Obesity is a pan-endemic health problem in both developed and developing countries and is asso-ciated with considerable increase in morbidity and mortality.1–3For the severely obese patient, nonsur-gical methods (including diet, exercise, and behav-ioral modification) are usually ineffective and rarely result in sustained weight loss.4,5 Surgery is the only treatment that has been proven to
consistently achieve long-term reduction of excess weight in patients with severe clinical obesity.4–6 g Laparoscopic adjustable gastric banding (LAGB) is a minimally invasive surgical procedure for the treatment of morbid obesity. Kuzmak devel-oped the adjustable silicone gastric band, which was implanted via laparotomy.7In 1993, a modi-fied laparoscopic device, the Lap-Band (Bioenterics
Weight Loss and Improvement of
Obesity-related Illness Following Laparoscopic
Adjustable Gastric Banding Procedure for
Morbidly Obese Patients in Taiwan
Wei-Jei Lee,1,2Weu Wang,1,2Po-Li Wei,1,2Ming-Te Huanggg *2,3
Background/Purpose:Laparoscopic adjustable gastric banding (LAGB) is a newly developed minimallyy invasive surgical procedure for the treatment of morbid obesity. This study was conducted to evaluate body weight loss, surgical complications, and comorbidities after LAGB surgery.
Methods: Ninety-one morbidly obese patients (mean age, 31.2 years; mean preoperative weight, 120.8 kg)
c underwent LAGB in a private Taiwan hospital setting within a comprehensive multidisciplinary bariatric program. Patients were followed up to 36 months. Comorbidities were assessed in 55 patients who com-g pleted more than 12 months of follow-up by comparing each comorbid condition before surgery and during follow-up.
Results: All procedures were performed laparoscopically with no conversion. Mean operation time was
88.7± 32.9 minutes. There were no intraoperative or major postoperative complications. Minor complication of stoma stenosis occurred in three (3.3%) patients. At 36 months after surgery, mean body mass index had decreased from 42.7 to 33.9 kg/m2, and mean percentage of excess weight loss was 44.8%. Late complications
w
were as follows: intractable vomiting requiring band removal in one (1.1%) patient, tubing problems requir-ing revision surgery in four (4.3%), and stoma obstruction in two (2.1%). There was no mortality. Resolution or improvement of comorbidities was significant for hyperglycemia and diabetes-related index, dyslipidemia, abnormal liver function, hyperuricemia, sleep apnea, and arthralgia, but not for hypertension.
Conclusion:LAGB provides good weight loss and significant reduction in comorbidities with few minorr complications. [J Formos Med Assoc 2006;105(11):887–894]
Key Words: gastric banding, morbidly obesity, obese-related illness
©2006 Elsevier & Formosan Medical Association . . . .
1Department of Surgery, Taoyuan Min-Sheng General Hospital, Taoyuan, 2Department of Surgery, National Taiwan University Hospital and
College of Medicine, National Taiwan University, and3Department of Surgery, Taipei Medical University Hospital, Taipei, Taiwan.
Received: October 21, 2005 Revised: November 30, 2005 Accepted: April 4, 2006
*Correspondence to: Dr Ming-Te Huang, Department of Surgery, Taipei Medical University Hospital,
252 Wu-Hsing Street, Taipei, Taiwan. E-mail: [email protected]
Corp., Carpinteria, CA, USA) was first implanted (Figure 1).8Initial trials in Europe and worldwide use were expanded later.9–13In June 2001, the US Food and Drug Administration approved the Lap-Band System in the United States. Currently, LAGB is the most commonly performed bariatric surgery w
worldwide.6
This report describes our series of 91 con-secutive Taiwanese patients, making this the first clinical trial in Taiwan.
