The Value of Losartan Suppression Test in the Confirmatory Diagnosis
of Primary Aldosteronism in
Patients Over 50 Years Old
Chin-Chi Kuo1, Poojitha Balakrishnan1, Yenh- Chen Hsein 2, Vin-Cent Wu3, Shih-Chieh Jeff Chueh4, Yung-Ming Chen3, Kwan-Dun Wu3, Ming-Jiuh Wang5 and TAIAPI group 1Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, USA
2Division of Clinical Pathology, National Taiwan University Hospital Yun-Lin Branch, Yun-Lin, Taiwan
3Department of Internal Medicine, National Taiwan University Hospital and National Taiwan University, College of Medicine, Taipei, Taiwan
4Cleveland Clinic Lerner College of Medicine & Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, USA
5Department of Anesthesiology and Forensic Medicine, National Taiwan University Hospital, Taipei, Taiwan
Correspondence author:
Ming-Jiuh Wang, M.D. Ph.D.
Department of Anesthesiology and Forensic Medicine National Taiwan University Hospital
7 Chung-Shan South Road, Taipei, Taiwan Telephone: +886-2-23562082
Fax: +886-2-23934176 Email: [email protected]
Index Words: Primary aldosteronism, aldosterone-renin ratio, plasma aldosterone concentration, plasma renin activity, hypertension, captopril, losartan
Word count: Abstract-200; Text- 3371 Tables: 3; Figures: 4
# Taiwan Primary Aldosteronism Investigation (TAIPAI) Study Group: Vin-Cent Wu,
MD, Yen-Hung Lin, MD, Yi-Luwn Ho, MD, PhD, Hung-Wei Chang, MD, PhD, Lian-Yu Lin,MD, Fu-Chang Hu, MS, ScD, Kao-Lang Liu, MD, Shuo-Meng Wang, MD, Kuo-How Huang, MD, Yung-Ming Chen , MD, Chin-Chi Kuo, MD, Chin-Chen Chang, MD, Shih-Chieh Chueh, MD, PhD, Ching-Chu Lu, MD , Shih-Cheng Liao, MD, Ruoh-Fang Yen , MD, PhD, Wei-Chou Lin, MD, PhD, Bor-Sen Hsieh , MD, PhD and Kwan-Dun Wu, MD, PhD
Potential conflicts of interest. All authors: no conflicts.
Funding Acknowledgements: This research was supported in part by National Heart,
Lung, and Blood Institute training grant T32 HL7024-38, Ta-Tung Kidney Foundation, and the Taiwan National Science Council (grant NSC 96-2314-B-002-164, grant NSC 96-2314-B-002-033-MY3, and grant NSC 97-2314-B-002-155-MY2).
Abstract:
Objective
The diagnosis of primary aldosteronism (PA) among the older-aged population has posed a crucial challenge. Among patients over 50 years old, this trial assessed comparability of the performance of two PA diagnostic tests: losartan and captoril suppression tests.
Methods
A post-hoc subgroup analysis from a prospective cohort was conducted by TAIPAI (Taiwan Primary Aldosteornism Investigation) group between July 2003 and July 2006. Of the 160 patients in the cohort, 60 patients over 50 years received captopril and losartan tests to confirm PA.
Results:
Among the 60 patients over 50 years old, 31 patients had PA confirmed by
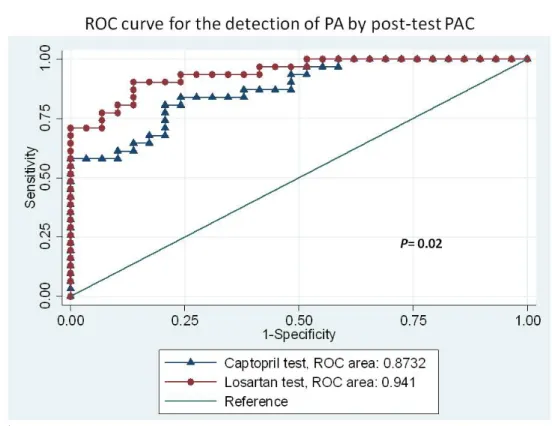
standardized protocol. The area under the receiver-operating characteristic (ROC) curve of the captopril aldosterone was significantly less than that of the post-losartan plasma aldosterone concentration (0.87 vs. 0.94, p = 0.02). Using ARR>35 with PAC>10 ng/dL, the specificity was 82.76% vs. 93.1% and the sensitivity was 77.42% vs. 87.10% for the captopril and losartan tests, respectively. The equivalence between the two tests were confirmed by exact McNemar test (p= 1.0).
Conclusion
“elderly-friendly” confirmatory test will be the first step to prepare the specific diagnostic model of PA for older-aged population.
Introduction:
As populations are aging worldwide, the global burden of hypertension has dramatically increased as the elderly persons have the highest prevalence of this disease.1-3. The unique characteristic of hypertension in the near-elderly and elderly is that secondary causes are more prevalent and different compared to the younger population.4, 5 Primary aldosteronism (PA) has long been considered a rare cause of hypertension in near-elderly and elderly.6 An increasing body of literature has demonstrated a greater prevalence of PA, about 10% in patients with increasing hypertension severity, presenting a growing concern.7 A long-standing of aldosterone excess has been proofed to induce arterial stiffness and endothelial injury8. PA is also related to kidney damage9, metabolic syndrome10, and left ventricular hypertrophy.11. Therefore, an accurate and safe diagnostic test for these populations is an
unaddressed clinical and epidemiological concern.
As the capacity to adjust excess fluid level is gradually declining in near-elderly and elderly, the oral sodium loading, saline infusion and fludrocortisone suppression tests may not be the first choice especially if patients also have been diagnosed with heart failure, advanced liver disease, and renal insufficiency. Consequently, the captopril challenge test may be the only suitable diagnostic test. Compared to the captopril test, the losartan test has demonstrated potentially better diagnostic
accuracy in general population while losartan also provides a better safety profile than captopril regarding the development of angioedema, a potentially
life-threatening event.12-14 In this post-hoc analysis, we aimed to verify the performance of the losartan test for PA in patients older than 50 years old. As PA becomes
increasingly prevalent in this specific age range, the safety issues and applicability of diagnostic tests would become a critical concern in this population.
