Published Ahead of Print 16 December 2011.
10.1128/AEM.05605-11.
2012, 78(4):1107. DOI:
Appl. Environ. Microbiol.
and Hung-Chih Lin
Feng-Rong Chuang, Chiu-Ching Huang, Chih-Hsueh Lin
Chang, Yi-Ying Wu, Chu-Huang Chen, Chi-Yuan Li,
Chung-Chih Lin, Hsin-Hung Lin, Yao-Lung Liu, Yi-Chih
Liang, Chiz-Tzung Chang, Huey-Liang Kuo, Ya-Fei Yang,
I-Kuan Wang, Hsueh-Chou Lai, Cheng-Ju Yu, Chih-Chia
Microbiotas in Peritoneal Dialysis Patients
Real-Time PCR Analysis of the Intestinal
http://aem.asm.org/content/78/4/1107
Updated information and services can be found at:
These include:
REFERENCEShttp://aem.asm.org/content/78/4/1107#ref-list-1
at:
This article cites 37 articles, 14 of which can be accessed free
CONTENT ALERTS
more»
articles cite this article),
Receive: RSS Feeds, eTOCs, free email alerts (when new
http://aem.asm.org/site/misc/reprints.xhtml Information about commercial reprint orders:
http://journals.asm.org/site/subscriptions/ To subscribe to to another ASM Journal go to:
on January 30, 2012 by guest
http://aem.asm.org/
Dialysis Patients
I-Kuan Wang,a,b,c,dHsueh-Chou Lai,eCheng-Ju Yu,eChih-Chia Liang,bChiz-Tzung Chang,bHuey-Liang Kuo,bYa-Fei Yang,b
Chung-Chih Lin,bHsin-Hung Lin,bYao-Lung Liu,bYi-Chih Chang,fYi-Ying Wu,fChu-Huang Chen,a,dChi-Yuan Li,aFeng-Rong Chuang,g
Chiu-Ching Huang,bChih-Hsueh Lin,hand Hung-Chih Lini,j
Graduate Institute of Clinical Medical Science, College of Medicine, China Medical University, Taichung, Taiwana; Divisions of Kidney Disease, China Medical University
Hospital, Taichung, Taiwanb; Department of Internal Medicine, College of Medicine, China Medical University, Taichung, Taiwanc; L5 Center, China Medical University
Hospital, Taichung, Taiwand; Department of Gastrointestinal Disease, China Medical University Hospital, Taichung, Taiwane; Department of Medical Laboratory Science
and Biotechnology, China Medical University, Taichung, Taiwanf; Division of Nephrology, Kaohsiung Chang Gung Memorial Hospital, and Chang Gung University College
of Medicine, Kaohsiung, Taiwang; Department of Family Medicine, China Medical University Hospital, Taichung, Taiwanh; and School of Chinese Medicine, College of
Chinese Medicine, China Medical University, Taichung, Taiwani; and Department of Pediatrics, China Medical University Hospital, Taichung, Taiwanj
Bifidobacterium and Lactobacillus can beneficially affect the host by producing acetic acid and lactic acid, which lower pH and
thereby inhibit the growth of pathogens or allow the probiotic bacteria to compete with pathogens for epithelial adhesion sites
and nutrients. The transmural migration of enteric organisms into the peritoneal cavity can cause peritonitis in peritoneal
dialy-sis (PD) patients. We hypothesized that the composition of the intestinal microbiota with regard to Lactobacillus species and
Bifidobacterium species differed between PD patients and healthy controls. The aim of the study was to investigate these
differ-ences by real-time PCR analysis of fecal samples. From 1 August 2009 to 31 March 2010, a total of 29 nondiabetic PD patients and
41 healthy controls from China Medical University Hospital were recruited after giving their informed consent. Fecal samples
were collected from the PD patients and their age-matched counterparts in the morning using a standardized procedure. DNA
extracted from these samples was analyzed by real-time PCR. All bifidobacteria, Bifidobacterium catenulatum, B. longum, B.
bifidum, Lactobacillus plantarum, L. paracasei, and Klebsiella pneumoniae were less frequently detected in the patient samples.
Dysbiosis (microbial imbalance) may impair intestinal barrier function and increase host vulnerability to pathogen invasion.
Further studies are necessary to confirm our findings before clinical trials with probiotic supplementation in PD patients.
