Contents lists available atScienceDirect
Antiviral Research
j o u r n a l h o m e p a g e :w w w . e l s e v i e r . c o m / l o c a t e / a n t i v i r a l
Review
A new tool linking human cytomegalovirus drug resistance mutations to
resistance phenotypes
Meike Chevillotte
a, Jens von Einem
a, Benjamin M. Meier
c, Feng-Mao Lin
d,
Hans A. Kestler
b,c,∗, Thomas Mertens
a,∗∗aInstitute of Virology, University Hospital Ulm, D-89081 Ulm, Germany bInternal Medicine I, University Hospital Ulm, D-89081 Ulm, Germany
cInstitute of Neural Information Processing, University of Ulm, D-89069 Ulm, Germany
dInstitute of Bioinformatics and Systems Biology, National Chiao Tung University, Hsin-Chu 300, Taiwan, ROC
a r t i c l e i n f o
Article history:Received 31 July 2009
Received in revised form 2 October 2009 Accepted 10 October 2009 Keywords: UL97 UL54 Genotype Clinical outcome HCMV GCV CDV FOS
a b s t r a c t
Drug resistant strains of human cytomegalovirus (HCMV) in patients at risk may increasingly develop into a problem in the clinical setting. Genotypic resistance testing is becoming the method of choice, but requires previous phenotypic characterisation of each newly found mutation. In order to facilitate the interpretation of the patient’s CMV sequence data, a web-based search tool was generated that links the sequence to a database containing all published UL97 (protein kinase) and UL54 (DNA polymerase) mutations and corresponding antiviral drug susceptibility phenotypes. It is reasonable to assume that HCMV drug resistance testing will provide relevant data for an adjustment of therapy and on prognosis of clinical outcome. HCMV drug susceptibility testing will become even more important once new drugs will be available for therapy allowing a wider choice of antiviral agents to treat HCMV disease. These topics will also play a pivotal role for optimising antiviral therapy of HCMV- and other viral diseases.
© 2009 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . 319
2. Currently available systemic drugs and their resistance mechanisms . . . 319
3. Antiviral drug susceptibility testing of HCMV . . . 319
3.1. Current methods for phenotypic characterisation of drug susceptibility in HCMV . . . 319
3.2. Genotypic susceptibility testing . . . 320
3.3. Linking genotypic and phenotypic susceptibility testing of HCMV . . . 320
3.3.1. Marker transfer analyses of resistance mutations . . . 320
3.3.2. A new search tool and database of UL97 and UL54 mutations . . . 321
4. Current treatment options for HCMV infection and disease . . . 323
4.1. Prophylaxis, pre-emptive and deferred therapy . . . 323
4.2. HCMV resistance: clinical incidence and impact . . . 323
5. Future needs . . . 324
5.1. Clinical evaluation—correlation of assay data with clinical outcome data . . . 324
5.2. Incorporation of new drugs and targets into the database . . . 324
6. Conclusions . . . 324
Acknowledgements . . . 325
References . . . 325
∗ Corresponding author at: Institute of Neural Information Processing, University of Ulm, 89069 Ulm, Germany. Tel.: +49 731 5024248; fax: +49 731 5024156. ∗∗ Corresponding author at: Institute of Virology, University Hospital Ulm, 89081 Ulm, Germany. Tel.: +49 731 500 65100; fax: +49 731 500 65102.
E-mail addresses:[email protected](H.A. Kestler),[email protected](T. Mertens). 0166-3542/$ – see front matter © 2009 Elsevier B.V. All rights reserved.
1. Introduction
Human cytomegalovirus (HCMV) is a highly relevant oppor-tunistic pathogen for individuals with a compromised or immature immune system, such as transplant recipients, patients with acquired immunodeficiency disease syndrome (AIDS) or connatal infected children. HCMV is the leading cause of birth defects caused by intrauterine virus infections, but unfortunately, no effective treatment is currently licensed during pregnancy. Without antivi-ral intervention, HCMV-associated disease represents a main cause of morbidity and mortality in solid organ transplant (SOT) and in bone marrow or hematopoietic stem cell transplant (BMT/HSCT) recipients (Boeckh et al., 2004; Boeckh and Ljungman, 2009; Sia
and Patel, 2000; Sun et al., 2008). The incidence of HCMV-related
complications and death in AIDS patients has declined due to the introduction of highly active antiretroviral therapy (HAART) (Kedhar and Jabs, 2007; Palella et al., 1998), but still remains a con-cern in patients with low CD4+ cell counts. Therefore, diagnosis and monitoring of active HCMV infection and, in many cases, long-term antiviral therapy against HCMV are life-saving for patients at risk for severe HCMV disease.
Many factors influence the success of anti-HCMV treatment, such as the underlying disease, the severity of immunosuppression, concentrations of the antiviral drugs, and finally the susceptibility of the patient’s viral strain – or viral strains – to the administered antiviral drug. Virologists have to provide clinically validated meth-ods for fast and reproducible drug susceptibility testing in order to (i) determine viral drug resistance as reason for failure of ther-apy, (ii) optimise antiviral therther-apy, (iii) provide a new prognostic marker.
This review recapitulates current treatment options for HCMV infection and disease, resistance mechanisms and methods for drug susceptibility testing. In this context, a new tool is presented that links HCMV genotypes to a database of published in vitro drug susceptibility phenotypes, thereby providing information for an optimisation of antiviral therapy. Furthermore, future needs are discussed, such as required clinical validation of antiviral resis-tance testing using the proposed interpretation system as well as the incorporation of future drugs and drug targets into the database.
2. Currently available systemic drugs and their resistance mechanisms
Three systemic drugs are currently licensed to treat HCMV infections and disease: Ganciclovir (GCV) including its prodrug Val-ganciclovir (ValGCV), Cidofovir (CDV) and Foscarnet (FOS). All drugs target the viral DNA polymerase, pUL54. GCV acts as nucleoside analogue and has to be initially phosphorylated by the HCMV pro-tein kinase, pUL97 (Cihlar and Chen, 1996; Michel et al., 1998; Sullivan et al., 1992). CDV does not require this initial phosphoryla-tion step and acts as nucleotide analogue. Finally, FOS has a different mode of action by acting as pyrophosphate analogue (Chrisp and Clissold, 1991).
The two viral proteins involved in resistance mechanisms against these three drugs are pUL97 and pUL54. Defined muta-tions in pUL97 lead to reduced phosphorylation activities resulting in lower levels of monophosphorylated – and thus active – GCV
(Baldanti et al., 2002a; Biron et al., 1986). The degree of residual
pUL97 phosphorylation activity and reduced drug susceptibility is quite variable, depending on the position of the mutated amino acid (Baldanti et al., 2002a; Chou et al., 1995a, 1995b). Hence, mutations in UL97 exclusively confer resistance to GCV, and about 90% of all GCV resistances detected so far have been attributed to mutations in UL97 (Chou, 1999). Mutations in the polymerase may increase its exonuclease activity, so that the nucleoside analogues GCV and CDV are recognised and excised from the DNA chain more
effi-ciently. Additionally, other polymerase mutations are thought to decrease affinity for antiviral compounds, a mechanism that con-cerns all three antivirals mentioned and thus may lead to multidrug resistance (Gilbert and Boivin, 2005a).
It has been described that the evolution of antiviral resistance occurs in a stepwise fashion (reviewed inNijhuis et al., 2009; Müller
and Kräusslich, 2009). Prior treatment, the entire virus population
naturally contains only a small fraction of less drug susceptible variants. This phenomenon can be explained by a reduction of replicative fitness of those variants. When subsequent antiviral treatment does not suppress viral replication completely, e.g. due to suboptimal levels of antiviral drugs or extreme immunosup-pression of the host, a selection process favouring these variants is initiated. Since they can further replicate in the presence of the antiviral drug, they are able to evolve and acquire additional mutations that enhance replicative fitness and possibly increase resistance, finally resulting in a large population of highly resistant and replication competent viruses. Concerning HCMV, this model is supported by the fact that major risk factors for HCMV drug resistance are the residual capacity of the host’s immune system to control viral replication and the overall amount and duration of viral replication (Drew, 2000). The clinical virologist has to keep these selection mechanisms in mind when monitoring viral loads in patients responding to antiviral therapy. Furthermore, the moment of antiviral drug susceptibility testing combined with the sensitiv-ity of applied assays has to be critically evaluated.