Materials and Methods:
Patients: From July 2003 to January 2006, 64 patients older than 50 years old were
enrolled into the Taiwan Primary Aldosteronism Investigation (TAIPAI) database after follow-up screening at or referral to the National Taiwan University Hospital and its affiliated hospitals. Since this was a subgroup analysis from our previous published prospective cohort study investigating the diagnostic accuracy of losartan test,12 we carefully examined the study power according to the subgroup sample size. Based on the study sample size of 30 in each group with a 0.70 proportion of positive ratings, and 0.60 kappa, we have 90% power for a 2-sided test.15 The initial evaluation
included: 1) an age at onset of hypertension or hypokalemia of < 35 years; 2) difficult-to-control hypertension after therapy initiation; 3) the clinical occurrence of a
adrenal incidentaloma with hypertension or hypokalemia. Difficult-to-control hypertension was defined as patients taking more than three antihypertensive medications while their blood pressure still did not reach their therapeutic target16. Hypertensive crises are characterized by severely elevated blood pressure (BP), usually higher than 180/110 mmHg, along with progressive or impending target organ damage17. The ethnic composition of our cohort reflected a typical Taiwanese population18.
All antihypertensive medications were discontinued for at least 21 days before the study. Diltiazem and/or doxazosin were administered for control of marked high blood pressure when required.19 Medications that might interfere with the renin-aldosterone axis such as steroids, sex hormones, licorice, or non-steroidal anti-inflammatory drugs were also withheld for at least 6 weeks. All patients consumed a low-salt diet with 6 g of NaCL daily and were supplied with potassium during the testing period if hypokalemia was identified. The database was constructed for quality assurance in one medical center (National Taiwan University Hospital, Taipei, Taiwan) and its three branch hospitals in different cities (National Taiwan University Hospital Yun-Lin branch, Yun-Lin, southern Taiwan; En Chu Kong Hospital, Taipei County; and, Tao-Yuan General Hospital, Tao-Yuan, middle Taiwan). All patients with intention to confirm and requiring a suppression test or adrenal venous sampling
(AVS) were recruited and the data were prospectively collected. This post-hoc subgroup analysis from the previous prospective cohort study was approved by the Institutional Review Board of National Taiwan University Hospital(NTUH No.
9461700402).
Confirmation of primary aldosteronism: In this subcohort, a diagnosis of
pheochromocytoma was made in one patient, renal artery stenosis was diagnosed in one patient, and polycystic kidney disease was diagnosed in one patient. Only one patient who did not give his informed consent was excluded. The remaining 60 patients received both captopril and losartan tests (Figure 1). The two tests were performed on 2 consecutive days. As previously reported, the time-to-peak plasma concentration of losartan was proportional to the dose and was ~1.5 h with the 50 mg dose.20 With oral captopril, the time-to-peak was >0.5 h.21 In our previous head-to-head comparative study,12 we have set the sampling period at least one half-life of plasma renin activity (PRA) or plasma aldosterone concentration (PAC) because the biological half-life of aldosterone is ~30 min22 and the half-life of PRA is ~15 min.23. The patients were asked to sit for at least 10 minutes for the baseline blood samples at 9 am, and allowed to ambulate moderately until the second sampling. The second blood samples were obtained either 1 hour after the administration of 50 mg of captopril, or 2 hour after the administration of 50 mg of losartan12.
An ARR >35 with a PAC >10 ng/dL (>277 pmol/l) after the administration of captopril or losartan was defined as a positive test for PA. We constructed an ARR >35 (ngdL-1 per ngmL-1h-1) because this value had the best sensitivity and specificity to differentiate PA from EH in the TAIPAI database. Patients with both negative captopril and losartan suppression tests underwent a saline infusion test on a separate day to evaluate the autonomous secretion of aldosterone. After at least 1 hour in the supine position, two liters of 0.9% NaCl solution were administrated intravenously from 8:00 to 12:00 am, and blood samples for PRA and PAC were drawn before and at the end of the saline infusion. Patients in whom the PAC >10 ng/dl after saline infusion were diagnosed with PA in TAIPAI database.24
Differential Imaging studies: A computerized tomography (CT) of the adrenal glands
with a non-ionic iodinated contrast agent was done on all enrolled patients, with at least 3-mm contiguous slices in a normal surrounding. Although there were no strict measurements of normal adrenal size, CT imaging was considered abnormal when any volume thicker than 10 mm3 was detected. Those with inconclusive CT findings underwent dexamethasone suppression adrenocortical scintigraphy with CT (NP-59, I-131-6-beta-iodomethyl-19- norcholesterol & NP59-SPECT/CT).25 Bilateral adrenal venous sampling (AVS) was required if image studies were ambiguous. Successful venous cannulation was defined as the ratio of the cortisol level of the adrenal vein
to that of the inferior vena cava > 3. Lateralization of aldosterone secretion was defined by a greater than four-fold difference in the aldosterone/cortisol ratio between the two adrenal glands.24
Histopathological studies: All of the surgically removed adenomas were
re-evaluated by a histopathologist in the TAIPAI study group who was blinded to the clinical data. A histological diagnosis of aldosterone-producing adenomas (APA) was based on well-defined, encapsulated tumors predominantly consisting of foamy clear cells.26 Adenoma appeared as nodules of clear cells in sheets or nests that were sharply demarcated by a pseudo-capsule and compressed the non-neoplastic, uninvolved adrenal gland.27 Adenomas were differentiated from nodular adrenal hyperplasia by their solitary and well-circumscribed nature.27, 28 Adrenal glands from the idiopathic hyperaldosteronism (IHA) patients were marked by diffuse hyperplasia of cells resembling those of normal zona glomerulosa with or without macro- or micro-nodules.29
Measure of aldosterone and renin: The concentration of aldosterone was
measured by radioimmunoassay (RIA) using commercial kits (Aldosterone MAIA Kit, Biochem ImmunoSystems, Bologna, Italy) as previously described.30, 31 The detection limit was 10.0 pg mL-1 with a 90% confidence interval, with the normal range of 70– 350 pg mL-1 in an upright position. PRA was measured as the generation of
angiotensin I in vitro using a commercially available RIA kit (Incstar Corporation, Stillwater, Minnesota, US). Its normal range was 2.63 ± 1.32 ng mL-1h-1 with patient in an upright position. In our three centers over a period of 13 years, the same
aldosterone and renin assays were used.
Diagnostic criteria: Identification of APA in hypertensive patients required all of the
following “modified 4 corners score” criteria:12, 24, 32 1) evidence of autonomous excess aldosterone production based on an ARR > 35 ngdL-1 per ngmL-1h-1 and a PAC > 10 ng dL-1after any confirmatory test; (2) lateralization of aldosterone secretion at adrenal vein sampling or during dexamethasone suppression NP-59 SPECT/CT;25 (3) evidence of adenoma on a CT; and 4) pathologically proven adenoma after an adrenalectomy, and cure of hypertension without antihypertensive agents or improved hypertension, potassium, PAC, and PRA as described.32
IHA was established based on the following criteria:33 1) evidence of
autonomous excess aldosterone production based on an ARR > 35 ngdL-1 per ngmL-1h -1 and a PAC > 10 ng dL-1after any confirmatory test; 2) non-lateralization of
aldosterone secretion at adrenal vein sampling, or after undergoing dexamethasone suppression adreno-cortical scintigraphy;25 3) evidence of bilateral diffuse
enlargement on a CT; and 4) evidence of diffuse cell hyperplasia in the pathology studies. In patients with negative captopril and losartan tests, the pre-specified ARR <
35 ngdL-1 per ngmL-1h-1 and PAC < 25 ng dL-1, and negative salt-loading results were considered to be diagnostic of essential hypertension (EH).
