UPDATE
Staging of gastric cancer with 16-channel MDCT
C.-Y. Chen,
1D.-C. Wu,
2W.-Y. Kang,
3J.-S. Hsu
11Department of Medical Imaging, Kaohsiung Medical University, No. 100 Tz You 1st Road, Kaohsiung, 807 Taiwan 2
Department of Medical Gastroenterology, Kaohsiung Medical University, No. 100 Tz You 1st Road, Kaohsiung, 807 Taiwan
3
Department of Pathology, Kaohsiung Medical University, No. 100 Tz You 1st Road, Kaohsiung, 807 Taiwan
Abstract
Early detection and accurate preoperative staging of gastric cancer are clinically important because the prog-nosis and choice of an optimal therapeutic approach are directly related to the stage of a neoplasm at time of presentation. Multidetector row computed tomography is a potentially powerful tool for noninvasive gastric evaluation. When thin collimation is used, near-isotropic imaging of the stomach is possible. Proper air distention of the stomach is used with virtual gastroscopic images; the technique is able to evaluate endoluminal lesions of the stomach and assist in early detection of gastric can-cer. Adequate water-filled dynamic multiplanar refor-matted images allow the radiologist to choose the optimal imaging plane to accurately evaluate depth of tumor invasion of the gastric wall and perigastric fat plane infiltration, identify a thin fat plane between a tumor and adjacent organs, avoid partial volume aver-aging effects, and better differentiate lymph nodes from small perigaskric vessels. Thus, the combination of air distention and hydrodistention of the stomach and dy-namic contrast-enhanced multidetector row computed tomography with near-isotropic imaging offer improved diagnosis and staging of gastric cancers.
Key words: Staging of gastric cancer—Multidetector computed tomography—Virtual gastroscopy—Multi-planar reformation
The overall incidence and mortality from gastric carci-noma have been steadily decreasing over the past few decades, but it remains one of the leading causes of cancer death worldwide, with a relative increase in the incidence of proximal and cardiac lesions [1, 2]. In Japan, gastric cancer is a leading cause of cancer death [3]. In
patients who have suspected gastric cancer, early detec-tion and accurate preoperative staging are crucially connected to the prognosis and may influence the choice of an optimal therapeutic approach. An early small gastric cancer that is confined to the submucosa (T1 stage) can be treated with nonsurgical endoscopic mucosal resection [4, 5], whereas preoperative chemo-therapy and radiation chemo-therapy can be recommended for advanced gastric cancer for downstaging. Terminally ill patients may exhibit incurable disease on preoperative imaging studies and can thus avoid unnecessary surgery. To select the optimal treatment modality, accurate pre-operative staging is necessary, namely staging that will benefit patients with gastric cancer in terms of cure and quality of life. Unfortunately, in the West, most patients are diagnosed as having advanced disease, with possible curative resection in only approximately 50% and a poor overall 5-year survival rate of 7% to 15% [6].
Endoscopy and double contrast barium examination of the upper gastrointestinal tract remain the basic investigational tools for diagnosing gastric cancer. However, these techniques are exclusively based on depiction of the gastric mucosa and are limited by their inherent inability to evaluate transmural and extraserosal extensions of disease. This means that they are unsuitable for T staging according to the TNM system.
Endoscopic ultrasonography and computed tomog-raphy (CT) are often used for preoperative imaging in staging gastric carcinoma. Endoscopic ultrasonography was superior to CT in T staging and perigastric lymph node evaluation in previous studies [7]; however, it can-not be used for nodal staging beyond the first dimension of nodes, peritoneal dissemination, and liver metastasis due to diminution of the field of view. Recently, fast scanning with rapid infusion of intravenous administra-tion of contrast medium (dynamic CT) and filling the stomach with a large amount of low-density fluid [8, 9] have been used to overcome the limitations of conven-tional CT in the evaluation of transmural and extrase-rosal spreads of disease, with accuracy rates of 65% to
Correspondence to:C.-Y. Chen; email: ccy@ rad.kmu.edu.tw
stagings [19]. Another study reported low detectability of early gastric cancers (EGCs) when using MRI due to problems with spatial resolution [20]. Moreover, MRI is more expensive than CT and not as widely available.