3. Antiviral drug susceptibility testing of HCMV
3.1. Current methods for phenotypic characterisation of drug susceptibility in HCMV
Before the establishment of genotypic testing, phenotypic test-ing of clinical isolates was the method of choice for determintest-ing HCMV drug susceptibility and it still is in many laboratories. In the-ory, phenotyping should be advantageous, since drug susceptibility of the clinical isolate including all acquired mutations can directly be assessed. However, major disadvantages of phenotypic testing are the difficulties in obtaining the isolate from a patient’s sample – especially after onset of therapy – selection of a sensitive virus population during the isolation process and in general the slow replication of HCMV which delays results up to several weeks. In consequence, phenotypic testing can in most cases only be used for retrospective determination of resistance. Although the method is still used for diagnostic purposes, the main importance of pheno-typic testing today relies on the characterisation of newly found mutations after marker transfer experiments in order to provide the necessary basis for genotypic resistance testing.
As recommended by the Food and Drug Administration in 2007, drug susceptibility of a viral strain to a specific antiviral agent should be expressed as the drug concentration that is effective to inhibit viral replication in vitro by 50% (EC50). Today, the gold
stan-dard for phenotypic characterisation of HCMV is still the plaque reduction assay (PRA), which measures viral spread in cell culture using different antiviral drug concentrations and counting newly formed viral plaques. However, assay and especially inter-laboratory standardisation of the PRA has been shown to be very difficult (Landry et al., 2000). These difficulties can be attributed mainly to differences in cell cultures used by different labora-tories. In consequence, efforts have been made to develop new assays, which allow for a better standardisation. Some are based on reporter cell lines measuring HCMV spread in cell culture reflected by luciferase activity (Gilbert and Boivin, 2005b), green fluorescent protein (GFP) (Ueno et al., 2006; Ueno and Ogawa-Goto, 2009), or enhanced green fluorescent protein (EGFP) (Luganini et al., 2008). Another approach is to use quantitative real-time PCR to detect
the declining number of genome copies in cell culture due to dif-ferent concentrations of the antiviral agent (Schnepf et al., 2009). As these assays measure a signal instead of counting plaques, they are less biased and thus allow for a better standardisation of drug susceptibility testing of clinical isolates. Other assays are based on recombinant viruses and can therefore not be applied directly for characterisation of clinical isolates, but are used for marker trans-fer experiments. These viruses express diftrans-ferent reporter proteins in infected cells, such as secreted alkaline phosphatase (Chou et al., 2005), GFP (Marschall et al., 2000), EYFP (Dal Pozzo et al., 2008) or EGFP (Chevillotte et al., 2009). The expression of reporter proteins can be quantified in a plate reader detecting chemiluminescence (Chou et al., 2005) or fluorescence (Chevillotte et al., 2009) or by flow cytometry (Dal Pozzo et al., 2008; Marschall et al., 2000) and used to calculate EC50 values. Finally, EC50values have also
been determined by a non-radioactive in vitro assay which deter-mines viral polymerase activity by measuring the incorporation of labelled nucleotides (Ducancelle et al., 2007).
These new methods are often easier to perform and better stan-dardised than the PRA, and are important tools to identify and characterise mutations relevant for reduced drug susceptibility. Still, all assays, including the PRA, lack clinically validated data defining which increase in the EC50value is likely to cause clinical
resistance in the patient.
3.2. Genotypic susceptibility testing
Genotypic susceptibility testing is becoming the method of choice, because reliable results can be obtained within hours
(Drew, 2007). Concerning the drugs available today, the two
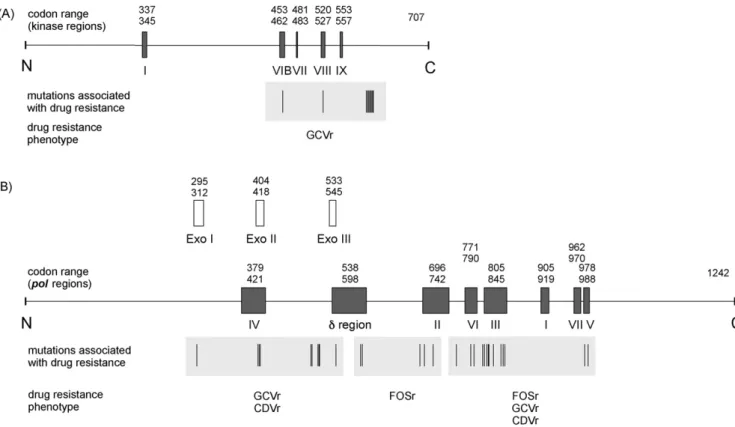
rel-evant genes, UL97 and UL54, are amplified from patient material and subsequently screened for mutations. pUL97 comprises 707 amino acids (AA), and all resistance associated mutations proven by marker transfer are located between AA 460 and 607 (reviewed inChou, 2008; Schreiber et al., 2009) (Fig. 1A). Therefore a relatively small region of approx. 600 base pairs of UL97 has to be sequenced. In addition, the five most frequently detected resistance conferring mutations – M460V, H520Q, A594V, L595L and C603W – represent about 80% of all found UL97 mutations (Schreiber et al., 2009).
In contrast, the situation for UL54 is much more complex: (i) the protein is much larger, (ii) number and diversity of mutations are higher and (iii) resistance associated mutations are located in several clusters (Fig. 1B), which all together requires sequencing of a region of over 2.5 kb. In addition, the position of the mutation in the protein seems to determine the resistance phenotype. Muta-tions located in the exonuclease domains tend to confer resistance against the two nucleoside analogues (Chou et al., 2003; Cihlar et al., 1998a, 1998b; Drew et al., 2006; Ducancelle et al., 2005; Lurain et al., 1992; Marfori et al., 2007; Scott et al., 2007), whereas mutations between AA 588 and 715 have been described in association with FOS resistance (Baldanti et al., 1996; Cihlar et al., 1998a; Ducancelle et al., 2005; Mousavi-Jazi et al., 2001; Springer et al., 2005). Finally, mutations between AA 756 and 982 are linked to resistance against any of the three drugs – to one drug alone or combinations (Baldanti et al., 1996; Chou and Marousek, 2008; Chou et al., 1997, 2003; Cihlar et al., 1998a; Drew et al., 2006; Mousavi-Jazi et al., 2001; Scott et al., 2007; Springer et al., 2005; Tchesnokov et al., 2006; Weinberg et al., 2003) (Fig. 1B).
One important advantage of genotypic resistance testing is the detection of mutant virus subpopulations. Up to now, the sensitiv-ity of PCR followed by conventional (Sanger) sequencing methods is sufficient to detect subpopulations that exceed 10% of the whole virus population (Schreiber et al., 2009). However, this might not be sensitive enough to detect subpopulations in the early phase of therapy. A novel approach to overcome this problem and to increase sensitivity could be the use of pyrosequencing techniques (Ronaghi
et al., 1998), which reliably allows for the detection and
quantifi-cation of mixed UL97 populations starting from 6%, and for specific mutations even starting from 2 to 3% (Bernd Ehlers, personal com-munication).
An additional matter of genotypic resistance testing may be that HCMV populations may differ in their composition within one sin-gle patient in different compartments (Eckle et al., 2000; Erice et
al., 1997; Michel et al., 2003). For example, this has been described
by analysing the proportion of a genotypically resistant subpopula-tion in different isolates from various compartments, obtained on the same day from a heart transplant patient (Michel et al., 2003). The report showed that the percentage of resistant virus was 80% in the isolated virus population obtained from a throat wash, 50% from urine, and no resistant virus could be detected in the isolate obtained from leucocytes. These results highlight the importance not only to investigate the composition of the viral population but also to consider the relevant compartments.
