (13.7) 84 (11.2)
3 (%) 0 (0.00) 4 (1.9) 2 (0.6) 6 (0.8)
EMS scenes <0.001
Local Health Center and Clinics (%) 13 (6.8) 32 (17.1) 14 (5.0) 59 (9.7) Public places (%) 73 (38.2) 50 (26.7) 112 (40.3) 235 (35.2) Private House and other (%) 105 (55.0) 105 (56.1) 152 (54.7) 362 (55.3) Dispatched without patient transported
to hospital (%) 24 (11.3) 28 (13.2) 64 (18.8) 116 (15.2) 0.036 The missing value of Official/Non-Official Emergency Medical Technicians and the EMS scenes are from the cases of dispatched ambulance without patient transported to hospital. * Reasons of non-patient transport included 46 (39.7%) patients refused to be transported (either refused to go to hospital or refused to go to hospital via ambulance), 41 (35.3%) cancelled mission after being dispatched, 15 (12.9%) missions without patients found on scene, 5 (4.3%) patients was transported via other vehicles, 4 (3.4%) declaration of death on scene, and other unknown and miscellaneous.
Table 2. The Characteristic of EMS Patients in Ren-Ai and Sinyi of Nantou County Branch A Branch B Branch C Total
p value
Total EMS cases(N) 212 213 340 765
Gender 0.199 male (%) 107 (56.3) 122 (64.9) 173 (62.7) 402 (61.5) female (%) 83 (43.7) 66 (35.1) 103 (37.3) 252 (38.5) Age 0.001 0~14 (%) 9 (4.9) 6 (3.2) 11 (4.0) 26 (4.0) 15-64 (%) 135 (73.0) 112 (60.5) 211 (76.7) 458 (71.0) 65 and more (%) 41 (22.2) 67 (36.2) 53 (19.3) 161 (25.0) History
heart and lung 66 (34.7) 86 (46.0) 101 (36.5) 253 (38.7) 0.055
diabetes mellitus 33 (17.4) 45 (24.1) 39 (14.1) 117 (17.9) 0.031
end stage renal disease 3 (1.6) 2 (1.1) 2 (0.7) 7 (1.1) 0.354
cerebrovascular disease. 5 (2.6) 2 (1.1) 3 (1.1) 10 (1.4) 0.128
Cancer 3 (1.6) 4 (2.1) 2 (0.7) 9 (1.5) 0.163
Mission Classify 0.226
trauma (%) 60 (31.6) 62(33.7) 111(40.1) 233 (35.6) Non-trauma (%) 130 (68.4) 125(66.3) 166(59.9) 421 (64.4)
Advanced Life Support (ALS) tendency 0.411
high probability of ALS case (%) 80 (37.7) 76 (35.7) 140 (41.2) 296 (38.7) less probability of ALS case (%) 132 (62.3) 137 (64.3) 200 (58.8) 469 (61.3)
Respiratory treatment <0.001
Received cases (%) 73 (38.6) 59 (31.5) 157 (56.9) 289 (44.3) Not-received cases (%) 116 (61.4) 128 (68.5) 119 (43.1) 363 (55.7)
Table 3. The time of EMS branches of Ren-Ai and Sinyi of Nantou County
Brach A Brach B Brach C Average p value
Response time (min) 9.6±10.2 10.0±13.4 22.9±19.7 15.3±16.9 <0.001
On-scene time (min) 5.7±5.2 5.5±5.8 6.7±8.5 6.1±6.9 0.137
Transportation time (min) 44.1±13.9 40.4±14.0 32.2±16.5 38.0±16.0 <0.001 In-hospital time(min) 13.0±4.9 13.0±8.0 12.7±7.3 12.9±6.9 0.918 Return time(min) 61.1±22.0 50.5±20.0 33.5±24.7 46.4±25.5 <0.001 * The distance from fire station to the mostly nearby hospital is 45.6km for Branch A, 32.4km for Branch B, and 25.6 km for Branch C. Branch severed 1,273 km2 administrative area
Table 4. The EMS efficiency in branches of Ren-Ai and Sinyi in Nantou County High probability of ALS Less probability of ALS p value Traumatic rescue Non-Traumatic rescue p value
Response time (min) 16.3±18.2 13.0±12.7 0.019 16.4±15.7 14.9±17.6 0.274
On-scene time (min) 5.9±6.6 6.4±7.8 0.496 6.9±7.0 5.4±6.6 0.006
Transportation time (min) 37.8±16.5 38.5±14.2 0.360 36.9±17.4 38.6±15.0 0.183 In-hospital time(min) 12.7±7.1 13.4±6.3 0.650 14.3±8.5 12.1±5.7 <0.001 Return time(min) 45.0±25.4 49.9±25.5 0.956 43.8±23.6 47.8±26.4 0.061
Table 5. The EMS comparison in different areas of Taiwan
Intensive EMS Urban EMS Rural EMS Mountain EMS
Population (persons) 4,146,948 3,715,590 6,212,921 32,677 Area (km2) 425 1,559 17,811 2,695 Crews 64 67 163 3 Expertise (persons) EMT I 292 335 516 0 EMT II 1282 997 1674 31 EMT P 84 53 46 0 Ratios Crews/100km2 15.1 4.3 0.9 0.1 Crews/10,0000 population 1.5 1.8 2.6 9.2 EMTs/10,0000 population 40.0 37.3 34.0 94.9
EMS: emergency medical service; EMT: emergency medical technician
Intensive EMS: Taipei City & Kaohsiung City; Urban EMS: Tainan City, Taichung City & Taoyuan City; Rural EMS: Xinzhu county, Taichung Conuty, Jiayi County, Tainan County, Kaohsiung County, Taitung County; Mountain EMS: Ren-Ai and Sinyi of Nantou County.