PSYCHOSOCIAL AND BIOLOGICAL FACTORS ASSOCIATED
WITH GLYCEMIC CONTROL FOR PATIENTS WITH TYPE 2
DIABETES: AN APPLICATION OF STRUCTURAL EQUATION
MODELING ANALYSIS
HUI-CHING WENG
Department of Health Management, I-Shou University
CHAO-MING HUNG
Department of General Surgery, E-Da Hospital Department of Medical Nutrition, I-Shou University
SHU-CHING CHI
Department of Nursing, E-Da Hospital
ABSTRACT
The purpose of this study is to identify the psychosocial and biologic factors associated with the effectiveness of glycemic control in a type 2 diabetes management program. The study group was comprised of 285 patients with type 2 diabetes mellitus who were enrolled for 12 months in the National Diabetes Pay-by-Quality Program. Structural equation modeling analysis was employed to determine the importance of various parameters to the effectiveness of glycemic control. The results showed that effectiveness of glycemic control was significantly associated with gender, number of complications, locus of control, stages of change and previous status of glycemic control. The final model proved to be valid (χ2
= 32.18, df = 29, p = .31), showing a sound fit (AGFI = 0.96 and RMSEA = 0.018). The model explained 49% of the variance of metabolic control at glycemic control. The findings obtained in this study offer an insight into the complexity of patient behavior in diabetes management. Health system specialists must understand the dilemmas of type 2 diabetic patients and their clinicians well as the limitations to successful treatments before expending substantial resources on
34 Pan-Pacific Management Review January
disease management.
Keywords: glycemic control, diabetes, depression, stage of change, structural equation modeling
INTRODUCTION
Since the 1980s, a variety of studies designed to supplement medical management and empower patients through educational or psychological interventions have been performed. Published studies reveal the benefits of disease management and self-education for T2DM patients. Unfortunately, a wide gap still exists between current and desired diabetes care and practices. Recent meta-analyses reveal that the difference of the mean for reduction in percent glycated hemoglobin between intervention and control groups is less than 1% with statistical insignificance (Ismail, Winkley, & Rabe-Hesketh, 2004; Glasgow, Goldstein, Ockene, & Pronk, 2004). Whether the improvement in glycemic control of less than 1% at immediate follow-up (often <= 6 months) is clinically significant remains doubtful. Therefore, the true clinical efficacy of disease management or diabetes self-education programs in treatment of patients with T2DM remains controversial and findings are considered inconclusive. Accordingly, a clear rationale exists to identify factors that associate with or determine the effectiveness of glycemic control in disease management programs for patients with T2DM. Identification of such factors should prove beneficial for designing interventions that will be effective in sustaining glycemic control.
To date, many program evaluations indicate that methodological issues and institutional factors influence the execution of intervention programs and that the processing and mediating of variables associated with patient adherence to glycemic control merit more attention (Peterson & Hughes, 2002). While the relationships between these variables are usually examined singly in current studies, the present study attempted to include as many of the above-mentioned factors simultaneously to provide an overall picture of treatment conditions for T2DM patients. The goal of the present study was to assess the relationships among patient demographic characteristics, biological variables, psychosocial factors and long-term effects of glycemic control for T2DM patients who participated in a disease management program. Demographic, clinical and psychosocial factors are recognized to influence glycemic control
for T2DM patients (Rose, Fliege, Hildebrandt, Schirop, & Klapp, 2002; Glasgow, 1995; Alberti & Gray, 1998; Lockington, Meadows, & Wise, 1987; Beck & Beamesderfer, 1974; Sutton, 2000; Davis, Cull, Holman, & UK Prospective Diabetes Study (UKPDS) Group, 2001). Based on previous studies, Glasgow’s (2004) models of diabetes education were employed and the assumption made that glycemic control in T2DM is influenced by a network of interacting forces (Figure 1). To keep the analysis within manageable boundaries, focus was placed solely on patient factors whereas factors associated with healthcare providers, institutions or social backgrounds were not examined. Hypothesized model was shown in figure 1. First, patients’ sex, educational levels and income would have effects on knowledge about HbA1c control. Second, patients’ knowledge would have effects on their attitude, stage of changes and HbA1c control. Third, patient income would have effect on patient depression, stage and HbA1c control. Sex Education Income Knowledge Attitude Depression Stage HbA1c Basaline 6 mo 12 mo
FIGURE 1 Hypothesized model concerning a network of psychosocial determinants for glycemic control in patients with type 2 diabetes
METHOD
SampleThe study group was comprised of 285 T2DM patients enrolled in a disease management program at the Diabetic Clinic of PingTung Christian Hospital under the guidance of the
36 Pan-Pacific Management Review January
National Health Bureau of Taiwan. Patients who enrolled in the program and agreed to complete the survey underwent a comprehensive assessment of complications and risk factors based on the guidelines of National Cholesterol Education Program (NCEP) and the American Diabetes Association (ADA) statement recommendations for clinical treatment and targeting of control of diabetes. A diabetes educator provided scheduled orientations for diabetic self-management education, and consultations with a dietitian were also scheduled. The case manager (usually a registered nurse) took an active role in case management for both patient guidance and coordination of collective care. The disease management program was implemented in 3 stages as follows: (1) enrollment and initial encounter, (2) intervention and patient education, and (3) follow-up visits.