Finally, the major challenge of genotypic resistance testing is to link its results to corresponding resistance phenotypes. Genotypic susceptibility testing definitely requires prior phenotypic charac-terisation of the respective mutations – and combinations – in order to distinguish between “baseline” – clinically irrelevant – and resistance conferring mutations. In fact, a number of poten-tially resistance associated mutations found in clinical isolates have been shown not to be responsible for an increase in EC50values in
marker transfer experiments.
3.3. Linking genotypic and phenotypic susceptibility testing of HCMV
3.3.1. Marker transfer analyses of resistance mutations
In marker transfer experiments, mutations suspected to confer resistance are introduced into a well defined, drug-sensitive viral background and then tested phenotypically. Thus, these experi-ments are able to provide the link between genotype and drug susceptibility phenotype. Different protocols have been published for the generation of such recombinant HCMV strains for drug sus-ceptibility testing.
Early protocols were based on either cotransfection of HCMV DNA or transfection of HCMV infected cells with linear DNA con-taining the mutated sequence. After recombination of the DNA in the transfected cell, recombinant viruses bearing the desired mutation could be reconstituted and then plaque purified in order to avoid wild-type virus contamination (Baldanti et al., 1996; Bourgeois et al., 1997; Chou et al., 2000; Cihlar et al., 1998a; Faizi Khan et al., 1998; Lurain et al., 1992; Mousavi-Jazi et al., 2001;
Sullivan et al., 1992). These approaches do not produce a clonal
virus population, as wild-type virus contaminations can never be completely suppressed, influencing the results of drug suscepti-bility testing. Other methods use a drug-sensitive parental HCMV strain that bears unique restriction sites in the target gene. The parental DNA is digested with a restriction enzyme and cotrans-fected with a plasmid containing the mutation(s) of interest in the respective gene. Recombination between overlapping sequences in the plasmid and the digested parental DNA in cotransfected cells results in viable recombinant virus harbouring the desired mutation(s) (Chou, 2008; Chou and Marousek, 2008; Chou et al., 2003, 2005; Drew et al., 2006; Iwasenko et al., 2009; Marfori et al., 2007; Scott et al., 2007; Springer et al., 2005; Weinberg et al., 2003). This method highly increases the selective pressure for the formation of recombinant virus compared to wild-type virus, but plaque purification is still necessary. The problem of wild-type virus contamination has been first circumvented using an in vitro assay, where only the mutated enzymes, and not viruses, are generated and tested for drug susceptibility (Ducancelle et al., 2005, 2007). More recently, bacterial artificial chromosome (BAC) technology
Fig. 1. (A) HCMV UL97 (kinase) and (B) UL54 (polymerase) regions, mutations associated with drug resistance and corresponding drug resistance phenotypes. Shown are only marker transfer proven mutations. N = N-terminus; C = C-terminus; pol = polymerase; Exo = exonuclease domain; GCVr = Ganciclovir resistance; CDVr = Cidofovir resistance; FOSr = Foscarnet resistance.
has been applied to generate clonal recombinant viruses for marker transfer experiments. Since all progeny viruses go back to BAC DNA from one single bacterial colony, clonal virus populations are obtained. Several protocols have been published for the generation of recombinant BACs for HCMV marker transfer purposes, based on a flip recombinase (Martin et al., 2006), RED recombinase (Chou, 2009), or RED-GAM recombinase system (Chevillotte et al., 2009). Only the latter two are markerless mutagenesis methods, meaning that they leave no trace of the recombination procedure in the BAC sequence (Tischer et al., 2006; Warming et al., 2005). BAC muta-genesis is efficient and relatively fast, and is now becoming the method of choice for the characterisation of the many still unchar-acterised mutations. The number of needed marker transfers has further increased since we know that combinations of mutations in UL97 and UL54 on the one hand sometimes have a synergistic effect on the decrease of drug susceptibility (Ducancelle et al., 2007;
Mousavi-Jazi et al., 2001; Scott et al., 2007), but can on the other
hand also partially compensate for each other (Ijichi et al., 2002). Therefore, the influence of combinations is difficult to predict and has to be analysed in additional marker transfer experiments. 3.3.2. A new search tool and database of UL97 and UL54 mutations
More than 60 publications on HCMV resistance mutations are now available, reporting over 50 UL97 and over 150 UL54 muta-tions. In order to allow a fast interpretation of sequence data from genotypic susceptibility testing, we have generated a web-based search tool where a patient’s CMV UL97 or UL54 sequence can be uploaded and will be subsequently compared to the wild-type sequence of the drug-sensitive HCMV strain TB40-BAC4
(Chevillotte et al., 2009; Sinzger et al., 2008). Detected mutations
will be linked to a regularly updated database that contains all published UL97 and UL54 mutations and the corresponding in vitro phenotypes, thus providing important parameters for the
evaluation of mutations. If a mutation is found that is not yet known or presented in the database, it can be reported (via email) and will be integrated into the database. The procedure for the HCMV mutation identification is as follows: We use BLASTX (ver-sion: NCBI BLAST 2.2.18) (Altschul et al., 1990, 1997) to align UL54/UL97 wild-type protein sequence and a given UL54/UL97 nucleotide sequence (see Fig. 2). Possible amino acid mutations of the given HCMV strand can then be identified. According to the mutation locations and mutated amino acids, the system com-pares the mutations with HCMV mutation database and reports which type of mutations and associated literature are present in the given HCMV sequence (see
http://www.informatik.uni-ulm.de/ni/mitarbeiter/HKestler/hcmv).
The results provided for a previously published mutation con-tain (i) its qualitative drug susceptibility phenotype (as stated by the respective authors), (ii) its quantitative drug susceptibility phe-notype (the ratio of EC50values compared to wild type), (iii) its viral
replicative fitness, a parameter that might also influence clinical outcome (Emery and Griffiths, 2000), (iv) the respective publica-tion, with a link to pubmed, and (v) the assay used in the cited publication. In addition, the location of the mutation is indicated in a linear scheme of the respective protein containing all resistance associated entries represented in the database. If a sequence has been submitted, its position is shown in the scheme, so that it can be easily controlled whether all relevant regions are covered by the sequencing reaction (Fig. 3).
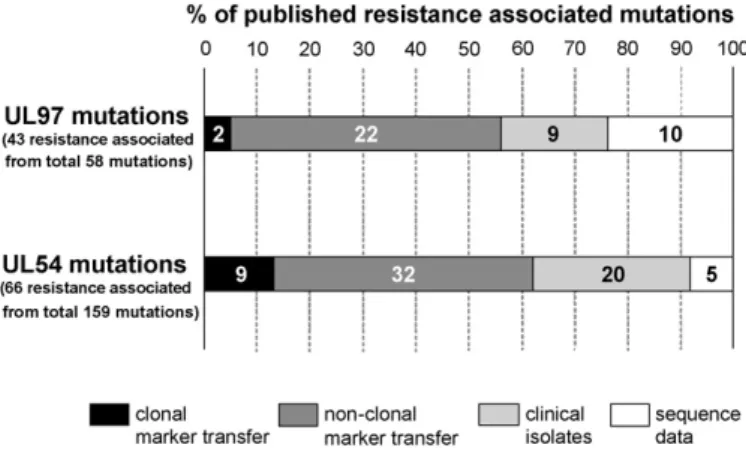
The success of all “genotype to phenotype” approaches in reveal-ing relevant data highly depends on the quality of the phenotypic data. Therefore, knowledge of the methods used for generating the phenotypic data is very important regarding the assessment of reli-ability. For example, reliability is much higher when the data is based on clonal marker transfer experiments combined with the use of a reporter system for a phenotypic readout than when it is entirely based on sequence data from a patient with therapy failure
Fig. 2. Flowchart of the sequence analysis.
Fig. 4. Quality of phenotypic data for published proven and suspected resistance associated UL97 and UL54 mutations from the database.
without any phenotypic characterisation. Currently, the majority of published mutations has been characterised by marker transfer experiments, albeit only few by clonal marker transfer experiments
(Fig. 4). The remaining mutations, only known from
characteri-sation of clinical isolates or from sequence data, still have to be properly characterised in marker transfer experiments to allow better interpretation of genotypes.