Materials and Methods
AA comprehensive, multidiscipliniary, bariatric man-agement program was in place for the preoperative preparation and postoperative management of pa-tients. The program included support groups and
ancillary personnel to provide nutritional, exercise and psychologic care. Nurse specialists for medical and psychiatric management were part of the team. Inclusion/exclusion criteria followed the standard National Institutes of Health guidelines: > 18 years old, body mass index (BMI)> 35 kg/m2with im-portant comorbidities, no alcohol abuse and con-f current psychiatric illness. The ethics committee of En-Chu-Kong Hospital and the National Depart-ment of Health of Taiwan approved this trial.
y Patients were placed supine in the lithotomy position, then to the reverse Trendelenburg po-A sition, and an orogastric tube was inserted. A five-trocar technique was used (Figure 2). Pneu-moperitoneum was achieved with a Veress-type needle introduced at the supraumbilical area and maintained at 15 mmHg. All bands were placed using the pars flaccid technique.5 Briefly, the
A B
i
Figure 1. (A) The Lap-Band system with inflatable inner cuff (arrow) that connects by silicon tubing to the implanted (A) The Lap-Band system with inflatable inner cuff (arrow) that connects by silicon tubing to the implanted subcutaneous injection port (arrowhead). (B) Drawing shows placement of the band around the upper portion of the stomach, creating a small upper pouch with stoma to the remainder of the stomach.
A B
i
Figure 2.(A) Trocar placement. Trocar 1: a 15-mm port about 4 cm above the umbilicus, from the midline to across thef left rectus muscle, viewing telescope and injection port site. Trocars 2 and 4 are placed in the bilateral subcostal areas with 5 mm for bilateral working ports. Trocar 3: a 5-mm port placed subxyphoidal, liver retractor. Trocar 5: a 10-mm port at the left anterior axillary line, gastric grasper. (B) Intraoperative picture.
dissection began at the Angle of His. A very small opening was created in the avascular phrenogas-tric ligament, close to the gasphrenogas-tric wall at the Angle of His. The dissection was then moved to the lesser curvature side. The pars flaccid (gastrohepatic ligaments) was incised and the right crus of the diaphragm was identified. Blunt dissection was performed to create a passage between the dia-phragmatic pillars and the posterior aspect of the gastroesophageal junction. The band was then placed around the cardia of the stomach and su-tured in place with gastric to gastric sutures. The band tubing was brought outside the abdomen and connected to the access port. The port was fixed to the left rectus fascia.
The surgeon, with the support of the nurse coordinator and nutritionist, provided postoper-ative follow-up. After discharge, patients were in-structed to follow a clear to full liquid diet for the first 48 hours, followed by a soft diet for the first w
week. Small amounts of solid food were intro-duced starting in the second week, as tolerated. Patients returned to the office a week after surgery for wound check. They were then scheduled to re-turn between 1 and 2 months later. For adjust-ment of the LAGB, saline was not added to the band reservoir until at least 4 weeks had elapsed after surgery. We routinely performed adjustments in the clinic. Computed tomography (CT)-guided adjustment was only indicated occasionally. The first adjustment usually involved the addition of 1 mL of sterile saline. The second adjustment involved the addition of 0.5 mL when patients failed to lose weight but had sustained satiety between meals.
Prior to surgery, all patients underwent a thorough laboratory work-up including meta-bolic profile and complete blood count with in-dices. For the purpose of comorbidity assessment, patients (n=56) who had completed at least t 12 months of follow-up were included.
Obesity-g related illness status was assessed by comparing each comorbidity before surgery and 1 year later. Criteria used to define metabolic comorbidities are listed in Table 1.
Descriptive data are expressed as mean± standard deviation. Group characteristics were compared by the paired t test and differences between proportions were tested by the χ2 test. Statistical analysis was performed using SPSS
r version 8.0 (SPSS Inc., Chicago, IL, USA) for y Windows. Statistical significance was inferred by a two-tailed p value of less than 0.05.
