Original Article
Carglumic acid promotes apoptosis and
suppresses cancer cell proliferation in vitro and
in vivo
Chun-Te Chen1*, Yi-Chun Chen1*, Hirohito Yamaguchi1, Mien-Chie Hung1,2,3
1Department of Molecular and Cellular Oncology, The University of Texas MD Anderson
Cancer Center, Houston, Texas 77030, USA; 2Center for Molecular Medicine and Graduate
Institute of Cancer Biology, China Medical University, Taichung 404, Taiwan; 3Department of
Biotechnology, Asia University, Taichung 413, Taiwan. *Equal contributors.
Abstract: Drug repurposing is a therapeutic strategy that applies drugs to treat different diseases based on new therapeutic function. Carglumic acid (Carbaglu; Orphan Europe) is an orphan drug approved by the FDA for hyperam- monemia. Administration of carglumic acid for treatment of hyperammonemia has few side effects and has been used for 10 years to effectively treat hyperammonemia symptoms of both adult and pediatric patients. Here, we tested the potential of carglumic acid to be repurposed as an anticancer agent and showed that carglumic acid promotes apoptosis and inhibits cancer cell growth ina wide variety of human cancers, including pancreatic ductal adenocarcinoma, triple-negative breast cancer (TNBC), hepatoma, and lung cancer. Our data from in vivo models indicates that orally taking 10% of the carglumic acid dose currently used for the treatment of hyperammonemia ise ffective to suppress the growth of pancreatic ductal adenocarcinomaand TNBC. If given intravenously, only 5% of the carglumic acid doseis needed to be effective against TNBC. These findings suggest that carglumic acid may serve as a safe and effective therapeutic to treat both TNBC and pancreatic cancer.
Keywords: Carbaglu, carglumic acid, urea cycle disorder, drug repurposing
Introducti on
The practice of drug repurposing, which is a strategy of using a drug to treat a condition other than that for which the drug was originally approved, has become more common in cur- rent decade [1]. Drug repurposing is also known as drug repositioning, reprofiling, and therapeu-tic switching which have proven to be success- ful approaches for repurposing existing drugs for new indications. For example, thalidomide, an immunomodulatory drug, was successfully repurposed to treat cancer, and miltefosine, originally approved as an anticancer drug, was repurposed to treat visceral leishmaniasis [2]. One of the main advantages of drug repurpos- ing is that the drugs of interest have already been approved by the U.S. Food and Drug Administrationand are
known to be safe. In addition, repurposed drugscan bypass the early drug development stages, thereby reduc- ingthe time and cost of research and develop- ment [3].
In this study, we tested the potential of carglu- mic acid (Carbaglu; Orphan Europe), an orphan drug that was approved in 2010 by the U.S. Food and Drug Administration for treatment of hyperammonemia, to be repurposed as an anti- cancer agent [4-6]. Hyperammonemia is a dis- order of the urea cycle, a biochemical reaction that eliminates ammonia in humans and other mammals by converting it into urea. Urea cycle disorder is caused by genetic deficiencies in urea cycle enzymes or liver function failure, resulting in excess ammonia in the human body. Ammonia is highly toxic and can causese- rious harm to the human body, especially to the brain [7, 8]. The first enzymein the urea cycle to process excess ammonia is carbamoyl phos- phate synthetase 1 (CPS1). CPS1 can be acti- vated only by N-acetylglutamate (NAG), which is synthesized from glutamate and acetyl coen- zymeA by NAG synthase (NAGS). Inactivation of NAGS reduces cellular NAG levels, which causes CPS1 inactivation and hyperammonemia [9,
10]. Carglumic acid, a functional analogue of NAG and a CPS1 activator, is used to treat acute and chronic hyperammonemia associat- ed with NAGS deficiency.
In seeking to assess the potential of carglumic acid to be repurposed as an anticancer agent, we were guided in part by the example of sodi- um phenylbutyrate (PB). PB facilitates an alter- native pathway for excretion of excess ammo- nia and has been used to treat urea cycle dis- order for over a decade [11, 12]. PB functions as a histone deacetylase inhibitor [13-15], which is distinct from carglumic acid. However, both PB and carglumic acid are able to reduce ammonemia. PB has been shown to induce apoptosis and cell cycle arrest and associate with anticancer activity [13]. Although it is not yet known whether the anticancer activity of PB is due to urea cycle activation, weasked wheth- ercarglumic acid might also possess anti can- cer activity.
