Introduction
Congenital diarrheal disorders (CDD) are a group of rare chronic enteropathies caused by heterogeneous genetic defects and are characterized by severe diarrhea in infancy. Berni Canani et al [1] suggested that CDD be classified into four categories in relation to the defects: (1) defects of digestion, absorption and transport of nutrients and electrolytes: congenital lactase deficiency
M
ICROVILLUS
I
NCLUSION
D
ISEASE
: P
RENATAL
U
LTRASOUND
F
INDINGS
, M
OLECULAR
D
IAGNOSIS AND
G
ENETIC
C
OUNSELING OF
C
ONGENITAL
D
IARRHEA
Chih-Ping Chen1,2,3,4,5,6*, Ming-Chou Chiang7, Tzu-Hao Wang8, Chuen Hsueh9, Shueen-Dyh Chang8, Fuu-Jen Tsai4,10, Chao-Ning Wang8, Schu-Rern Chern2, Wayseen Wang2,11
Departments of 1Obstetrics and Gynecology and 2Medical Research, Mackay Memorial Hospital, 5Institute of Clinical and
Community Health Nursing, 6Department of Obstetrics and Gynecology, School of Medicine, National Yang-Ming University, and 11Department of Bioengineering, Tatung University, Taipei; 3Department of Biotechnology, Asia University,
4School of Chinese Medicine, College of Chinese Medicine, China Medical University, and 10Departments of
Medical Genetics and Medical Research, China Medical University Hospital, Taichung; Departments of
7Pediatrics, 8Obstetrics and Gynecology, and 9Pathology, Lin-Kou Medical Center,
Chang-Gung Memorial Hospital, Chang-Gung University, Tao-Yuan, Taiwan.
SUMMARY
Objective: To present prenatal ultrasound findings and molecular diagnosis of microvillus inclusion disease, and to review the literature of abnormal prenatal ultrasound findings associated with congenital diarrhea.
Materials, Methods and Results: A 21-year-old woman, gravida 1, para 0, had generalized bowel dilation of the fetus on prenatal ultrasound at 29 gestational weeks. She and her husband were non-consanguineous, and there was no family history of congenital diarrhea. Prenatal ultrasound at 29 gestational weeks revealed a honeycomb appearance of the bowel without ascites or intraperitoneal calcification. At 36 gestational weeks, polyhydramnios dilated bowel loops were observed, and a 3,355-g male baby was delivered with a distended abdomen. Post-natally, the neonate suffered from watery diarrhea and abdominal distension but there was no mechanical bowel obstruction. An endoscopic biopsy of the small bowel revealed intracytoplasmic inclusions lined by intact microvilli in the apical surface of the intestinal epithelial cells consistent with the diagnosis of microvillus inclusion disease. Mutation analysis of blood samples of the neonate and parents revealed a heterozygous nonsense mutation of c.445C> T, p.Q149X in exon 4 of the MYO5B gene in the father and proband, and a heterozygous nonsense mutation of c.1021C> T, p.Q341X in exon 9 of the MYO5B gene in the mother and proband.
Conclusion:Prenatal sonographic identification of dilated bowel loops in association with polyhydramnios suggests congenital diarrhea and a differential diagnosis of microvillus inclusion disease in addition to congeni-tal chloride diarrhea and congenicongeni-tal sodium diarrhea. Molecular analysis of the MYO5B gene is helpful in genetic counseling and prenatal diagnosis of recurrent microvillus inclusion disease in subsequent pregnancies. [Taiwan J Obstet Gynecol 2010;49(4):487–494]
Key Words:congenital diarrhea, microvillus inclusion disease, MYO5B, prenatal diagnosis, ultrasound
*Correspondence to: Dr Chih-Ping Chen, Department of Obstetrics and Gynecology, Mackay Memorial Hospital, 92, Section 2, Chung-Shan North Road, Taipei, Taiwan.
