行政院國家科學委員會補助專題研究計畫成果報告
※※※※※※※※※※※※※※※※※※※※※※※※※
※ ※
※ 中國人之白袍高血壓的研究(III) ※
※ Study on White Coat Hypertension in Chinese (III) ※
※ ※
※※※※※※※※※※※※※※※※※※※※※※※※※
計畫類別:3個別型計畫 □整合型計畫
計畫編號:NSC89-2314-B-002-067
執行期間:88 年 8 月 1 日至 89 年 7 月 31 日
計畫主持人:曾淵如 教授
執行單位:國立台灣大學醫學院內科
中 華 民 國 八十九 年 十 月 三十 日
行政院國家科學委員會專題研究計畫成果報告
計畫名稱:中國人之白袍高血壓的研究(III)
Study on White Coat Hyper tension in Chinese (III)
計畫編號:NSC89-2314-B-002-067
執行期限:88 年 8 月 1 日至 89 年 7 月 31 日
主持人:曾淵如 教授
執行機構及單位名稱:國立台灣大學醫學院內科
E-mail: [email protected]
中文摘要
以 188 位(88 位男性及 100 位女性), 年齡介於 26 至 75 歲之受檢者,作為有白袍高 血壓之目標器官損傷的研究對象。診斷之隨機 血壓測定是利用傳統水銀柱血壓計。24 小時 移動式血壓的記錄是利用 Del Mar Avionics, 1990 IV 系統之記錄器。目標器官之評估利用 心電圖、胸部 X 光、尿液分析、眼底檢查。 結果,有 6.4%之受檢者有目標器官損 傷,其中胸部 X 光顯示左心室肥厚出現於 1.1%的受檢者,心電圖顯示左心室肥厚出現於 2.7%的受檢者,蛋白尿出現於 1.6%的受檢 者,而視網膜病變出現於 1.1%的受檢者。 因此,白袍高血壓代表孤立性診室高血壓 的較低危險層,但是病人必須確立並規則的追 蹤。 關鍵詞:白袍高血壓,左心室肥厚,蛋白尿, 視網膜病變,移動式血壓Abstr act
To investigate the target organ damage in subjects with white coat hypertension. A total of 188 consecutive subjects (88 men and 100 women), aged 26 to 75 years were studied. Office casual blood pressure measurements were obtained by standard sphygmomanometric methods. 24-hour blood pressures were
recorded by a commercial ambulatory pressure recorder (Del Mar Avionics, model 1990 pressurometer IV system). Their hypertension-related target organ complications were assessed by ECG, chest x-ray, urinalysis and an eye-fundus examinations.
There were 6.4% of the studied subjects with target organ damage. The roentgenographic LVH was found in 1.1% of the studied subjects and the electrocardiographic LVH in 2.7% of the studied subjects. The proteinuria was observed in 1.6% of subjects studied and the retinopathy in 1.1% of subjects studied.
Accordingly, WCH represents a low risk stratum of subjects with isolated office hypertension. However, those subjects should be identified and followed up regularly.
Keywor ds: white coat hypertension, left
ventricular hypertrophy, proteinuria, retinopathy, ambulatory blood pressure.
Introduction
Hypertension has been one of the major risk factors for premature death and disability of adults in developed countries. Anti-hypertension strategy plays an important role on the prevention of the above conditions. However, there are risks of inappropriate therapy. It is difficult to identify subjects who need treatment and correctly labeling individual as hypertension had medical, social and economic importance.
Some patients are identified as having hypertension in the clinical setting but have normal ambulatory, or self-measured blood
pressure (BP) outside the physician's office. This type of hypertension is called white coat hypertension (WCH) [1-3]. Some studies have demonstrated that there is no particular cardiovascular, adverse effects in patients with WCH [4-8]. Some researchers have suggested that such patients are at a relatively low risk of cardiovascular morbidity and that pharmacologic treatment of their blood pressure may be inappropriate [2, 9-18]. Contrarily, it is reported that hemodynamics of subjects with WCH were quite different from those of normotensives [19]. Functional cardiovascular abnormalities were identified in subjects with WCH [20]. Several studies have also demonstrated that white coat hypertensive patients have cardiac structural and functional changes similar to those of persistent hypertensives [21-23]. Therefore, they cannot be considered as having an entirely innocuous condition [4, 24-32]. They do benefit from anti-hypertensive treatment [33, 34]. The long-term prognostic significance of WCH has not been established, whether it needs to be treated is yet unclear. The WCH has thus continued to be debated issue regarding its definition and risk. This paper is an attempt to investigate the target organ damage in subjects with WCH.
