Research report
Increased risk of developing stroke among patients with bipolar
disorder after an acute mood episode: A six-year follow-up study
Herng-Ching Lin
a, Shang-Ying Tsai
b,c, Hsin-Chien Lee
b,c,⁎
a
School of Health Care Administration, Taipei Medical University, Taipei, Taiwan
bDepartment of Psychiatry, Taipei Medical University Hospital, 252 Wu-Hsing St., Taipei 110, Taiwan cDepartment of Psychiatry, School of Medicine, Taipei Medical University, Taipei, Taiwan
Received 17 July 2006; received in revised form 16 September 2006; accepted 18 September 2006 Available online 23 October 2006
Abstract
Background: Despite cerebrovascular diseases having been reported as one of the major causes of death among patients with bipolar disorder, there is scant information on the risk of stroke among this patient population. This study estimated the relative risk of developing stroke among patients with bipolar disorder in 6 years following hospitalization for an acute mood episode compared with patients undergoing appendectomy.
Methods: Two study cohorts were identified from the Taiwan National Health Insurance Research Database for the year 1998: patients hospitalized with bipolar disorder, and patients undergoing an appendectomy. Follow-up was undertaken to determine whether sampled patients had utilized emergency medical services for the management of any type of stroke in the period 1998–2003. Results: Stroke occurred among 2.97% of patients with bipolar disorder and 1.50% of patients undergoing appendectomy between 1998 and 2003. The adjusted odds ratio of developing stroke, by cohort, shows that after adjusting for demographic characteristics, comorbid medical disorder, and substance or alcohol dependence, patients with bipolar disorder were more likely to develop stroke (OR = 2.05; 95% CI = 1.73–3.54).
Limitations: The validity of diagnoses, lacking of information on smoking, body mass index, and socioeconomic status, and possible selection bias might compromise the findings.
Conclusions: During the six-year follow-up period, the likelihood of developing stroke was twice as great amongst patients with bipolar disorder as patients undergoing an appendectomy. A requirement exists for the initiation of research providing an understanding of the pathophysiological mechanisms of the association between stroke and bipolar disorder.
© 2006 Elsevier B.V. All rights reserved.
Keywords: Bipolar disorder; Stroke; Case-control studies
1. Introduction
As a major psychiatric disorder characterized by fluctuations between depression and mania, bipolar disorder is a devastating condition with severe economic and social impacts (Simon, 2003). The lines of evidence suggest that in addition to the psychiatric symptoms and attendant dysfunction, bipolar disorder is associated ⁎ Corresponding author. Department of Psychiatry, Taipei Medical
University Hospital, 252 Wu-Hsing St., Taipei 110, Taiwan. Tel.: +886 2 2737 2181x3667; fax: +886 2 2378 9788.
E-mail address:[email protected](H.-C. Lee).
0165-0327/$ - see front matter © 2006 Elsevier B.V. All rights reserved. doi:10.1016/j.jad.2006.09.016
with several medical conditions leading to substantial morbidity and mortality (Osby et al., 2001; Angst et al., 2002). As a result of the increasing medical burden in the healthcare of patients with bipolar disorder, it has now become a matter of some urgency to gain a greater understanding of this condition (Kupfer, 2005).
Within the studies focusing on medical illnesses among patients with bipolar disorder, the most common medical problems cited are obesity, diabetes mellitus and subsequent cardiovascular disease; all of these medical conditions, as well as depressive symptoms, are recog-nized as risk factors for stroke (Everson et al., 1998; Krishnan, 2005). Thus, there would appear to be a bio-logically plausible association between bipolar disorder and stroke.
Nevertheless, there is scant information on the risk of developing stroke among patients with bipolar disorder, despite cerebrovascular diseases having been reported as one of the major causes of death among this particular patient population (Hoyer et al., 2000; Joukamaa et al., 2001; Tsai et al., 2005). Indeed, there has been only one prior study, undertaken byNilsson and Kessing (2004), which used a Danish registry dataset to estimate the risk, among patients previously discharged with affective disorder, of receiving a stroke diagnosis. They could not find any association between manic/bipolar disorder and stroke.