The diagnosis of T2DM was based upon the WHO criteria (Alberti & Gray, 1998). Three patients presenting with symptoms suggestive of type 1 diabetes, defined as diabetic ketoacidosis, acute presentation with heavy (3+) ketonuria, or requirement for continuous insulin therapy within 1 year of diagnosis were excluded. Patients who enrolled this program less than one year were also excluded. Fourteen patients (4.9%) declined to participate because of distance or time limitations or family concerns. Each patient was asked to complete a questionnaire which included personal demographic information and information regarding disease history. This study was approved by the Human Research Ethics Committee of Pingtung Hospital, and informed consent was obtained from each patient.
Biomedical Data
All patients underwent complete physical examinations, and routine biochemical analyses of blood and urine as well assessments of the presence and extent of macrovascular or microvascular diabetic complications were performed. Glycemic control was assessed by a latent variable which was composite of HbA1c measured at baseline, 6-moth and 12-month follow-up.
Social-psychological Data
questionnaire. This questionnaire was then employed to evaluate factors including socioeconomic status, knowledge, depression and stage of change. Questionnaires were checked for proper completion and plausibility. Patient knowledge of diabetes was assessed through a questionnaire designed by the Taiwanese Association of Diabetes Educators (1998) and which included questions regarding causes of diabetes, glycemic control and therapy, diet, exercise, and complications. The questionnaire consists of 21 questions with three possible dichotomized answers (yes/no/unknown). A correct answer receives a score of one point such that possible total scores range between 0 and 21. The attitudinal scale concerning diabetes was averaged to form from seven items out of a 31-item attitude scale developed by Lockington, Meadows, and Wise (1987) (on a 5-point scale (1 = strongly disagree to 5 = strongly agree). Cronbach’s alpha for attitude was .78. Depression score was measured by use of the Beck Depression Inventory (BDI). The BDI yields a reliability of 0.83 and has also been shown to have high validity. Stage was assigned according to Peterson et al (Beck & Beamesderfer, 1974). and involved the following 5 statements of “willingness to change”: 1) pre-contemplation stage (“No, and I do not intend to make changes in my diabetes management.”); 2) contemplation stage (“Yes, and I intend to make changes in my diabetes management in the next 6 months.”); 3) preparation stage (“Yes, and I intend to make changes in my diabetes management in the next 30 days.”); 4) action stage (“Yes, and I have made changes in my diabetes management in the last 6 months.”); and 5) maintenance stage (“Yes, and my diabetes has been well-controlled for more than 6 months.”)
Statistical Analysis
Relationships between the glycemic control outcome and anthropometric, biochemical, and psychosocial parameters were examined using Pearson correlation coefficients with two-tailed tests of significance. A p value < 0.05 was considered significant. A structural equation model (SEM) was used for the analysis of factors associated with the glycated hemoglobin outcome upon completion of the 12-month diabetes disease management program. In essence, SEM combines the techniques of multiple regression analysis and path analysis, thereby allowing relationships among many variables to be tested simultaneously (Jöreskog,
38 Pan-Pacific Management Review January
Sörbom, & du Toitl, 2000). All statistical analyses were performed using the Statistical Package for Social Science (SPSS 13). Structural equation modeling of variables was undertaken using the LISREL 8.71. The results of confirmatory factor analysis proved to be valid (χ2
= 32.18, df = 29, p = .31), revealing a sound fit (AGFI = 0.96 and RMSEA = 0.018). Given that many variables are included in the conceptual model, a preliminary zero-order correlation analysis was conducted to eliminate certain of the unrelated variables and thereby assure that the final model was parsimonious.