To this end, we tested the activity of carglumic acid against 19 human cancer cell lines, includ- ing human pancreatic ductal adenocarcinoma (PDAC), human triple-negative breast cancer, human hepatoma, and human non-small cell lung carcinoma cell lines. We also tested the activity of carglumic acid in orthotopic mouse models of human pancreatic and breast can- cer. This work demonstrates a novel anticancer function of carglumic acid, with less toxicity than that of chemotherapeutic agents. Carglu- mic acid therefore may represent an effective alternative for cancer treatment.
Materials and methods
Drug s
Carglumic acid and paclitaxel were purchas- ed from Sigma-Aldrich (St. Louis, MO, USA). Gemcitabine was
obtained from the Department of Pharmacy of The University of Texas MD Anderson Cancer Center (Houston, TX, USA).
Cell lines
The human pancreatic
adenocarcinoma cell lines Capan1 and AsPc1/luc; murine pancreat- ic adenocarcinoma cell line PanO2/luc; human triple-negative breast cancer cell lines MDA- MB-231, MDA-MB-468, and HS578T; murine triple-negative breast cancer cell line 4T1;
human hepatoma cell lines Hu7,
HepG2, Hep3B, HA22T/VGH,
HA59T/VGH, PCL/PRF/5, TONG, SK-Hep-1, and Mahlavu; and human lung cancer cell lines PC9 and H1299 were maintained in Dulbecco modified Eagle/F12 medium supplemented with 10% fetal bovine serum. Human papillomavirus type 16 E6E7-immortalized human pancreatic ductal epithe- lial cells (HPDE-E6E7 cells) were maintained in keratinocyte serum-free medium. The breast epithelial cell line MCF-12A was maintained in Ham’s F12/Dulbecco modified Eagle medium- supplemented with 5% horse serum, penicillin (50 U ml-1), streptomycin (50 U ml-1), epidermal growth factor (20 ng ml-1), insulin (10 μg ml-1), cholera toxin (1 ng ml-1), and hydrocortisone. AsPc1/luc and PanO2/luc cells with stable luciferase expression were maintained in a cul- ture medium containing G418. Cell lines were validated by short tandem repeat DNA finger- printing using the AmpFISTR Identifiler PCR Amplification Kit (Applied Biosystems; cata- logue no. 4322288) according to the manufac- turer’s instructions.
Cell viability
assay
Cell viability was evaluated by MTT (3-(4,5- dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide) assay [16]. In brief, various cancer cell lines were seeded (1 x 104 cells/well) in a
96-well plate and treated with different doses of carglumic acid, paclitaxel, or gemcitabine. After 48 h, 50 μl of MTT solution per well (stock solution concentration 5 mg/ml; Sigma-Aldrich) was added to each well, and the cells were incubated for 2 h more, followed by addition of
100 μl of dimethyl sulfoxide (Sigma-Aldrich) to each well. Absorbance at 570 nm was mea- sured immediately using a multiwell scanner (Labsystems, Helsinki, Finland).
Cell cycle
assay
After cells were treated with different doses of carglumic acid for 48 h, they were detached by trypsin-EDTA and washed with phosphate-buff- ered saline. The cells were suspended in 0.5 ml of phosphate-buffered saline and fixed with 4.5 ml of 70% ethanol. After removal of ethanol and a wash with phosphate-buffered saline, the cells were mixed with 500 μl of 0.1 mg/ml prop- idium iodide (P4170, Sigma) and 500 μl of 2 mg/kg RNase (R5125, Sigma-Aldrich) staining
Figure 1. Effect of carglumic acid on viability of pancreatic cancer cells. Human pancreatic cancer cell lines were treated with the indicated doses of carglumic acid. Cell viability (absorbance at 570 nm) was determined by MTT assay. The viability of untreated cells (control) was assigned a value of 100%. Each samplewas tested in triplicate.
Figure 2. Effect of carglumic acid on viability of triple-negative breast cancer cells. Breast cancer cell lines were treated with the indicated doses of carglumic acid. Cell viability (absorbance at 570 nm) was determined by MTT assay. The viability of untreated cells (control) was assigned a value of 100%. Each sample was tested in triplicate.
solution at room temperature in the dark for
45 min. DNA content profiles were evaluated with a BD FACSCanto II cell analyzer (BD Im- munocytometry
Systems; BD Biosciences, San Jose, CA, USA).