The aim of the present study is to estimate the risk of developing stroke among patients with bipolar disorder in 6 years following hospitalization for an acute mood episode, as compared to another cohort of patients un-dergoing an appendectomy during the same period. Patients were identified from a nationwide population-based dataset provided by the Taiwan National Health Insurance Research Database (NHIRD) for the year 1998, with follow-up being carried out until the end of 2003. The risks of developing stroke for these two cohorts were subsequently calculated and compared after adjusting for demographic characteristics and co-morbid medical conditions.
2. Methods 2.1. Database
This study used administrative claims data from the NHIRD, published by the National Health Research Institute in Taiwan, covering the years 1998 to 2003. The dataset includes all claims data from the National Health Insurance (NHI) program, a program implemen-ted in Taiwan in March 1995 as a means of financing healthcare for all Taiwanese citizens. The NHI program
currently has over 21 million enrollees, representing around 96% of the island's population, and is charac-terized by a single-payer payment system with unre-stricted access to any mental healthcare provider of the patient's choice. Thus, the NHRID is possibly the largest and most comprehensive population-based data source currently available anywhere, and offers a unique opportunity to identify the risk of developing stroke amongst patients with bipolar disorder.
3. Study sample
Our two study cohorts comprised of (i) all patients, aged 18 or over, hospitalized for bipolar disorder, with an ICD-9-CM code of 296.0X, 296.4X, 296.5X, 296.6X, 296.7X, 296.80 or 296.89 as the primary diagnosis between January and December 1998; and (ii) all patients aged 18 or over hospitalized for an appendectomy, with an ICD-OP code of 47.0 as the primary operative procedure over the same period. Patients undergoing an appendec-tomy were excluded if they had been diagnosed as having any major psychiatric disorder (ICD-9-CM codes 290, 294, 295, 296 or 297). Ultimately, 18,702 eligible patients were selected for this study, 2289 with bipolar disorder and 16,413 undergoing an appendectomy.
The reason for the selection of those patients who had undergone an appendectomy as the control group was that they were relatively indistinguishable from the general population; indeed, there were no statistically-significant differences found between the control cohort and the general population with regard to either gender or age. Furthermore, to the best of our knowledge, the procedures involved in an appendectomy have no known long-term impacts on brain functioning, and indeed, there has never been any study reporting any increased risk of bipolar disorders among patients undergoing an appendectomy.
Follow-up of these two study cohorts was subse-quently undertaken until the end of 2003 in order to determine whether any of sampled patients had utilized emergency medical services for the management of any type of stroke (ICD-9-CM codes 430–438). Since a substantial number of stroke victims do not survive beyond their visit to the emergency department, the utilization of emergency department services, rather than the consumption of inpatient care, may better reflect the actual scenario of stroke incidence.
4. Statistical analysis
The SAS statistical package (SAS System for Win-dows, Version 8.2) was used to perform the statistical
analyses. Descriptive statistical analyses, including fre-quency and percentage, were performed on all of the identified variables, with Chi-square tests also being used to examine the differences between the two cohorts, in terms of demographic characteristics, comorbid medical disorders, and alcohol or substance dependence. Demo-graphic characteristics included age, gender and geo-graphical region, with patient age being categorized into one of the four groups,b45, 45–64, 65–74 and N74 years. The geographical region within which patients were located was also taken into consideration since geograph-ical variations in the incidence of strokes has been demonstrated in a prior study (Engstrom et al., 2001). Comorbid medical disorders including hypertension, diabetes, hyperlipidemia, chronic obstructive pulmonary disease (COPD) or renal disease were recognized from claim data at the time of the index discharge because they might increase the risk of developing stroke.