T
here is a large, complex, and diverse microbial community in
the human intestine. The intestinal microbiota plays an
im-portant role in digesting food, metabolizing endogenous and
ex-ogenous compounds, and producing essential vitamins. It also
stimulates the immune system and prevents the colonization of
the gastrointestinal tract by pathogens, and hence it influences
human health (7, 9). The gastrointestinal microbiota of an adult
human consists of more than 500 species, with 10
11to 10
12CFU
per gram of stool (12, 25). The predominant microorganisms are
non-spore-forming, obligate anaerobes, such as Bacteroides,
Fuso-bacterium, EuFuso-bacterium, and Bifidobacterium species. Other
an-aerobic bacteria found in large numbers include Lactobacillus
spe-cies, various anaerobic Gram-positive cocci, and Clostridium
species (4). Hida et al. studied the fecal flora of hemodialysis (HD)
patients and healthy controls using traditional plating methods
and found quantitative and qualitative differences between the
two groups (13). It is plausible to suggest that the chronic
inflam-matory state in dialysis patients is in part due to a microbial
im-balance in the gut, resulting in alteration of proinflammatory
cy-tokines and production of uremic toxins from proteins fermented
in the large intestine (16). Moreover, impaired intestinal barrier
function in peritoneal dialysis (PD) patients allows enteric
organ-isms to enter the peritoneal cavity by transmural migration and to
cause peritonitis (8, 27). Peritonitis occasionally causes death and
results in significant morbidity, including catheter loss, transfer to
hemodialysis, transient loss of ultrafiltration, and possible
perma-nent membrane damage (22). Bifidobacterium and Lactobacillus
can beneficially affect the host by inhibiting the growth of
patho-gens through production of acetic acid and lactic acid, which
lower pH, or by competing with pathogens for epithelial adhesion
sites and nutrients (10).
To the best of our knowledge, no study has investigated the
intestinal microbiota in PD patients before. The aim of this study,
therefore, was to evaluate the differences in the intestinal
micro-biota between PD patients and healthy controls by examining
fe-cal samples. We focused on Bifidobacterium species, Lactobacillus
species, Escherichia coli, Klebsiella pneumoniae, Pseudomonas
aeruginosa, and Enterococcus species. E. coli, K. pneumoniae, P.
aeruginosa, and Enterococcus species are the common bacterial
pathogens derived from bowel tissue and causing peritonitis in PD
patients (20).
MATERIALS AND METHODS
Study population. Between 1 August 2009 and 31 March 2010, we
re-cruited nondiabetic PD patients and healthy controls from China Medical University Hospital, a tertiary-care medical center in central Taiwan. The inclusion criteria were PD for more than 3 months, absence of diabetes, at least 18 years of age, and an estimated glomerular filtration rate of⬍15 ml/min. Exclusion criteria were active infectious conditions within the previous 30 days, pregnancy, autoimmune diseases, or the consumption
Received 25 May 2011 Accepted 6 December 2011 Published ahead of print 16 December 2011
Address correspondence to Hung-Chih Lin, [email protected]. Copyright © 2012, American Society for Microbiology. All Rights Reserved.
doi:10.1128/AEM.05605-11
on January 30, 2012 by guest
http://aem.asm.org/
of antibiotics or yogurt within 30 days prior to sample collection. The protocol of this study was approved by the Institutional Review Board of China Medical University Hospital.
Fecal samples were collected from the PD patients and age-matched adults in the morning after they gave their informed consent to participate in the study. The samples were put immediately on ice and processed within 1 h after defecation.
DNA extraction from fecal samples. One gram of fecal sample was
suspended in a solution containing 10 ml of normal saline and homoge-nized by vortexing for 1 min. The slurry was filtered through sterile gauze to remove any large particles and debris. One ml of filtered fecal solution was placed into a tube and centrifuged at 15,000 rpm for 2 min. The supernatants were discarded, and the pellets were treated with 20l of 6-mg/ml lysozyme and 30l of 50-U/ml mutanolysin at 37°C for 2 h, then with 0.1 ml of 10% sodium dodecyl sulfate and 80l of benzyl chloride at 60°C for 2 h, and finally with 80l of chloroform. After centrifugation at 12,500 rpm for 2 min, the supernatants were collected, and DNA was obtained by alcohol precipitation. Finally, the DNA was suspended in 50 l of deionized water and stored at ⫺80°C before use.
Bacterial strains. All bacterial strains are listed in Table 1.
Species-specific quantitative real-time PCR. The primers and probes
for the 5= nuclease assays were based on sequences of the 16S-23S inter-genic spacer regions of the different Bifidobacterium species and
Lactoba-cillus species according to previous studies (10, 11).