Multidetector row CT (MDCT) is a potentially powerful tool for noninvasive gastric evaluation. When thin collimation is used, near-isotropic imaging of the stomach is possible, thus allowing high-quality multi-planar reformation (MPR) and three-dimensional Nav-igator virtual gastroscopic (VG) scanning of gastric images. When proper air distention of the stomach is used with VG images, the technique can be used to evaluate endoluminal lesions of the stomach. Adequate distention of the stomach using water as a negative contrast agent is a prerequisite for assessing the gastric wall. Because of a substantial decrease in scanning time, optimization of intravenous contrast material injection is necessary with multidetector scanning. Proper injection techniques of contrast material improve differentiation of tumor tissue from normal mucosa [21]. Although such techniques have been used with single-section spiral CT to improve staging of gastric malignancies, single-section scanning is substantially limited by a relatively large section thickness [22, 23]. MPR is an evolving method for assessment of intra- and extraluminal processes of the gastric wall and for evaluation of more distant regions such as paraaortic lymph nodes and abdominal organs.
Thus, the combination of air distention and hydrodi-stention of the stomach and dynamic contrast-enhanced MDCT with near-isotropic imaging improve diagnosis of many gastric diseases. This report describes the role of MDCT in the diagnosis and preoperative staging of gastric cancer.
CT protocol and techniques
All patients fasted for at least 8 h before examination. The CT techniques in our department are preceded by two steps: (a) air distention of the stomach with nonen-hanced CT is used for virtual gastroscopy to evaluate gastric mucosal lesions and (b) water distention of the stomach and dynamic contrast-enhanced CT with MPR are used for TNM staging.
CT protocol
CT was performed with a 16-channel MDCT scanner (Light Speed 16, GE Medical Systems, Milwaukee, WI,
USA). The scan parameters were 16- ·; 1.25-mm colli-mation, 27.5-mm/s table speed, 250 to 300 mAs, and 120 kV. We reconstructed raw datasets at 1.25-mm slice thickness and 0.9-mm reconstruction intervals for VG and MPR images.
Air distention of the stomach with
nonenhanced CT
Each patient received orally 6 g of gas-producing crystals shortly before nonenhanced CT examination for VG images. In case of insufficient air filling of the stomach, an additional 3 g of gas-producing crystals was given. Un-enhanced CT scans of the upper abdomen from the dia-phragmatic domes to 2 cm below the lower margin of the air-distended gastric body were performed. VG images were obtained with Navigator software (AW 4.1, GE).
Water-filled stomach with dynamic
contrast-enhanced CT
Before performing contrast-enhanced dynamic study by MDCT, each patient drank 800 to 1000 mL of tap water for gastric filling. A 100-mL bolus of nonionic iodine contrast agent (Ultravist, Schering, Berlin, Germany) was administered with an automatic injector into the antecu-bital vein at a flow rate of 3 mL/s through a 20-gauge needle. CT acquisitions were performed in the arterial phase (start delay 40 s), portal venous phase (start delay 70 s), and delayed phase (start delay 150 s). At the time of MDCT scanning, we restricted arterial and parenchymal phase acquisitions to the stomach. Portal venous phase CT examination included the entire abdomen and pelvis, from the diaphragmatic domes to the anal verge. All CT data were transferred to a workstation (Advantage 4.1, GE Medical Systems) for MPR images. Depth of tumor invasion was detected by a plane vertical to the tumor to avoid partial volume effects. All lymph nodes were eval-uated by axial, coronal, and sagittal images at the same time.
N3 Metastasis in >15 regional lymph nodes M0 No distant metastasis
Pathologic TNM staging and image
analysis
Staging system
For the purpose of staging of gastric cancer, we suggest using the pathologic TNM staging system developed by the American Joint Committee on Cancer and the International Union against Cancer [22] (Table 1). It redefines nodal status on the basis of the number of in-volved nodes rather than on their location. Ichikura et al. [23] showed that the number of positive lymph nodes significantly affects survival.