Materials and Methods
The subjects diagnosed to have mild hypertension without treatment at outpatient clinic and from a mass survey will be enrolled to this study. Signed informed consent were obtained from all participators. Each participator made 5 visits for the study clinic over a 3-4 week periods. The following data were collected: medical history with emphasis on cardiovascular diseases, height, weight, blood chemistry, standardized reading blood pressure measurement on sitting position, urinalysis, electrocardiogram, chest x-ray, echocardiogram, eye ground finding and 24-hour ABPM.
Office BP was measured in standardized fashion using appropriately sized cuff and a random-zero mercury sphygmomanometer. Systolic blood pressure (SBP) was recorded at Konotkoff phase 1, and diastolic blood pressure (DBP) at phase 5. The BP was taken after at least 10 minutes of rest when subjects visited the clinic, and was defined as the average of two sitting blood pressure readings obtained at
2-minute intervals taken on the same arms [35]. All patients in this study fulfilled the following: (1) systolic blood pressure on at least three different clinic visits during a 3-4 week periods are 140 mmHg or higher, or diastolic blood pressure are 90 mmHg or higher or both; (2) no use of anti-hypertensive agents, psychotropic agents or sympathomimetics for at least one month prior to blood pressure measurement; (3) no use of caffeine containing materials and no smoking for at least 2 hours before blood pressure measurements, and (4) no DM, renal disease, coronary or other organic heart disease or secondary hypertension.
24-hour ABPM was carried out using a commercially available automated ambulatory BP recorder (Del Mar Avionics model 1990 pressureometer IV system). Monitoring was done on a work day. All participants were encouraged to pursue a variety or routine activities during monitoring. Each participant kept a diary of his or her activities and sleep during monitoring. All participants were instructed to stay still, with the forearm extended, during each reading. All ambulatory blood pressure (ABP) readings were taken using the participant’s nondominant arm, at a frequency of once every 15 minutes interval from 07:00 to 23:00 (daytime period) and 30 minutes interval from 23:00 to 07:00 (nighttime period). The accuracy of the recorder was cross-checked against blood pressures measured manually through the same cuff system using a “Y” tube connected to a mercury sphygmomanometer at the beginning of the monitoring period. Only those data within 5 mmHg difference between these two measurements were accepted as valid.
The data of ABPM were analyzed by a microcomputer. Any ABP readings that showed an inconsistent increase or decrease in systolic/diastolic BP > 20 mmHg was excluded in this analysis [36]. Tracings were analyzed only if more than 85% of the maximal number of readings during the 24-hour period passes the deletion criteria. The respective mean ambulatory BP for whole-day, daytime or nighttime was separately calculated. Blood pressure loads, blood pressure varieties and circadian blood pressure patterns were analyzed.
ECG evidence of left ventricular hypertrophy was based on criteria of Sokolow and Lyon [37] cardiac enlargement by radiological examination was diagnosed as a cardiothoracic ratio > 50% [38]. Changes in the optic fundi
were classified according to a modification criteria of Keith et al [39]. Urinalysis was performed with Ames Reagent strips (Multistix 9).
One hundred and eighty-eight consecutive subjects who had abnormally elevated blood pressure (systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg or both) in the outpatient clinic but a normal ABP average were included in this study. Their ages ranged from 26 to 75 years. They consisted of 88 men and 100 women.
Results
The target organ complication was observed in 12 (6.4%) of 188 subjects with WCH. Most of them were under the age of 60 years. Equal number was for both sexes.