E-mail: [email protected] Accepted: September 29, 2010
(LCT gene), sucrase-isomaltase deficiency (SI gene), maltase-glucoamylase deficiency (MGAM gene), glucose-galactose malabsorption (SLC5A1 gene), fructose mal-absorption (GLUT5 gene), Fanconi-Bickel syndrome (GLUT2 gene), cystic fibrosis (CFTR gene), acrodermati-tis enteropathica (SLC39A4 gene), congenital chloride diarrhea (SLC26A3 gene), congenital sodium diarrhea (SPINT2 gene), lysinuric protein intolerance (SLC7A7 gene), congenital bile acid diarrhea (SLC10A2 gene), enterokinase deficiency (PRSS7 gene), trypsinogen defi-ciency (PRSS1 gene), pancreatic lipase defidefi-ciency (PNLIP gene), abetalipoproteinemia (MTP gene), hypobetalipo-proteinemia (APOB gene) and chylomicron retention disease (SAR1B gene); (2) defects of enterocyte differ-entiation and polarization: microvillus inclusion disease (MVID) (MYO5B gene), congenital tufting enteropathy (EpCAM gene) and syndromic diarrhea; (3) defects of enteroendocrine cell differentiation: enteric anendo-crinosis or congenital malabsorptive diarrhea (NEUROG3 gene), enteric dysendocrinosis and proprotein convertase 1 deficiency (PCSK1 gene); and (4) defects of modula-tion of the intestinal immune response: immunodysreg-ulation polyendocrinopathy, enteropathy and X-linked syndrome (IPEX) (FOXP3 gene), IPEX-like syndrome, immunodeficiency-associated autoimmune enteropathy, autoimmune polyendocrine syndrome-1 (AIRE gene) and autoimmune enteropathy with colitis-generalized autoimmune gut disorder. Most defects of CDD are inherited as an autosomal recessive trait, and IPEX is inherited as an X-linked recessive trait. We present here the prenatal ultrasound findings and molecular genetic diagnosis of MVID, a very rare autosomal recessive dis-order, which belongs to CDD category II.
Materials, Methods and Results
A 21-year-old woman, gravida 1, para 0, had general-ized bowel dilation of the fetus on prenatal ultrasound
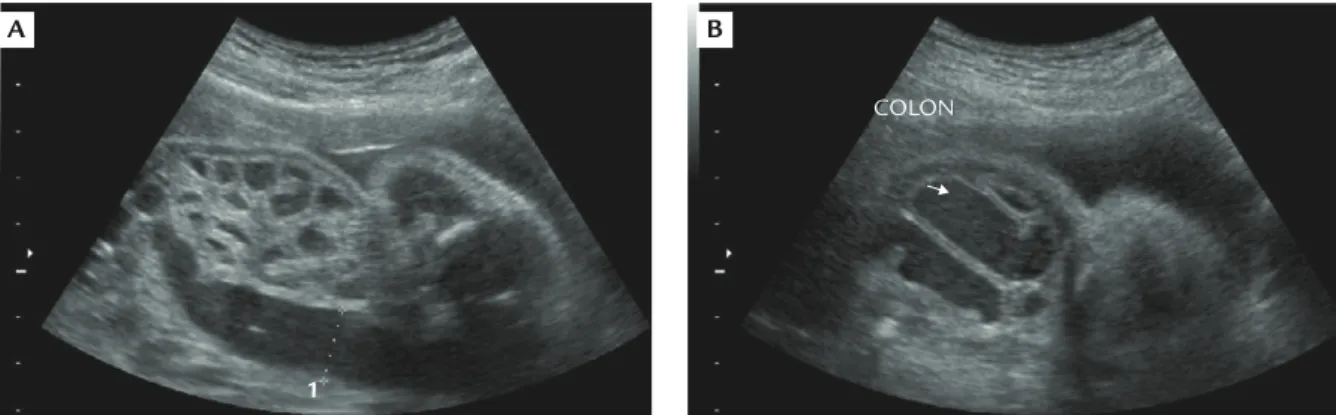
at 29 gestational weeks. Her husband was 37 years old. She and her husband were non-consanguineous, and there was no family history of congenital malformations or CDD. During this pregnancy, a maternal serum screen-ing test for Down syndrome was negative. Routine sono-graphic examinations were normal until 29 gestational weeks when prenatal ultrasound showed a honeycomb appearance of the bowel with generalized dilation of the bowel from the small intestines to colon with a thick intestinal wall but without ascites