RESULTS
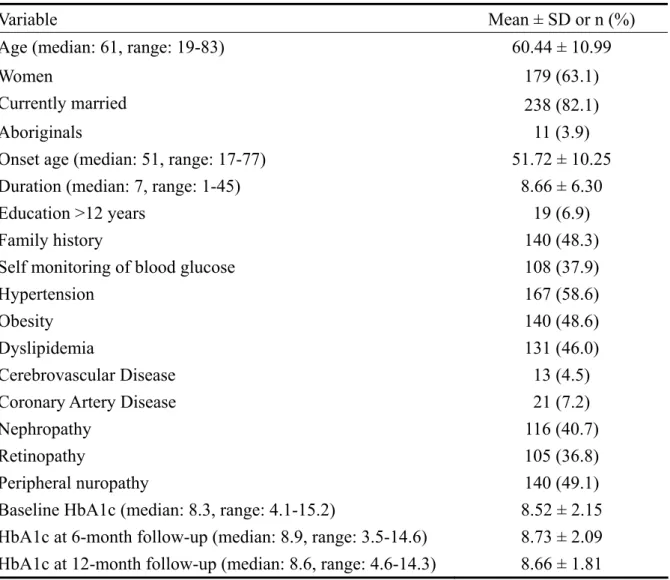
Patient demographic and biological variables are given in Table 1, with data presented as the mean SD or number (%). The mean age of subjects was 60.4 years and the mean age of onset of diabetes was 51.7 years. The majority of the subjects were women (63.1%), and most subjects (82.1%) were currently married. The duration of diabetes was 8.7 ± 6.3 years. The mean value for baseline percent HbA1c, 6-month follow-up and 12-month follow-up were 8.5 ± 2.1, 8.73, and 8.66 respectively. The results of repeated analysis of variance show that there was no significant difference of the percent HbA1c values across 12-month period.
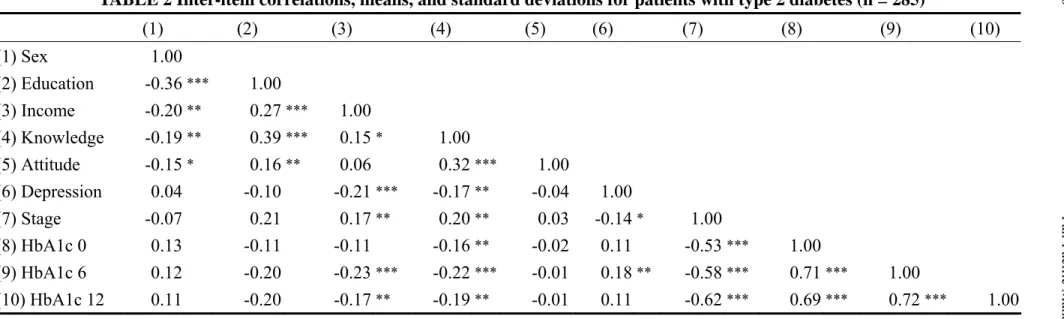
The zero-order correlation matrix of the nine variables related to HbA1c measured at baseline, 6-moth and 12-month follow-up is shown in Table 2. Higher HbA1c 12 was significantly associated with lower educational level, lower income, higher depression scores, stronger internal locus of control, stronger external locus of control, lower level of TTM stage and higher HbA1c. Significant correlation identified a subset of psychosocial factors that were therefore reanalyzed using SEM with statistical controls for the effects of demographic factors.
The model explained 49% of the variance of HbA1c. As shown in Figure 1, knowledge (γ = -.11, p <.05) and stage of change (β = -.54, p <.001) have direct effects on HbA1c. Female (γ = -.07, p <.10) and more educated patients (γ =.37, p <.001) are more likely to have more knowledge regarding T2DM management. Also, patient with more income (γ =.13, p <.01) and more knowledge (γ = .27, p <.001) tend to have more advanced stage of changes. In other words, these patients tend to have more intent and stronger motivation for behavioral changes. Attitude and depression also have some effects on HbA1c, but not at significant level. The
present study indicates that patients’ sex, education, income, knowledge and stage of changes have either direct or indirect effects through two major mediating variables (i.e., knowledge and stage of changes) on glycemic control. The amounts of variance explained for knowledge, attitude, depression, stage of change and HbA1c were 22%, 13%, 7%, 7% and 49%, respectively.