The Roentgenographic Left Ventricular Hypertrophy in Subjects with White Coat Hypertension (Table 1)
The roentgenographic left ventricular hypertrophy was found in 2 (1.1%) of 188 subjects with WCH. There was no predilection for groups in terms of age, sex and ABP threshold levels.
The Electrocardiographic Left Ventricular Hypertrophy in Subjects with White Coat Hypertension (Table 2)
The electrocardiographic left ventricular hypertrophy was noted in 5 (2.7%) of 188 subjects with WCH. The abnormal ECG finding was observed in subjects under age of 60 years, and in 2 men and 3 women. There was still no predilection for study groups in terms of age, sex and ABP threshold levels.
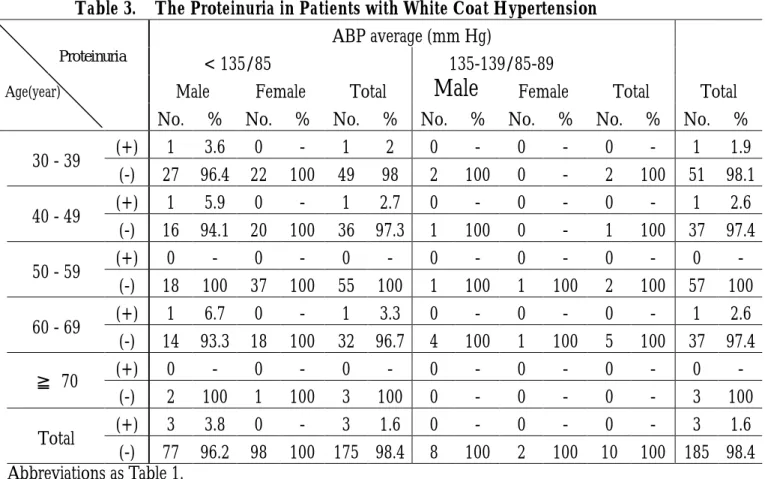
The Proteinuria in Subjects with White Coat Hypertension (Table 3)
Porteinuria was found in 3 (1.6%) of 188 subjects with WCH. They were men. However, this proteinuria occurred without significant predilection for groups in terms of age, sex and ABP threshold levels.
The Retinopathy in Subjects with White Coat Hypertension (Table 4)
Retinopathy was observed in 2 (1.1%) of 188 subjects with WCH. There were women and under age of 60. However, this complication still
occurred without significant predilection for groups in terms of age, sex and ABP threshold levels.
Discussion
Blood pressure levels have been shown to be positively and continuously related to the cardiovascular event [40,41] and renal disease [42]. Hypertension has been considered as one of the major risk factors for morbidity and mortality of cardiovascular system. The clinical significance and the prognostic implications of the so-called white coat hypertension is still not agree upon. Controversy remains on whether WCH is a benign clinical condition or carries an increased risk of target organ damage [2-6, 11, 12, 21, 22, 25, 43-50]. Some researchers concluded that WCH is associated with degree of hypertensive complications [3, 4, 12, 21, 44, 46-48]. The other authors claimed that WCH is not a harmful condition [2, 5, 6, 11, 25, 45]. Some studies have reported that WCH are characterized by alternated left ventricular function [21, 22] and associated with increased left ventricular mass [3, 4, 12, 21, 22, 44, 46-50]. Other studies have not shown the association between WCH with cardiac function [2], and with cardiac structural change [5, 6, 11, 25, 45]. In our study, only 1.1% of subjects with WCH had roentgenographic LVH and 2.7% of subjects had electrocardiographic LVH.
Burnier et al [44] found the increased renal dysfunction in patients with WCH. Hoegholm et al [12] noted the increase microalbuminuria in patients with WCH, but Palatini and colleagues [27] observed that no significant differences in urine albumin were found between the white coat hypertensives and the normotensive subjects. In our study, proteinuria was found only in 1.6% of subjects with WCH.
Palatini and colleagues [48] reported the increased retinopathy in subjects with WCH. But the retinopathy was found in 1.1% of our subjects with WCH.