Caspase activity assay
Caspase activity was measured by using a fluo- rimetric caspase-3 assay kit (CASP3F, Sigma- Aldrich). In brief, cells that were treated with
Figure 3. Effect of carglumic acid on viability of hepatoma cancer cells. Humanhepatoma cancer cell lines were treated with the indicated doses of carglumic acid. Cell viability (absorbance at 570 nm) was determined by MTT assay. The viability of untreated cells (control) was assigned a value of 100%. Each sample was tested in triplicate.
carglumic acid or that were left untreated were lysed in a lysis buffer, and 50 μg of protein ly- sate was incubated with Ac-DEVD-AMC (N-ace-tyl-Asp- Glu-Val-Asp-7-amino-4-methylcouma- rin) substrate in the assay buffer for 1 h. The resultant fluorescence signals were read by using a fluorometer (excitation 360 nm, emis- sion 460 nm), and the results were tabulated as fold changes relative to the untreated con- trol cells.
Mouse studies
For orthotopic cancer models, AsPC1/luc hu- man pancreatic cancer cells (1 x 106) were injected into the pancreas of nude mice or MDA-MB-231
human triple-negative breast cancer cells (3 x 106) were injected into the mammary fat pad of nude mice [17]. Carglumic
acid was administered to mice 5 days after tumor inoculation in the pancreatic cancer model and 7 days after tumor inoculation in the triple-negative breast cancer model. Tumor-bearing mice received acarglumic aciddose of
120 mg/kg orally every day for 10 days, 60 mg/kg orally three times per week for 2 weeks, or 60 mg/kg intravenously three times per week for 2 weeks. A 120-mg/kg/day dose of carglumic acid in mice isequivalent to a 10-mg/ kg/daydose in humans, which is 10% of the maintenance therapy dose of carglumic acid for hyperammonemia patients [18]. Tumor volume was determined by measuring luciferase sig- nals using the IVIS invivo imaging system (Xenogen, Alameda, CA, USA) in the pancreatic cancer model. All animal procedures were con- ducted in accordance with the regulations of the Department of Veterinary Medicine and
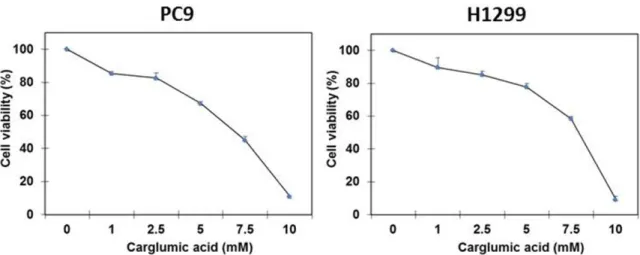
Figure 4. Effect of carglumic acid on viability of lung cancer cells. Human non-small cell lungcancer cell lines were treated with the indicated doses of carglumic acid. Cell viability (absorbance at 570 nm) was determined by MTT assay. The viability of untreated cells (control) was assigned a value of 100%. Each sample was tested in triplicate.
Figure 5. Carglumic acid inducesapoptosis in cancer cells. AsPC1 and MDA-MB-231 cells were treated with the indicated doses of carglumic acid. Treated and untreated (0 mM) cancer cells were stained with propidium iodide to evaluate cell apoptosis. A. Percent sub-G1-phase cells among AsPC1 cells. B. Percent sub-G1-phase cells among MDA-MB-231 cells. C. Caspase-3 activity in AsPC1 cells. Each sample was tested in triplicate.
Surgeryat The University of Texas MD Anderson
Cancer Center. The protocol (protocol no.
190511133) was reviewed and approved by the Institutional Animal Care and Use Com- mittee of The University of Texas MD Anderson Cancer Center.