In addition, the primers and probes for Escherichia coli and Bacteroides
fragilis were based on 16S rRNA gene sequences, while those for Klebsiella pneumoniae were based on the phoE gene sequence. The primers and
probes for Pseudomonas aeruginosa and Enterococcus species were based on 23S rRNA gene sequences. Species-specific sequences were used to design primers and probes for Bifidobacterium breve, B. bifidum, B.
catenulatum, B. longum (11), Lactobacillus plantarum, L. rhamnosus, L. paracasei (10), E. coli (14), K. pneumoniae (28), P. aeruginosa (26), Entero-coccus species (6), and B. fragilis (33). All lactobacilli, all bifidobacteria,
and total bacteria were also detected using previously designed primers and probes (10, 11). Table 2 shows the primers and probes used.
TaqMan minor-groove-binding probes were used to increase the specificity and the sensitivity of the assays. Extracted DNA, primers, and probes were added to TaqMan Universal PCR Mastermix (Applied Bio-systems, Foster City, CA) to a final concentration of 1M for each primer and 250 nM for the TaqMan probes.
Real-time PCRs were performed in a Roche LightCycler 480. The tem-perature profile for the amplification was 10 min at 95°C, followed by 60 cycles of 20 s at 95°C, 1 min at 60°C, and 1 s at 72°C. Real-time PCR quantification of species-specific DNA was performed using a standard curve generated from the dilution series of a reference strain (Table 1).
Statistical analysis. Values are expressed as means⫾ standard
devia-tions. Variables were compared using the chi-square test or Fisher’s exact
test for categorical variables. Independent t and Mann-Whitney U tests were used for comparison of continuous variables. All analyses were per-formed using SPSS statistical software (version 12.0 for Windows; SPSS, Inc.). A P value of⬍0.05 was considered significant.
RESULTS
Twenty-nine PD patients (mean age, 53.7
⫾ 11.7 years) and 41
healthy controls (58.2
⫾ 12.8 years) were enrolled (P ⫽ 0.1)
(Ta-ble 3). There was no between-group difference in gender and
mean fecal weight. The major etiology of end-stage renal disease
was chronic glomerulonephritis, accounting for 82.8% of cases.
The mean duration of PD was 49.7
⫾ 35.4 months.
Table 4 shows the detection limits. The detection limits ranged
from 0.05 to 2.53 CFU/ml, which are similar to those in a previous
report (10). Table 5 presents the mean colony numbers in samples
from colonized patients and the percentages of
real-time-PCR-positive fecal samples. Fecal samples from PD patients were less
likely to be positive for all bifidobacteria (P
⬍ 0.001), B.
catenula-tum (P
⫽ 0.003), B. longum (P ⬍ 0.001), B. bifidum (P ⫽ 0.001), L.
plantarum (P
⫽ 0.001), L. paracasei (P ⬍ 0.001), and K.
pneu-moniae (P
⫽ 0.004). However, fecal samples from both groups
were equally likely to contain B. breve, all Lactobacillus spp., E. coli,
P. aeruginosa, Enterococcus species, and B. fragilis. For PD patients,
the mean colony count in samples from colonized patients was
lower for all bacteria (P
⬍ 0.001), L. plantarum (P ⫽ 0.014), K.
pneumoniae (P
⫽ 0.005), and Enterococcus species (P ⬍ 0.001) and
higher for P. aeruginosa (P
⫽ 0.029). In addition, L. rhamnosus
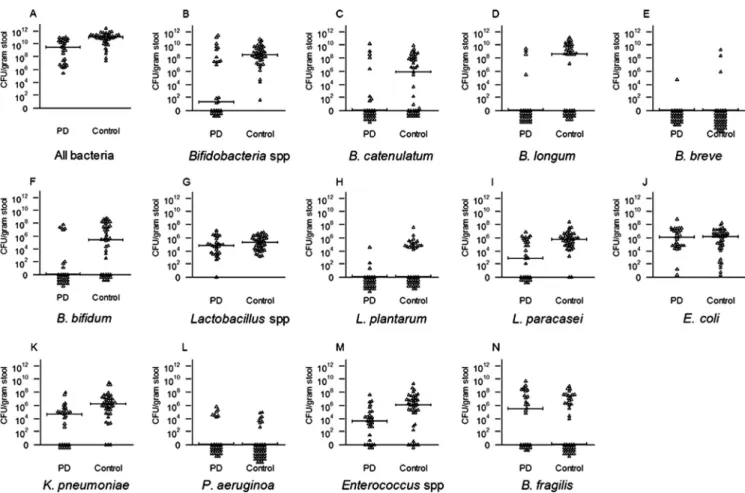
was not detectable in either group. Figure 1 shows the distribution
of bacterial counts in samples from both groups.