Statistical analysis: The primary objective of the study was to compare the diagnostic
accuracy of the losartan test vs. the captopril test for PA in patients older than 50 years old. The data were provided as the mean values ± standard deviation (s.d.). As the data of PAC, PRA and calculated ARR were not normally distributed, median level with interquartile range were provided34.
Statistical analyses were performed using STATA version 12.0 statistical software (StataCorp LP, College Station, Texas). A normal distribution was attained by
appropriate transformations of skewed variables such as PAC and ARR. Comparisons of variables between PA and EH were based on t-test statistics. The κ-test was used to evaluate the agreement of defining PA between captopril and losartan suppression tests. The results were expressed as a kappa coefficients and were classified
according to the scale of Landis and Koch.35 The exact McNemar test was used to check the equality among captopril and losartan tests and the reference standard— the “modified 4 corners score” criteria. The sensitivity, specificity, accuracy, positive percent agreement and negative percent agreement for both losartan and captopril tests were calculated and compared by using receiver operating characteristic (ROC) curve. In addition, the age- and potassium- adjusted probabilities of having PA
according to the results of both suppression tests were also computed. The P-value equating significance was <0.05.
Results:
Demography of study population:Among 60 hypertensive patients who had
underwent the confirmatory TAIPAI protocol24 (31 women and 29 men; mean age, 60.9±7.5 years), 28 patients had positive captopril or losartan tests (Figure 1). Also, three patients with negative captopril and losartan tests were diagnosed based on a positive saline-loading test and abnormal imaging findings. Finally, 31 patients (16 women and 15 men; mean age, 57.9±5.3 years) had the diagnosis of PA, 20 patients were diagnosed with APA, and 11 patients were diagnosed with IHA. All of the EH patients had been affirmed by the negative saline infusion test. AVS was performed in total 12 patients with positive confirmatory tests (4 patients for initial negative CT imaging; 2 patients with bilateral adenoma; 1 for bilateral diffusely nodular adrenal gland on CT imaging; 5 patients with incompatible NP59-SPECT/CT and CT findings).
The demographics of PA patients and EH patients are shown in Table 1. EH patients tended to be older. There were no statistically significant differences in sex, BMI, systolic and diastolic blood pressures between the PA and EH groups. The basal levels of serum potassium (SK), PRA, PAC, and ARR were statistically significantly different between the PA and EH patients (all P < 0.05).
Changes of PAC and ARR after captopril and losartan suppression tests: In all
enrolled patients, the pretest PACs of the captopril and losartan tests were not statistically significantly different (34.5 ± 5.5 ng/dl vs. 29.8 ± 2.9 ng/dl, P = 0.34). However, the postcaptopril PAC was lower than the post-losartan PAC in PA patients (34.7 ± 4.9 ng/dl vs. 53.5 ± 8.2 ng/dl, P = 0.03). In EH patients, there was no
difference in the postcaptopril and postlosartan PAC (16.1 ± 2.0 ng/dl vs. 15.1 ± 2.0 ng/dl, P = 0.72). There was a statistically significant correlation between the
postcaptopril PAC and postlosartan PAC (r = 0.43, P = 0.0006) in all patients.
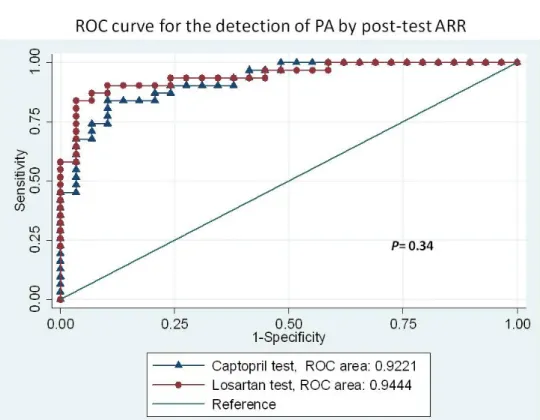
The performance of captopril and losartan tests on patients older than 50 years old with PA and EH: With the diagnostic criteria for PA based on an ARR >35 after captopril or losartan, the area under the ROC curve analyzed with the post-test ARR revealed no difference between the captopril and losartan tests after adjusted by age and serum potassium level (0.92 vs. 0.94, P = 0.34; Figure 2a). When the ROC curve was analyzed with the post-test PAC to differentiate PA from EH, the area under the curve of post-captopril PAC was inferior to that of post-losartan PAC adjusted by age and serum potassium (0.87 vs. 0.94, P = 0.02; Figure 2b). Using an ARR >35 with a PAC >10 ng/dl, the specificity was 82.76% vs. 93.1% and the sensitivity was 77.42% vs. 87.10% for the captopril test vs. the losartan test respectively. An accuracy of 80.0% for the diagnosis of PA from EH was achieved with the captopril test, with
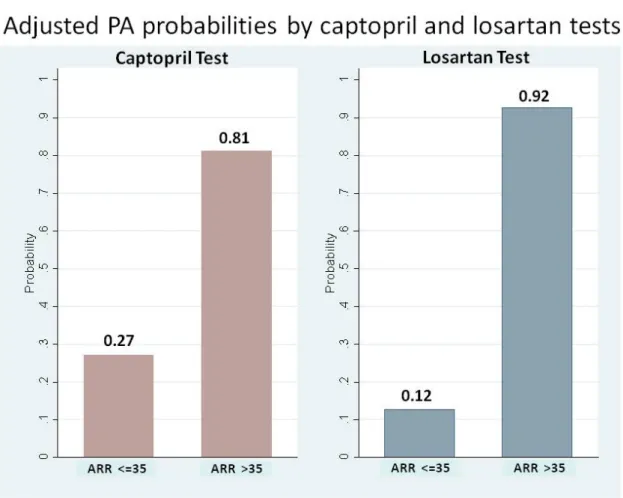
moderate agreement by the κ-test (k = 0.60, p<0.01) while the accuracy for losartan test was 90.0% and k =0.8 (p<0.01). The exact McNemar test comparing captopril and losartan tests revealed equivalence (p=1.00). The positive percent agreement was 82.8% and negative percent agreement was 83.9% between captopril and losartan tests (Table 2). The probability of having PA using post-test ARR cut-off 35 was 81% vs. 92% for the captopril test vs. the losartan test respectively (Figure 3).