Our study demonstrated that 6.4% of subjects with WCH had target organ damage. Therefore, WCH represents a low risk stratum of subjects with isolated office hypertension. However, those subjects should be identified and followed up regularly.
References
1. Pickering TG, James GD, Boddie C, Harshfield GA, Blank S, Laragh JH: How common is white coat hypertension? JAMA 259; 225-228, 1988.
2. White WB, Schulman P, McCabe EJ, Dey HM: Average daily blood pressure, not office blood pressure, determines cardiac function in patients with hypertension. J Am Med Assoc 261; 873-877, 1989.
3. Julius S, Mejia A, Jones K, et al: “White
coat” versus “sustained” borderline hypertension in Tecumseh, Michigan. Hypertension 16; 617-623, 1990.
4. Cardillo C, De Felice F, Campia U, Folli G: Psychophysiological reactivity and cardiac end organ changes in white coat hypertension. Hypertension 21; 836-844, 1993.
5. Hoegholm A, Kristensen KS, Bang LE, Nielsen JW, Nielsen WB, Madsen NH: Left ventricular mass and geometry in patients with established hypertension and white coat hypertension. Am J Hypertens 6; 282-286, 1993.
6. Cavallini C, Roman MJ, Pickering TG, Schwartz JE, Pini R, Devereux RB: Is white coat hypertension associated with arterial disease or left ventricular hypertrophy? Hypertension 26; 413-419, 1995.
7. Cuspidi C, Marabini M, Lonati L, Sampieri L, Comerio G, Pelizzoli S, et al: Cardiac and carotid structure in patients with established hypertension and white-coat hypertension. J Hypertens 13; 1707-1711, 1995.
8. Ferrara LA, Guida L, Pasanisi F, Celentano AI, Palmieri V, Iannuzzi R, et al: Isolated office hypertension and end organ damage. J Hypertens 15; 979-985, 1997.
9. Pickering TG, Friedman R: The white coat effect: a neglected role for behavioral factors in hypertension. In: McCabe PM, Schniderman N, Field TM, et al, eds. Stress, Coping and Disease. Hillsdale: LR Erlbaum, p. 35-49, 1991.
10. Boone JL: Stress and hypertension. In: Boone JL, ed. Primary Care; Vol 18. “Clinics in office practice.” Philadelphia: WB Saunders, p. 623-650, 1991.
11. Gosse P, Promax H, Durandet P, Clementy
J: “White coat” hypertension. No harm for the heart. Hypertension 22; 766-770, 1993.
12. Hoegholm A, Bang LE, Kristensen KS, Nielsen JW, Holm J: Microalbumin- uria in 411 untreated individuals with established hypertension, white coat hypertension, and normotension. Hypertension 24; 101-105, 1994.
13. Verdecchia P, Schillaci G, Borgioni C, Giucci A, Zampi I, Gattobigio R, Sacchi N, Porcellati C: White coat hypertension and white coat effect. Similarities and differences. Am J Hypertens 8; 790-798, 1995.
14. Kario K, Matsuo T, Kobayashi H, Matsuo M, Sakata T, Miyata T, Shimada K: Factor VII hyperactivity and endothelial cell damage are found in elderly hypertensives only when concomitent with microalbuminuria. Atheroscl Throm Vas Biol 16; 455-461, 1996.
15. Hoegholm A, Kristensen KS, Bang LE, Nielsen JW: White coat hypertension and target organ involvement: the impact of different cut-off levels on albuminuria and left ventricular mass and geometry. J Human Hypertens 12; 433-439, 1998. 16. Pierdomenico SD, Costantini F, Bucci A,
De Cesaare D, Cuccurullo F, Mezzetti A: Low-density lipoprotein oxidation and vitamins E and C in sustained and white-coat hypertension. Hypertension 31; 621-626, 1998.
17. Verdecchia P, Schillaci G, Borgioni C, Ciucci A: White coat hypertension not guilty when correctly defined. Blood Press Monit 3; 147-152, 1998.