The multiple logistic regression analyses were em-ployed in order to compare calculations, between these two study cohorts, of the crude and adjusted odds ratio of developing stroke after the index discharge. Our analysis provides adjustment for patient demographic character-istics, comorbid medical disorders, and alcohol or sub-stance dependence. A significance level of pb0.05 was adopted for this study.
5. Results
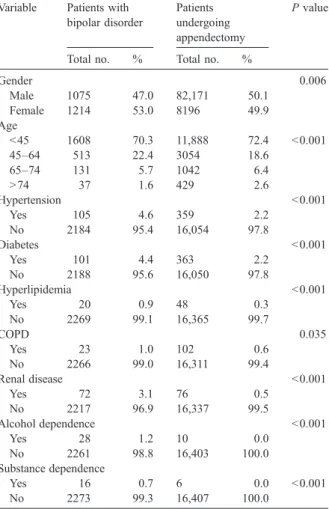
The results show that the median age for those patients with bipolar disorder was 36 years (interquartile range, 28–47 years), while the median age for those patients undergoing an appendectomy was 34 years (interquartile range, 26–46 years).Table 1describes the distribution of the demographic characteristics and comorbid medical disorders for these two cohorts. As the table shows, as compared to those patients undergoing an appendectomy, patients with bipolar disorder were more likely to be female and comorbid with hypertension ( pb0.001), dia-betes ( pb0.001), hyperlipidemia ( pb0.001), COPD ( p = 0.035), renal disease ( pb0.001), alcohol dependence ( pb0.001) or substance dependence ( pb0.001) at the time of the index discharge.
Table 2 provides details for the six-year follow-up period on the likelihood of developing stroke for the two cohorts, with stroke having occurred among 2.97% of the patients with bipolar disorder, and 1.50% of the patients undergoing an appendectomy between 1998 and 2003 ( pb0.001). The crude odds ratio indicates that, as compared to patients undergoing an appendec-tomy, the likelihood of developing stroke during the follow-up period was twice as great for patients with bipolar disorder.
Details on the adjusted odds ratio of the development of stroke, by cohort, are presented in Table 3. As the table shows, after adjusting for demographic character-istics, comorbid medical disorders, and substance or Table 1
Demographic characteristics and comorbid medical disorders of sampled patients with bipolar disorder and undergoing an appendectomy in Taiwan, 1998 (n = 18,702)
Variable Patients with bipolar disorder
Patients undergoing appendectomy
P value
Total no. % Total no. %
Gender 0.006 Male 1075 47.0 82,171 50.1 Female 1214 53.0 8196 49.9 Age b45 1608 70.3 11,888 72.4 b0.001 45–64 513 22.4 3054 18.6 65–74 131 5.7 1042 6.4 N74 37 1.6 429 2.6 Hypertension b0.001 Yes 105 4.6 359 2.2 No 2184 95.4 16,054 97.8 Diabetes b0.001 Yes 101 4.4 363 2.2 No 2188 95.6 16,050 97.8 Hyperlipidemia b0.001 Yes 20 0.9 48 0.3 No 2269 99.1 16,365 99.7 COPD 0.035 Yes 23 1.0 102 0.6 No 2266 99.0 16,311 99.4 Renal disease b0.001 Yes 72 3.1 76 0.5 No 2217 96.9 16,337 99.5 Alcohol dependence b0.001 Yes 28 1.2 10 0.0 No 2261 98.8 16,403 100.0 Substance dependence Yes 16 0.7 6 0.0 b0.001 No 2273 99.3 16,407 100.0 Table 2
Crude odds ratio of developing stroke during six-year follow-up period for sampled patients with bipolar disorder and undergoing an appendectomy in Taiwan (n = 18,702)
Variable Patients with bipolar disorder
Patients undergoing appendectomy Total no. % Total no. % Developing stroke
Yes 69 2.97 246 1.50
No 2221 97.93 16,166 98.50
Crude OR 2.00 1.00
alcohol dependence, sampled patients with bipolar disorder were more likely to develop stroke during the follow-up period than their counterparts undergoing an appendectomy (OR = 2.05; 95% CI = 1.73–3.54). Fur-thermore, as expected, there was a greater likelihood of the development of stroke among those patients comor-bid with hypertension (OR = 1.89; 95% CI = 1.32–2.69) and diabetes (OR = 2.48; 95% CI = 1.73–3.58).