Discussion:
This study verified the diagnostic value of losartan challenge test in near-elderly and elderly patients, a subpopulation of major interest in current global healthcare.36, 37 The losartan test was initially thought to be less diagnostically powerful but has been recently validated as a comparable test as captopril test in the general population by our previously published head-to-head study.12 The current nested case-cohort investigated the diagnostic accuracy of the losartan test in population over 50 years old. Since the pharmacodynamics/pharmacokinetic profiles are different among older-aged patients for ACEI, analyzing this subgroup provides additional clinical insight to previously published work. 12, 38, 39 In addition, our study has demonstrated a good agreement between captopril and losartan tests with kappa value of 0.67 (p<0.01).
over 50 years in contrast to current concept of PA regarding the prevalence of subtype.40 This “reversing” phenomenon reflects the multiple and intertwined problems of approaching PA in the near-elderly and elderly. First, the prevalence of PA in elder persons has rarely been the focus of contemporary literature, perhaps the most significant grey area in the management of hypertension on older-aged
patients. Second, the presence of clinical comorbidities poses noteworthy limitations to current PA diagnostic system such as adherence and tolerance to multi-step diagnostic tests. Finally, the cut-off value in many morbid subgroups remains
undetermined e.g. patients with end stage renal disease (ESRD) and congestive heart failure (CHF). All above-mentioned perspectives may lower the awareness of primary clinicians toward PA in daily practice with a blunt and insensitive approach.
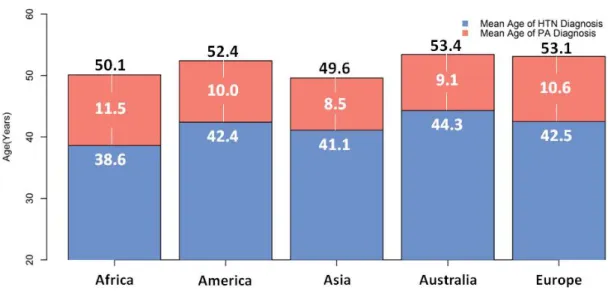
Although previously thought to be an extremely rare condition, PA now has been considered as one of the most common causes of secondary hypertension.41, 42 Also, a family history of early hypertension (<40 years40), indicating an increased pretest probability, has long been considered a triggering factor of the PA screening test.40, 43 However, the prevalence of PA may be stable across all age spectrum.4 Meanwhile, the average age at which PA was diagnosed in recent published studies from five continents is 52.1 years old, nearly the U.S. Census Bureau’s definition of “older” population(Table 3).44 The average hypertension duration is 10.1 years which
echoes the tendency of delayed diagnosis and the wastage of medical resources under current clinical practices (Table 3). Furthermore, the hypothetical PA onset age is approximately 41.8 years old (Table 3 & Figure 4). By updating the epidemiological profile, public awareness of PA in cases over 50 years old has the potential to
increase.
The call for adequate diagnostic testing of PA in near-elderly and elderly is still largely unaddressed as are the clinical practice guidelines for other more common diseases.45 Current three-step diagnostic system of PA greatly compromises the adherence among the elderly. Furthermore, multiple comorbid conditions often limit the selection of diagnostic tests. In patients with hypertensive pulmonary edema, congestive heart failure or kidney diseases that are vulnerable to fluid-overload, salt-loading and fludrocortisones tests are obviously inappropriate. Furthermore, to avoid possible angioedema from captopril in such a susceptible population,14 losartan test turns out to be a feasible choice. From the standpoints of safety and test adherence, conducting a large prospective study to verify losartan test in an ethnically diverse population would be fundamental to formulate a specific diagnostic model for patients over 50 years old.
In this post-hoc analysis restricting the sample to patients over 50 years old, the proportion of APA is significantly higher than IHA. Although this prevalence profile
might be affected by the selection criteria in our TAIPAI screening protocol,24 the curability of APA offers a cost-benefit opportunity to avoid unnecessary long-term anti-hypertensive medication. The accurate diagnosis of IHA also facilitates the use of effective target therapies such as spironolactone and eplerenon.46 And timely
diagnosis of PA in elder population may considerably lower the risk of long-term complications ranging from cardiovascular diseases4748, kidney damage9, to
metabolic syndrome49 related to aldosterone excess and consequently interrupt the vicious cycles of PA and coexisting organ damages.
The strength of our study is its prospective head-to-head design and that all patients underwent both captopril and losartan suppression tests. Moreover, the rigorous protocol based three-step investigation minimizes the possibilities of misclassification and ascertainment bias.24, 40
There are some limitations to the study. First, as a study investigating a
confirmatory test, larger numbers would offer a more accurate unbiased estimation on the sensitivity and specificity of the losartan test.50 The relatively small sample size may also mask the true difference due to insufficient statistical power. Yet the results seem promising since even with limited sample size the losartan test is comparable to captopril test as a useful confirmatory tool in hypertensive patients over 50 years. Second, a selection bias may be inherent in the selection criteria. Regarding the
proportion of subtypes of PA, the TAIPAI protocol employed hypokalemia as a selection criteria which may lead to selective inclusion of more severe form of PA, APA.51 Third, spectrum bias is an inevitable issue for studies conducted in tertiary medical centers, which may overestimate the performance of the diagnostic tests. This bias may be even more prominent for confirmatory tests due to the study population would have been highly selected after the screening protocol. However due to the head-to-head design, it is fair to compare both captopril and losartan tests and verify the “rule in” and “rule out” performances of the losartan test.52
Also, we are aware that confirmatory tests based on perturbation of the renin-angiotensin system will lead to exclude patients with Angiotensin II responsive APA53. Therefore, our finding may not be generalized to non-Angiotensin II autonomous APA. Finally, the target population restricted to Asian population in our study; therefore, the statistical inference toward other race/ethnicities needs to be further validated.
In summary, we found that the losartan test is comparable to captopril test in patients older than 50 years old. With comparable diagnostic accuracy, the losartan test has better safety profile compared to the captopril test which is an advantage to the case management for patients over 50 years old. We believe the verification of this “elderly-friendly” confirmatory test will be the first step to prepare the specific
diagnostic model of PA for near-elderly and elderly in contrast to current one-size-fits-all practice.
References:
1. Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. Jan 15-21 2005;365(9455):217-223.
2. Lloyd-Jones DM, Evans JC, Levy D. Hypertension in adults across the age spectrum: current outcomes and control in the community. JAMA. Jul 27 2005;294(4):466-472.