or intraperitoneal calcification (Figure 1). The amniotic fluid index was normal. Other organs were unremarkable. Maternal TORCH (toxoplasmosis, rubella, cytomegalovirus and herpes simplex) serologic test results were negative. A tentative diagnosis of congenital megacolon or imper-forate anus was made. At 36 gestational weeks, poly-hydramnios (amniotic fluid index= 27.3cm) was evident in addition to the dilated bowel loops (Figure 2), and a 3,355-g male baby was delivered with a distended abdomen and respiratory distress. Postnatally, the neo-nate suffered from watery diarrhea and abdominal dis-tension but there was no mechanical bowel obstruction. An endoscopic biopsy of the small bowel revealed intracytoplasmic inclusions lined by intact microvilli in
A B
COLON
1
Figure 1. Prenatal ultrasound at 29 gestational weeks showing (A) a honeycomb appearance of multiple dilated loops of bowel and (B) fluid-filled large bowel.
BOWEL
15 cm 17 fps Figure 2. Prenatal ultrasound showing fluid-filled bowel loops at 36 gestational weeks.
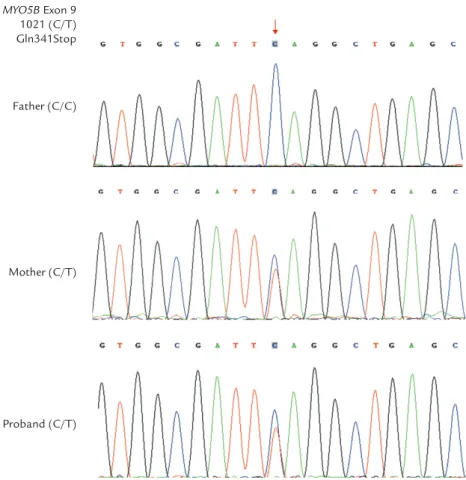
the apical surface of the intestinal epithelial cells con-sistent with the diagnosis of MVID. The neonate was on long-term total parenteral nutrition but died of sep-sis, malnutrition and multiple organ failure at the age of 6 months. Mutation analysis of peripheral blood sam-ples of the neonate and the parents revealed a c.445C>T nonsense mutation in exon 4 of the MYO5B gene that predicts a p.Q149X in the neonate and the father (Figure 3), and a c.1021C> T nonsense muta-tion in exon 9 of the MYO5B gene that predicts a p.Q341X in the neonate and the mother (Figure 4).
Discussion
MVID or DIAR2, diarrhea 2 with microvillus atrophy (OMIM 251850), is an autosomal recessive disorder of intestinal epithelial cells. MVID is characterized by in-tractable life-threatening watery diarrhea during infancy and can be caused by mutations in the MYO5B gene (OMIM 606540) on chromosome 18q21. MVID was first described by Davidson et al [2] in 1978 as familial enteropathy presenting with protracted diarrhea from birth, failure to thrive and hypoplastic villus atrophy. Characteristic pathologic and electron-microscopic find-ings of MVID include atrophy of microvilli on mature
enterocytes, apical accumulation of numerous periodic-acid-Schiff-positive secretory granules in immature en-terocytes, and microvillus inclusion bodies containing rudimentary or fully differentiated microvilli in mature enterocytes [3–5].