Another important yet controversial point is the definition of resistance. Different publications use different definitions, e.g. 2-fold increases in EC50values (Chou et al., 2003) or absolute EC50
values that have to be exceeded (Drew et al., 2006; Smith et al., 1997). Others have defined mutations detected in a specimen from an individual patient as resistance conferring based on correla-tion with clinical failure of therapy (Oshima et al., 2008). However, those definitions are arbitrary and lack proper clinical validation. We decided to enter information on the qualitative susceptibility phenotype into the database “as stated by the respective authors” without adding an additional arbitrary definition. In the future, clin-ical studies have to be performed in order to assess the relevance of specific mutations for clinical outcome and the need of adjustment of therapy.
Up to now, the knowledge about drug resistance of HCMV is mainly based on phenotypic data from cell culture experiments. These data are now easily accessible via our search tool. Clini-cal evaluation of the data will be a major challenge in the future, which is indispensable in order to further improve the basis for an optimisation of antiviral therapy against HCMV.
4. Current treatment options for HCMV infection and disease
There are basically two options to help the patient’s organ-ism in terminating an active systemic HCMV infection: either by improving the immunologic situation, or by the administration of antiviral drugs. Enhancement of the patient’s immune status can be achieved, e.g. by reduction of an immunosuppressive therapy after SOT (Egli et al., 2007) or by effective treatment of an HIV infection by HAART (Goossens et al., 2009). All available antiviral drugs for treatment of HCMV infections may induce considerable drug spe-cific and potentially severe adverse effects (reviewed inSchreiber
et al., 2009). Therefore, it is of utmost importance to accurately
identify specific patients and clinical situations requiring antiviral therapy or prophylaxis in order to avoid undue therapy.
4.1. Prophylaxis, pre-emptive and deferred therapy
During the past two decades, it has become clear that differ-ent patidiffer-ent groups – such as recipidiffer-ents of renal or liver transplants,
recipients of heart and lung allografts or patients after allogenic HSCT – carry different and specific risks of developing severe HCMV disease. Due to unknown reasons, disease manifestations like retinitis, pneumonitis, gastrointestinal ulcers, or even arthe-riosclerosis in the organ graft are preferentially connected to specific patient groups at risk, e.g. retinitis in AIDS but intersti-tial pneumonia in HSCT patients. The HCMV serostatus of donor and recipient in the transplant situation is an important factor, but the consequences for risk calculation are different between SOT and HSCT. The amount and type of immunosuppression rep-resents yet another very important risk factor. It has been shown that in vivo/ex vivo T-cell depletion for graft versus host disease prophylaxis in BMT is a strong risk factor for active systemic HCMV infection (Hertenstein et al., 1995). The same is true for rejection therapy using anti-T-cell antibodies in renal transplant recipients (von Müller et al., 2006). Interestingly, in the latter situation, the alloreaction seems to play an additional role in triggering a sys-temic HCMV reactivation. In addition, there is data indicating that different immunosuppressive drugs themselves, such as mycophe-nolate mofetil, have the potential to trigger an active systemic viral infection (ter Meulen et al., 2000) while others lower the incidence of systemic viral infection (Vigano et al., 2009). Underlying mech-anisms remain unclear, but it can be assumed that influences on CD8+ populations or intrinsic antiviral activity of the drugs may contribute to the reported effects.
Some HCMV disease manifestations like interstitial pneumoni-tis in HSCT patients need to be treated as early as possible to prevent severe disease or even mortality (Reusser et al., 2002). In general, diagnosis of an active systemic HCMV infection (by detection of virus, viral antigen or DNA in the blood compartment) indicates a greater risk for severe HCMV disease than an organ restricted active infection (detectable e.g. only by virus shedding in the urine).
In summary, correct stratification of the patients for differ-ent therapeutic regimens – prophylaxis, pre-emptive and deferred therapy – is still very complex and the optimum therapeutic pro-cedure has to be determined for each group. It is obvious that undue treatment differs between the regimens: prophylaxis > pre-emptive therapy > deferred therapy. An antiviral prophylactic regimen is often used for patients bearing the highest risk of developing severe HCMV-disease (e.g. heart and lung transplant recipients). For HSCT, pre-emptive therapy – meaning therapy of active systemic HCMV infections without disease manifestations – has been proven to be most effective (Einsele et al., 1995; Reusser et al., 2002). In contrast, in patients after liver transplantation deferred therapy is feasible. It is possible to delay antiviral treatment until HCMV disease manifestations do occur without an increased risk for life threatening disease or loss of transplanted organ function in these patients.
4.2. HCMV resistance: clinical incidence and impact
“Clinical resistance” and “viral resistance” are often used syn-onymously, although they represent two different entities. The term “clinical resistance” means no response of clinical parameters to the antiviral drug (Reusser et al., 1996). Yet, clinical resistance may have other reasons than the presence of a resistant HCMV, such as the underlying disease, the type and severity of immunosuppres-sion, and concentrations of the antiviral drugs. In contrast, the term “viral resistance” stands for the presence of a drug resistant viral strain, and is commonly divided into phenotypic and genotypic resistance, depending on the method of testing.
The incidence of viral drug resistance of HCMV strongly varies in the numerous studies analysing this problem, depending on dif-ferent parameters such as (i) the group of patients (pre-existing conditions), (ii) the medication profile, (iii) the time of testing, (iv) the method of testing (e.g. geno- or phenotypic), (v) whether the
study was performed retrospectively or prospectively and finally (vi) the definition of “resistance”. All mentioned parameters make it difficult to directly compare the data of these respective studies. The emergence of drug resistant HCMV strains was first described in AIDS patients. Up to 27% of AIDS patients carried a phe-notypically resistant HCMV strain after 12 months of anti-HCMV therapy (Jabs et al., 1998a, 1998b). The baseline phenotypic resis-tance – before treatment – was below 3%. The percentage increased with the duration of therapy and the occurrence of resistant HCMV strains was generally associated with unfavourable clinical out-come in those patients. In another study, the authors found that after 12 months of anti-HCMV therapy 12.8% of patients carried genotypically resistant strains (Boivin et al., 2001), indicating the impact of the method of testing mentioned above on the incidence of viral drug resistance. Since introduction of HAART, the frequency of HCMV disease in AIDS patients has sharply declined, due to an improvement of the immunologic situation of the patients (Kedhar
and Jabs, 2007; Palella et al., 1998). Nevertheless, HCMV disease
together with antiviral resistance remains a problem in patients with failure of HAART therapy (Baldanti et al., 2002b).
For SOT patients, the clinical impact seems to be lower than for AIDS patients. A large retrospective study including 240 SOT patients found genotypic resistance in 2.1% of all patients at a median of 10 months post-transplantation (Limaye et al., 2000). Resistance was only detected in previously seronegative patients who had obtained a seropositive graft (D+/R−), and the percent-age of viral resistance was 7%. Among these patients, resistance was most frequently found after kidney-pancreas transplantation with an incidence of 21%. Overall, resistant HCMV strains were responsible for 20% of HCMV diseases during the first year post-transplantation. However, it is possible that these retrospective studies tend to overestimate the prevalence of HCMV resistance because of a selection bias. This is supported by two prospective studies with SOT patients, where a lower incidence of genotypic resistance (between 0% (treatment with ValGCV) and 6.1% (oral GCV)) was found (Boivin et al., 2004, 2005). Interestingly, in the latter two studies, resistant strains did not seem to be necessarily associated with adverse clinical outcome, as some patients har-bouring resistant strains remained totally asymptomatic.
In a setting of pronounced immunosuppression, the maximum frequency of HCMV resistance in adult HSCT patients has been reported to be as high as 8% (Boeckh et al., 2003, 2004; Boeckh and
Ljungman, 2009). Apart from these data, only case reports seem to
be available for the HSCT/BMT patients setting (Erice et al., 1998; Julin et al., 2002; Springer et al., 2005), reporting poor clinical out-come associated with the detection of resistant HCMV strains. The situation is slightly different in the pediatric setting, where resis-tant strains seem to emerge very rapidly, starting from weeks after exposure to the drug (Eckle et al., 2000, 2002; Wolf et al., 1998).