Results
Between May 2002 and May 2005, LAGB was performed on 91 consecutive patients. There were
f 47 men and 44 women, with a mean age of
f 31.2 years (range, 18–56 years) and mean BMI of 42.7 kg/m2 (range, 35.0–62.7 kg/m2). Of the 91 patients, 80 suffered from obesity-related co-morbidities such as hypertension, diabetes, hy-perlipidemia, arthritis, asthma, sleep apnea and venous stasis (Table 2). The mean operating time was 88.7± 32.9 minutes. The mean operating time for the first 10 cases was 107 minutes, and it was r 83 minutes for the last 10 cases. There was neither conversion nor major complication in this series.
Table 1. Definition criteria of obesity-related comorbidities
Comorbidity Definition
Hypertension Blood pressure> 140/90 mmHg or previous diagnosis of hypertension on pharmacologic treatment
Hyperglycemia Fasting glycemia> 109 mg/dL or previous diagnosis of diabetes on pharmacologic treatment
Hyperlipidemia Fasting triglycerides> 200 mg/dL and/or cholesterol > 200 mg/dL Hyperuricemia Fasting uric acid> 8.0 mg/dL in men and > 6.5 mg/dL in women
Minor complications occurred in three (3.3%) pa-tients, all were transient stoma obstruction and subsided after conservative treatment (Figure 3). Hospital stay averaged 3.2 days (range, 2–10 days).
P
Patient follow-up
Of the 91 patients, the follow-up rate was 100%. Late complications occurred in seven (7.7%)
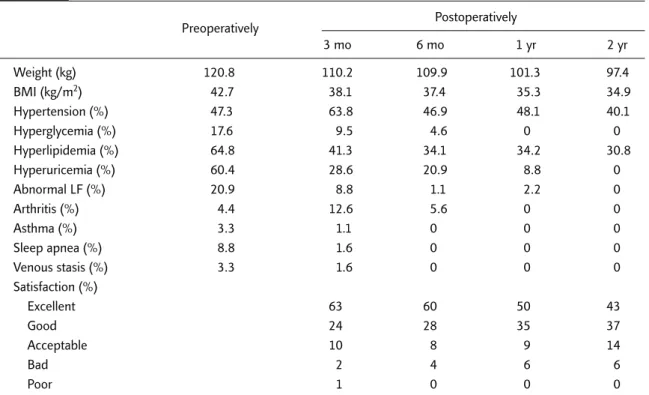
t patients. One (1.1%) had her band removed at 3 months postoperatively due to intractable vomit-r ing. Four (4.4%) received port revision surgery for tubing problems. Another patient had acute food obstruction and required admission for treatment. No band was removed in these patients. The ma-jority of patients received two to five band adjust-ments during the first year after surgery.Almostt Table 2. Preoperative and follow-up clinical data of patients who underwent laparoscopic adjustable
gastric banding Preoperatively Postoperatively 3 mo 6 mo 1 yr 2 yr Weight (kg) 120.8 110.2 109.9 101.3 97.4 BMI (kg/m2) 42.7 38.1 37.4 35.3 34.9 Hypertension (%) 47.3 63.8 46.9 48.1 40.1 Hyperglycemia (%) 17.6 9.5 4.6 0 0 Hyperlipidemia (%) 64.8 41.3 34.1 34.2 30.8 Hyperuricemia (%) 60.4 28.6 20.9 8.8 0 Abnormal LF (%) 20.9 8.8 1.1 2.2 0 Arthritis (%) 4.4 12.6 5.6 0 0 Asthma (%) 3.3 1.1 0 0 0 Sleep apnea (%) 8.8 1.6 0 0 0 Venous stasis (%) 3.3 1.6 0 0 0 Satisfaction (%) Excellent 63 60 50 43 Good 24 28 35 37 Acceptable 10 8 9 14 Bad 2 4 6 6 Poor 1 0 0 0
BMI= body mass index; LF = liver function test.
A B
i
Figure 3. ( )(A) Upper gastrointestinal radiograph after placement of the laparoscopic adjustable gastric band (LAGB) withl d h f l f h l d bl b d ( ) h normal stoma. (B) Upper gastrointestinal radiograph of stoma stenosis after LAGB placement.
all patients required their first band adjustment w
within the first 3 months after surgery. Seven pa-tients required CT-guided adjustment due to malposition of the port or massive subcutaneous fat (Figure 4).