Result s
Carglumic acid inhibits cancer cell growth
To test the therapeutic effect of carglumic acid in human cancers, we first determined the cyto- toxic effect of carglumic acid in variouscancer cell lines. Carglumic acid suppressed cell viabil- ity in the pancreatic ductal adenocarcinoma
cell lines (Figure 1), triple-negative breast can- cercell lines (Figure 2), hepatomacell lines (Figure 3), and human non-small cell lung carcinoma cell lines (Figure 4) in adose-depen-dent manner. The 50% inhibitory concentration (IC ) of carglumic acid against those cell lines was between 5 and 7.5 mM, suggesting that carglumic acid potently suppressed cancer cell growth.
Carglumic acid inhibits cancer cell prolifera- tion andinduces apoptosis
To further validate the antiproliferation activity ofcarglumic acid in cancer cells, we performed fluorescence-activated cell sorting analysis.
Figure 6. Carglumic acid is less cytotoxic than gemcitabine and paclitaxel in normal epithelial cells and is less toxic to normal epithelial cells than to cancer cells. The pancreatic ductal epithelial cell line HPDE-E6E7 and the human pancreatic ductal adenocarcinoma cell line AsPC1 were treated with carglumic acid or gemcitabine. The normal breast epithelial cell line MCF-12A and the triple-negative breast cancer cell line MDA-MB-231 were treated with carglumic acid or paclitaxel. Cell viability (absorbance at 570 nm) was determined by MTT assay. The viability of untreated cells (0 mM or 0 μM) was assigned a value of 100%. A. Effects of carglumic acid onviability of HPDE-E6E7 and AsPC1 cells. B. Effects of gemcitabine on viability of HPDE-E6E7 and AsPC1 cells. C. Effects of carglumic acid on viability of MCF-12A and MDA-MB-231 cells. D. Effects of paclitaxel on viability of MCF-12A and MDA-MB-231 cells. Each sample was tested in triplicate.
Carglumic acid-treated and untreated cancer cells were stained with propidium iodide to determine DNA contents in AsPC1 and MDA- MB-231. In addition to revealing cell cycle sta-tus, this assay can be used to assess cell death by analysis of DNA fragmentation [19]. The results showed that carglumic acid did not induce complete cell cycle arrest. Instead, we observed more sub-G1 cells among carglumic acid-treated AsPC1 and MDA-MB-231 cells than among untreated cells, indicating that cell death occurred in response to carglumic acid. Sub-G1 cells accounted for 1.6% and 26.3% of untreated and treated AsPC1 cells, respective- ly (Figure 5A), and for 1.8% and 12.8% of untreated and treated MDA-MB-231
cells, respectively (Figure 5B). In order to further determine whether cancer cells under go cell death through apoptosis after carglumic acid treatment, we measured caspase activity in
AsPC1 cells treated with carglumic acid. The results showed that caspase-3 activity increa- sed in a dose-dependent manner (Figure 5C). Together, these data suggest that carglumic acid inhibits cancer cell proliferation by induc- ing apoptosis.
Carglumic acid is a relatively safer
anti-cancer agent than
chemotherapeutic drugs
To determine whether carglumic acid cytotoxic- ity is specific to cancer cells, we determined the cytotoxic effect of carglumic acid in various human normal epithelial cells, including normal pancreatic ductal epithelial cells and normal breast epithelial cells. We also compared the cytotoxic effects of carglumic acid and chemo- therapeutic drugs between normal epithelial cell lines and cancer cell lines. The chemother- apeutic drugs we tested were paclitaxel and
Figure 7. Therapeutic efficacy of carglumic acid in orthotopic models of human pancreatic adenocarcinoma and triple-negative breast cancer. A. AsPC1/luc cells were inoculated into the pancreas in mice to generate human pancreatic adenocarcinoma. Starting at 5 days after cancer cell inoculation, mice were orally administered 120 mg/kg carglumic acidevery day for 10 days. B. MDA-MB-231 cells were inoculated into mouse mammary glands to generate human triple-negative breast cancer. Starting at 7 days after tumor inoculation, mice were orally adminis- tered 120 mg/kg carglumic acid every day for 10 days. C. The oral (PO) and intravenous (IV) routes of carglumic acid administration were compared in terms of tumor volume reduction in the orthotopictriple-negative breast cancer model. Tumor-bearing mice were treated with 60 mg/kg carglumic acid either orally or intravenously three times per week for 2 weeks. Arrows represent carglumic acid dose administrations. *P < 0.05; n = 5.