DISCUSSION
To the best of our knowledge, this study is the first to analyze
intestinal microbiotas by real-time PCR in PD patients. The
nat-ural intestinal microbiota is disrupted in uremic patients. In 1978,
Simenhoff et al. reported increased numbers of both aerobic (10
6bacteria/ml) and anaerobic (10
7bacteria/ml) organisms in the
duodenum and jejunum of patients with chronic kidney disease
but very low numbers or no bacterial colonies in healthy controls
(29). Hida et al. found no significant difference in the total
num-ber of bacteria in the colon of hemodialysis (HD) patients and
healthy controls using traditional plating methods to analyze fecal
samples (13). However, the HD group had increased numbers of
intestinal aerobic bacteria (E. coli, K. pneumoniae, and
Enterococ-cus) and intestinal anaerobic Clostridium perfringens and
de-creased numbers of intestinal anaerobic bacteria (Bifidobacterium
species).
In our study, fecal samples from PD patients were less likely to
contain all Bifidobacterium species, B. catenulatum, B. longum, B.
bifidum, L. plantarum, L. paracasei, and K. pneumoniae. In adults,
B. catenulatum, B. longum, and B. bifidum are common intestinal
Bifidobacterium species (17, 18), whereas L. plantarum and L.
pa-racasei are common intestinal Lactobacillus species (1, 35). In
con-trast to Hida’s study, our study found no significant
between-group differences in the rate of E. coli detection. Moreover, the
detection rate and bacterial counts for K. pneumoniae were lower
in PD patients.
Several possible mechanisms may account for changes in the
intestinal microbiota in uremic patients. Kalantar-Zadeh et al.
showed that HD patients eat less dietary fiber than healthy
con-trols (12.4
⫾ 5.8 g/day versus 17.9 ⫾ 10.6 g/day; P ⬍ 0.05) (15).
TABLE 1 Bacterial strains used in this study
Organism Straina B. catenulatum ATCC 27539 B. longum ATCC 15707 B. breve ATCC 15700 B. bifidum NCDO 1454 L. plantarum ATCC 14917 L. rhamnosus ATCC 53103 L. paracasei ATCC 11582 E. coli ATCC 25922 K. pneumoniae ATCC 13883 P. aeruginosa ATCC 27853 Enterococcus species DSM 20478 B. fragilis ATCC 25285
aATCC, American Type Culture Collection; NCDO, National Collection of Dairy Organisms; DSM, Deutsche Sammlung von Mikroorganismen und Zellkulturen. Wang et al.
1108 aem.asm.org Applied and Environmental Microbiology
on January 30, 2012 by guest
http://aem.asm.org/
TABLE 2 Primers and probes used in the real-time PCR
Microorganism Primer or probe Sequence (5=¡3=) GenBank accession no. Reference
All bacteria Forward TCCTACGGGAGGCAGCAGT GQ893232.1 11
Reverse GGACTACCAGGGTATCTAATCCTGTT
Probe CGTATTACCGCGGCTGCTGGCAC
All Bifidobacteria Forward GGGATGCTGGTGTGGAAGAGA DQ298393.1 11
Reverse TGCTCGCGTCCACTATCCAGT
Probe TCAAACCACCACGCGCCA
B. catenulatum Forward GTGGACGCGAGCAATGC U09522.1 11
Reverse AATAGAGCCTGGCGAAATCG
Probe AAGCAAACGATGACATCA
B. longum Forward TGGAAGACGTCGTTGGCTTT AP010890.1 11
Reverse ATCGCGCCAGGCAAAA
Probe CGCACCCACCGCA
B. breve Forward GTGGTGGCTTGAGAACTGGATAG AJ245850.1 11
Reverse CAAAACGATCGAAACAAACACTAAA
Probe TGATTCCTCGTTCTTGCTGT
B. bifidum Forward GTTGATTTCGCCGGACTCTTC U09517.1 11
Reverse GCAAGCCTATCGCGCA
Probe ACTCCGCTGGCAACACAAATCATCA
All Lactobacillus spp. Forward TGGATGCCTTGGCACTAGGA AY365115.1 10
Reverse AAATCTCCGGATCAAAGCTTACTTAT
Probe TATTAGTTCCGTCCTTCATC
L. plantarum Forward TGGATCACCTCCTTTCTAAGGAAT AB362387.1 10
Reverse TGTTCTCGGTTTCATTATGAAAAAATA
Probe ACATTCTTCGAAACTTTGT
L. rhamnosus Forward CGGCTGGATCACCTCCTTT AP011548.1 10
Reverse GCTTGAGGGTAATCCCCTCAA