TABLE 1 Baseline characteristics of subjects (n = 285)
Variable Mean ± SD or n (%)
Age (median: 61, range: 19-83) 60.44 ± 10.99
179 (63.1) Women
Currently married 238 (82.1)
Aboriginals 11 (3.9)
Onset age (median: 51, range: 17-77) 51.72 ± 10.25
Duration (median: 7, range: 1-45) 8.66 ± 6.30
Education >12 years 19 (6.9)
Family history 140 (48.3)
Self monitoring of blood glucose 108 (37.9)
Hypertension 167 (58.6)
Obesity 140 (48.6)
Dyslipidemia 131 (46.0)
Cerebrovascular Disease 13 (4.5)
Coronary Artery Disease 21 (7.2)
Nephropathy 116 (40.7)
Retinopathy 105 (36.8)
Peripheral nuropathy 140 (49.1)
Baseline HbA1c (median: 8.3, range: 4.1-15.2) 8.52 ± 2.15 HbA1c at 6-month follow-up (median: 8.9, range: 3.5-14.6) 8.73 ± 2.09 HbA1c at 12-month follow-up (median: 8.6, range: 4.6-14.3) 8.66 ± 1.81
40 Pan-Pacific Management Review January
TABLE 2 Inter-item correlations, means, and standard deviations for patients with type 2 diabetes (n = 285)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (1) Sex 1.00 (2) Education -0.36 *** 1.00 (3) Income -0.20 ** 0.27*** 1.00 (4) Knowledge -0.19 ** 0.39*** 0.15* 1.00 (5) Attitude -0.15 * 0.16** 0.06 0.32*** 1.00 (6) Depression 0.04 -0.10 -0.21*** -0.17** -0.04 1.00 (7) Stage -0.07 0.21 0.17** 0.20** 0.03 -0.14* 1.00 (8) HbA1c 0 0.13 -0.11 -0.11 -0.16** -0.02 0.11 -0.53*** 1.00 (9) HbA1c 6 0.12 -0.20 -0.23*** -0.22*** -0.01 0.18** -0.58*** 0.71*** 1.00 (10) HbA1c 12 0.11 -0.20 -0.17** -0.19** -0.01 0.11 -0.62*** 0.69*** 0.72*** 1.00
8 Pan-Pacific Management Review January
40 P an -P ac ifi c M an ag em en t R ev ie w J an ua ry
FIGURE 2 Final model concerning a network of psychosocial determinants for glycemic control in patients with type 2 diabetes
DISCUSSION
The present study reveals that patients with lower income, higher education, poorer knowledge of diabetes, stronger locus of control, and lower stage of change were more likely to have poorer glycemic control. Among these variables, income and education are demographic variables which are difficult to change, especially for elderly patients. To the contrary, knowledge and stage of change are variables associated with greater potential for modification of T2DM patient behavior.
The finding that patients with diabetes are embedded in a complex network of interacting forces echoes the notion of Glasgow et al. (2004) that “Self-management behaviors are not only multi-dimensional, they are also multiply determined.” Compared with the explained variances (5~18%) in other studies using SEM analyses, the variances explained for two glycemic control measures (49%) in the present study are sound. The notion of Jones et al. (2003) that focus should be placed on the association of a single variable (i.e., stage of change) with glycemic control or other health behaviors merits consideration. Accordingly, stage of change was one of the associated factors investigated in the present study. In addition, Sutton (2002) reported that cross-sectional studies provide the weakest evidence for stage theories. The present study appears to provide more persuasive evidence by using a composite measure of
Pan-Pacific Management Review January 42
combining HbA1c at baseline and two follow-up values to illustrate that stage of change is one of the key mediating factors of behavioral changes in diabetic management.