3. Wolf-Maier K, Cooper RS, Banegas JR, et al. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States.
JAMA. May 14 2003;289(18):2363-2369.
4. Anderson GH, Jr., Blakeman N, Streeten DH. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J
Hypertens. May 1994;12(5):609-615.
5. Dluhy RG. Uncommon forms of secondary hypertension in older patients. Am
J Hypertens. Mar 1998;11(3 Pt 2):52S-56S.
6. Aronow WS, Fleg JL, Pepine CJ, et al. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus documents developed in collaboration with the American Academy of Neurology, American Geriatrics Society, American Society for Preventive Cardiology, American Society of Hypertension, American Society of Nephrology,
Association of Black Cardiologists, and European Society of Hypertension. J
Am Coll Cardiol. May 17 2011;57(20):2037-2114.
7. Mosso L, Carvajal C, Gonzalez A, et al. Primary aldosteronism and hypertensive disease. Hypertension. Aug 2003;42(2):161-165.
8. Wu VC, Lo SC, Chen YL, et al. Endothelial progenitor cells in primary aldosteronism: a biomarker of severity for aldosterone vasculopathy and prognosis. J Clin Endocrinol Metab. Oct 2011;96(10):3175-3183.
9. Kuo CC, Wu VC, Tsai CW, Wu KD. Relative kidney hyperfiltration in primary aldosteronism: a meta-analysis. J Renin Angiotensin Aldosterone Syst. Jun 2011;12(2):113-122.
10. Fallo F, Veglio F, Bertello C, et al. Prevalence and characteristics of the metabolic syndrome in primary aldosteronism. J Clin Endocrinol Metab. Feb 2006;91(2):454-459.
11. Lin YH, Wang SM, Wu VC, et al. The association of serum potassium level with left ventricular mass in patients with primary aldosteronism. Eur J Clin Invest. Jul 2011;41(7):743-750.
12. Wu VC, Chang HW, Liu KL, et al. Primary Aldosteronism: Diagnostic Accuracy of the Losartan and Captopril Tests. Am J Hypertens. May 14 2009;22(8):821-827.
13. Matchar DB, McCrory DC, Orlando LA, et al. Systematic review: comparative effectiveness of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers for treating essential hypertension. Ann Intern Med. Jan 1 2008;148(1):16-29.
14. Sanchez-Borges M, Gonzalez-Aveledo LA. Angiotensin-converting enzyme inhibitors and angioedema. Allergy Asthma Immunol Res. Jul 2010;2(3):195-198.
15. Sim J, Wright CC. The kappa statistic in reliability studies: use, interpretation, and sample size requirements. Phys Ther. Mar 2005;85(3):257-268.
16. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. Jama. May 21 2003;289(19):2560-2572.
17. Vidt DG. Hypertensive crises: emergencies and urgencies. J Clin Hypertens
(Greenwich). Sep 2004;6(9):520-525.
18. Su TC, Hwang LC, You SL, Chen CJ. Ethnic variation in hypertension prevalence of women in Taiwan. J Hum Hypertens. Mar 2009;23(3):160-167.
19. Wu KD, Liao TS, Chen YM, et al. Preoperative diagnosis and localization of aldosterone-producing adenoma by adrenal venous sampling after administration of metoclopramide. J Formos Med Assoc. Sep 2001;100(9):598-603.
20. Munafo A, Christen Y, Nussberger J, et al. Drug concentration response relationships in normal volunteers after oral administration of losartan, an angiotensin II receptor antagonist. Clin Pharmacol Ther. May 1992;51(5):513-521.
21. Capoten, Captopril. Product Information. Princeton, NJ,: Bristol-Myers Squibb; 1996.
22. Tait JF, Tait SA, Little B, Laumas KR. The disappearance of 7-H-3-d-aldosterone in the plasma of normal subjects. J Clin Invest. Jan 1961;40:72-80.
23. Skrabal F. Half-life of plasma renin activity in normal subjects and in malignant hypertension. Klin Wochenschr. Dec 15 1974;52(24):1173-1174.
24. Kuo CC, Wu VC, Huang KH, et al. Verification and evaluation of aldosteronism demographics in the Taiwan Primary Aldosteronism Investigation Group (TAIPAI Group). J Renin Angiotensin Aldosterone Syst. Sep 2011;12(3):348-357.
SPECT/CT for primary aldosteronism patients with inconclusive adrenal venous sampling and CT results. J Nucl Med. Oct 2009;50(10):1631-1637.
26. Aiba M, Suzuki H, Kageyama K, et al. Spironolactone bodies in
aldosteronomas and in the attached adrenals. Enzyme histochemical study of 19 cases of primary aldosteronism and a case of aldosteronism due to
bilateral diffuse hyperplasia of the zona glomerulosa. Am J Pathol. Jun 1981;103(3):404-410.
27. Omura M, Sasano H, Fujiwara T, Yamaguchi K, Nishikawa T. Unique cases of unilateral hyperaldosteronemia due to multiple adrenocortical micronodules, which can only be detected by selective adrenal venous sampling.
Metabolism. Mar 2002;51(3):350-355.
28. Novitsky YW, Kercher KW, Rosen MJ, Cobb WS, Jyothinagaram S, Heniford BT. Clinical outcomes of laparoscopic adrenalectomy for lateralizing nodular hyperplasia. Surgery. Dec 2005;138(6):1009-1016; discussion 1016-1007.
29. Wu VC, Chueh SC, Chang HW, et al. Association of kidney function with residual hypertension after treatment of aldosterone-producing adenoma.
Am J Kidney Dis. Oct 2009;54(4):665-673.
30. Chang HW, Chu TS, Huang HY, et al. Down-regulation of D2 dopamine receptor and increased protein kinase Cmu phosphorylation in aldosterone-producing adenoma play roles in aldosterone overproduction. J Clin
Endocrinol Metab. May 2007;92(5):1863-1870.
31. Loh KC, Koay ES, Khaw MC, Emmanuel SC, Young WF, Jr. Prevalence of primary aldosteronism among Asian hypertensive patients in Singapore. J Clin
Endocrinol Metab. Aug 2000;85(8):2854-2859.
32. Rossi GP, Belfiore A, Bernini G, et al. Comparison of the captopril and the saline infusion test for excluding aldosterone-producing adenoma.
Hypertension. Aug 2007;50(2):424-431.
33. Wu VC, Chueh SC, Chang HW, et al. Bilateral aldosterone-producing adenomas: differentiation from bilateral adrenal hyperplasia. Qjm. Jan 2008;101(1):13-22.
34. Weinberger MH, Fineberg NS. The diagnosis of primary aldosteronism and separation of two major subtypes. Arch Intern Med. Sep 27
1993;153(18):2125-2129.