Probe CCTGCACACACGAAA
L. paracasei Forward ACATCAGTGTATTGCTTGTCAGTGAATAC AJ542563.1 10
Reverse CCTGCGGGTACTGAGATGTTTC
Probe TGCCGCCGGCCAG
E. coli Forward CATGCCGCGTGTATGAAGAA JF412031.1 14
Reverse CGGGTAACGTCAATGAGCAAA
Probe TATTAACTTTACTCCCTTCCTCCCCGCTGAA
K. pneumoniae Forward CCTGGATCTGACCCTGCAGTA AF009172.1 28
Reverse CCGTCGCCGTTCTGTTTC
Probe CAGGGTAAAAACGAAGGC
P. aeruginosa Forward TCCAAGTTTAAGGTGGTAGGCTG AJ549386.1 26
Reverse CTTTTCTTGGAAGCATGGCATC
Probe AGGTAAATCCGGGGTTTCAAGGCC
All Enterococcus spp. Forward AGAAATTCCAAACGAACTTG HM007611.1 6
Reverse CAGTGCTCTACCTCCATCATT
Probe TGGTTCTCTCCGAAATAGCTTTAGGGCTA
B. fragilis Forward TCRGGAAGAAAGCTTGCT AB618793.1 33
Reverse CATCCTTTACCGGAATCCT
Probe ACACGTATCCAACCTGCCCTTTACTCG
on January 30, 2012 by guest
http://aem.asm.org/
Although there was no significant between-group difference in
protein intake, potassium restriction compels uremic patients to
reduce vegetable and fruit intake and thereby fiber intake. In
ad-dition, colon transit times are longer in uremic patients. The
prev-alence of constipation is as high as 63% in HD patients and 29% in
PD patients, compared to 10 to 20% in healthy controls (36).
Inactivity, phosphate binders, potassium absorbents, water
re-striction diet, lack of fiber intake, and comorbidities such as
dia-betes may play roles in the high prevalence of constipation in
uremic patients. Because bacterial growth is promoted by
peristal-sis, which mixes fibers with bacteria widely, increased colon
tran-sit time is correlated with reduced bacterial cell mass in stool (3,
30). The populations of lactobacilli and bifidobacteria are reduced
among adults with chronic constipation (23). In our study, the
rate of constipation was 31.0%. The lower counts of all bacteria
and K. pneumoniae in PD patients might be due to a longer colon
transit time. We excluded diabetic patients to eliminate the
founding effect of diabetes. Moreover, markedly increased
con-centrations of urea, creatinine, and other nitrogen metabolites
accumulate in the blood and diffuse into the gut, where they
be-come accessible to microbial metabolism. Fecal ammonia is
mainly derived from bacterially mediated hydrolysis of urea.
Thus, a high level of ammonia is responsible for elevation of
lu-minal and fecal pH, which might lead to changes in the intestinal
microbiota in uremic patients (4).
Probiotics containing Bifidobacterium species and Lactobacillus
species could beneficially affect the host by suppressing the growth or
epithelial invasion of pathogenic bacteria, improving intestinal
bar-rier function, and modulating immune system activity (2, 5, 19, 24).
Few studies have assessed the possible benefit of probiotics for
pa-tients with chronic kidney disease. The demonstrated benefits in HD
patients include reduction of plasma levels of uremic toxins,
espe-cially those of indoxyl sulfate and p-cresol, inhibition of overgrowth
of aerobic bacteria (13, 21, 31), decrease in pre-HD serum levels of
homocysteine (probably as a result of folate produced by B. longum in
the intestine), and normalization of bowel habits (21, 32).
Rangana-than et al. (23a) reported that probiotics containing L. acidophilus, B.
longum, and S. thermophilus significantly reduced blood urea
nitro-gen and improved the quality of life without serious side effects in
patients with stage 3 and 4 chronic kidney disease. Our scientific
ev-idence justifies proceeding with clinical trials to evaluate the efficacy
of oral probiotics in PD patients.