18. Mallion JM, Baguet JP, Siche JP, Tremel F, De Gaudemaris R: Clinical value of ambulatory blood pressure monitoring. J Hypertens 17; 585-595, 1999.
19. Soma J, Aakhus S, Dahl K, Slordahl S, Wiseth R, Wideroe TE, Skjaerpe T: Hemodynamics in white coat hypertension compared to ambulatory hypertension and normotension. Hypertension 10; 17-20, 1996.
20. Glen SK, Elliott ML, Curzio JL, Lees KR, Reid JL: White coat hypertension as a cause of cardiovascular dysfunction. Lancet 348; 654-657, 1996.
Kuramoto K: Is white coat hypertension innocent? Structure and function of the heart in the elderly. Hypertension 22; 826-831, 1993.
22. Pose-Reino A, Gonzalez-Juanate Y JR, Pastor C, Mendez I, Estevez JC, Alvarez D, et al: Clinical implications of white coat hypertension. Blood Press 5; 264-273, 1996.
23. Soma J, Wideroe TE, Dahl K, Rossvoll O, Skjaerpe T: Left ventricular systolic and diastolic function assessed with two-dimenional and doppler echocardiography in "white coat" hypertension. J Am Coll Cardiol 28; 190-196, 1996.
24. Verdecchia P, Schillaci G, Boldrini F, Zampi I, Porcellati C: Variability between current definitions of “normal” ambulatory blood pressure. Implications in the assessment of white coat hypertension. Hypertension 20; 555-562, 1992.
25. Cerasola G, Cottone S, Nardi E, D’Ignoto G, Volpe V, Mule G, Carollo C: White coat hypertension and cardiovascular risk. J Cardiovas Risk 2; 545-549, 1995.
26. Rizzo V, Cicconetti P, Bianchi A, Lorido A, Morelli S, Vetta F, Salza MC, Marigliano V: White-coat hypertension and cardiac damage in elderly subjects. J Human Hypertens 10; 293-298, 1996.
27. Palatini P, Mormino P, Santonastaso M, Mos L, Dal Follo M, Zanata G, Pessina AC: Target-organ damage in stage I hypertensive subjects with white coat and sustained hypertension: results from the HARVEST study. Hypertension 31; 57-63, 1998.
28. Muscholl MW, Hense HW, Brockel U, Doring A, Riegger GA, Schunkert H: Changes in left ventricular structure and function in patients with white coat hypertension: cross sectional survey. BMJ 317; 565-570, 1998.
29. Carmona J, Amado P, Vasconcelos N, Santos I, Pinto C, Forte G, Arsenio A, Nazare J: “White-coat hypertension”: variation of normality or of hypertension? Revista Portuguesa de Cardiol 17; 505-512, 1998.
30. Feola M, Boffano GM, Procopio M, Reynaud S, Allemano P, Rizzi G: Ambulatory 24-hour blood pressure monitoring: correlation between blood pressure variability and left ventricular
hypertrophy in untreated hypertensive patients. Giornale Italiano di Cardiol 28; 38-44, 1998.
31. Bar J, Maymom R, Padoa A, Wittenberg C, Boner G, Ben Rafael Z, Hod M: White coat hypertension and pregnancy outcome. J Human Hypertens 13; 541-545, 1999. 32. Pickering T, Levenstein M, Walmsley for
Hypertension and Lipid Trial Study Group: Differential effects of doxazosin on clinic and ambulatory pressrue according to age, gender and prevalence of white coat hypertension. Results of HALT study. Am J Hypertens 7; 848-852, 1994.
33. Waeber B, Heynen G, Bruner HR: Analysis of ambulatory blood pressure monitoring: the problem of white coat hyeprtension. Responders and no responders. Blood Pressure Monit 1; 289-291, 1996.
34. Pickering TG: White coat hypertension. In: Waeber B, O‘Brien E, O’Malley K, eds. Twenty-Four-Hour Ambulatory Blood Pressure Monitoring in Clinical Practice. New York: Raven Press, p. 33-45, 1994.