Weight loss and comorbidity assessment A
After a median follow-up of 30 months, the group had a significant reduction in BMI (Figure 5). Mean preoperative BMI was 42.7 kg/m2and had decreased to 33.9 kg/m23 years after LAGB. Mean body weight decreased from 120.8 kg to 94.7 kg. Mean BMI and (reduction of excess BMI as com-pared to BMI= 25 kg/m2) were 38.8 (22.1%), 37.4
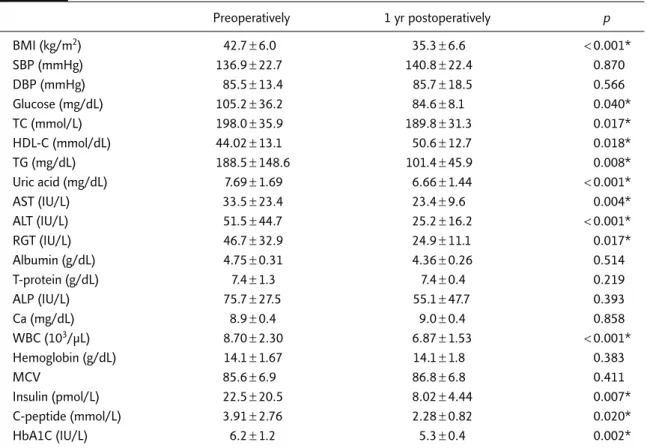
(29.7%), 35.1 (41.7%), 34.9 (44.0%) and 33.9 (44.8%) at 3, 6, 12, 24 and 36 months, respec-tively. At 2 years after LAGB, all obesity-related y comorbidities had been eliminated significantly except for hypertension (Table 2). Table 3 shows the changes in various clinical variables before and 1 year after LAGB. Recovery from diabetes, hypertriglyceridemia, abnormal liver function and hyperglycemia were more favorable, whereas recovery from hypertension did not differ. The white blood cell count also decreased signifi-cantly after surgery. There was no detectable dif-ference in calcium metabolism, hemoglobin, and albumin levels pre- and postoperatively.
A B
R
i
Figure 4. bdAbdominal computed tomography (CT) shows: (A) subcutaneous injection port floating in the massive sub-l d h ( ) h ( ) b fl h b cutaneous fat (arrow); and (B) tilting injection port (arrow). Both cases required CT-guided injection for adjustment.
42.7 38.8 37.4 34.1 34.9 35.3 30 32 34 36 38 40 42 44 Before 3 Months 6 9 1 2 3
Body mass inde
x (kg/m
2)
Years i
Table 3. Laboratory data before and 1 year after laparoscopic adjustable gastric banding Preoperatively 1 yr postoperatively p BMI (kg/m2) 42.7± 6.0 35.3± 6.6 < 0.001* SBP (mmHg) 136.9± 22.7 140.8± 22.4 0.870 DBP (mmHg) 85.5± 13.4 85.7± 18.5 0.566 Glucose (mg/dL) 105.2± 36.2 84.6± 8.1 0.040* TC (mmol/L) 198.0± 35.9 189.8± 31.3 0.017* HDL-C (mmol/dL) 44.02± 13.1 50.6± 12.7 0.018* TG (mg/dL) 188.5± 148.6 101.4± 45.9 0.008* Uric acid (mg/dL) 7.69± 1.69 6.66± 1.44 < 0.001* AST (IU/L) 33.5± 23.4 23.4± 9.6 0.004* ALT (IU/L) 51.5± 44.7 25.2± 16.2 < 0.001* RGT (IU/L) 46.7± 32.9 24.9± 11.1 0.017* Albumin (g/dL) 4.75± 0.31 4.36± 0.26 0.514 T-protein (g/dL) 7.4± 1.3 7.4± 0.4 0.219 ALP (IU/L) 75.7± 27.5 55.1± 47.7 0.393 Ca (mg/dL) 8.9± 0.4 9.0± 0.4 0.858 WBC (103/μL) 8.70± 2.30 6.87± 1.53 < 0.001* Hemoglobin (g/dL) 14.1± 1.67 14.1± 1.8 0.383 MCV 85.6± 6.9 86.8± 6.8 0.411 Insulin (pmol/L) 22.5± 20.5 8.02± 4.44 0.007* C-peptide (mmol/L) 3.91± 2.76 2.28± 0.82 0.020* HbA1C (IU/L) 6.2± 1.2 5.3± 0.4 0.002*
*p< 0.05. BMI = body mass index; SBP = systolic blood pressure; DBP = diastolic blood pressure; TC = total cholesterol; HDL-C; high-density lipoprotein cholesterol; TG = triglycerides; AST = aspartate aminotransferase; ALT = alanine aminotransferase; RGT = gamma-glutamyl transpeptidase; ALP = alkaline phosphatase; WBC = white blood cell; MCV = mean corpuscular volume; HbA1C = glycosylated hemoglobin.