Other DIAR categories in OMIM include DIAR1: congenital chloride diarrhea (OMIM 214700) caused by mutations in the SLC26A3 gene (OMIM 126650) on chromosome 7q31; DIAR3: congenital sodium diarrhea (OMIM 270420) caused by mutations in the SPINT2 gene (OMIM 605124) on chromosome 19q13.1; DIAR4: congenital malabsorptive diarrhea (OMIM 610370) caused by mutations in the NEUROG3 gene (OMIM 604882) on chromosome 10q21.3; and DIAR5: con-genital tufting enteropathy (OMIM 613217) caused by mutations in the EpCAM gene (OMIM 185535) on chromosome 2p21. All are rare autosomal recessive disorders.
The present case was associated with early-onset MVID and novel heterozygous nonsense mutations in the MYO5B gene (c.445C> T, p.Q149X and c.1021C>T, p.Q341X). Both nonsense mutations predict early trun-cation of MYO5B and cause loss of MYO5B function. Müller et al [6] first identified seven different nonsense, missense, splice-site or in-frame insertion mutations in the MYO5B gene in patients with MVID from seven MYO5B Exon 4 445(C/T) Gln149Stop Father (C/T) Mother (C/C) Proband (C/T)
families. MYO5B encodes the unconventional class V dimeric non-filamentous myosin, or myosin Vb, which regulates membrane trafficking along the recycling pathway in polarized epithelial cells [6,7]. Mutations of the MYO5B gene disrupt epithelial cell polarity, and loss-of-function mutations of MYO5B are a major cause of MVID [6,8,9]. There are two types of MVID: the early-onset type presenting watery diarrhea within the first day of life and the late-onset type presenting symptoms after 3 or 4 months of life [6]. In patients with MVID without transplantation, the prognosis is very poor be-cause there is no successful medical treatment, and the patients remain dependant on total parenteral nutrition and are likely complicated with metabolic decomposi-tion, sepsis and/or liver failure. Recently, small bowel transplantation with or without liver transplantation and colon grafting for the treatment of MVID have achieved variable success [10–14].
The present case manifested multiple dilated loops of small and large bowel at 29 gestational weeks and polyhydramnios at 36 gestational weeks. The present case provides evidence that fetuses with MVID may pres-ent multiple dilated loops of bowel and polyhydramnios mimicking intestinal obstruction in the early third tri-mester. To date, there has only been one report of MVID
prenatally presenting as multiple dilated loops of bowel and polyhydramnios [15]. To our knowledge, the pres-ent case is the second case report of this condition. Phillips and Schmitz [3] surveyed 23 cases of MVID but did not describe abnormal prenatal findings of bowel dilation and polyhydramnios in their series. Ruemmele et al [4] suggested that in cases of MVID, the preg-nancy and delivery are generally uneventful, and there is no polyhydramnios except in rare isolated cases. Our case is one of those rare isolated cases. We consider that the unusual severe prenatal phenotype in this case may be in part due to a genotype-phenotype correlation of concomitant nonsense mutations of the MYO5B gene in association with early truncation of MYO5B, and pre-natal severe bowel dilation and polyhydramnios. We suggest that prenatal diagnosis of dilated bowels should include a differential diagnosis of MVID in addition to jejunoileal atresia, volvus, meconium ileus, meconium peritonitis, Hirschsprung’s disease, cystic fibrosis, enteric duplications, anorectal atresia, congenital sodium diar-rhea, and congenital chloride diarrhea.
Enterocyte differentiation and polarization defects and iron transport defects associated with CDD have been reported to present dilated bowel and poly-hydramnios on prenatal ultrasound (Table). Kirkinen MYO5B Exon 9 1021 (C/T) Gln341Stop Father (C/C) Mother (C/T) Proband (C/T)
Figure 4. A heterozygous nonsense mutation (c.1021C> T, p.Q341X) in exon 9 of the MYO5B gene in the mother and proband.
