BRIEF C O M M U N I C A T I O N S
Transcatheter embolization in treatment
of congenital coronary artery aneurysm
Ming-Fong Chen, MD, a Kuo-Liong Chien, MD, a Yvk-Ming Tsang, MD, b Chiau-Suong Liau, MD, a and Ynan-Teh Lee, MDa
Taipei, Taiwan
Congenital coronary artery aneurysm and coronary arterio- venous fistula are two rare conditions.l~ An interesting case of a congenital coronary artery aneurysm that drained to a coronary arteriovenous fistula is presented. The aneurysm was successfully treated by transcatheter embolization with a complex helical fibered platinum coil. TO the best of our knowledge this is the first case report of such an aneurysm treated by artificial embolization.
A 52-year-old man was admitted with a 1-year history of occasional chest tightness. His coronary risk factors in- cluded family history, male sex, sedentary lifestyle, and age. The result of physical examination was unremark- able. Blood pressure was 120/76 mm Hg. The pulse rate was 72 beats/min~ with regular beat. A chest x-ray film and a resting electrocardiogram were normal. A treadmill ex- ercise test with the standard Bruce protocol showed a neg- ative result. The exercise duration was 8 minutes without significant changes. Echocardiography and all blood chem- istries were normal. No oxygen step-u p occurred during cardiac catheterization. Left ventriculography showed nor- mal chamber size and wall motion. Select coronary arteri- ograms showed a patent right coronary artery. However, the left coronary artery had a saccular type aneurysm (1.2 × 1.1 × 1.3 cm) rising from a branch of the left ante- rior descending coronary artery (Fig. 1, left). The efferent vessel of the aneurysm connected to a coronary arterio- venous fistula originating from the left main coronary ar- tery, which drained to the left pulmonary artery. To pre- vent sudden death from aneurysm rupture, treatment of such a condition was considered mandatory. A 7F JL4 guiding catheter (Cordis) for coronary angioplasty was put to the orifice of the left coronary artery through the right femoral artery. A 3F infusion catheter (Target Therapeu- tics) was introduced into the neck of the aneurysm via a steerable 0.016-inch guide wire. The guide wire was then removed. A 2 mm/10 mm complex helical fibered platinum coil (Target Therapeutics) was pushed to the neck of the aneurysm by a coil pusher (Target Therapeutics), but high blood flow pushed the coil into the aneurysm. Another 3
From the aDepartments of Internal Medicine (Cardiology) and bRadiology National Taiwan University Hospital.
Reprint requests: Ming-Fong Chen, MD, Department of Internal Medicine (Cardiology), National Taiwan University Hospital, 7, Chung-Shan South Rd., Taipei, 10002, Taiwan.
AM HEART J 1996;131:396-7.
Copyright © 1996 by Mosby-Year Book, Inc. 0002-8703/96/$5.00 + 0 4]4]68061
mm/30 mm coil was put in place. The distal portion of the coil was put into the aneurysmal sac, and the proximal half was put in the afferent vessel. Follow-up angiograms showed the aneurysm as gradually nonvisualized. Approx- imately 15 rain later the whole aneurysm and the efferent vessel had virtually no flow (Fig. 1, right). The coronary arteriovenous fistula was not treated because it had no hemodynamic significance. No complications occurred. Follow-up has been uneventful for 10 months.
Coronary artery aneurysm and coronary arteriovenous fistula are detected with increasing frequency through the advent of coronary arteriography. These conditions are found in 1% to 2% and 0.31%, respectively, in patients who undergo coronary arteriographies.l-4 In adults more than half of the aneurysms are atherosclerotic in origin. In most cases the fistulae are small and without significant shunt, and the patient remains without symptoms. In the pres- ence of large shunts normal coronary trees may not be clearly visualized because of the "steal" effect of the fistula. Congestive heart failure may develop, especially during later life. The coexistence of these two anomalies is unusual. This patient had a fully visualized left coronary artery and no evidence of heart failure or oxygen step-up, which is compatible with a small shunt.
Cardiac catheterization with selective coronary angio- grams is the best modality for complete diagnosis of these two diseases, especially for the delineation of the distal drainage site. 1, 3,4 Other diagnostic procedures such as two-dimensional Doppler echocardiography with color flow mapping can accurately evaluate some of the anatomic features. 5 However, these examinations were of no value in our case. The most likely cause of the aneurysm in this patient would seem to be congenital. No history of trauma or clear history of Kawasaki disease was reported. Other workups for connective tissue disease and arteritis were unrevealing. It is interesting that the efferent vessel of the aneurysm did not drain to the myocardium, as is usual. Instead, it connected to a coronary arteriovenous fistula. This manifestation gave the chance of artificial emboliza- tion without risk of iatrogenic myocardial infarction. Transcatheter embolization has been used in the treat- ment of various diseases of the heart and elsewhere in the body. 6 This therapeutic modality provides precise and ef- fective occlusion of the target vessel, resulting in less my- ocardial damage, avoiding operative risks an ensuring a shorter hospital stay.
REFERENCES
1. Barettella MB, Bott-Silverman C. Coronary artery aneurysms: an un- usual case report and a review of the literature. Cathet Cardiovasc Di- agn 1993;29:57-61.