Discussion
TThis is the first prospective study of LAGB in T
Taiwan and Asia. The present study confirmed that LAGB is a safe and effective minimally invasive bariatric surgical procedure suitable for use in A
Asians. In our experience, LAGB could be per-formed with a 0% major complication rate and 3.3% minor complication rate, which are compat-ible with other reports.9–14The only early compli-cation in this study was postoperative transient esophageal stenosis due to the band being too small for the super-obese patient. This complica-tion can be avoided either by removal of the thick fat pad over the His angle or by using a larger band. A
All the three incidences of this complication in our study occurred before the introduction of a larger LAGB (the Vanguard Lap-Band system). This com-plication was avoided thereafter. Before the matu-ration of this technique, the late complication rate
was reported to be up to 30%, including slippage, band erosion and tube failure.8In this study, no slippage, band erosion or port infection was ob-served up to 2 years postoperatively, and only one band (1.1%) has been removed up till now.
Results of LAGB in the West have shown that good weight loss and significant reduction in obesity-related illness can be achieved. Inter-national experience with the LAGB in Europe and Australia shows a reduction in BMI of 9–13 kg/m2 from baseline within 2 years of placement.9–14 Weight loss continues even up to 5 years after sur-gery and stabilizes up to 9 years of follow-up.9–14 Data from the United States are controversial. An initial trial reported a mean BMI reduction of 8.7 over 3 years and 28% of the LAGB were removed because of complications.15 However, with im-provements in the techniques, some recent studies have reported similar data to the international experience.16,17 The mean BMI reduction of 8.8
and late complication rate of 7.7% in this series are consistent with other studies.
Vertical banded gastroplasty (VBG) has been a popular bariatric operation in Taiwan for the past two decades, and results have shown the procedure to be effective over a 15-year follow-up.18 After a report of the feasibility of laparoscopic VBG (LVBG),19we conducted a retrospective study com-paring conventional VBG and LVBG, and con-cluded that LVBG was a better procedure because of less pain, shorter hospital stay and less woundaa complications.20However, VBG has some notori-ous long-term problems, such as regain of weight, v
vomiting, and impairment of gastrointestinal quality of life. In an analysis by van Germert et al, up to 56% of VBG patients needed revisional surgery over a period of 12 years.21In our 5-year follow-up, the revision rate was 9.2%, which is compatible with the reported results for conven-tional VBG.22,23LAGB, as an alternative restrictive procedure, has the benefits of simpler standard-ized procedure, fewer complications, and sus-tained weight loss due to its adjustability. Our study confirmed the safety of LAGB and sustained w
weight loss up to 3 years. The mean operation time is also shorter in LAGB than in LVBG, 88.3 minutes v
versus 173 minutes.20 Although the results of w
weight reduction are similar between LAGB and LVBG, the 0% major complication rate and 3.3% minor complication rate of LAGB are lower than the 1% major complication rate and 5% minor complication rate of LVBG. The revision rate of LAGB is 1.3%, which is also lower than the 9.2% revision rate of LVBG.22,23Therefore, we strongly recommend LABG to replace LVBG in Taiwan.