6. Discussion
To the best of our knowledge, our study represents the first attempt to investigate the risk of developing stroke among patients with bipolar disorder in 6 years following hospitalization for an acute mood episode, after adjusting for patient's demographic characteris-tics, comorbid medical disorders, and substance or alcohol dependence. We find that the likelihood of the development of stroke during the six-year follow-up
period was twice as great among patients with bipolar disorder as compared to their counterparts who had undergone an appendectomy. The findings of this study contradict the observations reported in the prior study by Nilsson and Kessing (2004); nonetheless, patients with affective disorder in their study were categorized in accordance with the ongoing episode at the time of their referral, as patients suffering from either depres-sion or mania. Those patients in the depresdepres-sion group who were found to have an increased risk of developing stroke may actually have been cases of bipolar disorder with a depressive episode. A further reason for the discrepancy could actually arise from the control cohort, since patients with osteoarthritis may have been taking non-steroidal anti-inflammatory drugs (NSAIDs) which would of course have some influence on the risk of developing stroke (Qureshi et al., 2001; Qureshi, 2003).
The actual mechanisms contributing to the associa-tion between bipolar disorder and the subsequent devel-opment of stroke remain unclear. An unhealthy lifestyle, comorbid medical conditions, and the use of psycho-tropic medications could all contribute to the increased risk of stroke among patients with bipolar disorder; however, they could also be at an increased risk of stroke as a result of their existing brain vulnerability. A number of prior neuroimaging studies have consistently reported structural brain abnormalities among patients with bipolar disorder (Drevets et al., 1997; Adler et al., 2005; Lyoo et al., 2006). The neuroanatomical deficits may well be present in the early stages of bipolar dis-order and may become aggravated as the disease prog-resses (Kaur et al., 2005).
Enhanced platelet activity and hypercoagulability have been reported to be associated with depression (Nemeroff and Musselman, 2000; von Kanel et al., 2001). These alterations in hemostatic function may contribute to the development of stroke among patients with bipolar disorder. Besides, studies indicate activa-tion of inflammatory response system in patients with bipolar disorder (Tsai et al., 1999; Tsai et al., 2001). The elevation of certain proinflammatory cytokines may play an important role in the pathogenesis of stroke (Arumugam et al., 2005).
Furthermore, it is possible that bipolar disorder may share a common etiology with stroke, with recent studies having suggested that glycogen synthase kinase-3 (GSK-3), an emerging therapeutic target for bipolar disorder, could be a crucial element in the pathogenesis of atherothrombosis (Gould et al., 2004; Eto et al., 2005). The close relationship between bipolar disorder and stroke indicates the urgent need for the integration of Table 3
Adjusted odds ratio of developing stroke during six-year follow-up period for sampled patients with bipolar disorder and undergoing an appendectomy in Taiwan (n = 18,702)
Variables Developing stroke
OR 95% CI p value Cohort
Bipolar disorder 2.05 1.73–3.54 b0.001 Appendectomy (reference group) 1.00
Gender
Male 1.48 1.17–1.87 0.001 Female (reference group) 1.00
Age b45 (reference group) 1.00 45–64 7.06 5.10–9.78 b0.001 65–74 14.99 10.49–21.42 b0.001 N74 26.19 17.51–39.18 b0.001 Geographic location
Northern (reference group)
Central 1.05 0.77–1.44 0.743 Southern 1.31 1.00–1.70 0.049 Eastern 1.88 1.03–3.44 0.039 Hypertension Yes 1.89 1.32–2.69 b0.001 Diabetes Yes 2.48 1.73–3.58 b0.001 Hyperlipidemia Yes 0.65 0.08–5.09 0.697 COPD Yes 1.09 0.51–2.33 0.817 Renal disease Yes 0.57 0.17–1.85 0.347 Alcohol dependence Yes 3.42 1.21–9.22 b0.001 Substance dependence Yes 8.69 1.06–71.06 0.044
psychiatry into the mainstream of medicine as a clinical neuroscience discipline (Insel and Quirion, 2005). 7. Limitations
A particular strength of this study is the use of a population-based dataset which enables us to trace all stroke incidents; nevertheless, this study still suffers from three limitations which should be addressed. First of all, the psychiatric and stroke diagnoses, which rely on administrative data reported by physicians or hos-pitals, may be less accurate than those made under a standardized schedule; however, the development of such a population-based dataset containing this sort of information would be extremely costly and difficult to achieve.