Certain investigators (Colleran, Starr, & Burge, 2003; Glasgow, Goldstein, Ockene, & Pronk, 2004) have observed that glycemic control is strongly associated with socioeconomic status. The present study also reveals that income is negatively and indirectly associated with glycemic control. Regarding the effect of knowledge on glycemic control, findings of previous studies have not been consistent. Although Campbell et al. (1996) observed an association between an increase in knowledge and an improvement in glycemic control, one study found no evidence for such an association (Rose, Fliege, Hildebrandt, Schirop, & Klapp, 2002). The present study demonstrates that glycemic control is influenced internally by knowledge gained and/or utilized during this period.
Previous investigators have drawn conclusions similar to those of the present study regarding development of effective interventions for patients with diabetes (Kawamura, Tsurumoto, Fukuda, & Sasahara, 2001; Marshall & Biddle, 2001). It is therefore proposed that stage of change could be used to tailor clinical effectiveness more efficiently and to address the needs of patients in a more targeted manner. In the present study, most patients (66.3%) were classified into the pre-action stage (i.e., precontemplation, contemplation and preparation). Patients in either the action or maintenance stages were considered to be members of target groups with greater possibilities for successful change, whereas most patients at the pre-action stage were considered to be more deserving of attention and effort on the part of clinicians. It is suggested that, prior to implementing an intervention program, better understanding of the mechanism(s) by which mediators exert their effects should be acquired. Better understanding is also needed regarding the ways through which these mechanisms can be enhanced individually and in combination in order to develop an effective and efficient program tailored to the patient’s individual needs. However, in clinical settings, identification of the specific needs of an individual patient and classification of patients to different target groups is both difficult and time-consuming. The questionnaire
employed in the present study was comprised of more than 200 questions. Approximately 20-40 minutes were required for patients to complete the face-to-face interview with the diabetes educator. In this daily clinical setting, it was not feasible for the total diabetic population of the study (>1000 patients) to complete the questionnaire. However, those patients who were reluctant or who refused to complete the questionnaire might be the patients in greatest need of help. To assist patients with respect to the initial assessment of their treatment requirements and to ease the workload of clinicians, development of a more concise questionnaire with acceptable validity and reliability is warranted.
Some limitations of the present study should be addressed. It should be noted that the psychosocial measures, which were based on face-to-face interviews with nurses, may have been affected by the desire of patients to provide socially-desirable answers. It should also be noted that, because all participants had T2DM and were recruited through a single hospital under one governed-sponsored disease management program, findings of this study may not prove applicable to other treatment groups. In addition, the present study only included patient variables in model building, the program- or provider-related variables might have some relevance to glycemic control for T2DM patients. The context effect should not be ignored when interpreting the results of the present study.
CONCLUSION
Findings of the present study reveal that glycemic control in T2DM is significantly associated with demographic variables, knowledge, and stage of change. Although income, education, and knowledge do not directly affect glycemic control, these factors influence glycemic control indirectly through knowledge and stage of change. Findings of the present study offer new insight into the complexity of patient behavior in diabetes management. Given the complexity of the biology and behaviorism of diabetes, factors without direct statistical significance, such as attitude and depression should not be ignored when implementing educational programs.
Pan-Pacific Management Review January 44
REFERENCES
Alberti, K. & Gray, D. P. 1998. The care of diabetes. Diabetic Medicine, 15(S3): S3-4. Beck, A. & Beamesderfer, A. 1974. Assessment of depression: The depression
inventory. Modern Problems of Pharmacopsychiatry, 7: 151-169.
Campbell, E., Redman, S., Moffitt, P., & Sanson-Fisher, R. 1996. The relative
effectiveness of educational and behavioral instruction programs for patients with NIDDM: A randomized trial. The Diabetes Educator, 22(4): 379-386.
Colleran, K.M., Starr, B., & Burge, M.R. 2003. Putting diabetes to the test: Analyzing glycemic control based on patients' diabetes knowledge. Diabetes Care, 26(7): 2220-2221.
Davis, T. M., Cull, C. A., Holman, R. R., & UK Prospective Diabetes Study (UKPDS) Group. 2001. Relationship between ethnicity and glycemic control, lipid profiles, and blood pressure during the first 9 years of type 2 diabetes: UK Prospective Diabetes Study (UKPDS 55). Diabetes Care, 24(7): 1167-1174.
Glasgow, R. E. 1995. A practical model of diabetes management and education.
Diabetes Care, 18(1): 117-126.