There are several limitations to our study. The small number of
patients may have led to the chance occurrence of statistically
significant results. In addition, L. rhamnosus, a common
Lactoba-cillus species, was not detectable in either group. L. rhamnosus can
TABLE 3 Characteristics of the PD patients (n⫽ 29) and healthy
controls (n⫽ 41)
Characteristic PD patients Controls P value
Age (yr) 53.7⫾ 11.7a 58.2⫾ 12.8a 0.13
Gender (F/M) 19/10 26/15 0.86b
No (%) with ESRDcetiology
Chronic glomerulonephritis 24 (82.8) Tubulointerstitial nephritis 3 (10.3) Hypertension 2 (6.9) Duration of dialysis (mo)
(range)
49.7⫾ 35.4a(3–135)
Fecal wt (grams) 0.9⫾ 0.6a 1.1⫾ 0.9a 0.28 aMean⫾ standard deviation.
bChi-square test. cEnd-stage renal disease.
TABLE 4 Detection limits of target organisms
Target organism Detection limit (CFU/ml)
All bacteria 0.54 Bifidobacterium spp. 1.31 B. catenulatum 0.48 B. longum 1.44 B. breve 0.96 B. bifidum 0.05 Lactobacillus spp. 1.20 L. plantarum 1.96 L. paracasei 1.35 E. coli 1.30 K. pneumoniae 2.53 P. aeruginosa 1.92 Enterococcus spp. 0.37 B. fragilis 1.02
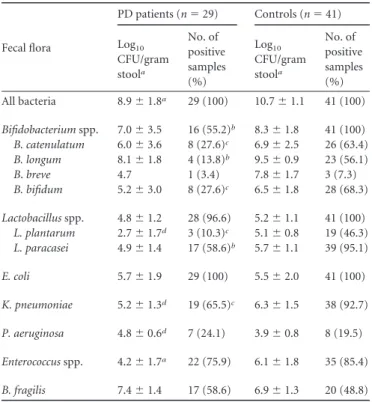
TABLE 5 Comparison of the fecal microbiotas of PD patients
and controls Fecal flora PD patients (n⫽ 29) Controls (n⫽ 41) Log10 CFU/gram stoola No. of positive samples (%) Log10 CFU/gram stoola No. of positive samples (%) All bacteria 8.9⫾ 1.8a 29 (100) 10.7⫾ 1.1 41 (100) Bifidobacterium spp. 7.0⫾ 3.5 16 (55.2)b 8.3⫾ 1.8 41 (100) B. catenulatum 6.0⫾ 3.6 8 (27.6)c 6.9⫾ 2.5 26 (63.4) B. longum 8.1⫾ 1.8 4 (13.8)b 9.5⫾ 0.9 23 (56.1) B. breve 4.7 1 (3.4) 7.8⫾ 1.7 3 (7.3) B. bifidum 5.2⫾ 3.0 8 (27.6)c 6.5⫾ 1.8 28 (68.3) Lactobacillus spp. 4.8⫾ 1.2 28 (96.6) 5.2⫾ 1.1 41 (100) L. plantarum 2.7⫾ 1.7d 3 (10.3)c 5.1⫾ 0.8 19 (46.3) L. paracasei 4.9⫾ 1.4 17 (58.6)b 5.7⫾ 1.1 39 (95.1) E. coli 5.7⫾ 1.9 29 (100) 5.5⫾ 2.0 41 (100) K. pneumoniae 5.2⫾ 1.3d 19 (65.5)c 6.3⫾ 1.5 38 (92.7) P. aeruginosa 4.8⫾ 0.6d 7 (24.1) 3.9⫾ 0.8 8 (19.5) Enterococcus spp. 4.2⫾ 1.7a 22 (75.9) 6.1⫾ 1.8 35 (85.4) B. fragilis 7.4⫾ 1.4 17 (58.6) 6.9⫾ 1.3 20 (48.8)
aP⬍ 0.001 versus controls (Mann-Whitney U test). bP⬍ 0.001 versus controls (chi-square test). cP⬍ 0.01 versus controls (chi-square test). dP⬍ 0.05 versus controls (Mann-Whitney U test). Wang et al.