Secondly, there was no availability for use in this study of data on tobacco use, body mass index and socioeconomic status, all of which might influence the risk of developing stroke. Since a number of prior studies have observed a greater frequency of heavy smoking among psychiatric patients, there may even be some underestimation of the odds ratio of the develop-ment of stroke among patients with bipolar disorder.
Thirdly, the sample of patients bipolar disorder used in this study was based upon acute mood episodes which occurred during the first year of the study period; as such, they may not be a truly representative cohort of all patients with bipolar disorder since symptom-free pa-tients would have been excluded from the study sample. 8. Conclusions
Despite these limitations, we have found that during the six-year follow-up period, the risk of developing stroke was about twice as great amongst patients with bipolar disorder, as compared patients undergoing an appendectomy, and that this association was totally independent of any initial comorbid hypertension, diabe-tes, hyperlipidemia and alcohol or substance dependence. We believe that there is an urgent requirement for the initiation of research aimed at gaining a better under-standing of the underlying pathophysiological mecha-nisms of stroke and their association with bipolar disorder. The findings of this study may also fill the knowledge gap with regard to the comorbidity of bipolar disorder with other medical illnesses, reflecting the fact that the treatment of bipolar disorder has traditionally been segregated from general medical care.
In order to prevent any adverse outcomes, practicing psychiatrists and other mental healthcare professionals must be aware of the increased risk of the development
of stroke among patients with bipolar disorder and encouraged to be with the ultimate aim of providing more integrated intervention.
Acknowledgements
This study is supported by Topnotch Stroke Research Center Grant, Ministry of Education, Taiwan. This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by the National Health Research Institutes, Taiwan. The interpretations and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health, or the National Health Research Institutes.
References
Adler, C.M., Levine, A.D., DelBello, M.P., Strakowski, S.M., 2005. Changes in gray matter volume in patients with bipolar disorder. Biol. Psychiatry 58, 151–157.
Angst, F., Stassen, H.H., Clayton, P.J., Angst, J., 2002. Mortality of patients with mood disorders: follow-up over 34–38 years. J. Affect. Disord. 68, 167–181.
Arumugam, T.V., Granger, D.N., Mattson, M.P., 2005. Stroke and T-cells. Neuromolecular Med. 7, 229–242.
Drevets, W.C., Price, J.L., Simpson Jr., J.R., Todd, R.D., Reich, T., Vannier, M., Raichle, M.E., 1997. Subgenual prefrontal cortex abnormalities in mood disorders. Nature 386 (6627), 824–827. Engstrom, G., Jerntorp, I., Pessah-Rasmussen, H., Hedblad, B., Berglund,
G., Janzon, L., 2001. Geographic distribution of stroke incidence within an urban population: relations to socioeconomic circumstances and prevalence of cardiovascular risk factors. Stroke 32, 1098–1103. Eto, M., Kouroedov, A., Cosentino, F., Luscher, T.F., 2005. Glycogen synthase kinase-3 mediates endothelial cell activation by tumor necrosis factor-α. Circulation 112, 1316–1322.
Everson, S.A., Roberts, R.E., Goldberg, D.E., Kaplan, G.A., 1998. Depressive symptoms and increased risk of stroke mortality over a 29-year period. Arch. Intern. Med. 158, 1133–1138.