Laparoscopic gastric bypass (LGB) is another common surgical procedure for morbidly obese patients and is the most commonly performed bariatric procedure in the United States.5Although LGB is more effective than LVBG, the complication rate is higher than that of LVBG. In our previous study, we found that LGB is much more difficult in terms of technique and carried more than three times the risk of major complications than VBG.24 T
The learning curve for LGB is also much steeper than for LAGB. For example, the complication rate
for a surgeon performing the first 19 cases was g reported to be four times higher than performing the procedure after 20 cases.25 In our series, the learning curve of LAGB is 10 cases, which is much lower than the 20 cases for LGB.24Although LGB r results in better weight reduction than LVBG or f LAGB, there is no difference in the resolution of obesity-related comorbidities.26Because bariatricc surgery in Asia is still in its infancy, how laparo-scopic bariatric surgery can be performed safely is the most important current issue. Therefore, LAGB is the recommended primary bariatric procedure for Asian people at present.27
The well-known inverse relationship between life expectancy and obesity is presumably, in large part, due to multiple cardiovascular and meta-bolic comorbidities. Our previous study disclosed a higher prevalence of metabolic abnormalities t in obese Taiwanese patients referred for weight reduction surgery.28However, significant weightt reduction 1 year after surgery markedly improved all aspects of the metabolic syndrome and resulted in a cure rate of over 95%.26This study confirmed the efficacy of bariatric surgery in the resolution of obesity-related comorbidities except hyperten-sion. The possible explanation for this might be that the case number is small and the procedure is different compared to our previous report.26The r follow-up is also short when compared to another study.29As hypertension has a more complicated mechanism than the other metabolic complica-tions of obesity, ethnic differences may also be a possible explanation.30,31
y Current indications for surgery in morbidly obese patients include BMI> 40 kg/m2 or > 35 kg/m2if comorbidities are present. However, these criteria are based on data from Caucasians.4 Itt has been amply demonstrated that Asians, in general, have a higher percent of body fat at a given BMI than Caucasians.30,31Morbidities and mortality among Asians occur at lower BMIs and c smaller waist circumferences. The Asia-Pacific Bariatric Surgery Group has recently recom-mended bariatric surgery in Asian patients with BMI> 37 kg/m2 or > 32 kg/m2 when diabetes or two other obesity-related comorbidities are
present.26Cost-effectiveness studies of LAGB in the treatment of severely obese patients are needed.
References
1. Must A, Spadano J, Coakley EH, et al. The disease burden associated with overweight and obesity. JAMA 1999;282: 1523–9.
2. Allison DB, Fontaine KR, Manson JE, et al. Annual deaths attributable to obesity in the United States. JAMA 1999; 284:1530–8.
3. Mokdad AH, Marks JS, Stroup DR, et al. Actual causes of death in the United States, 2000. JAMA 2004;291:1238–45. 4. NIH Conference. Gastrointestinal surgery for severe
obe-sity. Ann Int Med 1991;115:959–61.
5. Fisher BL, Schauer P. Medical and surgical options in the treatment of severe obesity. Am J Surg 2002;12:569–72. 6. Buchwald H, Avidor Y, Brauwald E, et al. Bariatric surgery:
a systematic review and meta-analysis. JAMA 2004;292: 1724–37.
7. Kuzmak L. Silicone gastric banding: a simple and effective
operation for morbid obesity. Comtemp Surg 1986;28:13–8. 8. Belachew M, Legrand M, Vincent V, et al. Laparoscopic adjustable gastric banding. World J Surg 1998;22:955–63. 9. O’Brien PE, Brown WA, Smith A, et al. Prospective study of a laparoscopically placed, adjustable gastric band in the treatment of morbid obesity. Br J Surg 1999;86:113–8. 10. Dixon JB, O’Brien PE. Changes in comorbidities and
im-provements in quality of life after LAP-BAND placement. Am J Surg 2002;184:51S–4S.