35. Cohen J. Weighted kappa: nominal scale agreement with provision for scaled disagreement or partial credit. Psychol Bull. Oct 1968;70(4):213-220.
36. Eyre H, Kahn R, Robertson RM, et al. Preventing cancer, cardiovascular disease, and diabetes: a common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association.
Circulation. Jun 29 2004;109(25):3244-3255.
37. Renehan AG, Howell A. Preventing cancer, cardiovascular disease, and diabetes. Lancet. Apr 23-29 2005;365(9469):1449-1451.
38. Chobanian AV. The use of angiotensin converting enzyme inhibitors in elderly patients with hypertension. J Am Geriatr Soc. Mar 1987;35(3):269-270.
39. Reid JL. Angiotensin converting enzyme inhibitors in the elderly. Br Med J
(Clin Res Ed). Oct 17 1987;295(6604):943-944.
40. Funder JW, Carey RM, Fardella C, et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. Sep 2008;93(9):3266-3281.
41. Aronow WS, Fleg JL, Pepine CJ, et al. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents.
Circulation. May 31 2011;123(21):2434-2506.
42. Mattsson C, Young WF, Jr. Primary aldosteronism: diagnostic and treatment strategies. Nat Clin Pract Nephrol. Apr 2006;2(4):198-208; quiz, 191 p following 230.
43. Rossi GP. A comprehensive review of the clinical aspects of primary aldosteronism. Nat Rev Endocrinol. 2011;7(8):485-495.
44. U.S.Census.Bureau. Age Data of the United States. In: U.S. Census Bureau PD, ed; 2011.
45. Boyd CM, Darer J, Boult C, Fried LP, Boult L, Wu AW. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance. JAMA. Aug 10
2005;294(6):716-724.
46. Karagiannis A, Tziomalos K, Papageorgiou A, et al. Spironolactone versus eplerenone for the treatment of idiopathic hyperaldosteronism. Expert Opin
Pharmacother. Mar 2008;9(4):509-515.
47. Catena C, Colussi G, Nadalini E, et al. Cardiovascular outcomes in patients with primary aldosteronism after treatment. Arch Intern Med. Jan 14 2008;168(1):80-85.
48. Lin YH, Wu XM, Lee HH, et al. Adrenalectomy reverses myocardial fibrosis in patients with primary aldosteronism. J Hypertens. Aug 2012;30(8):1606-1613.
49. Fallo F, Pilon C, Urbanet R. Primary Aldosteronism and Metabolic Syndrome.
Horm Metab Res. Nov 24 2011.
50. Dendukuri N, Joseph L. Bayesian approaches to modeling the conditional dependence between multiple diagnostic tests. Biometrics. Mar
51. Blumenfeld JD, Sealey JE, Schlussel Y, et al. Diagnosis and treatment of primary hyperaldosteronism. Ann Intern Med. Dec 1 1994;121(11):877-885.
52. Ransohoff DF, Feinstein AR. Problems of spectrum and bias in evaluating the efficacy of diagnostic tests. N Engl J Med. Oct 26 1978;299(17):926-930.
53. Gordon RD, Hamlet SM, Tunny TJ, Klemm SA. Aldosterone-producing adenomas responsive to angiotensin pose problems in diagnosis. Clin Exp
Pharmacol Physiol. Mar 1987;14(3):175-179.
54. Rayner BL, Opie LH, Davidson JS. The aldosterone/renin ratio as a screening test for primary aldosteronism. S Afr Med J. Apr 2000;90(4):394-400.
55. Williams JS, Williams GH, Raji A, et al. Prevalence of primary
hyperaldosteronism in mild to moderate hypertension without hypokalaemia.
J Hum Hypertens. Feb 2006;20(2):129-136.
56. Umpierrez GE, Cantey P, Smiley D, et al. Primary aldosteronism in diabetic subjects with resistant hypertension. Diabetes Care. Jul 2007;30(7):1699-1703.
57. Murashima M, Trerotola SO, Fraker DL, Han D, Townsend RR, Cohen DL. Adrenal venous sampling for primary aldosteronism and clinical outcomes after unilateral adrenalectomy: a single-center experience. J Clin Hypertens
(Greenwich). Jun 2009;11(6):316-323.
58. Stehr CB, Mellado R, Ocaranza MP, et al. Increased levels of oxidative stress, subclinical inflammation, and myocardial fibrosis markers in primary
aldosteronism patients. J Hypertens. Oct 2010;28(10):2120-2126.
59. Horita Y, Inenaga T, Nakahama H, et al. Cause of residual hypertension after adrenalectomy in patients with primary aldosteronism. Am J Kidney Dis. May 2001;37(5):884-889.
60. Benchetrit S, Bernheim J, Podjarny E. Normokalemic hyperaldosteronism in patients with resistant hypertension. Isr Med Assoc J. Jan 2002;4(1):17-20.
61. Fukudome Y, Fujii K, Arima H, et al. Discriminating factors for recurrent hypertension in patients with primary aldosteronism after adrenalectomy.
Hypertens Res. Jan 2002;25(1):11-18.
62. Takakuwa H, Shimizu K, Izumiya Y, et al. Dietary sodium restriction restores nocturnal reduction of blood pressure in patients with primary aldosteronism.
Hypertens Res. Sep 2002;25(5):737-742.
63. Matsumura K, Fujii K, Oniki H, Oka M, Iida M. Role of aldosterone in left ventricular hypertrophy in hypertension. Am J Hypertens. Jan 2006;19(1):13-18.
64. Satoh F, Abe T, Tanemoto M, et al. Localization of aldosterone-producing adrenocortical adenomas: significance of adrenal venous sampling. Hypertens
Res. Nov 2007;30(11):1083-1095.
65. Kim RM, Lee J, Soh EY. Predictors of resolution of hypertension after adrenalectomy in patients with aldosterone-producing adenoma. J Korean
Med Sci. Jul 2010;25(7):1041-1044.
66. Mukherjee JJ, Khoo CM, Thai AC, Chionh SB, Pin L, Lee KO. Type 2 diabetic patients with resistant hypertension should be screened for primary aldosteronism. Diab Vasc Dis Res. Jan 2010;7(1):6-13.
67. Nakajima Y, Yamada M, Taguchi R, et al. Cardiovascular complications of patients with aldosteronism associated with autonomous cortisol secretion. J
Clin Endocrinol Metab. Aug 2011;96(8):2512-2518.
68. Sukor N, Gordon RD, Ku YK, Jones M, Stowasser M. Role of unilateral adrenalectomy in bilateral primary aldosteronism: a 22-year single center experience. J Clin Endocrinol Metab. Jul 2009;94(7):2437-2445.