In conclusion, prospective, standardised studies have to be per-formed in order to assess the occurrence of resistant HCMV strains as well as their relevance for clinical outcome. To address this point, the generation of a database where results from such clinical stud-ies can be uploaded and evaluated seems to be an excellent tool.
5. Future needs
5.1. Clinical evaluation—correlation of assay data with clinical outcome data
Our new web-based search tool together with the database as it is today is derived from published associations between HCMV genotypes and corresponding cell culture resistance pheno-types, which is currently the best information available. However, medical validation of such a tool – and of resistance testing in general – is a crucial point for its successful use in the clinical
setting. It is therefore necessary to perform studies linking the susceptibility data to standardised studies, monitoring viral and clinical data longitudinally. With this knowledge, it is essential to define procedures for therapeutic recommendations and prog-nosis of therapeutic response. Databases of rules have already been established for other viruses, e.g. the Stanford University HIV drug resistance database (http://hivdb.stanford.edu/), Genafor’s geno2pheno tool (http://www.geno2pheno.org), the HIV Grade tool (http://www.hiv-grade.de) or the HIV French resistance tool
(http://www.hivfrenchresistance.org), and some of these have
already undergone clinical evaluation.
Regarding HCMV, only few case reports are currently avail-able to answer questions about therapeutic recommendation and clinical prognosis. One example is the UL97 mutation C592G, orig-inating from an AIDS patient (Chou et al., 1997). This mutation has been shown to confer a moderate, 2.3- to 2.9-fold, increase of EC50 values for GCV in marker transfer analyses (Chou et al.,
2005; Iwasenko et al., 2009). C592G was detected after therapy
with oral GCV and antiviral therapy was continued. Consequently, highly resistant virus populations, bearing other UL97 and addi-tional UL54 mutations, were selected, which led to therapeutic failure and caused the death of the patient (Chou et al., 1997). Another case report described the effect of the UL97 mutation N597D, found in a heart transplant patient after ValGCV treatment. This mutation confers only low-grade reduction of susceptibility to GCV (EC50ratio 1.4, confirmed by marker transfer analyses).
Con-tinuation of therapy with ValGCV lead to clearance of CMV from the blood, and the patient had no further episodes of CMV-related symptoms (Iwasenko et al., 2009), indicating that the virus popula-tion bearing this mutapopula-tion can be controlled by applying optimum doses of GCV. Obviously, prospective studies have to be performed in order to define a clear cut-off for EC50values indicating the need
of switching therapy to another antiviral drug.
5.2. Incorporation of new drugs and targets into the database As already mentioned, all available anti-HCMV drugs share the same target, pUL54, so that one single mutation may lead to mul-tidrug resistance. Therefore, it is imperative to find new drugs against HCMV having different targets. Several compounds are currently under investigation, targeting viral entry, replication, or virion assembly and egress (reviewed inAndrei et al., 2008, 2009). The most promising among these compounds is Maribavir (MBV), although its future is unclear because of unfavourable results in clinical phase III trials (Mark Uknis, symposium at the 12th
Inter-national CMV/Betaherpesvirus Workshop, Boston, MA, 2009). MBV acts as an inhibitor of UL97 (Biron et al., 2002) and so far, no cross-resistance to GCV, CDV and FOS has been reported. Up to now, mutations conferring a reduced susceptibility have been found only in vitro (Chou and Marousek, 2008; Chou et al., 2007). These have been shown to map in the viral genes UL97 and UL27 (Chou et al.,
2004; Komazin et al., 2003). The example of MBV demonstrates that
the complexity of HCMV resistance testing will increase not only because of additional drugs, but also because of additional targets bearing new resistance associated mutations. Once licensed, these new drugs and their respective targets will be incorporated into the database, thereby increasing its importance, as information from the database will allow more systematic choices of medications based on the resistance profiles.
6. Conclusions
In recent years, the treatment of HCMV disease and clinical outcome has been enormously improved by monitoring active sys-temic infections and the introduction of HCMV antiviral therapy.
Nevertheless, the situation concerning HCMV treatment is complex and still not satisfying. Taken the current knowledge into account, it can be assumed that many factors contribute to the overall drug susceptibility phenotype of a patient’s virus population. Among those are the underlying disease, the degree of immunosupression, the clinical sample, the type and position of mutations in UL97 and UL54, the viral replicative fitness, and finally – depending on the replicative fitness – the dynamics of a resistant virus population.
The questions of the treating clinician are clearly defined: (i) who has to be treated, (ii) when to start, (iii) which antiviral drug to use, (iv) when to augment the dosage or switch the drug due to virological susceptibility findings?
Since phenotypical testing of isolated viruses is not practicable in the clinics, genotyping is the method of choice because results can be obtained reliably within hours. Still, all individual mutations in the genes relevant for resistance have to be characterised phe-notypically, including combinations of these mutations. Our new web-based search tool and database will be a major improvement for the fast evaluation of sequence data regarding their suscepti-bility phenotype. Finally, reduced drug susceptisuscepti-bility – virological resistance – has to be correlated with therapy failure – clinical resistance – and patient’s outcome in prospective clinical studies.
Acknowledgements
We would like to thank Johann M Kraus and Ludwig Lausser for technical support and Bernd Ehlers for the information on detection of HCMV subpopulations by pyrosequencing. Meike Chevillotte is participant in the International Graduate School in Molecular Medicine Ulm, funded by the Excellence Initiative of the Ger-man federal and state governments. University Hospital Ulm and the Robert-Koch-Institut, Berlin (Netzwerk für Infektionen bei Immundefizienz oder Schwangerschaft), supported the work of Meike Chevillotte. The German Academic Exchange Service (DAAD) supported the work of Feng-Mao Lin and this research was partly funded by a “Forschungsdozent” grant through the “Stifterverband für die Deutsche Wissenschaft” and by the German Science Foun-dation (SFB 518, Project C05) to Hans A. Kestler.
References
Altschul, S.F., Gish, W., Miller, W., Myers, E.W., Lipman, D.J., 1990. Basic local align-ment search tool. J. Mol. Biol. 215, 403–410.
Altschul, S.F., Madden, T.L., Schaffer, A.A., Zhang, J., Zhang, Z., Miller, W., Lipman, D.J., 1997. Gapped BLAST and PSI-BLAST: a new generation of protein database search programs. Nucleic Acids Res. 25, 3389–3402.
Andrei, G., de Clercq, E., Snoeck, R., 2008. Novel inhibitors of human CMV. Curr. Opin. Investig. Drugs 9, 132–145.
Andrei, G., de Clercq, E., Snoeck, R., 2009. Drug targets in cytomegalovirus infection. Infect Disord. Drug Targets 9, 201–222.
Baldanti, F., Michel, D., Simoncini, L., Heuschmid, M., Zimmermann, A., Minisini, R., Schaarschmidt, P., Schmid, T., Gerna, G., Mertens, T., 2002a. Mutations in the UL97 ORF of ganciclovir-resistant clinical cytomegalovirus isolates differen-tially affect GCV phosphorylation as determined in a recombinant vaccinia virus system. Antiviral Res. 54, 59–67.
Baldanti, F., Paolucci, S., Parisi, A., Meroni, L., Gerna, G., 2002b. Emergence of mul-tiple drug resistant human cytomegalovirus variants in 2 patients with human immunodeficiency virus infection unresponsive to highly active antiretroviral therapy. Clin. Infect. Dis. 34, 1146–1149.
Baldanti, F., Underwood, M.R., Stanat, S.C., Biron, K.K., Chou, S.W., Sarasini, A., Silini, E., Gerna, G., 1996. Single amino acids changes in the DNA polymerase confer foscarnet resistance and slow-growth phenotype, while mutations in the UL97-encoded phosphotransferase confer ganciclovir resistance in three double-resistant human cytomegalovirus strains recovered from patients with AIDS. J. Virol. 70, 1390–1395.