gemcitabine, which arecommonly used
to treat respectively (Figure 6C), and the IC s of
pacli-breast cancer and pancreatic cancer, respec- tively [20, 21]. The human pancreatic ductal epithelial cell line HPDE-E6E7 and human pan- creatic ductal adenocarcinoma cell line AsPC1 were treated with different concentrations of carglumic acid or gemcitabine. The normal breast epithelial cell line MCF-12A and triple-negative breast cancer cell line MDA-MB-231 were treated with different concentrations of carglumic acid or paclitaxel. In AsPC1 and
taxel were over 100 μM and 0.39 μM, respec- tively (Figure 6D). Thus, cancer cells are much more resistant to chemotherapeutics, e.g., gemcitabine and paclitaxel, than normal cells. Carglumic acid does not have this drawback as an anti-cancer drug as it inhibited proliferation of cancer cells slightly more effectively than that of normal cells. Therefore, carglumic acid is expected to be relatively safer than chemo- therapeutic drugs.
HPDE-E6E7 cells, the
IC s of carglumic acid
were 5 mM and over 10 mM,
respectively Carglumic acid inhibits tumor growth in vivo
(Figure 6A), and
the IC s of gemcitabine
were-over 100 μM and 1 μM, respectively (Figure
6B). In MDA-MB-231 and MCF-12A cells, the s of carglumic acid were 5 mM and 6 mM,
To test the therapeutic effect of carglumic acid in vivo, we established an AsPc1/luc orthotopic pancreatic cancer model and an MDA-MB-231 50
50
orthotopic triple-negative breast cancer model [16, 22]. Tumor-bearing mice were given 120 mg/kg carglumic acid orally once a day for 10 days (1200 mg/kg/mouse total). We monitored tumor growth as described in Materials and Methods. The results showed that carglumic acid, but not the vehicle control, markedly inhibited tumor growth. In the orthotopic pan-creatic cancer model, tumor growth inhibition by carglumic acid on day 21 was 80% (Figure
7A, P < 0.01). In the orthotopic triple-negative breast cancer model, tumor growth inhibition by carglumic acid on day 20 was 82% (Figure
7B, P < 0.01). These results indicate that car- glumic acid suppresses tumor growth in pan- creatic cancer and triple-negative breast can- cer.
We also compared the anticancer effect of car- glumic acid administered orally with the anti- cancer effect of carglumic acid administered intravenously in the orthotopic triple-negative breast cancer model. Tumor-bearing mice were given 60 mg/kg carglumic acid by either oral administration or intravenous injection. The drug was given to mice three times per week for
2 weeks (360 mg/kg/mouse total). On day 20, mean tumor growth inhibition in orally and intravenously treated mice was 55% and 93%, respectively, relative to untreated mice (Figure 7C, P < 0.01). These results suggest that the dose of carglumic acid required to produce a >
80% reduction in triple-negative breast tumor volume by intravenous injection is one-third the dose required to produce the same effect by oral administration.
Discussio n
Drug repurposing offers the advantages of time and cost savings stemming from the fact that the drug being repurposed has already passed toxicity and safety testing and therefore has a
reduced chance of failure [23]. In this study, we found that carglumic acid, which is convention- ally used to treat hyperammonemia, has anti- cancer activity. We found that carglumic acid induced apoptosis in various cancer cells in vitro. Our results indicated that carglumic acid inhibits proliferation of human pancreatic can- cer, triple-negative breast cancer, hepatoma, and lung cancer cells by inducing apoptosis. Importantly, carglumic acid is a relatively safer anti-cancer agent than gemcitabine or
pacli-taxel, which is in agreement with the fact that no serious safety issue has been identified for the use of carglumic acid in treatment of hyper- ammonemia. Carglumic acid also demonstrat- ed potent antitumor activity in vivo in orthotopic mouse models of human pancreatic and breast cancer. Together, these findings demonstrate a novel anticancer function of carglumic acid, with less toxicity than that of chemotherapeutic agents. Carglumic acid therefore represents an effective alternative for cancer treatment.
Carglumic acid suppresses tumor growth and promotes cell apoptosis by activating caspase
3. The two major mechanisms of caspase cas- cade-associated apoptosis are an extrinsic sig- naling pathway involving the tumor necrosis factor receptor gene superfamily to conduct intracellular signaling pathways and an intrinsic mitochondrial pathway initiates non-receptor- mediated intracellular signals [24]. Further in-vestigation is required to distinguish the two mechanisms and to identify other potential mechanisms, such as dysregulation of cancer cell metabolism (see below), which may be associated with carglumic acid-mediated anti- cancer activities.