T
able.
Repor
ted cases of congenit
al diarr
hea with abnormal pr
enat
al ultr
asound f
indings of the gastr
oint estinal tr act Gest ational Author (year) Disease Mat ernal age at Pr enat al ultr asound Family histor y and outcome age (yr) diagnosis
findings and management
(wk) Kir kinen and Joup pila [16] (1984) Case 1 CLD 26 33 P olyhydr amnios, dist ended int estinal loops Deliver y at 36 wk , 3,000 g, f emale, sever e diarr hea af ter bir th with a
high chloride concentr
ation in the stool, normal development at
3 year s old f ollowing substitut e ther apy Case 2 CLD 31 26 P olyhydr amnios, dist ended int estinal loops Deliver y at 30 wk , 1 ,840 g, f emale, postnat al diarr hea, hypochlor
emia, high chloride concentr
ation in the stool, normal
development at 4 year s old f ollowing substitut e ther apy Case 3 CLD 27 35 P olyhydr amnios, dist ended int estinal loops Deliver y at 36 wk , 2,880 g, f emale, wat er
y stool rich in chloride,
condition impr oved af ter specif ic electr olyt e ther apy Gr oli et al [19] CLD 32 28 Dist ended int
estinal loops, polyhydr
amnios Deliver y at 35 wk , 2,450 g, male, wat er y stool with a (1986) 31
high chloride concentr
ation af ter bir th, normal at 3 34 year s old f ollowing or al administr ation of chlorides Pat el et al [20] CLD 25 30 P olyhydr amnios, dist ended int estinal loops T wo pr evious pr
egnancies with polyhydr
amnios and f et al CLD; (1989) bir th weight of 1 ,760 g, wat er y diarr
hea with high chloride
concentr
ation, normal at 7 weeks old af
ter chloride ther
apy Langer et al [17] CLD 25 30 P olyhydr amnios, dilat ed bowel loops Deliver y at 35 wk , 3,000 g, f emale, postnat al wat er y stool with (1991)
a high chloride concentr
ation, normal at 6 months old af
ter chloride ther apy Rose et al [21] CLD 28 24 P olyhydr
amnios, massively dilat
ed small and Deliver y at 32 wk , 2,773 g, f emale, dilat ed bowel, ileostomy for (1992) lar ge bowel, negative T OR CH t est, ther apeutic decompr ession, dehydr
ation and electr
olyt e losses af ter sur ger y amniocent esis f or amnior eduction, AF: 46,XX P oggiani et al [22] CLD NA 33 P olyhydr amnios, dist
ension of the int
estinal loops
Deliver
y at 36 wk
, 3,300
g, f
emale, abnormal yellow
ish
(1993)
liquid f
eces with no meconium, abdominal dist
ension, e xplor ator y lapar otomy to e
xclude anatomical obstruction or meconium ileus,
normal r
esults of bowel biopsy
, high chloride concentr
ation in the
stool, normal at 4 year
s old af
ter tr
eatment with NaCl and K
T able. (Continued) Gest ational Author (year) Disease Mat ernal age at Pr enat al ultr asound Family histor y and outcome age (yr) diagnosis
findings and management
(wk)
L
undkvist et al [23] (1996) 8 case series
CLD
NA
NA
Eight cases showed pr
onounced polyhydr
amnios
Thr
ee of eight cases had f
amily histories, two cases wer
e f alse ly and f et al int
estinal dilation of all int
estine with
diagnosed as having aganglionosis, one under
went ileostomy
, and
normal int
estinal perist
alsis
the other under
went sigmoidostomy bef
or e the corr ect diagnosis Rowlands CLD 34 28 Mar ked polyhydr
amnios, multiple dilat
ed loops Deliver y at 37 wk , 3,415 g, f emale, cy stic f ibr osis was e xcluded, et al [24] (1996) of f et
al bowel with perist
alsis, amniocent
esis:
wat
er
y stool, hypochlor
emia, normal at 19 day
s old af ter tr eat ment 46,XX, no evidence of mat ernal inf ection with K Cl and NaCl Husu et al [25] CLD NA 32 P olyhydr amnios, f