69. Pimenta E, Gordon RD, Ahmed AH, et al. Cardiac dimensions are largely determined by dietary salt in patients with primary aldosteronism: results of a case-control study. J Clin Endocrinol Metab. Sep 2011;96(9):2813-2820.
70. Rossi E, Regolisti G, Negro A, Sani C, Davoli S, Perazzoli F. High prevalence of primary aldosteronism using postcaptopril plasma aldosterone to renin ratio as a screening test among Italian hypertensives. Am J Hypertens. Oct
2002;15(10 Pt 1):896-902.
71. Enberg U, Volpe C, Hoog A, et al. Postoperative differentiation between unilateral adrenal adenoma and bilateral adrenal hyperplasia in primary aldosteronism by mRNA expression of the gene CYP11B2. Eur J Endocrinol. Jul 2004;151(1):73-85.
72. Juutilainen AM, Voutilainen ET, Mykkanen L, Niskanen L. Plasma aldosterone to renin ratio predicts treatment response in primary aldosteronism: is volume loading needed? Blood Press. 2005;14(4):245-250.
73. Lumachi F, Ermani M, Basso SM, Armanini D, Iacobone M, Favia G. Long-term results of adrenalectomy in patients with aldosterone-producing adenomas: multivariate analysis of factors affecting unresolved hypertension and review of the literature. Am Surg. Oct 2005;71(10):864-869.
74. Ribstein J, Du Cailar G, Fesler P, Mimran A. Relative glomerular hyperfiltration in primary aldosteronism. J Am Soc Nephrol. May 2005;16(5):1320-1325.
75. Sechi LA, Novello M, Lapenna R, et al. Long-term renal outcomes in patients with primary aldosteronism. JAMA. Jun 14 2006;295(22):2638-2645.
76. Zacharieva S, Orbetzova M, Elenkova A, et al. Diurnal blood pressure pattern in patients with primary aldosteronism. J Endocrinol Invest. Jan
77. Fogari R, Preti P, Zoppi A, Rinaldi A, Fogari E, Mugellini A. Prevalence of primary aldosteronism among unselected hypertensive patients: a
prospective study based on the use of an aldosterone/renin ratio above 25 as a screening test. Hypertens Res. Feb 2007;30(2):111-117.
78. Giacchetti G, Ronconi V, Turchi F, et al. Aldosterone as a key mediator of the cardiometabolic syndrome in primary aldosteronism: an observational study.
J Hypertens. Jan 2007;25(1):177-186.
79. Bernini G, Galetta F, Franzoni F, et al. Arterial stiffness, intima-media thickness and carotid artery fibrosis in patients with primary aldosteronism. J
Hypertens. Dec 2008;26(12):2399-2405.
80. Mourad JJ, Girerd X, Milliez P, Lopez-Sublet M, Lejeune S, Safar ME. Urinary aldosterone-to-active-renin ratio: a useful tool for predicting resolution of hypertension after adrenalectomy in patients with aldosterone-producing adenomas. Am J Hypertens. Jul 2008;21(7):742-747.
81. Matrozova J, Steichen O, Amar L, Zacharieva S, Jeunemaitre X, Plouin PF. Fasting plasma glucose and serum lipids in patients with primary
aldosteronism: a controlled cross-sectional study. Hypertension. Apr 2009;53(4):605-610.
82. Reincke M, Rump LC, Quinkler M, et al. Risk factors associated with a low glomerular filtration rate in primary aldosteronism. J Clin Endocrinol Metab. Mar 2009;94(3):869-875.
83. Somloova Z, Widimsky J, Jr., Rosa J, et al. The prevalence of metabolic
syndrome and its components in two main types of primary aldosteronism. J
Figure and Legends:
Figure 1. Study flow diagram. The diagnosis of primary aldosteronism is based on
Taiwan Primary Aldosteronism Investigation Group (TAIPAI) protocols.24
Aldosterone–renin ratio >35 after administration of captopril or losartan indicated a positive result. A plasma aldosterone concentration >10 ng/dl after saline infusion is positive for the test (see text). APA, aldosterone-producing adenoma; EH, essential hypertension; IHA, idiopathic hyperaldosteronism.
Figure 2. Receiver-operating characteristic (ROC) curves for the detection of all
primary aldosteronism by (a)post-test PAC, and (b) post-test ARR. PAC, plasma aldosterone concentration; ARR, aldosterone-renin ratio.
(a)
post-losartan ARR at the cut-off value of 35 ng/dl per ng/ml/h. ARR, aldosterone-renin ratio.
Figure 4. The mean PA age at diagnosis and hypertension duration summarized from recent PA studies between January 2000 and July 2012 in five continents. The
number in each red bar indicates the mean duration of hypertension.
Table 1. Main Demographic and biochemical characteristics of the study patients
PA (n=31) EH (n=29) p value
Sex, male(%) 15 (48.4) 14 (48.3) 0.99 SBP, mmHg 156.1 (22.5) 163.7 (17.6) 0.16 DBP, mmHg 93.5 (13.1) 89.6 (13.9) 0.29 BMI, kg/m2 25.6 (2.8) 26.2 (3.7) 0.55 Creatinine, mg/dL 1.1 (0.3) 1.2 (0.4) 0.28 Potassium, mmol/L 3.5 (0.8) 4.3 (0.6) < 0.001 Captopril test PAC (ng/dL) 25.3 (16.4-46.8) 14.1 (9.8-18.4) < 0.001 PRA (ng/ml/h) 0.2 (0.06-0.5) 3.2 (0.7-6.3) < 0.001 ARR 225.6 (52.1-950) 4.9 (1.9-10.9) < 0.003 Losartan test PAC (ng/dL) 39.8 (20.6-57.5) 12.2 (9.8-18.2) < 0.001 PRA (ng/ml/h) 0.3 (0.1-0.5) 2.8 (1.0-4.7) 0.006 ARR 144.6 (41.1-545) 7.2 (3.3-12.0) 0.001
Data as the mean values ± standard deviation (SD) except for PAC, PRA, and ARR which were presented as median with interquartile range.
Abbreviations: APA, aldosterone-producing adenoma; ARR, aldosterone–renin ratio
(ng/dl per ng/ml/h); BMI, body mass index; DBP, diastolic blood pressure; EH, essential hypertension; IHA, idiopathic hyperaldosteronism; MBP, mean blood pressure; NS, not significant; PAC, plasma aldosterone concentration; PRA, plasma renin activity; SBP, systolic blood pressure.