1110 aem.asm.org Applied and Environmental Microbiology
on January 30, 2012 by guest
http://aem.asm.org/
be detected in the feces of infants in Taiwan (34). Dietary change
may make it undetectable in adults. Another concern relates to the
lack of standardization of diet in both groups. Selective
carbohy-drate ingestion may alter the gastrointestinal environment (e.g.,
by changing the pH). Moreover, because the duration of dialysis
ranged from 3 to 135 months, differences in gut microbiota may
either be due to renal disease or be an effect of PD.
In conclusion, Bifidobacterium species, B. catenulatum, B.
longum, B. bifidum, L. plantarum, and L. paracasei were detected at
lower rates in PD patients. Dysbiosis might result in impaired
intestinal barrier function and increased host vulnerability to
pathogen invasion. Further studies are necessary to confirm our
findings before clinical trials with probiotics supplementation in
PD patients.
ACKNOWLEDGMENTS
This study was supported by China Medical University Hospital (DMR98-019) and the Department of Health (grant number DOH100-TD-B-111-004).
REFERENCES
1. Ahrne S, et al. 1998. The normal Lactobacillus flora of healthy human rectal and oral mucosa. J. Appl. Microbiol. 85:88 –94.
2. Borruel N, et al. 2002. Increased mucosal tumour necrosis factor alpha production in Crohn’s disease can be downregulated ex vivo by probiotic bacteria. Gut 51:659 – 664.
3. Chen HL, Cheng HC, Wu WT, Liu YJ, Liu SY. 2008. Supplementation of konjac glucomannan into a low-fiber Chinese diet promoted bowel
movement and improved colonic ecology in constipated adults: a placebo-controlled, diet-controlled trial. J. Am. Coll. Nutr. 27:102–108. 4. Evenepoel P, Meijers BK, Bammens BR, Verbeke K. 2009. Uremic toxins
originating from colonic microbial metabolism. Kidney Int. Suppl. 2009: S12–S19.
5. Foligne B, et al. 2007. Correlation between in vitro and in vivo immuno-modulatory properties of lactic acid bacteria. World J. Gastroenterol. 13: 236 –243.
6. Frahm E, Obst U. 2003. Application of the fluorogenic probe technique (TaqMan PCR) to the detection of Enterococcus spp. and Escherichia coli in water samples. J. Microbiol. Methods 52:123–131.
7. Fuller R. 1989. Probiotics in man and animals. J. Appl. Bacteriol. 66:365– 378.
8. Galeev YM, et al. 2009. Scintigraphic visualization of bacterial transloca-tion in experimental strangulated intestinal obstructransloca-tion. Eur. J. Nucl. Med. Mol. Imaging. 36:1822–1828.
9. Gibson GR, Roberfroid MB. 1995. Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. J. Nutr. 125: 1401–1412.
10. Haarman M, Knol J. 2006. Quantitative real-time PCR analysis of fecal Lactobacillus species in infants receiving a prebiotic infant formula. Appl. Environ. Microbiol. 72:2359 –2365.
11. Haarman M, Knol J. 2005. Quantitative real-time PCR assays to identify and quantify fecal Bifidobacterium species in infants receiving a prebiotic infant formula. Appl. Environ. Microbiol. 71:2318 –2324.
12. Harmsen HJ, Raangs GC, He T, Degener JE, Welling GW. 2002. Extensive set of 16S rRNA-based probes for detection of bacteria in hu-man feces. Appl. Environ. Microbiol. 68:2982–2990.
13. Hida M, et al. 1996. Inhibition of the accumulation of uremic toxins in the blood and their precursors in the feces after oral administration of Lebenin, a lactic acid bacteria preparation, to uremic patients undergoing hemodialysis. Nephron 74:349 –355.
FIG 1 Distribution of bacterial counts in feces from the PD and control groups. Horizontal lines represent median values.
on January 30, 2012 by guest
http://aem.asm.org/
14. Huijsdens XW, et al. 2002. Quantification of bacteria adherent to gastro-intestinal mucosa by real-time PCR. J. Clin. Microbiol. 40:4423– 4427. 15. Kalantar-Zadeh K, Kopple JD, Deepak S, Block D, Block G. 2002. Food
intake characteristics of hemodialysis patients as obtained by food fre-quency questionnaire. J. Ren. Nutr. 12:17–31.
16. Kotanko P, Carter M, Levin NW. 2006. Intestinal bacterial microflora— a potential source of chronic inflammation in patients with chronic kid-ney disease. Nephrol. Dial. Transplant. 21:2057–2060.
17. Matsuki T, et al. 2004. Quantitative PCR with 16S rRNA-gene-targeted species-specific primers for analysis of human intestinal bifidobacteria. Appl. Environ. Microbiol. 70:167–173.