luid within small bowel,
Deliver
y at 36 wk
, f
emale, no passage of meconium, abdominal
(2001)
dist
ended bowel
dist
ension, hyperbilirubinemia, hyponatr
emia, hypok alemia, hypochlor emia, met abolic alk alosis, high f
ecal chloride concentr
ation Kennea et al [15] MVID 28 35 P olyhydr
amnios, multiple dilat
ed loops of Bir th weight of 3,720 g, male, wat er y diarr hea af ter bir th, s tool (2001)
small and lar
ge bowel
electr
olyt
e study e
xcluded CLD
, small bowel biopsy conf
irmed
MVID
, tr
eatment with TPN and sur
vival
Kim and Kim [26] (2001)
1st pr egnancy CLD 25 33 Multiple dilat
ed bowel loops with perist
alsis Deliver y at 38 wk , male, wat er y diarr hea af ter bir th without e vidence
of mechanical bowel obstruction, wat
er
y stool with ionic cont
ent, recover y af ter electr olyt e corr ection 2nd pr egnancy CLD 30 26 P olyhydr amnios, dilat ed bowel loops Family histor y of a pr
evious child with CLD
, deliver y at 38 wk , male, CLD , electr olyt e r eplacement and r ecover y T sukimori CLD 36 32 P olyhydr amnios, gener
alized dilation of the bowel with
Deliver y at 36 wk , 2,755 g, male, wat er y diarr hea, high stool et al [27] (2007) perist alsis, negative TR OCH t est, amnior eduction, chloride concentr ation, r ecover y af ter electr olyt e corr ectio n AF: 46,XY , elevat ed AF chloride level Colombani et al [18] (2010) Case 1 CLD 27 27 P olyhydr amnios, f et
al bowel dilation, multiple dilat
ed Deliver y at 34 wk , 2,300 g, male, wat er y diarr
hea, high chlo
ride in
bowel loops, AF chloride level at the up
per thr eshold stool, r ecover y, a mut ation of the SL C26A3 gene
of normal values, normal k
ar
yotype at amniocent
and Jouppila [16] first reported distended loops of fetal intestine and polyhydramnios at 26–35 gestational weeks in three fetuses affected with congenital chlo-ride diarrhea. Langer et al [17] reported a false diag-nosis of intestinal obstruction in a fetus with congenital chloride diarrhea. The fetus manifested multiple dilated fluid-filled loops of intestine and polyhydram-nios on prenatal ultrasound similar to that seen with intestinal obstruction. Kennea et al [15] reported con-genital MVID presenting as prenatal bowel obstruction in a 35-gestational-week fetus with polyhydramnios and multiple dilated loops of small and large bowel. They suggested that ultrasound may prenatally identify some cases with MVID, and careful postnatal assessment of congenital enteropathy is needed in such cases if there is no evidence of bowel obstruction. Colombani et al [18] reported prenatal diagnosis of multiple dilated bowel loops, polyhydramnios and elevated amniotic fluid electrolyte concentrations in two cases with genital chloride diarrhea and in two cases with con-genital sodium diarrhea at 22–30 gestational weeks.
Since MVID is an autosomal recessive disorder, the recurrence risk is 25% for the family that has had a pre-vious affected child with MVID. Currently, prenatal diag-nosis can be made by molecular genetic diagdiag-nosis in early pregnancy or by preimplantation genetic diagno-sis in addition to prenatal ultrasound diagnodiagno-sis of a dilated bowel and polyhydramnios in pregnancies with a positive family history. We suggest that MVID be con-sidered a possible diagnosis in cases in which prenatal ultrasound findings manifest a distended bowel in combination with polyhydramnios.