For the potential use of carglumic acid to treat cancer, intravenous injection offers a greater tumor volume reduction over than oral adminis-tration. Intravenous injection delivers the drug directly to the blood stream, by passing liver metabolism and facilitating essentially 100% bioavailability. Intravenous injection also avoids the side effects associated with irritation of the gastrointestinal tract by orally administered carglumic acid, such as vomiting, abdominal pain, and diarrhea [25, 26].
Since as an analog of NAG, carglumic acid acti- vates CPS1, the first enzyme and rate-limiting step of the urea cycle, hyperactivation of the urea cycle may result in dysregulation of cancer cell metabolism. Recently, it has been shown that cancer cells and normal cells have differ- ent metabolic
profiles, and these differences may render cancer cells more vulnerable [27]. The mechanism by which the activation of the urea cycle induces apoptosis in cancer cells warrants further investigation. In addition to playing a role in urea cycle regulation, CPS1 may play an important rolein suppressing can- cer cell growth by inducing cell apoptosis. Alternatively, activation of urea cycle by itself
may induce anti-cancer activities via dysregula- tion of cancer cell metabolism.
Acknowledgeme nts
We thank Arthur Gelmis from Scientific Publications at MD Anderson for editing the manuscript. This work was supported in part by National Institutes of Health (CA109311, CA099031, and Cancer Center Support Grant CA016672), the Center for Biological Pathways and the ShRNA and ORFeome Core Facility of MD Anderson Cancer Center, National Breast Cancer Foundation, Inc., the Breast Cancer Research Foundation, the Patel Memorial Breast Cancer Endowment Fund, The University of Texas MD Anderson Cancer Center Sister Institution Network Fund (M.-C. Hung), Ministry of Science and Technology, International Rese- arch-intensive Centers of Excellence in Taiwan (I-RiCE; MOST 104-2911-I-002-302), and Ministry of Health and Welfare, China Medical University Hospital Cancer Research Center of Excellence (MOHW104-TDU-B-212-124-002).
Disclosure of conflict of interest
M.-C. Hung, C.-T. Chen, and Y.-C. Chen are inventors on patents for carglumic acid as an anticancer drug.
Address correspondence to: Mien-Chie Hung, De- partment of Molecular and Cellular Oncology, The University of Texas MD Anderson Cancer Center,
1515 Holcombe Boulevard, Unit 108, Houston, TX
77030, USA. Tel: 713-792-3668; Fax:
713-794-3270; E-mail: mhu n g @md a nd e r s o n. or g
Referenc es
[1] Ashburn TT and Thor KB. Drug repositioning: identifying and
developing new uses for exist- ing drugs. Nat Rev Drug Discov 2004; 3:
673-683.
[2] Aronson JK. Old drugs--new uses. Br J Clin
Pharmacol 2007; 64: 563-565.
[3] Chong CR and Sullivan DJ Jr. New uses for old drugs. Nature 2007; 448: 645-646.
[4] Cartagena A, Prasad AN, Rupar CA, Strong M, Tuchman M, Ah Mew N and Prasad C. Recurrent encephalopathy: NAGS (N-acetylg- lutamate synthase) deficiency in adults. Can J Neurol Sci 2013; 40: 3-9.
[5] Haberle J. Role of carglumic acid in the tre- atment of acute hyperammonemia due to N-acetylglutamate synthase deficiency. Ther Clin Risk Manag 2011; 7: 327-332.
[6] Daniotti M, la Marca G, Fiorini P and Filippi L.
New developments in the treatment of hyper- ammonemia: emerging use of carglumic acid. Int J Gen Med 2011; 4: 21-28.
[7] Sedel F. [Inborn errors of metabolism in adu- lt neurology]. Rev Neurol (Paris) 2013; 169
Suppl 1: S63-69.
[8] Walterfang M, Bonnot O, Mocellin R and Velakoulis D. The neuropsychiatry of inborn er- rors of metabolism. J Inherit Metab Dis 2013; 36:
687-702.