Biron, K.K., Fyfe, J.A., Stanat, S.C., Leslie, L.K., Sorrell, J.B., Lambe, C.U., Coen, D.M., 1986. A human cytomegalovirus mutant resistant to the nucleoside analog 9-([2-hydroxy-1-(hydroxymethyl)ethoxy]methyl)guanine (BW B759U) induces reduced levels of BW B759U triphosphate. Proc. Natl. Acad. Sci. U.S.A. 83, 8769–8773.
Biron, K.K., Harvey, R.J., Chamberlain, S.C., Good, S.S., Smith III, A.A., Davis, M.G., Talarico, C.L., Miller, W.H., Ferris, R., Dornsife, R.E., Stanat, S.C., Drach, J.C., Townsend, L.B., Koszalka, G.W., 2002. Potent and selective inhibition of human
cytomegalovirus replication by 1263W94, a benzimidazole L-riboside with a unique mode of action. Antimicrob. Agents Chemother. 46, 2365–2372. Boeckh, M., Fries, B., Nichols, W.G., 2004. Recent advances in the prevention of CMV
infection and disease after hematopoietic stem cell transplantation. Pediatr. Transplant. 8 (Suppl 5), 19–27.
Boeckh, M., Ljungman, P., 2009. How we treat CMV in hematopoietic cell transplant recipients. Blood 113, 5711–5719.
Boeckh, M., Nichols, W.G., Papanicolaou, G., Rubin, R., Wingard, J.R., Zaia, J., 2003. Cytomegalovirus in hematopoietic stem cell transplant recipients: current sta-tus, known challenges, and future strategies. Biol. Blood Marrow Transplant. 9, 543–558.
Boivin, G., Gilbert, C., Gaudreau, A., Greenfield, I., Sudlow, R., Roberts, N.-A., 2001. Rate of emergence of cytomegalovirus (CMV) mutations in leukocytes of patients with acquired immunodeficiency syndrome who are receiving valgan-ciclovir as induction and maintenance therapy for CMV retinitis. J. Inf. Dis. 184, 1598–1602.
Boivin, G., Goyette, N., Gilbert, C., Humar, A., Covington, E., 2005. Clinical impact of ganciclovir-resistant cytomegalovirus infections in solid organ transplant patients. Transpl. Infect. Dis. 7, 166–170.
Boivin, G., Goyette, N., Gilbert, C., Roberts, N., Macey, K., Paya, C., Pescovitz, M.-D., Humar, A., Dominguez, E., Washburn, K., Blumberg, E., Alexander, B., Freeman, R., Heaton, N., Covington, E., 2004. Absence of cytomegalovirus resistance muta-tions after valganciclovir prophylaxis, in a prospective multicenter study of solid organ transplant recipients. J. Inf. Dis. 189, 1615–1618.
Bourgeois, C., Sixt, N., Bour, J.B., Pothier, P., 1997. Value of a ligase chain reaction assay for detection of ganciclovir resistance-related mutation 594 in UL97 gene of human cytomegalovirus. J. Virol. Methods 67, 167–175.
Chevillotte, M., Schubert, A., Mertens, T., von Einem, J., 2009. A fluorescence-based assay for phenotypic characterisation of human cytomegalovirus polymerase mutations regarding drug susceptibility and viral replicative fitness. Antimicrob. Agents Chemother. 53, 3752–3761.
Chou, S., 2008. Cytomegalovirus UL97 mutations in the era of ganciclovir and marib-avir. Rev. Med. Virol. 18, 233–246.
Chou, S., 2009. Diverse cytomegalovirus UL27 mutations adapt to loss of viral UL97 kinase activity under maribavir. Antimirob. Agents Chemother. 53, 81–85. Chou, S., Marousek, G.I., 2008. Accelerated evolution of maribavir resistance in a
cytomegalovirus exonuclease domain II mutant. J. Virol. 82, 246–253. Chou, S., Marousek, G.I., Senters, A.E., Davis, M.G., Biron, K.K., 2004. Mutations in the
human cytomegalovirus UL27 gene that confer resistance to maribavir. J. Virol. 78, 7124–7130.
Chou, S., Marousek, G.I., Van Wechel, L.C., Li, S., Weinberg, A., 2007. Growth and drug resistance phenotypes resulting from cytomegalovirus DNA polymerase region III mutations observed in clinical specimens. Antimicrob. Agents Chemother. 51, 4160–4162.
Chou, S.W., 1999. Antiviral drug resistance in human cytomegalovirus. Transpl. Infect. Dis. 1, 105–114.
Chou, S.W., Erice, A., Jordan, M.C., Vercellotti, G.M., Michels, K.R., Talarico, C.L., Stanat, S.C., Biron, K.K., 1995a. Analysis of the UL97 phosphotransferase coding sequence in clinical cytomegalovirus isolates and identification of mutations conferring ganciclovir resistance. J. Infect. Dis. 171, 576–583.
Chou, S.W., Guentzel, S., Michels, K.R., Miner, R.C., Drew, W.L., 1995b. Frequency of UL97 phosphotransferase mutations related to ganciclovir resistance in clinical cytomegalovirus isolates. J. Infect. Dis. 172, 239–242.
Chou, S.W., Lurain, N.S., Thompson, K.D., Miner, R.C., Drew, W.L., 2003. Viral DNA polymerase mutations associated with drug resistance in human cytomegalovirus. J. Infect. Dis. 188, 32–39.
Chou, S.W., Marousek, G., Guentzel, S., Follansbee, S.E., Poscher, M.E., Lalezari, J.P., Miner, R.C., Drew, W.L., 1997. Evolution of mutations conferring multidrug resis-tance during prophylaxis and therapy for cytomegalovirus disease. J. Infect. Dis. 176, 786–789.
Chou, S.W., Miner, R.C., Drew, W.L., 2000. A deletion mutation in region V of the cytomegalovirus DNA polymerase sequence confers multidrug resistance. J. Infect. Dis. 182, 1765–1768.
Chou, S.W., van Wechel, L.C., Lichy, H.M., Marousek, G., 2005. Phenotyping of cytomegalovirus drug resistance mutations by using recombinant viruses incor-porating a reporter gene. Antimicrob. Agents Chemother. 49, 2710–2715. Chrisp, P., Clissold, S.P., 1991. Foscarnet. A review of its antiviral activity,
pharma-cokinetic properties and therapeutic use in immunocompromised patients with cytomegalovirus retinitis. Drugs 41, 104–129.
Cihlar, T., Chen, M.S., 1996. Identification of enzymes catalyzing two-step phos-phorylation of cidofovir and the effect of cytomegalovirus infection on their activities in host cells. Mol. Pharmacol. 50, 1502–1510.
Cihlar, T., Fuller, M.D., Cherrington, J.M., 1998a. Characterization of drug resistance-associated mutations in the human cytomegalovirus DNA polymerase gene by using recombinant mutant viruses generated from overlapping DNA fragments. J. Virol. 72, 5927–5936.
Cihlar, T., Fuller, M.D., Mulato, A.S., Cherrington, J.M., 1998b. A point mutation in the human cytomegalovirus DNA polymerase gene selected in vitro by cidofovir confers a slow replication phenotype in cell culture. Virology 248, 382–393.
Dal Pozzo, F., Andrei, G., Daelemans, D., Winkler, M., Piette, J., De Clercq, E., Snoeck, R., 2008. Fluorescence-based antiviral assay for the evaluation of compounds against vaccinia virus, varicella zoster virus and human cytomegalovirus. J. Virol. Methods 151, 66–73.
Drew, W.L., 2000. Ganciclovir resistance: a matter of time and titre. Lancet 356, 609–610.
Drew, W.L., 2007. Laboratory diagnosis of cytomegalovirus infection and disease in immunocompromised patients. Curr. Opin. Infect. Dis. 20, 408–411.
Drew, W.L., Miner, R.C., Marousek, G., Chou, S.W., 2006. Maribavir sensitivity of cytomegalovirus isolates resistant to ganciclovir, cidofovir or foscarnet. J. Clin. Virol. 37, 124–127.
Ducancelle, A., Alain, S., Petit, F., Sanson Le Pors, M.J., Mazeron, M.C., 2007. Development and validation of a non-radioactive DNA polymerase assay for studying cytomegalovirus resistance to foscarnet. J. Virol. Methods 141, 212–215.