Acknowledgments
This work was supported by research grants NSC-96-2314-B-195-008-MY3 and NSC-97-2314-B-195-006-MY3 from the National Science Council, and MMH-E-99004 from Mackay Memorial Hospital, Taipei, Taiwan.
References
1. Berni Canani R, Terrin G, Cardillo G, Tomaiuolo R,
Castaldo G. Congenital diarrheal disorders: improved under-standing of gene defects is leading to advances in intestinal physiology and clinical management. J Pediatr Gastroenterol Nutr 2010;50:360–6.
2. Davidson GP, Cuiz E, Hamilton JR, Gall DG. Familial
enteropathy: a syndrome of protracted diarrhea from birth, failure to thrive, and hypoplastic villous atrophy. Gastro-enterology 1978;75:783–90. Case 2 CSD NA 22 P olyhydr
amnios, multiple dilat
ed bowel loops, elevat
ed
Deliver
y at 33 wk
, 3,200
g, f
emale, abdominal dist
ension, ac
id and
AF sodium level, normal k
ar
yotype at amniocent
esis
wat
er
y stool emission, high sodium in the stool, ileostomy
Case 3 CSD NA 30 P olyhydr
amnios, multiple dilat
ed bowel loops, elevat
ed
Consanguineous couple; deliver
y at 37 weeks, 3,300
g, male,
AF sodium level, normal k
ar
yotype at amniocent
esis
abdominal dist
ension, acid and wat
er
y stool emission, high sodium
in stool, f luid r eplacement ther apy Case 4 CLD NA 30 P olyhydr
amnios, multiple dilat
ed bowel loops Deliver y at 32 wk , 2,500 g, f emale, wat er y diarr
hea, high chloride in
the stool, r eplacement ther apy , normal k ar yotype Pr esent case MVID 21 29 Multiple dilat
ed bowel loops, polyhydr
amnios No f amily histor y; deliver ed at 36 wk , 3,335 g, male, dif fuse bo wel 36 dilation, wat er y diarr hea, TPN tr
eatment, bowel biopsy conf
irmed
MVID
, death at 6 months old due to sepsis and multiple or
gan
failur
e, het
er
ozygous nonsense mut
ations in the
MYO5B
gene
CLD
=
congenital chloride diarrhea; TOR
CH
=
to
xoplasmosis, rubella, cytomegalo
virus, her pes sim ple x; AF = amnio tic f luid; NA = no t av ailable; MVID = micro
villus inclusion disease; TPN
= to tal parenter al nutrition; CSD = congenit al sodium diarrhea.
3. Phillips AD, Schmitz J. Familial microvillous atrophy: a clin-icopathological survey of 23 cases. J Pediatr Gastroenterol Nutr 1992;14:380–96.
4. Ruemmele FM, Schmitz J, Goulet O. Microvillous inclusion
disease (microvillous atrophy). Orphanet J Rare Dis 2006;1:22.
5. Iancu TC, Manov I. Ultrastructural aspects of enterocyte
defects in infancy and childhood. Ultrastruct Pathol 2010;34: 117–25.
6. Müller T, Hess MW, Schiefermeier N, et al. MYO5B mutations
cause microvillus inclusion disease and disrupt epithelial cell polarity. Nat Genet 2008;40:1163–5.
7. Rodriguez OC, Cheney RE. Human myosin-Vc is a novel
class V myosin expressed in epithelial cells. J Cell Sci 2002; 115:991–1004.
8. Erickson RP, Larson-Thome K, Valenzuela RK, Whitaker SE,
Shub MD. Navajo microvillous inclusion disease is due to a mutation in MYO5B. Am J Med Genet 2008;146A:3117–9.
9. Ruemmele FM, Müller T, Schiefermeier N, et al.
Loss-of-function of MYO5B is the main cause of microvillus inclusion disease: 15 novel mutations and a CaCo-2 RNAi cell model. Hum Mutat 2010;31:544–51.