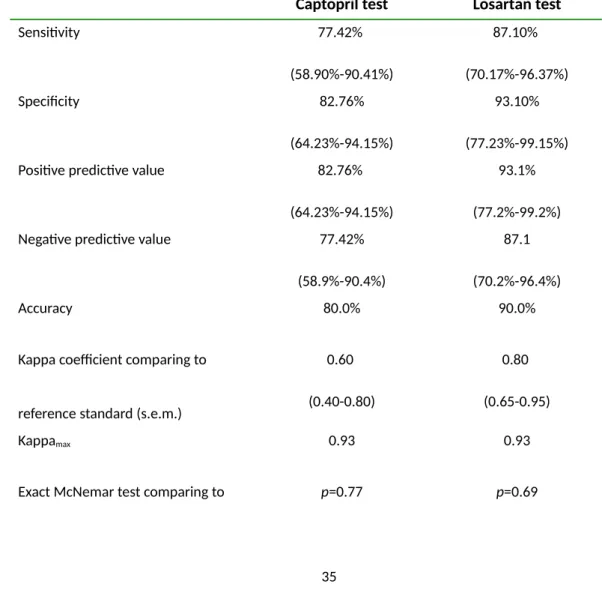
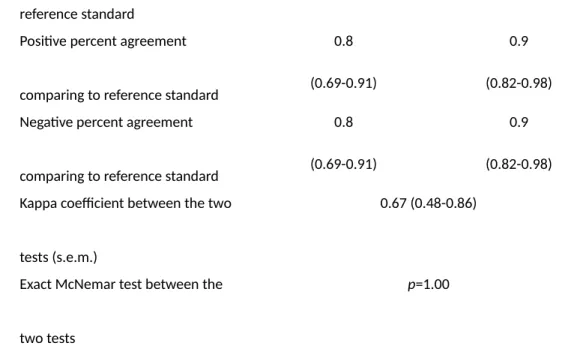
Table 2. Comparison of diagnostic performances between losartan and captopril
tests.
Captopril test Losartan test
Sensitivity 77.42% (58.90%-90.41%) 87.10% (70.17%-96.37%) Specificity 82.76% (64.23%-94.15%) 93.10% (77.23%-99.15%) Positive predictive value 82.76%
(64.23%-94.15%)
93.1% (77.2%-99.2%) Negative predictive value 77.42%
(58.9%-90.4%)
87.1 (70.2%-96.4%)
Accuracy 80.0% 90.0%
Kappa coefficient comparing to
reference standard (s.e.m.)
0.60 (0.40-0.80)
0.80 (0.65-0.95)
Kappamax 0.93 0.93
reference standard
Positive percent agreement
comparing to reference standard
0.8 (0.69-0.91)
0.9 (0.82-0.98) Negative percent agreement
comparing to reference standard
0.8 (0.69-0.91)
0.9 (0.82-0.98) Kappa coefficient between the two
tests (s.e.m.)
0.67 (0.48-0.86)
Exact McNemar test between the
two tests
p=1.00
Table 3. Recent studies (study population more than 10 patients) of primary
duration of hypertension including primary care and referral settings published between January 1, 2000 and July 4, 2012 from two electronic databases, MEDLINE and EMBASE.
The key words “primary aldosteronism” or “hyperaldosteronism” were used and two reviewers (C.C. Kuo and V.C. Wu) independently screened the titles, abstracts, and contents to identify potentially eligible studies and to avoid the duplication by collate authors’ name and affiliation to minimize the possibility of extracting repeat data from the same study group.
Continents Number of PA patients Mean Age of PA at diagnosis, years Mean (SD) Mean Duration of HTN, years Mean (SD) Country Author Reference, Year
Africa Rayner54, 2000 69 50.1(12.6) 11.5(9.8) South Africa America Williams55, 2006 11 49.5 (6.3) 9.6 (6.6) United States Umpierrez56, 2007 14 57(6) 15(7) United States Murashima57, 2009 56 50.6 (10.0) 13.0 (9.4) (n=45) United States Stehr58, 2010 30 54.6(10.4) 3.2(1.8) Chile
Continental Summary 111 52.4 (9.6) 10.0 (8.5) (n=100) --Asia Loh31, 2000 16 50.6(11.3) 8.6 (6.9) Singapore Horita59, 2001, 25 45.4 (11.2) 5.1 (4.6) Japan Benchetrit60, 2002 20 56(8.9) 12(8.9) Israel Fukudome61, 2002 46 44(6.8) 7(5.4) Japan Takakuwa62, 2002 13 38.9(6.2) 5.4 (3.8) Japan Matsumura63, 2006 25 47.2(11) 7.6(6.0) Japan Satoh64, 2007 87 52.4(12.1) 12.9(19.6) Japan Kim65, 2010 27 45(4) 5.6(7.9) Korea Mukherjee66, 2010 13 60.2 (7.9) 16.2(10.8) Singapore Kuo9, 2011 346 48.6 (11.8) 7.2(7.2) Taiwan Nakajima67, 2011 76 53.9 (10.7) 11 (8.4) Japan Continental Summary 694 49.6 (11.6) 8.5 (10.0) --Australia Sukor68, 2009 40 52.2(9.5) 10.6(10.1) Australia Pimenta69, 2011 21 55.8(7.7) 6.1(5.5) Australia Continental Summary 61 53.4 (9.0) 9.1 (9.0) --Europe Rossi70, 2002 66 54.6(10.8) 5(4.9) Italy Enberg71,2004 27 49.3 (13.3) 7.5 (6.0) Sweden Juutilainen72, 2005 38 55(12.3) 11(6.2) Finland Lumachi73, 2005 98 47.7 (10.1) 4.4(1.7) Italy Ribstein74, 2005 25 49(10) 9(5) France Fallo10, 2006 85 55(9) 12.3(9.3) Italy Sechi75, 2006 50 53(12) 10(6) Italy Zacharieva76, 2006 64 46.2 (11.7) 9.7 (12.2) Bulgaria Fogari77, 2007 177 48(7) 9.3 (3.6) Italy Giacchetti78, 2007 61 51(10.5)) 8.8(6.3) Italy Bernini79, 2008 23 54.0(12.0) 7.5(6.7) Italy Mourad80, 2008 48 52(11) 11.4(1.1) France Matrozova81, 2009 460 51.9 (5.5) 12.3 (5.6) (n=438) France Reincke82, 2009 408 60(10) 12(9) Germany
Continental Summary 1730 53.1 (10.0) 10.6 (7.3)
(n=1708)
--Overall Five Continents
Overall Summary 2665 52.1 (10.6) 10.1 (8.3)
(n=2632)
Hypothetical mean age of PA onset = the average of the five continents’ (mean age of PA at diagnosis –
mean duration of hypertension) = 41.8 years PA, primary aldosteronism; HTN, hypertension