Ducancelle, A., Gravisse, J., Alain, S., Fillet, A.M., Petit, F., Sanson Le Pors, M.J., Mazeron, M.C., 2005. Phenotypic characterisation of cytomegalovirus DNA polymerase: a method to study cytomegalovirus isolates resistant to foscarnet. J. Virol. Meth-ods 125, 145–151.
Eckle, T., Lang, P., Prix, L., Jahn, G., Klingebiel, T., Handgretinger, R., Selle, B., Nietham-mer, D., Hamprecht, K., 2002. Rapid development of ganciclovir-resistant cytomegalovirus infection in children after allogeneic stem cell transplanta-tion in the early phase of immune cell recovery. Bone Marrow Transplant. 30, 433–439.
Eckle, T., Prix, L., Jahn, G., Klingebiel, T., Handgretinger, R., Selle, B., Hamprecht, K., 2000. Drug-resistant human cytomegalovirus infection in children after allo-geneic stem cell transplantation may have different clinical outcomes. Blood 96, 3286–3289.
Egli, A., Binggeli, S., Bodaghi, S., Dumoulin, A., Funk, G.A., Khanna, N., Leuenberger, D., Gosert, R., Hirsch, H.H., 2007. Cytomegalovirus and polyomavirus BK post-transplant. Nephrol. Dial. Transplant. 22, viii72–viii82.
Einsele, H., Ehninger, G., Hebart, H., Wittkowski, K.M., Schuler, U., Jahn, G., Mackes, P., Herter, M., Klingebiel, T., Loffler, J., 1995. Polymerase chain reaction moni-toring reduces the incidence of cytomegalovirus disease and the duration and side effects of antiviral therapy after bone marrow transplantation. Blood 86, 2815–2820.
Emery, V.C., Griffiths, P.D., 2000. Prediction of cytomegalovirus load and resistance patterns after antiviral chemotherapy. Proc. Natl. Acad. Sci. U.S.A. 97, 8039– 8044.
Erice, A., Borrell, N., Li, W., Miller, W.J., Balfour Jr., H., 1998. Ganciclovir susceptibil-ities and analysis of UL97 region in cytomegalovirus (CMV) isolates from bone marrow recipients with CMV disease after antiviral prophylaxis. J. Infect. Dis. 178, 531–534.
Erice, A., Gil-Roda, C., Pérez, J.L., Balfour, H.H., Sannerud, K.J., Hanson, M.N., Boivin, G., Chou, S.W., 1997. Antiviral susceptibilities and analysis of UL97 and DNA polymerase sequences of clinical cytomegalovirus isolates from immunocom-promised patients. J. Infect. Dis. 175, 1087–1092.
Faizi Khan, R., Mori, S., Eizuru, Y., Kumura Ishii, K., Minamishima, Y., 1998. Genetic analysis of a ganciclovir-resistant human cytomegalovirus mutant. Antiviral Res. 40, 95–103.
Gilbert, C., Boivin, G., 2005a. Human cytomegalovirus resistance to antiviral drugs. Antimicrob. Agents Chemother. 49, 873–883.
Gilbert, C., Boivin, G., 2005b. New reporter cell line to evaluate the sequential emergence of multiple human cytomegalovirus mutations during in vitro drug exposure. Antimicrob. Agents Chemother. 49, 4860–4866.
Goossens, V.J., Wolffs, P.F., van, L.I., Bruggeman, C.A., Verbon, A., 2009. CMV DNA levels and CMV gB subtypes in ART-naive HAART-treated patients: a 2-year follow-up study in The Netherlands. AIDS 23, 1425–1429.
Hertenstein, B., Hampl, W., Bunjes, D., Wiesneth, M., Duncker, C., Koszinowski, U., Heimpel, H., Arnold, R., Mertens, T., 1995. In vivo/ex vivo T cell depletion for GVHD prophylaxis influences onset and course of active cytomegalovirus infec-tion and disease after BMT. Bone Marrow Transplant. 15, 387–393.
Ijichi, O., Michel, D., Mertens, T., Miyata, K., Eizuru, Y., 2002. GCV resistance due to the mutation A594P in the cytomegalovirus protein UL97 is partially reconstituted by a second mutation at D605E. Antiviral Res. 53, 135–142.
Iwasenko, J.M., Scott, G.M., Rawlinson, W.D., Keogh, A., Mitchell, D., Chou, S., 2009. Successful valganciclovir treatment of post-transplant cytomegalovirus infec-tion in the presence of UL97 mutainfec-tion N597D. J. Med. Virol. 81, 507–510. Jabs, D.A., Enger, C., Dunn, J.P., 1998a. Cytomegalovirus retinitis and viral resistance:
ganciclovir resistance. J. Infect. Dis. 177, 770–773.
Jabs, D.A., Enger, C., Forman, M., Dunn, J.P., 1998b. Incidence of foscarnet resis-tance and cidofovir resisresis-tance in patients treated for cytomegalovirus retinitis. Antimicrob. Agents Chemother. 42, 2240–2244.
Julin, J.E., van Burik, J.H., Krivit, W., Webb, C., Holman, C.J., Clark, H.B., Balfour Jr., H.H., 2002. Ganciclovir-resistant cytomegalovirus encephalitis in a bone marrow transplant recipient. Transpl. Infect. Dis. 4, 201–206.
Kedhar, S.R., Jabs, D.A., 2007. Cytomegalovirus retinitis in the era of highly active antiretroviral therapy. Herpes 14, 66–71.
Komazin, G., Ptak, R.G., Emmer, B.T., Townsend, L.B., Drach, J.C., 2003. Resistance of human cytomegalovirus to the benzimidazole L-ribonucleoside maribavir maps to UL27. J. Virol. 77, 11499–11506.
Landry, M.L., Stanat, S., Biron, K., Brambilla, D., Britt, W., Jokela, J., Chou, S., Drew, W.L., Erice, A., Gilliam, B., Lurain, N., Manischewitz, J., Miner, R., Nokta, M., Reichelderfer, P., Spector, S., Weinberg, A., Yen-Lieberman, B., Crumpacker, C., A.C.T.G.C.M.V.R.W.G., 2000. A standardized plaque reduction assay for determi-nation of drug susceptibilities of cytomegalovirus clinical isolates. Antimicrob. Agents Chemother. 44, 688–692.
Limaye, A.P., Corey, L., Koelle, D.M., Davis, C.L., Boeckh, M., 2000. Emergence of ganciclovir-resistant cytomegalovirus disease among recipients of solid-organ transplants. Lancet 356, 645–649.
Luganini, A., Caposio, P., Mondini, M., Landolfo, S., Gribaudo, G., 2008. New cell-based indicator assays for the detection of human cytomegalovirus infection
and screening of inhibitors of viral immediate-early 2 protein activity. J. Appl. Microbiol. 105, 1791–1801.
Lurain, N.S., Thompson, K.D., Holmes, E.W., Read, S., 1992. Point mutations in the DNA polymerase gene of human cytomegalovirus that result in resistance to antiviral agents. J. Virol. 66, 7146–7152.
Marfori, J., Exner, M.M., Marousek, G.I., Chou, S., Gilbert, C., 2007. Development of new cytomegalovirus UL97 and DNA polymerase mutations conferring drug resistance after valganciclovir therapy in allogenic stem cell recipients. J. Clin. Virol. 38, 120–125.
Marschall, M., Freitag, M., Weiler, S., Sorg, G., Stamminger, T., 2000. Recombi-nant green fluorescent protein-expressing human cytomegalovirus as a tool for screening antiviral agents. Antimicrob. Agents Chemother. 44, 1588–1597. Martin, M., Gilbert, C., Covington, E., Boivin, G., 2006. Characterization of human
cytomegalovirus (HCMV) UL97 mutations found in a valganciclovir/oral ganci-clovir prophylactic trial by use of a bacterial artificial chromosome containing the HCMV genome. J. Infect. Dis. 194, 579–583.