35. National high blood pressure education program coordinating committee. Sixth Joint National Committee Report on the Detection, Evaluation and Treatment of High Blood Pressure (JNC VI). Arch Intern Med 157; 2413-2445, 1997.
36. Drayer JIM, Weber MA, DeYoung JL, Wyle FA: Circadian blood pressure patterns in ambulatory hypertensive patients. Am J Med 93; 493-499, 1982.
37. Sokolow M, Lyon TP: The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J 37; 161-186, 1949. 38. Ungerleider HE, Gubner R: Evaluation of
heart size measurements. Am Heart J 24; 494-510, 1942.
39. Keith NM, Wagener HP, Barker NW: Some different types of essential hypertension: their course and prognosis. Am J Med Sci 268; 336-345, 1974.
40. Eastern Stroke and Coronary Heart Disease Collaborative Research Group. Blood pressure, cholesterol and stroke in Eastern Asia. Lancet 352; 1801-1807, 1998.
41. Mac Mahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J, et al: Blood pressure,
stroke, and coronary heart disease. Part 1. Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 335; 765-774, 1990.
42. Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Ford CE, et al: Blood pressure and end-stage renal disease in men. N Engl J Med 334; 13-18, 1996.
43. Hoegholm A, Kristensen KS, Madsen NH, Svendsen TL: White coat hypertension diagnosed by 24-h ambulatory monitoring. Examination of 159 newly diagnosed hypertensive patients. Am J Hypertens 5; 64-70, 1992.
44. Burnier M, Biollaz J, Magnin JL, Bidlingmeyer M, Brunner HR: Renal sodium handing in patients with untreated hypertension and white coat hypertension. Hypertension 23; 496-502, 1994.
45. Verdecchia P, Porcellati C, Schillaci G, Borgioni G, Ciucci A, Battistelli M, Guerrieri M, Gatteschi C, Zampi I, Santucci A, Santucci C, Reboldi G: Ambulatory blood pressure: an independent predictor of prognosis in essential hypertension. Hypertension 24; 793-801, 1994.
46. Weber MA, Neutel JM, Smith DHG,
Graettinger WF: Diagnosis of mild hypertension by ambulatory blood pressure monitoring. Circulation 90; 2291-2298, 1994.
47. Pierdomenico SD, Lapenna D, Guglielmi MD, Antidormi T, Schiavone C, Cuccurullo F, Mezzetti A: Target-organ status and serum lipids in patients with white coat hypertension. Hypertension 26; 801-807, 1995.
48. Palatini P, Penzo M, Canali C, Dorigatti F, Pessina AC: Interactive action of the white coat effect and the blood pressure levels on cardiovascular complications in hypertension. Am J Med 103; 208-216, 1997.
49. Pickering TG: White coat hypertension. Curr Opin Nephr Hypertens 5; 192-198, 1996.
50. Muscholl MW, Hense HW, Bröckel U, Döring A, Riegger GAJ, Schunkert H. Changes in left ventricular structure and function in patients with white coat hypertension: cross sectional survey. BMJ 317; 565-570, 1998.