18. Matsuki T, Watanabe K, Tanaka R, Fukuda M, Oyaizu H. 1999. Distribution of bifidobacterial species in human intestinal microflora ex-amined with 16S rRNA-gene-targeted species-specific primers. Appl. En-viron. Microbiol. 65:4506 – 4512.
19. Matsumoto M, Benno Y. 2006. Anti-inflammatory metabolite produc-tion in the gut from the consumpproduc-tion of probiotic yogurt containing Bi-fidobacterium animalis subsp. lactis LKM512. Biosci. Biotechnol. Biochem. 70:1287–1292.
20. Mujais S. 2006. Microbiology and outcomes of peritonitis in North Amer-ica. Kidney Int. Suppl. 2006:S55–S62.
21. Nakabayashi I, et al. 2011. Effects of symbiotic treatment on serum level of p-cresol in haemodialysis patients: a preliminary study. Nephrol. Dial. Transplant. 26:1094 –1098.
22. Perez Fontan M, et al. 2005. Peritonitis-related mortality in patients undergoing chronic peritoneal dialysis. Perit. Dial. Int. 25:274 –284. 23. Quigley EM. 2011. The enteric microbiota in the pathogenesis and
man-agement of constipation. Best Pract. Res. Clin. Gastroenterol. 25:119 –126. 23a.Ranganathan N, et al. 2010. Pilot study of probiotic dietary supplemen-tation for promoting healthy kidney function in patients with chronic kidney disease. Adv. Ther. 27:634 – 647.
24. Sartor RB. 2004. Therapeutic manipulation of the enteric microflora in inflammatory bowel diseases: antibiotics, probiotics, and prebiotics. Gas-troenterology 126:1620 –1633.
25. Savage DC. 1977. Microbial ecology of the gastrointestinal tract. Annu. Rev. Microbiol. 31:107–133.
26. Schwartz T, et al. 2006. Real-time PCR detection of Pseudomonas aerugi-nosa in clinical and municipal wastewater and genotyping of the ciprofloxacin-resistant isolates. FEMS Microbiol. Ecol. 57:158 –167. 27. Schweinburg FB, Seligman AM, Fine J. 1950. Transmural migration of
intestinal bacteria; a study based on the use of radioactive Escherichia coli. N. Engl. J. Med. 242:747–751.
28. Shannon KE, Lee DY, Trevors JT, Beaudette LA. 2007. Application of real-time quantitative PCR for the detection of selected bacterial pathogens during municipal wastewater treatment. Sci. Total Environ.
382:121–129.
29. Simenhoff ML, et al. 1978. Bacterial populations of the small intestine in uremia. Nephron 22:63– 68.
30. Stephen AM, Wiggins HS, Cummings JH. 1987. Effect of changing transit time on colonic microbial metabolism in man. Gut 28:601– 609. 31. Takayama F, Taki K, Niwa T. 2003. Bifidobacterium in gastro-resistant
seamless capsule reduces serum levels of indoxyl sulfate in patients on hemodialysis. Am. J. Kidney Dis. 41:S142–S145.
32. Taki K, Takayama F, Niwa T. 2005. Beneficial effects of Bifidobacteria in a gastroresistant seamless capsule on hyperhomocysteinemia in hemodi-alysis patients. J. Ren. Nutr. 15:77– 80.
33. Tong J, Liu C, Summanen P, Xu H, Finegold SM. 2011. Application of quantitative real-time PCR for rapid identification of Bacteroides fragilis group and related organisms in human wound samples. Anaerobe 17:64 – 68. 34. Wang CY, Lin PR, Ng CC, Shyu YT. 2010. Probiotic properties of Lactobacillus strains isolated from the feces of breast-fed infants and Tai-wanese pickled cabbage. Anaerobe 16:578 –585.
35. Woodmansey EJ, McMurdo ME, Macfarlane GT, Macfarlane S. 2004. Comparison of compositions and metabolic activities of fecal microbiotas in young adults and in antibiotic-treated and non-antibiotic-treated el-derly subjects. Appl. Environ. Microbiol. 70:6113– 6122.
36. Yasuda G, et al. 2002. Prevalence of constipation in continuous ambula-tory peritoneal dialysis patients and comparison with hemodialysis pa-tients. Am. J. Kidney Dis. 39:1292–1299.
Wang et al.
1112 aem.asm.org Applied and Environmental Microbiology