Michel, D., Lanz, K., Michel, M., Wasner, T., Hauser, I., Just, M., Hampl, W., Mertens, T., Prösch, S., Cinatl, J., Scholz, M., 2003. Fast Genotypic Identification and Esti-mation of Ganciclovir-resistant Cytomegalovirus from Clinical Specimens, New Aspects of CMV-related Immunopathology. Karger, Basel, pp. 160–170. Michel, D., Schaarschmidt, P., Wunderlich, K., Heuschmid, M., Simoncini, L.,
Mühlberger, D., Zimmermann, A., Pavic, I., Mertens, T., 1998. Functional regions of the human cytomegalovirus protein pUL97 involved in nuclear localization and phosphorylation of ganciclovir and pUL97 itself. J. Gen. Virol. 79, 2105– 2112.
Mousavi-Jazi, M., Schloss, L., Drew, W.L., Linde, A., Miner, R.C., Harmenberg, J., Wahren, B., Brytting, M., 2001. Variations in the cytomegalovirus DNA poly-merase and phosphotransferase genes in relation to foscarnet and ganciclovir sensitivity. J. Clin. Virol. 23, 1–15.
Müller, B., Kräusslich, H.G., 2009. Antiviral strategies. Handb. Exp. Pharmacol. 189, 1–24.
Nijhuis, M., van Maarseveen, N.M., Boucher, C.A.B., 2009. Antiviral resistance and impact on viral replication capacity: Evolution of viruses under antiviral pres-sure occurs in three phases. Handb. Exp. Pharmacol. 189, 299–320.
Oshima, K., Kanda, Y., Kako, S., sano-Mori, Y., Watanabe, T., Motokura, T., Chiba, S., Shiraki, K., Kurokawa, M., 2008. Case report: persistent cytomegalovirus (CMV) infection after haploidentical hematopoietic stem cell transplantation using in vivo alemtuzumab: emergence of resistant CMV due to mutations in the UL97 and UL54 genes. J. Med. Virol. 80, 1769–1775.
Palella Jr., F.J., Delaney, K.M., Moorman, A.C., Loveless, M.O., Fuhrer, J., Satten, G.A., Aschman, D.J., Holmberg, S.D., 1998. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpa-tient Study Investigators. N. Engl. J. Med. 338, 853–860.
Reusser, P., Cordonnier, C., Einsele, H., Engelhard, D., Link, D., Locasciulli, A., Ljung-man, P., 1996. European survey of herpesvirus resistance to antiviral drugs in bone marrow transplant recipients. Infectious Diseases Working Party of the European Group for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant. 17, 813–817.
Reusser, P., Einsele, H., Lee, J., Volin, L., Rovira, M., Engelhard, D., Finke, J., Cordonnier, C., Link, H., Ljungman, P., 2002. Randomized multicenter trial of foscarnet versus ganciclovir for preemptive therapy of cytomegalovirus infection after allogeneic stem cell transplantation. Blood 99, 1159–1164.
Ronaghi, M., Uhlén, M., Nyrén, P., 1998. A sequencing method based on real-time pyrophosphate. Science 281, 363–365.
Schnepf, N., Boiteau, N., Petit, F., Alain, S., Sanson-Le Pors, M.-J., Mazeron, M.C., 2009. Rapid determination of antiviral drug susceptibility of human cytomegalovirus by real-time PCR. Antiviral Res. 81, 64–67.
Schreiber, A., Härter, G., Schubert, A., Bunjes, D., Mertens, T., Michel, D., 2009. Antivi-ral treatment of cytomegalovirus infection and resistant strains. Expert Opin. Pharmacother. 10, 191–209.
Scott, G.M., Weinberg, A., Rawlinson, W.D., Chou, S.W., 2007. Multidrug resistance conferred by novel DNA polymerase mutations in human cytomegalovirus iso-lates. Antimicrob. Agents Chemother. 51, 89–94.
Sia, I.G., Patel, R., 2000. New strategies for prevention and therapy of cytomegalovirus infection and disease in solid-organ transplant recipients. Clin. Microbiol. Rev. 13, 83–121.
Sinzger, C., Hahn, G., Digel, M., Katona, R., Sampaio, K.L., Messerle, M., Hengel, H., Koszinowski, U., Brune, W., Adler, B., 2008. Cloning and sequencing of a highly productive, endotheliotropic virus strain derived from human cytomegalovirus TB40/E. J. Gen. Virol. 89, 359–368.
Smith, I., Cherrington, J.M., Jiles, R.E., Fuller, M.D., Freeman, W.R., 1997. High-level resistance of cytomegalovirus to ganciclovir is associated with alterations in both the UL97 and DNA polymerase genes. J. Infect. Dis. 176, 69–77. Springer, C.L., Chou, S.W., Li, S., Giller, R.H., Quinones, R., Shira, J.E., Weinberg,
A., 2005. How evolution of mutations conferring drug resistance affects viral dynamics and clinical outcomes of cytomegalovirus-infected hematopoietic cell transplant recipients. J. Clin. Microbiol. 43, 208–213.
Sullivan, V., Talarico, C.L., Stanat, S.C., Davis, M., Coen, D.M., Biron, K.K., 1992. A protein kinase homologue controls phosphorylation of ganciclovir in human cytomegalovirus-infected cells. Nature 358, 162–164.
Sun, H.Y., Wagener, M.M., Singh, N., 2008. Prevention of posttransplant cytomegalovirus disease and related outcomes with valganciclovir: a systematic review. Am. J. Transplant. 8, 2111–2118.
Tchesnokov, E.P., Gilbert, C., Boivin, G., Götte, M., 2006. Role of helix P of the human cytomegalovirus DNA polymerase in resistance and hypersusceptibility to the antiviral drug foscarnet. J. Virol. 80, 1440–1450.
ter Meulen, C.G., Wetzels, J.F.M., Hilbrands, L.B., 2000. The influence of mycopheno-late mofetil on the incidence and severity of primary cytomegalovirus infections and disease after renal transplantation. Nephrol. Dial. Transplant. 15, 711–714. Tischer, B.K., von Einem, J., Kaufer, B., Osterrieder, N., 2006. Two-step Red-mediated recombination for versatile high-efficiency markerless DNA manipulation in Escherichia coli. BioTechniques 40, 191–197.
Ueno, T., Eizuru, Y., Katano, H., Kurata, T., Sata, T., Irie, S., Ogawa-Goto, K., 2006. Novel real-time monitoring system for human cytomegalovirus-infected cells in vitro that uses a green fluorescent protein-PML-expressing cell line. Antimicrob. Agents Chemother. 50, 2806–2813.
Ueno, T., Ogawa-Goto, K., 2009. Use of a GFP-PML-expressing cell line as a biosensor for human cytomegalovirus infection. Methods Mol. Biol. 515, 33–44. Vigano, M., Dengler, T., Mattei, M.F., Poncelet, A., Vanhaecke, J., Vermes, E., Kleinloog,
R., Li, Y., Gezahegen, Y., Delgado, J.F., 2009. Lower incidence of cytomegalovirus infection with everolimus versus mycophenolate mofetil in de novo
cardiac transplant recipients: a randomized, multicenter study. Transpl. Infect. Dis.
von Müller, L., Schliep, C., Storck, M., Hampl, W., Schmid, T., Abendroth, D., Mertens, T., 2006. Severe graft rejection, increased immunosuppression, and active CMV infection in renal transplantation. J. Med. Virol. 78, 394–399.
Warming, S., Costantino, N., Court, D., Jenkins, N.A., Copeland, N.G., 2005. Simple and highly efficient BAC recombineering using galK selection. Nucleic Acids Res. 33, e36.
Weinberg, A., Jabs, D.A., Chou, S.W., Martin, B.K., Lurain, N.S., Forman, M.S., Crumpacker, C.S., 2003. Mutations conferring foscarnet resistance in a cohort of patients with acquired immunodeficiency syndrome and cytomegalovirus retinitis. J. Infect. Dis. 187, 777–784.
Wolf, D.G., Yaniv, I., Honigman, A., Kassis, I., Schonfeld, T., Ashkenazi, S., 1998. Early emergence of ganciclovir-resistant human cytomegalovirus strains in children with primary combined immunodeficiency. J. Infect. Dis. 178, 535–538.