11. Favretti F, Cadiere GB, Segato G, et al. Laparoscopic band-ing: selection and technique in 830 patients. Obes Surg 2002;12:385–90.
12. Zinzindohouse F, Chevallier JM, Douard R, et al. Laparo-scopic gastric banding: a minimally invasive surgical treat-ment for morbid obesity. Ann Surg 2003;237:1–9. 13. Angrisani L, Furbetta F, Doldi SB, et al. Lap Band adjustable
gastric banding system: the Italian experience with 1863 pa-tients operated on 6 years. Surg Endosc 2003;17:409–12. 14. Dargent J. Surgical treatment of morbid obesity by
adjust-able gastric band: the case for a conservative strategy in the case of failure—a 9-year series. Obes Surg 2004;14: 986–90.
15. DeMaria EJ, Sugerman HJ, Meador JG, et al. High failure rate after laparoscopic adjustable gastric banding for treat-ment of morbid obesity. Ann Surg 2001;233:809–18.
f 16. Ren CJ, Weiner M, Allen JW. Favorable early results of gastric banding for morbid obesity: the American experi-ence. Surg Endosc 2004;18:543–6.
17. Spivak H, Hewitt MF, Onn A, et al. Weight loss and improve-ment of obesity related illness in 500 U.S. patients following laparoscopic adjustment gastric banding procedure. Am J Surg 2005;189:27–32.
18. Chen KM, Lee WJ, Lai HS, et al. Fifteen year’s experience with gastric partitioning for obesity treatment. J Formos Med Assoc 1998;97:381–6.
19. Lee WJ, Huang MT, Lai IR, et al. Laparoscopic vertical banded gastric partition. Formosan J Surg 1999;32:165–71. 20. Lee WJ, Lai IR, Huang MT, et al. Laparoscopic versus open vertical banded gastroplasty for the treatment of morbid obesity. Surg Laparosc Endosc Percut Techn 2001;11: 9–13.
21. van Gemert WG, van Wersch MD, Greve JWM, et al. Revisional surgery after failed vertical banded gastroplasty or conversion to gastric bypass. Obes Surg 1998;8:21–8.
f 22. Lee WJ, Yu PJ, Wang W, et al. Gastrointestinal quality of life following laparoscopic vertical banded gastroplasty. Obesity Surgery 2002;12:819–24.
23. Wang W, Huang MT, Wei PL, et al. Laparoscopic mini-gastric bypass for failed vertical banded gastroplasty. Obes Surg 2004;14:777–82.
24. Lee WJ, Huang MT, Yu PJ, et al. Laparoscopic vertical banded gastroplasty and laparoscopic gastric bypass: a comparison. Obes Surg 2004;14:626–34.
25. Flum DR, Dellinger EP. Impact of gastric bypass operation on survival: a population-based analysis. J Am Coll Surg 2004;199:543–51.
26. Lee WJ, Huang MT, Wang W, et al. Effects of obesity surgery on metabolic syndrome. Arch Surg 2004;139:1088–92. 27. Lee WJ, Wang W. Bariatric surgery: Asia-pacific
perspec-tive. Obes Surg 2005;15:751–7.
28. Lee WJ, Wang W, Wei PL, et al. Metabolic syndrome in obese patients referred for weight reduction surgery in Taiwan. J Formos Med Assoc 2003;102:459–64. 29. Sjostrom L, Lindroos AK, Peltonen M, et al. Lifestyle,
dia-betes, and cardiovascular risk factors 10 years after bariatric surgery. New Engl J Med 2004;351:2683–93.
30. Deurenberg P, Deurenberg-Yap M, van Staveren WA. Body mass index and percent body fat: a meta-analysis among different ethnic groups. Int J Obes 1998;22: 1164–71.
31. Chang CJ, Wu CH, Chang CS, et al. Low body mass index but high percent body fat in Taiwanese subjects: implica-tions of obesity cutoffs. Int J Obes 2003;27:253–9.