Glasgow, R. E., Goldstein, M. G., Ockene, J. K., & Pronk, N. P. 2004. Translating what we have learned into practice: Principles and hypotheses for interventions
addressing multiple behaviors in primary care. American Journal of Preventive
Medicine, 27(2): 88-101.
Ismail, K., Winkley, K., & Rabe-Hesketh, S. 2004. Systematic review and
meta-analysis of randomised controlled trials of psychological interventions to improve glycaemic control in patients with type 2 diabetes. Lancet, 363(9421): 1589-1597.
Jones, H., Edwards, L., Vallis, T.M., et al. 2003. Changes in diabetes self-care behaviors make a difference in glycemic control: The Diabetes Stages of Change (DiSC) study. Diabetes Care, 26(3): 732-737.
Jöreskog, K. G., Sörbom, D. S., & Du Toit, H. C. 2000. LISREL 8: New statistical
features. Chicago: Scientific Software International.
Kawamura, M., Tsurumoto, A., Fukuda, S., & Sasahara, H. 2001. Health behaviors and their relation to metabolic control and periodontal status in type 2 diabetic patients: A model tested using a linear structural relations program. Journal of
Periodontology, 72(9): 1246-1253.
Lockington, T. J., Meadows, K. A., & Wise, P. H. 1987. Compliant behaviour:
Relationship to attitudes and control in diabetic patients. Diabetic Medicine, 4(1): 56-61.
Marshall, S. J. & Biddle, S. J. 2001. The transtheoretical model of behavior change: A meta-analysis of applications to physical activity and exercise. Annals of
Peterson, K. A. & Hughes, M. 2002. Readiness to change and clinical success in a diabetes educational program. The Journal of the American Board of Family
Practice, 15(4): 266-271.
Rose, M., Fliege, H., Hildebrandt, M., Schirop, T., & Klapp, B. F. 2002. The network of psychological variables in patients with diabetes and their importance for quality of life and metabolic control. Diabetes Care, 25(1): 35-42.
Sutton, S. 2000. Interpreting cross-sectional data on stages of change. Psychology and
Health, 15(2): 163-171.
Taiwanese Association of Diabetes Educator. 1998. Clinical guide to diabetes mellitus:
Pan-Pacific Management Review January 46
Biographical Sketch
Hui-Ching Weng Ph.D. is currently an associate professor of the Department of Health Management at I-Shou University in Taiwan. She received her M.S. degree in Sociology and Anthropology, and Ph.D. degree in Purdue University in U.S. Her current research interests include patient-physician relationship, disease management, multi-level analysis and structural equation modeling.
Chao-Ming Hung M. D. is currently a chief of general surgery in E-Da Hospital in Taiwan. He is also an instructor of the Department of Medical Nutrition. His specialty is in minimal invasive laparoscopic surgery, nutrition and metabolism, and gastroenterology.
Shu-Ching Chi is currently the director in the Department of Nursing in E-Da Hospital. She got her master degree from the Department of Nursing, National Cheng Kung University, Taiwan. Her specialty is long-term care and nursing administration.
影響糖尿病人糖化血色素控制之心理、社會及生理因素之探討 翁慧卿* 義守大學健康管理學系 洪朝明 義大醫院一般外科 義守大學醫學營養學系 紀淑靜 義大醫院護理部 中文摘要 本研究主要探討影響糖尿病人糖化血色素控制之心理、社會及生理方面因素。本 研究蒐集285 位有完成一年健保局論質計酬第二型糖尿病病人。研究結果顯示糖 化血色素的控制與病人之性別、併發症數、個人內控、及行為改變階段有顯著相 關。本結果模型解釋了糖尿病人糖化血色素控制行為 49 % 的變異數(χ2 = 32.18, df = 29, p = .31),顯示配適度良好 (AGFI = 0.96, RMSEA = 0.018)。研究結果指出 女性、教育水準較高者,知識較高者、個人內控較強者、及行為改變階段較為高 階的在糖化血色素控制比較好。研究結果可作為未來進行健康管理的糖尿病衛教 的重要參考。 關鍵詞:糖化血色素的控制、糖尿病、憂鬱、行為改變階段、結構方程式 *通訊地址:翁慧卿,義守大學健康管理系,824 高雄縣燕巢鄉角宿村義大路 8 號。 E-mail: [email protected]