VG images provide an excellent overview of a tumor mass within the lumen of the stomach, and it is possible to accurately display gastric lesions as shown by gas-troscopy [24, 25] (Figs. 1 to 4). Three-dimensional endoluminal morphology can be classified into three subgroups within EGC [26] and four subcategories (Borrmann classification) within advanced gastric cancer [27]. The three groups of EGC are protruded (type I), superficial (type II), and excavated (type III). Type II is further divided into three subclasses: IIA (elevated), IIB (flat), and IIC (depressed). The Borrmann classification includes type I (polypoid carcinoma), type II (fungating
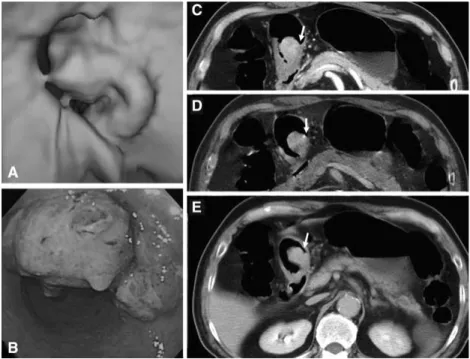
Fig. 1. EGC type IIc in a 51-year-old woman that was diagnosed by VG. A VG image shows a superficial depressed lesion (arrow) at the gastric angle. B Corresponding endoscopic finding (arrow). C Coronal MPR image displays no abnormality at the gastric angle (arrow). D Histologic image demonstrates cancer cells in the minimally depressed gastric mucosa (arrow). E Corresponding gross specimen (arrow).
Fig. 2. EGC type IIa in a 55-year-old woman. A VG image demonstrates a superficially elevated ulcerated lesion at the low body of the stomach. B Gastroendoscopic image shows a similar superficial elevated ulcerated lesion. C Postcontrast arterial phase axial image shows subtle focal wall thickening with well-enhanced mucosa (arrow). D
Postcontrast arterial phase oblique coronal image displays a well-enhanced mucosal tumor (arrow) with a visible outer layer of gastric wall and a clear fat plane around the tumor, indicating EGC. Surgically, it proved to be pathologic stage T1. This case is more clearly demonstrated in the reformatted image.
carcinoma), type III (ulcerated carcinoma), and type IV (diffusely infiltrative carcinoma)
MDCT diagnostic criteria for gastric cancer
The CT criteria of the mural invasion of cancer in gastric wall follow [3, 12–15, 28].
T0 tumors: no evidence of alteration of the gastric wall with a normal fat plane.
T1 tumors: focal thickening of the inner layer with a visible outer layer of the gastric wall and a clear fat plane around the tumor (Fig. 2).
T2 tumors: focal or diffuse thickening of the gastric wall with transmural involvement and a smooth outer border of the wall or only a few small linear strands of soft tissue extending into the fat plane involving less than one-third of the tumor extent (Fig. 3).
T3 tumors: transmural tumors with an irregular or micronodular outer border and/or wide reticular strands in the fat planes contiguous to the outer bor-der of the tumor (Fig. 4).
T4 tumors: obliteration of the fat plane between the gastric tumor and an adjacent organ or invasion of an adjacent organ (Fig. 5).
Fig. 3. Advanced T2 gastric cancer
(Borrmann type II) in a 64-year-old man. A VG image depicts a polypoid carcinoma in the antrum of the stomach. B Gastroendoscopic image shows a similar lesion. Dynamic axial images show a gradually transmural enhanced tumor (C, arterial phase; D, portal venous; E, delayed phase) with a smooth outer border of the gastric wall (arrows), suggesting
pathologic stage T2. Surgically, it proved to be pathologic stage T2.
Fig. 4. Advanced T3 gastric cancer
(Borrmann type III) in a 65-year-old man. A VG image shows an ulcerated tumor. B
Gastroscopic image displays a similar picture. C Delayed phase axial image show a focal transmural enhanced tumor (arrow) with a smooth outer border of the gastric walls, suggesting pathologic stage T2. D Delayed phase parasagittal MPR image shows a focal transmural hyperintense tumor (small arrow) with an irregular outer border of the stomach and reticular strands in the fat plane
contiguous to the outer border of the tumor (large arrow) in the posterior superior wall of the gastric antrum, suggesting pathologic stage T3. Surgically, it proved to be pathologic stage T3. This case is more clearly
Imaging-pathologic correlation of lymph nodes
(group-by-group analysis)
Regional lymph nodes were considered to be involved by metastases in two conditions: (a) if they were solitary nodes or separate nodes larger than 8 mm in long-axis diameter; (b) if they were cluster nodes with or without associated reticular strands or solitary nodes with associated reticular strands, independent of their size (Fig. 6).