2. Aufiero TX, Campbell DB, Waldhausen JA. Coronary artery aneu- ~wsms. Am CoU Cardiol Curr J Rev 1994;3:48-51.
3. Liberthson RR, Sagan K, Berkoben DP, Weintraub RM, Levine FH. Congenital coronary arteriovenous fistula: report of 13 cases, review of the literature and delineation of management. Circulation 1979;59:844- 54.
Volume 131, Number 2
et at.
American Heart Journal
At-~'a~[
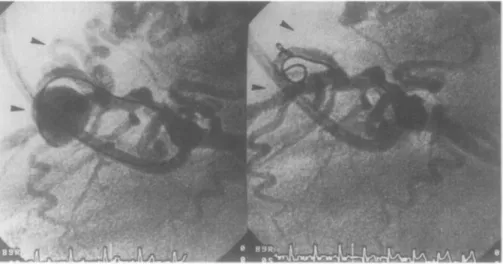
397Fig. 1. S a c c u l a r t y p e coronary a r t e r y a n e u r y s m is in l a t e r a l projection. A n e u r y s m a r i s e s from b r a n c h of left a n t e r i o r d e s c e n d i n g coronary a r t e r y
(left).
Efferent vessel of a n e u r y s m connects to coronary arterio- venous f i s t u l a o r i g i n a t i n g from left m a i n coronary a r t e r y , which d r a i n s to left p u l m o n a r y a r t e r y . Aneu- r y s m a n d efferent v e s s e l(arrows)
c a n n o t be seen after coil embolization(right).
4. Wright WP, Alpert MA, Mukerji V, Santolin CJ. Coronary artery an- eurysms: a case study and literature review. AngSology 1991;42:672-9. 5. Friedman DM, Rutkowski M. Coronary artery fistula: a pulsed Dop-
pler/two-dimensional echocardiographic study. Am J Cardiol 1985; 55:1652-5.
6. Reidy JF, Anjos RT, Qureshi SA, Baker EJ, Tynan MJ. Transcatheter embolization in the treatment of coronary artery fistulas. J Am Coll Cardiol 1991;18:187-92.
Left ventricular and aortic valve
thrombosis caused by polycythemia
rubra vera successfully treated with
streptokinase
S h u k r i A1-Saif, MB (Lon), M R C P ( U K ) , a
R a j i n d r a P. Bhat, MD, DM (Cardio), a A h m e d Hijazi, MD, DM, CES (Cardio), a A h m e d A1-Faraj, MD, C-ARBIM, a a n d
I s m a i l Quadri, MD, PhD b
Dammam, Saudi Arabia
Left v e n t r i c u l a r a n d left a t r i a l t h r o m b i a r e common a n d m a y r e s u l t in systemic embolization. P r o p h y l a c t i c antico- a g u l a t i o n is of p a r a m o u n t i m p o r t a n c e in t h e presence of a p r e d i s p o s i n g c a r d i a c lesion. ~ I n spite of this, some p a t i e n t s do not achieve a t h e r a p e u t i c level of a n t i c o a g u l a t i o n a n d a r e t h e r e f o r e a t r i s k of thrombosis. I n addition, p a t i e n t s a r e in de novo condition w i t h e s t a b l i s h e d t h r o m b i even
From the aDivision of Cardiovascular Medicine, Medical Oncology, and bRegional Laboratory Haematology Service, D a m m a m Central Hospital. Reprint requests: S. AI-Saif, MB, MRCP, ]P.O. Box 8606, D a m m a m 31942, Saudi Arabia.
AM HEART J 1996;131:397-9.
Copyright © 1996 by Mosby-Year Book, Inc. 0002-8703/96/$5.00 + 0 4/4/68059
Table I. Hemoglobin Hematocrit White blood count Platelets Bone marrow Oxygen saturation Leukocyte alkaline phosphatase score Prothrombin time Partial thromboplas- tin time Antithrombin III Lupus anticoagulant 18.4 gm/dl 61.6% 37.55 × 10 9/L 999 x 10 9/L
Hypercellular bone marrow on aspiration and biopsy involv- ing all three cell lines. Palli- sading of megakanycytes. De- pleted iron stores. Increased reticulin content.
(On room air) -96.2% 179 (reference range 30-100) 14.9 seconds (control 11.5 sec-
onds)
31.5 seconds (control 26 sec- onds)
Normal Negative
w h e n t h e y u n d e r g o a d e q u a t e anticoagulation. 2, 3 H e p a r i n is the s t a n d a r d t r e a t m e n t for t h e s e p a t i e n t s . 4 P a t i e n t s w i t h t h r o m b o s e d prosthetic valves a n d left v e n t r i c u l a r t h r o m b i h a v e been safely a n d successfully t r e a t e d w i t h thrombolytic t h e r a p y . 5, 6 This r e p o r t describes t h e use of such t h e r a p y i n a p a t i e n t w i t h t h r o m b i in t h e left ventricle a n d on t h e aortic valve caused b y p o l y c y t h e m i a r u b r a vera. A 60-year-old m a n was a d m i t t e d b e c a u s e of s u d d e n se- vere a b d o m i n a l pain. H e was found to h a v e congestive h e a r t failure, h y p e r t e n s i o n , a n d possible p o l y c y t h e m i a v e r a because of t h e l a b o r a t o r y findings d e t a i l e d in Table I. Before being a d m i t t e d to t h e hospital, he h a d h a d a n un- w i t n e s s e d episode of loss of consciousness l a s t i n g 10 m i n u t e s w i t h s u b s e q u e n t t o t a l recovery. Clinical a n d