Gould, T.D., Zarate, C.A., Manji, H.K., 2004. Glycogen synthase kinase-3: a target for novel bipolar disorder treatments. J. Clin. Psychiatry 65, 10–21.
Hoyer, E.H., Mortensen, P.B., Olesen, A.V., 2000. Mortality and causes of death in a total national sample of patients with affective disorders admitted for the first time between 1973 and 1993. Br. J. Psychiatry 176, 76–82.
Insel, T.R., Quirion, R., 2005. Psychiatry as a clinical neuroscience discipline. JAMA 294, 2221–2224.
Joukamaa, M., Heliovaara, M., Knekt, P., Aromaa, A., Raitasalo, R., Lehtinen, V., 2001. Mental disorders and cause-specific mortality. Br. J. Psychiatry 179, 498–502.
Kaur, S., Sassi, R.B., Axelson, D., Nicoletti, M., Brambilla, P., Monkul, E.S., Hatch, J.P., Keshavan, M.S., Ryan, N., Birmaher, B., Soares, J.C., 2005. Cingulate cortex anatomical abnormalities in children and adoles-cents with bipolar disorder. Am. J. Psychiatry 162, 1637–1643. Krishnan, K.R., 2005. Psychiatric and medical comorbidity of bipolar
Kupfer, D.J., 2005. The increasing medical burden in bipolar disorder. JAMA 293, 2528–2530.
Lyoo, I.K., Sung, Y.H., Dager, S.R., Friedman, S.D., Lee, J.Y., Kim, S.J., Kim, N., Dunner, D.L., Renshaw, P.F., 2006. Regional cerebral cortical thinning in bipolar disorder. Bipolar Disord. 8, 65–74. Nemeroff, C.B., Musselman, D.L., 2000. Are platelets the link
between depression and ischemic heart disease? Am. Heart J. 140, 57–62.
Nilsson, F.M., Kessing, L.V., 2004. Increased risk of developing stroke for patients with major affective disorder—a registry study. Eur. Arch. Psychiatry Clin. Neurosci. 254, 387–391.
Osby, U., Brandt, L., Correia, N., Ekbom, A., Sparen, P., 2001. Excess mortality in bipolar and unipolar disorder in Sweden. Arch. Gen. Psychiatry 58, 844–850.
Qureshi, A.I., 2003. Nonsteroidal anti-inflammatory drugs and the risk of intracerebral hemorrhage. Stroke 34, 379–386.
Qureshi, A.I., Tuhrim, S., Broderick, J.P., Batjer, H.H., Hondo, H., Hanley, D.F., 2001. Spontaneous intracerebral hemorrhage. N. Engl. J. Med. 344, 1450–1460.
Simon, G.E., 2003. Social and economic burden of mood disorders. Biol. Psychiatry 54, 208–215.
Tsai, S.Y., Chen, K.P., Yang, Y.Y., Chen, C.C., Lee, J.C., Singh, V.K., Leu, S.J., 1999. Activation of indices of cell-mediated immunity in bipolar mania. Biol. Psychiatry 45, 989–994.
Tsai, S.Y., Yang, Y.Y., Kuo, C.J., Chen, C.C., Leu, S.J., 2001. Effects of symptomatic severity on elevation of plasma soluble interleu-kin-2 receptor in bipolar mania. J. Affect. Disord. 64, 185–193. Tsai, S.Y., Lee, C.H., Kuo, C.J., Chen, C.C., 2005. A retrospective
analysis of risk and protective factors for natural death in bipolar disorder. J. Clin. Psychiatry 66, 1586–1591.
von Kanel, R., Mills, P.J., Fainman, C., Dimsdale, J.E., 2001. Effects of psychological stress and psychiatric disorders on blood coagulation and fibrinolysis: a biobehavioral pathway to coronary artery disease? Psychosom. Med. 63, 531–544.