10. Oliva MM, Perman JA, Saavedra JM, Young-Ramsaran J, Schwarz KB. Successful intestinal transplantation for micro-villous inclusion disease. Gastroenterology 1994;106:771–4. 11. Herzog D, Atkison P, Grant D, Paradis K, Williams S,
Seidman E. Combined bowel-liver transplantation in an infant with microvillous inclusion disease. J Pediatr Gastroenterol Nutr 1996;22:405–8.
12. Randak C, Langnas AN, Kaufman SS, Phillips AD, Wisecarver JL, Hadorn H-B, Vanderhoof JA. Pretransplant management and small bowel-liver transplantation in an in-fant with microvillus inclusion disease. J Pediatr Gastroenterol Nutr 1998;27:333–7.
13. Bunn SK, Beath SV, McKeirnan PJ, et al. Treatment of microvillus inclusion disease by intestinal transplantation. J Pediatr Gastroenterol Nutr 2000;31:176–80.
14. Ruemmele FM, Jan D, Lacaille F, et al. New perspectives for children with microvillous inclusion disease: early small bowel transplantation. Transplantation 2004;77:1024–8.
15. Kennea N, Norbury R, Anderson G, Tekay A. Congenital microvillous inclusion disease presenting as antenatal bowel obstruction. Ultrasound Obstet Gynecol 2001;17:172–4. 16. Kirkinen P, Jouppila P. Prenatal ultrasonic findings in
con-genital chloride diarrhoea. Prenat Diagn 1984;4:457–61. 17. Langer JC, Winthrop AL, Burrows RF, Issenman RM, Caco C.
False diagnosis of intestinal obstruction in a fetus with con-genital chloride diarrhoea. J Ped Surg 1991;26:1282–4. 18. Colombani M, Ferry M, Toga C, et al. Magnetic resonance
imaging in the prenatal diagnosis of congenital diarrhea. Ultrasound Obstet Gynecol 2010;35:560–5.
19. Groli C, Zucca S, Cesaretti A. Congenital chloridorrhea: ante-natal ultrasonographic appearance. J Clin Ultrasound 1986; 14:293–5.
20. Patel PJ, Kolawole TM, Ba’Aqueel HS, Al-Jisi N. Antenatal sonographic findings of congenital chloride diarrhea. J Clin Ultrasound 1989;17:115–8.
21. Rose NC, Kaplan P, Scott S, Kousoulis A, Librizzi R. Prenatal presentation of congenital chloride diarrhea: clinical report and review of the literature. Am J Perinatol 1992;9:398–400. 22. Poggiani C, Auriemma A, Menghini P, Lando B, Bonhoeffer P, Colombo A. Darrow-Gamble disease: ultrasonographic and radiographic findings. Pediatr Radiol 1993;23:65–6. 23. Lundkvist K, Ewald U, Lindgren PG. Congenital chloride
diarrhoea: a prenatal differential diagnosis of small bowel atresia. Acta Paediatr 1996;85:295–8.
24. Rowlands S, Kasby C, Poon C, Murray H. Antenatal ultra-sound diagnosis of dilated fetal bowel due to congenital chlo-ride diarrhoea. Aust N Z J Obstet Gynaecol 1996;36:366–8. 25. Husu S, Nelson N, Selbing A. Prenatal bowel dilatation:
congenital chloride diarrhoea. Arch Dis Child Fetal Neonatal Ed 2001;85:F65.
26. Kim SH, Kim SH. Congenital chloride diarrhea: antenatal ultrasonographic findings in siblings. J Ultrasound Med 2001; 20:1133–6.
27. Tsukimori K, Nakanami N, Wake N, Masumoto K, Taguchi T. Prenatal sonographic findings and biochemical assessment of amniotic fluid in a fetus with congenital chloride diarrhea. J Ultrasound Med 2007;26:1805–7.