Table 1. The Roentgenographic Left Ventricular Hypertrophy in Subjects with White Coat Hypertension
ABP average (mm Hg)
< 135/85 135-139/85-89
Male Female Total
Male
Female Total TotalAge(year) LVH
No. % No. % No. % No. % No. % No. % No. % (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -30 - 39 (-) 28 100 22 100 50 100 2 100 0 - 2 100 52 100 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -40 - 49 (-) 17 100 20 100 37 100 1 100 0 - 1 100 38 100 (+) 1 5.6 1 2.7 2 3.6 0 - 0 - 0 - 2 3.5 50 - 59 (-) 17 94.4 36 97.3 53 96.4 1 100 1 100 2 100 55 96.5 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -60 - 69 (-) 15 100 18 100 33 100 4 100 1 100 5 100 38 100 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -≧ 70 (-) 2 100 1 100 3 100 0 - 0 - 0 - 3 100 (+) 1 1.3 1 1 2 1.1 0 - 0 - 0 - 2 1.1 Total (-) 79 98.7 97 99 176 98.9 8 100 2 100 10 100 186 98.9 ABP: ambulatory blood pressure, LVH: left ventricular hypertrophy, (+) : presence (-): absence
Table 2. The Electrocardiographic Left Ventricular Hypertrophy in Subjects with White Coat Hypertension
ABP average (mm Hg)
< 135/85 135-139/85-89
Male Female Total
Male
Female Total TotalAge(year) LVH
No. % No. % No. % No. % No. % No. % No. % (+) 0 - 1 4.5 1 2 0 - 0 - 0 - 1 1.9 30 - 39 (-) 28 100 21 95.5 49 98 2 100 0 - 2 100 51 98.1 (+) 1 5.9 1 5 2 5.4 0 - 0 - 0 - 2 5.3 40 - 49 (-) 16 94.1 19 95 35 94.6 1 100 0 - 1 100 36 94.7 (+) 1 5.6 1 2.7 2 3.6 0 - 0 - 0 - 2 3.5 50 - 59 (-) 17 94.4 36 97.3 53 96.4 1 100 1 100 2 100 55 96.5 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -60 - 69 (-) 15 100 18 100 33 100 4 100 1 100 5 100 38 100 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -≧ 70 (-) 2 100 1 100 3 100 0 - 0 - 0 - 3 100 (+) 2 2.5 3 3.1 5 2.8 0 - 0 - 0 - 5 2.7 Total (-) 78 97.5 95 96.9 173 97.2 8 100 2 100 10 100 183 97.3 Abbreviations as Table 1.
Table 3. The Proteinuria in Patients with White Coat Hypertension
ABP average (mm Hg)
< 135/85 135-139/85-89
Male Female Total
Male
Female Total TotalAge(year)
No. % No. % No. % No. % No. % No. % No. % (+) 1 3.6 0 - 1 2 0 - 0 - 0 - 1 1.9 30 - 39 (-) 27 96.4 22 100 49 98 2 100 0 - 2 100 51 98.1 (+) 1 5.9 0 - 1 2.7 0 - 0 - 0 - 1 2.6 40 - 49 (-) 16 94.1 20 100 36 97.3 1 100 0 - 1 100 37 97.4 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -50 - 59 (-) 18 100 37 100 55 100 1 100 1 100 2 100 57 100 (+) 1 6.7 0 - 1 3.3 0 - 0 - 0 - 1 2.6 60 - 69 (-) 14 93.3 18 100 32 96.7 4 100 1 100 5 100 37 97.4 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -≧ 70 (-) 2 100 1 100 3 100 0 - 0 - 0 - 3 100 (+) 3 3.8 0 - 3 1.6 0 - 0 - 0 - 3 1.6 Total (-) 77 96.2 98 100 175 98.4 8 100 2 100 10 100 185 98.4 Abbreviations as Table 1.
Table 4. The Retinopathy in Subjects with White Coat Hypertension
ABP average (mm Hg)
< 135/85 135-139/85-89
Male Female Total
Male
Female Total TotalAge(year)
No. % No. % No. % No. % No. % No. % No. % (+) 0 - 1 4.5 1 2 0 - 0 - 0 - 1 1.9 30 - 39 (-) 28 100 21 95.5 49 98 2 100 0 - 2 100 51 98.1 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -40 - 49 (-) 17 100 20 100 37 100 1 100 0 - 1 100 38 100 (+) 0 - 1 2.7 1 1.8 0 - 0 - 0 - 1 1.8 50 - 59 (-) 18 100 36 97.3 54 98.2 1 100 1 100 2 100 56 98.2 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -60 - 69 (-) 15 100 18 100 33 100 4 100 1 100 5 100 38 100 (+) 0 - 0 - 0 - 0 - 0 - 0 - 0 -≧ 70 (-) 2 100 1 100 3 100 0 - 0 - 0 - 3 100 (+) 0 - 2 2 2 1.1 0 - 0 - 0 - 2 1.1 Total (-) 80 100 96 98 176 98.9 8 100 2 100 10 100 186 98.9 Abbreviations as Table 1. Retino-pathy Proteinuria