The CT images were evaluated for solid organs (liver, spleen, pancreas, kidneys, adrenal gland) metastases, ascites, parietal peritoneal thickening, and/or nodules on the parietal peritoneal surface, which were assessed on portal venous phase with MPR images (Figs. 5, 7).
Advantages and clinical value of MDCT in
gastric cancer staging
MDCT dramatically increased speed of scan acquisition and substantially improved spatial resolution and quality of MPR images through the routine use of thinner col-limation (16 · 1.25 mm). The use of MPR images al-lowed the radiologist to choose the optimal imaging plane to accurately evaluate the depth of tumor invasion of the gastric wall (Figs. 1, 3) and perigastric fat plane infiltration, identify a thin fat plane between a tumor and adjacent organs, and avoid partial volume averaging ef-fects. By using MPR images, good preoperative predic-tions of stage T1 to T4 lesions are possible.
Owing to decreases in scanning time for MDCT, optimization of intravenous contrast material injection is necessary and offers improved differentiation of tumor tissue from normal mucosa. Gastric cancer frequently shows hypervascularity (neovascularity) and accumula-tion of contrast medium (tumor stain) [29]. For incre-mental dynamic MDCT, the arterial phase was used for lesion detection, the portal venous phase was used to differentiate the stomach from adjacent organs and lymph node evaluations, and the delayed phase were used to help evaluate the depth of gastric wall invasion [30] (Figs. 2 to 5).
VG of an air-distended stomach can be used for abnormal endoluminal lesion detection. It helps for
Fig. 5. Postcontrast portal venous phase axial image shows a tumor mass in the pancreatic head (arrow) and obliteration of the fat planes between the gastric tumor and pancreatic head, indicating that the tumor directly invades the pancreatic head. Surgically, it proved to be pathologic stage T4.
Fig. 6. Oblique coronal image shows a cluster of small nodes (arrow) around the perigastric region, suggesting metastatic lymph nodes. Pathologic findings displayed met-astatic nodes.
Fig. 7. Coronal oblique MPR image demonstrates perito-neal carcinomatosis along the gastrocolic ligament (arrows).
main prognostic determinant in gastric cancer [32]. More accurate detection and measurement of lymph node diameter and better differentiation between lymph nodes and small perigastric vessels are possible with the use of MPR images. MPR images combined with modifica-tion of the N staging system may improve overall N staging [25].
In previous studies, CT images provided highly reli-able information regarding liver metastases but yielded less reliable information regarding perigastric invasion and peritoneal metastases [33]. MDCT can improve overall accuracy of perigastric invasion and peritoneal metastases because of good spatial resolution, an optimal imaging plane, and decreased partial volume averaging effects and can correctly detect smaller metastatic lesions than previous-generation CT imaging.
Early detection of liver, peritoneal cavity, and retro-peritoneal metastases, especially before surgery, is ex-tremely important for patient survival because it enables planning of a combined treatment of primary and sec-ondary diseases. Multidetector CT offers the opportunity to refine this concept by more accurately defining the group of patients for whom primary surgical therapy will be curable or unsuitable. If CT shows definitive trans-mural extension with peritoneal tumor spread, presurgi-cal chemotherapy is used to downstage the tumor. After completion of chemotherapy, restaging of the tumor is performed. If there is a positive response to chemother-apy, curative surgical therapy is attempted. Therefore, preoperative staging of gastric cancer appears to be by far the main clinical indication.
Limitations of MDCT in gastric cancer
staging
Despite substantial advances introduced by MDCT technology, there are several limitations.
MDCT cannot detect flat type EGC (IIb) even in combination with VG and MPR images [17, 18], whereas gastroscopy may demonstrate these lesions with direct visualization of small lesions and visibility of the mucosal color changes of flat lesions.
Another inherent limitation in some cases is over-staging T2 cancers with perigastric inflammation or vascular or lymphatic engorgement and understaging T3 cancers with microscopic infiltration of cancer cell pen-etration to the serosal layer [34].
patients with severe cachexia due to the limitation in the evaluation of perigastric fat plane infiltration.
The fourth limitation is the lack of reliable CT criteria for metastatic lymph nodes. MDCT is still relatively insensitive for the detection of nodal metastases due to its inability to detect microscopic nodal invasion and the presence of reactive nodes that may be larger than 10 mm [13, 35].
Conclusion
MDCT provides new opportunities for detailed evalua-tion of gastric morphology that can not only detect pri-mary tumors but also provide comprehensive staging, with accurate assessment of the neoplastic mass, regional and distant lymphadenopathies, and metastases. On the basis of these considerations, MDCT is an accurate modality for preoperative staging of gastric cancer, and the technique may have a positive effect on therapeutic decision making, particularly in the selection of patients for extended nodal resection and for the application of multimodal treatment strategies. Therefore, MDCT can be used as an all-in-one diagnostic test for the preoper-ative evaluation of patients with known, or strongly suspected, gastric carcinoma.
References
1. Rudiger Siewert J, Feith M, Werner M(2000) Adenocarcinoma of the esophagogastric junction: results of surgical therapy based on anatomical/topographic classification in 1,002 consecutive patients. Ann Surg 232:353–361
2. Kodera Y, Schwarz RE, Nakao A (2002) Extended lymph node dissection in gastric carcinoma: where do we stand after the Dutch and British randomized trials? J Am Coll Surg 195:855–864 3. Forman D, Goodman KJ (2000) The epidemiology of stomach
cancer: correlating the past with the present. Socioeconomic influences in early life can influence mortality in adult life. BMJ 320:1682–1683
4. Ohashi S, Segawa K, Okamura S, et al. (1999) The utility of endoscopic ultrasonography and endoscopy in the endoscopic mucosal resection of early gastric cancer. Gut 45:599–604 5. Meyers WC, Damiano RJ Jr, Rotolo FS, et al. (1987)
Adenocar-cinoma of the stomach. Changing patterns over the last 4 decades. Ann Surg 205:1–8
6. Hundahl SA, Phillips JL, Menck HR (2000) The National Cancer Data Base Report on poor survival of U.S. gastric carcinoma pa-tients treated with gastrectomy: fifth edition American joint com-mittee on cancer staging, proximal disease, and the ‘‘different disease’’ hypothesis. Cancer 88:921–932
7. Kelly S, Harris KM, Berry E, et al. (2001) A systematic review of the staging performance of endoscopic ultrasound in gastro-oesophageal carcinoma. Gut 49:534–539
8. Hori S, Tsuda K, Murayama S, et al. (1992) CT of gastric carci-noma: preliminary results with a new scanning technique. Radio-graphics 12:257–268
9. Tsuda K, Hori S, Murakami T, et al. (1995) Intramural invasion of gastric cancer: evaluation by CT with water-filling method. J Comput Assist Tomogr 19:941–947
10. Baert AL, Roex L, Marchal G, et al. (1989) Computed tomography of the stomach with water as an oral contrast agent: technique and preliminary results. J Comput Assist Tomogr 13:633–636 11. Kadowaki K, Hori S, Sakai Y, et al. (1989) [Computed
tomogra-phy of gastric cancer]. Rinsho Hoshasen 34:1549–1554
12. Minami M, Kawauchi N, Itai Y, et al. (1992) Gastric tumors: radiologic-pathologic correlation and accuracy of T staging with dynamic CT. Radiology 185:173–178
13. Cho JS, Kim JK, Rho SM, et al. (1994) Preoperative assessment of gastric carcinoma: value of two-phase dynamic CT with mechanical iv. Injection of contrast material. AJR 163:69–75
14. Rossi M, Broglia L, Maccioni F, et al. (1997) Hydro-CT in patients with gastric cancer: preoperative radiologic staging. Eur Radiol 7:659–664
15. DÕElia F, Zingarelli A, Palli D, et al. (2000) Hydro-dynamic CT preoperative staging of gastric cancer: correlation with pathological findings. A prospective study of 107 cases. Eur Radiol 10:1877– 1885
16. Botet JF, Lightdale CJ, Zauber AG, et al. (1991) Preoperative staging of gastric cancer: comparison of endoscopic US and dy-namic CT. Radiology 181:426–432
17. Hundt W, Braunschweig R, Reiser M (1999) Assessment of gastric cancer: value of breathhold technique and two-phase spiral CT. Eur Radiol 9:68–72
18. Takao M, Fukuda T, Iwanaga S, et al. (1998) Gastric cancer: evaluation of triphasic spiral CT and radiologic-pathologic corre-lation. J Comput Assist Tomogr 22:288–294
19. Sohn KM, Lee JM, Lee SY, et al. (2000) Comparing MR imaging and CT in the staging of gastric carcinoma. AJR 174:1551–1557 20. Wang CK, Kuo YT, Liu GC, et al. (2000) Dynamic
contrast-en-hanced subtraction and delayed MRI of gastric tumors: radiologic-pathologic correlation. J Comput Assist Tomogr 24:872–877 21. Fleischmann D, Rubin GD, Bankier AA, et al. (2000) Improved
uniformity of aortic enhancement with customized contrast med-ium injection protocols at CT angiography. Radiology 214:363–371
22. Greene FL, Page DL, Fleming ID, eds. (2002). AJCC manual of staging of cancer. 6th ed. New York: Springer-Verlag
23. Ichikura T, Tomimatsu S, Uefuji K, et al. (1999) Evaluation of the New American Joint Committee on Cancer/International Union against cancer classification of lymph node metastasis from gastric carcinoma in comparison with the Japanese classification. Cancer 86:553–558
24. Lee DH (1998) Three-dimensional imaging of the stomach by spiral CT. J Comput Assist Tomogr 22:52–58
25. Chen CY, Jaw TS, Liu GC, et al. (2004) Preoperative staging of gastric cancer with hydro- and air-distended 3D multi-detector row CT: correlation with surgical and histopathological results. Paper presented at the annual meeting of the RSNA; Chicago, Illinois 26. Merino S, Saiz A, Moreno MJ, et al. (1999) CT evaluation of
gastric wall pathology. Br J Radiol 72:1124–1131
27. Borrmann R (1926) Geshwulste des magens und duodenums. In: Henke F, Lubarsch O, eds. Handbuch der Speziellen Pathologischen Anatomieund Histologis. Berlin: Springer-Verlag, pp 865
28. Rossi M, Broglia L, Arata FM, et al. (1997) [The diagnostic accuracy and reproducibility of computed tomography with water distention and induced hypotonia in the preoperative staging of gastric tumors]. Radiol Med (Torino) 94:486–491
29. Efsen F, Fischerman K (1974) Angiography in gastric tumours. Acta Radiol Diagn (Stockh) 15:193–197
30. Lee JH, Jeong YK, Kim DH, et al. (2000) Two-phase helical CT for detection of early gastric carcinoma: importance of the mucosal phase for analysis of the abnormal mucosal layer. J Comput Assist Tomogr 24:777–782
31. Lee DH (2000) Two-dimensional and three-dimensional imaging of gastric tumors using spiral CT. Abdom Imaging 25:1–6
32. Yamamura Y, Nakajima T, Ohta K, et al. (2002) Determining prognostic factors for gastric cancer using the regression tree method. Gastric Cancer 5:201–207
33. Adachi Y, Sakino I, Matsumata T, et al. (1997) Preoperative assessment of advanced gastric carcinoma using computed tomography. Am J Gastroenterol 92:872–875
34. Kim AY, Kim HJ, Ha HK (2005) Gastric cancer by multidetector row CT: preoperative staging. Abdom Imaging 30(5):509–517 35. Sussman SK, Halvorsen RA Jr, Illescas FF, et al. (1988) Gastric
adenocarcinoma: CT versus surgical staging. Radiology 167: 335–340