[9] Ah Mew N and Caldovic L. N-acetylglutamate synthase deficiency: an insight into the genet- ics, epidemiology, pathophysiology, and treat- ment. Appl Clin Genet 2011; 4: 127-135.
[10] Martinez AI, Perez-Arellano I, Pekkala S, Barcelona B and Cervera J. Genetic, structural and biochemical basis of carbamoyl phos- phate synthetase 1 deficiency. Mol Genet Metab 2010; 101: 311-323.
[11] Wilcken B. Problems in the management of urea cycle disorders. Mol Genet Metab 2004;
81 Suppl 1: S86-91.
[12] Iannitti T and Palmieri B. Clinical and experi- mental applications of sodium phenylbutyrate. Drugs R D 2011; 11: 227-249.
[13] Zhang X, Wei L, Yang Y and Yu Q. Sodium
4-phenylbutyrate induces apoptosis of human lung carcinoma cells through activating JNK pathway. J Cell Biochem 2004; 93: 819-829.
[14] Shi MG, Huang Q, Dong J, Sun ZF and Lan Q. [Experimental study of combination therapy against human glioma xenograft by differentia- tion-inducing agent and cytotoxic chemothera- peutic drug]. Ai Zheng 2002; 21: 1090-1094.
[15] Lu YS, Chou CH, Tzen KY, Gao M, Cheng AL, Kulp SK and Cheng JC. Radiosensitizing effect of a phenylbutyrate-derived histone deacety- lase inhibitor in hepatocellular carcinoma. Int J Radiat Oncol Biol Phys 2012; 83: e181-189. [16] Chen CT, Yamaguchi H, Lee HJ, Du Y,
Lee HH, Xia W, Yu WH, Hsu JL, Yen CJ, Sun HL, Wang Y, Yeh ET, Hortobagyi GN and Hung MC. Dual tar- geting of tumor angiogenesis and
chemothera-py by endostatin-cytosine deaminase-uracil phosphoribosyltransferase. Mol Cancer Ther
2011; 10: 1327-1336.
[17] Chen CT, Du Y, Yamaguchi H, Hsu JM, Kuo HP, Hortobagyi GN and Hung MC. Targeting the IKKbeta/mTOR/VEGF signaling pathway as a potential therapeutic strategy for obesity-relat-ed breast cancer. Mol Cancer Ther 2012; 11:
2212-2221.
[18] Freireich EJ, Gehan EA, Rall DP, Schmidt LH and Skipper HE. Quantitative comparison of toxicity of anticancer agents in mouse, rat, hamster, dog, monkey, and man. Cancer Che- mother Rep 1966; 50: 219-244.
[19] Riccardi C and Nicoletti I. Analysis of apoptosis by propidium iodide staining and flow cytome- try. Nat Protoc 2006; 1: 1458-1461.
[20] Gluck S. nab-Paclitaxel for the treatment of ag- gressive metastatic breast cancer. Clin Breast Cancer 2014; 14: 221-7.
[21] Kleger A, Perkhofer L and Seufferlein T. Smar- ter drugs emerging in pancreatic cancer thera- py. Ann Oncol 2014; 25: 1260-70.
[22] Xie X, Xia W, Li Z, Kuo HP, Liu Y, Li Z, Ding Q, Zhang S, Spohn B, Yang Y, Wei Y, Lang JY, Evans DB, Chiao PJ, Abbruzzese JL and Hung MC. Targeted expression of BikDD eradicates pancreatic tumors in noninvasive imaging mo- dels. Cancer Cell 2007; 12: 52-65.
[23] DiMasi JA, Hansen RW, Grabowski HG and Lasagna L. Cost of innovation in the pharma- ceutical industry. J Health Econ 1991; 10:
107-142.
[24] Elmore S. Apoptosis: a review of programmed cell death. Toxicol Pathol 2007; 35: 495-516.
[25] Fotaki N. Pros and cons of methods used for the prediction of oral drug absorption. Expert Rev Clin Pharmacol 2009; 2: 195-208.
[26] Carbaglu. Orphan Europe 2010; prescribing information.
[27] Meadows AL, Kong B, Berdichevsky M, Roy S, Rosiva R, Blanch HW and Clark DS. Metabolic and morphological differences between rapid- ly proliferating cancerous and normal breast epithelial cells. Biotechnol Prog 2008; 24: