Research article 1
Study design: Intraarticular injection of hyaluronan versus saline in the treatment of 2
adjuvant-induced arthritis: a randomized controlled trial 3
4
Hyaluronan Modulates Accumulation of Hypoxia-Inducible Factor-1 alpha, Inducible 5
Nitric Oxide Synthase, and Matrix Metalloproteinase-3 in the Synovium of Rat 6
Adjuvant-Induced Arthritis Model 7
8
Li-Wei Chou, 1,2,3 John Wang, 4,5 Pei-Lin Chang,1 Yueh-Ling Hsieh1* 9
10
1 Department of Physical Therapy, Graduate Institute of Rehabilitation Science, China 11
Medical University, Taichung, Taiwan, Republic of China 12
2Department of Physical Medicine and Rehabilitation, China Medical University Hospital, 13
Taichung, Taiwan, Republic of China 14
3School of Chinese Medicine, China Medical University, Taichung, Taiwan, Republic of 15
China 16
4Department of Pathology and Laboratory Medicine, Taichung Veterans General Hospital, 17
Taichung, Taiwan, Republic of China 18
5Institute of Biomedical Nutrition, Hungkuang University, Taichung, Taiwan, Republic of 19
China 20
21
*Corresponding author: Yueh-Ling Hsieh, [email protected] 22
23
Li-Wei Chou and John Wang contributed equally to this work. 24
25 26
Abstract 27
Introduction: Hypoxia is a feature of the inflamed synovium in rheumatoid arthritis (RA). 28
Intra-articular injection of hyaluronan (HA) may be considered a potential way to treat RA. 29
However, the exact molecular mechanism of HA on decreased cellular responses to hypoxic 30
environment is unclear. The present study has been designed to use the adjuvant-induced 31
arthritis model to examine the effects of HA on the changes of immunohistochemical 32
expressions of hypoxia-inducible factor-1α (HIF-1α), inducible nitric oxide synthase (iNOS), 33
and matrix metalloproteinase-3 (MMP3) in the synovial tissues at the early phase of arthritic 34
inflammation. 35
Methods: Monoarthritis was induced in adult male Sprague-Dawley (250–300 gm) via 36
intraarticular injection of complete Freund's adjuvant (CFA) into the tibiotarsal joint. The 37
CFA-induction arthritis animals were divided into three groups: treatment (intraarticular 38
injection of HA), placebo (intraarticular injection of saline) and controls (no treatments). 39
Functional evaluations of edema and pain behavior, histology, and HIF-1α, iNOS, and MMP3 40
immunohistochemistry were performed before, after the first injection, three injections, and 41
on the follow-up injection of the treatments. 42
Results: Intra-articular injection of HA also significantly suppressed the mechanical 43
allodynia (p < 0.001) and overexpressions of HIF-1α (p < 0.001), iNOS (p = 0.004) and 44
MMP3 (p < 0.001) immunoreactivity in synovium. 45
Conclusions: This study demonstrated that early intervention of HA is an effective protection 46
against accumulation of inflammation-induced HIF-1α, iNOS, and MMP3 to limit erosive 47
damage in CFA-induced model of arthritis. 48
49 50
Introduction 51
52
Hypoxic microenvironment is a hallmark of the inflamed synovium and its 53
importance in the pathogenesis of rheumatoid arthritis (RA) has been documented [1-4]. In 54
human and animal arthritis models, the importance of hypoxia for the development and 55
persistence of RA has been demonstrated [1, 5]. Previous studies have demonstrated the 56
hypoxic nature of the synovium of patients with RA and the constitutive expression of 57
hypoxia-inducible factor-1α (HIF-1α), a key regulator of hypoxia transcriptional response. In 58
RA joints, it has been shown to express increased presence and accumulation of HIF-1α and 59
HIF-1 target genes in synovial lining cells and articular chondrocytes under hypoxic 60
condition, which aggravates joint inflammation [6, 7]. Previous studies also demonstrated 61
that hypoxia takes place in synovium at the pre-arthritic stage or early stage of the disease 62
and have a close spatial relationship and positive severity correlation with synovitis [8]. 63
Therefore, HIF-1α is identified to be a key player in the pathogenesis of RA and a potential 64
therapeutic target in RA development. 65
Nitric oxide (NO) synthesized from arginine by nitric oxide synthases (NOS), is an 66
important chemical mediator of inflammation. The inducible isoform of NOS (iNOS) is 67
primarily responsible for producing large amounts of NO and its overexpression has been 68
linked with the progressive inflammation and tissue destruction observed in hypoxic 69
experimental arthritis [9, 10] and human rheumatoid synovium [11, 12]. Matrix 70
metalloproteinases (MMPs), the most important matrix-degrading enzymes in RA, act as key 71
mediators of the resorption of cartilage, bone, synovial fluid, and adjacent soft tissue, which 72
occurs as part of the pathological destruction of joint tissue [13]. Among dozens of MMPs, 73
MMP3 (stromelysin 1) has been reported to be the major enzyme produced by fibroblasts and 74
macrophage-like cells in the synovium, and that the level of MMP3 is significantly higher in 75
synovial fluids from patients with RA [14-16]. Based on previous studies, under the 76
inflammatory conditions of RA, the levels of HIF-1α, iNOS, and MMP3 are significantly 77
higher in synovial fluids and implicated in the pathogenesis of RA. Expressions of iNOS and 78
MMP3 are probably regulated by HIF-1α in the cellular response to hypoxic and 79
inflammatory environments [11, 17, 18]. Therefore, inhibition and/or down-regulation of 80
these molecules may exert anti-hypoxic and anti-inflammatory effects. 81
Hyaluronan (HA) is a polymer of disaccharides, which has high capacity for holding 82
water and possesses high viscoelasticity [11]. The intra-articular supplementation of HA can 83
replace synovial fluid, which has lost its viscoelastic properties. HA has been widely used for 84
the treatment of osteoarthritis (OA) [19]. In addition to its characteristic as a lubricating agent, 85
exogenous administration of HA can suppress expression of inflammatory cytokines, MMPs 86
and free oxygen radicals to reduce inflammation in a postlaminectomy rat model [20] and 87
patients with RA [21]. Therefore, it has been expected that the intra-articular injection of HA 88
is more efficacious in treating RA, which principally characterizes articular synovitis [21, 22]. 89
However, its clinical use for RA joint treatment is still rare because the immunoregulatory 90
action of HA is still debatable. 91
Complete Freund's adjuvant (CFA)-induced arthritis shares some characteristics of 92
RA. This model mirrors much of the pathology of RA including hyperplasia of the synovial 93
tissues, inflammatory infiltration of the joints, and destruction of bone and cartilage in the 94
synovial joint [23]. The present study has been designed to use the adjuvant-induced arthritis 95
model to examine the effects of HA on the changes of immunohistochemical expressions of 96
HIF-1α, iNOS, and MMP3 in the synovial tissues at the early phase of arthritic inflammation. 97
We hypothesize that addition of HA will alleviate inflammatory nociception and impede the 98
accumulation of arthritis-induced HIF-1α, iNOS, and MMP3 productions at the early phase 99
of the experimental arthritic inflammatory joint. If this hypothesis is correct, it will offer at 100
least a partial explanation for efficacy of topical HA application in the subsequent inhibition 101
of hypoxic inflammation in this preclinical model. 102
103 104
Materials and methods 105
106
General design 107
Arthritis was induced arthritis on all animals by intra-articular injection of CFA. After 108
a day of CFA induction, the arthritic animals were randomly divided into three groups (n = 90) 109
according to three treatments named as: (1) Control (sham injection by needling, 110
intra-articularly manipulated and no solution administration, No-tr group, n = 30); (2) 111
Placebo (50 μl saline intra-articularly administered, SA group, n = 30); (3) Treatment (50 μl 112
HA intra-articularly administered, HA group, n = 30). Injections of HA or saline were given 113
every 2 d (Days 2, 4, and 6). The evaluation instruments were edematous swelling of the paw, 114
pain behavioral assessments, histology, and immunohistochemistry. Assessments were 115
performed at pre-arthritic (Day 0), post-arthritic (Day 1) and 3 h after the treatment of one 116
injection (1 dose, 1D) on Day 2, three injections (three doses, 3D) on Day 6, and follow-up 6 117
d after 3D (3D6d) on Day 12. The flow diagram is presented in figure 1. 118
119
Animal preparation 120
Ninety adult male Sprague-Dawley (CD(SD) IGS BR; purchased from BioLASCO 121
Taiwan Co., Ltd.) rats weighing 250–300 g were kept in the Laboratory Animal Center of 122
China Medical University. Effort was made to minimize discomfort and to reduce the number 123
of animals used. All animal experiments were conducted with the procedure approved by the 124
Animal Care and Use Committee of a university in accordance with the Guidelines for 125 Animal Experimentation. 126 127 Induction of monoarthritis 128
Monoarthritis was induced by an injection of CFA into the unilateral ankle articular 129
cavity. The rats were briefly anesthetized with 4% isoflurane (AERRANE, Baxer Healthcare 130
Corporation, Puerto Rico). A 28-gauge needle was vertically inserted distally into the 131
articular cavity from the gap between the tibiofibular and tarsus bone. CFA with volume of 132
50 μl (10 mg mycobacterium, F5881, Sigma, MO) was then injected. The monoarthritic 133
animals were separately placed in clear acrylic containers (10½" W × 19" D × 8" H), 134
allowing free movement for at least 24 h to let them adjust to these conditions before any 135 experimentation is performed. 136 137 Ultrasound-guided HA injection 138
Under brief isoflurane anesthesia, ultrasound (Terason t3000™ Ultrasound System, 139
Terason Division, Teratech Corporation, MA, USA) guided injection was performed on the 140
lateral side of tibiotarsal joint, with the transducer in the sagittal plane showing the distal end 141
of tibia and proximal part of the tarsus in the image plane. Needle insertion was 142
perpendicularly performed to the transducer. HA injection (MW: 1.2–1.4 ×106 Da; Ostenil®, 143
10 mg/ml sodium hyaluronate, TRB CHEMEDICA AG, München, Germany) was 144
documented by recording an image-clip during injection with the needle tip in the image 145
plane. 146
147
Pain threshold assessment 148
The pain thresholds were determined by nociceptive thresholds to mechanical 149
stimulation. The test consisted of evoking a hind paw flexion reflex with a handheld force 150
transducer (electronic von Frey anesthesiometer, IITC Inc., CA, USA) adapted with a 0.5 151
mm2 polypropylene tip. In a quiet room, the rats were placed in acrylic cages (32 × 22 × 27 152
cm high) with a wire grid floor for 15 -30 min habituation prior to testing. The polypropylene 153
tip was perpendicularly applied to the central area of the hind paw with with sufficient force 154
to bend the filaments into an “S” shape for 3-4 sec. The test consisted of poking a hind paw to 155
provoke a flexion reflex followed by a clear flinch response after paw withdrawal. Testing 156
was initiated with the filament corresponding to 20 log of force (g). The filaments were 157
applied with a gradual increase in pressure until a withdrawal reflex response was finally 158
detected from the animal. The response to this filament is defined if a series of weaker or 159
stronger filaments would be tested. The weakest filament able to elicit a response was taken 160
to be the paw withdrawal threshold (g). The intensity of the pressure was recorded and the 161
final value for the response was obtained by averaging five measurements. 162
163
Measurement of edematous swelling of the paw 164
The extent of peripheral swelling was assessed by measuring the circumference of the 165
paw at intact and CFA-injected sites with a flexible tape. The paw circumference was 166
obtained by averaging three measurements. The difference in the ankle circumference 167
between the initial value (pre-arthritic data) and that at each time point after injection is 168
expressed as change (%) = 100% × [(post-arthritic circumference) – (pre-arthritic 169
circumference)] / (pre-arthritic circumference). All assessments including paw withdrawal 170
and swelling measurements were performed with the assessor blinded with respect to 171
treatment. 172
173
Histology and immunohistochemistry 174
Animals were killed by anesthetic overdose after treatments of 1D (n = 10 for each 175
group), 3D (n = 10 for each group), and 3D6d (n = 10 for each group) on Days 2, 6, and 12. 176
Hind ankles were collected for histological and immunohistological analysis. The 177
formalin-fixed, paraffin-embedded joint tissues (including synovium and cartilage tissues) 178
were cut at thickness of 5 μm for histology and immunohistochemistry. Histological 179
confirmation of the arthritic pathology was performed with hematoxylin and eosin (H&E) 180
stained sections. Sections were deparaffinized in 200 ml of Trilogy (Cell Marque Corporation, 181
CA, USA) and incubated with 3% H2O2 in methanol for 20 minutes at room temperature. 182
Subsequently sections were treated with proteinase K (Sigma, St. Louis, Mo, USA) at 0.1 183
mg/mL for 20 min at room temperature to unmask epitopes followed by phosphate buffered 184
saline (PBS) rinse. Sections were incubated with blocking buffer (Power BlockTM, Biogenex, 185
USA) for 2 h at room temperature followed by incubation overnight at 4°C with the mouse 186
monoclonal antibody anti- HIF-1α (dil. 1:100, Thermo, CA, USA) and with the following 187
rabbit polyclonal antibodies: anti-iNOS (dil. 1:200, Thermo, CA, USA), anti-MMP3 (dil. 188
1:200, Abbiotec, CA, USA). After three washes with PBS containing 0.05% Tween-20 for 10 189
min, sections were incubated with biotinylated anti-rabbit and anti-mouse immunoglobulins 190
(Jackson immunoresearch, PA, USA), followed by a 30 min peroxidase-conjugated 191
streptavidin incubation (Jackson Immunoresearch, PA, USA). Sections were incubated with 192
3,3′-diaminobenzidine (Biogenex, CA, USA), dehydrated and cover-slipped with Permount 193
(Sigma, NJ, USA). Negative controls were performed by substituting the primary antibody 194
with non-immune serum. 195
The histopathology of synovium was analyzed by non-parametric scoring system 196
described by Smith et al. (24). The scores ranged from 0 to 3 on the each tissue criteria 197
including intimal hyperplasia, lymphocytic infiltration, subintimal fibrosis and vascularity. 198
The higher aggregate score was considered to reflect increased pathological changes. Five 199
randomly selected sections were scored and repeated two times for statistical analysis. 200
Quantitative analysis of immunostainings was carried out by light microscopy in synovial 201
tissue lining the joint cavity and synovial tissue attached to the cartilage. The number of 202
HIF-1α, iNOS and MMP3 immunoreactive cells was counted among at least five alternate 203
sections in the more representative fields by using a microscope. Positive nuclei and 204
cytoplasm staining cells for HIF-1α, iNOS, and MMP3 were counted in high-power fields 205
(200× magnification) that contained synovial lining cells. The area sizes of high power fields 206
were calculated by using a stage micrometer (with 100 gradations of 0.01 mm each) when 207
viewed using a 200× objective. Ten fields of each slide were counted for all samples and 208
repeated three times for statistical analysis. Results were expressed as the proportion (%) of 209
number of labeled cells per square millimeter of synovium. For statistical analysis, the mean 210
value obtained from the repeated counts was used. All of scoring and quantitative analyses 211
were assessed by two independent observers who were blinded to the origin of the sections to 212
avoid bias from interobserver variability. 213
214
Statistical analysis 215
The differences of value in each assessment between pre- and post-arthritic 216
evaluations were performed by Student’s t-test. The differences among the groups of HA, SA, 217
and No-tr on each dosage (1D, 3D, and 3D6d) were carried out using ANOVA, and later 218
further analyzed by a Bonferroni post-hoc method. Similar statistical analysis methods were 219
used to test the differences among dosages in each group. Non-parametric data (histological 220
synovial scoring) was analyzed using the Kruskal–Wallis test for multiple groups and 221
following Mann–Whitney U-tests for between-group comparisons. Pearson correlation test 222
was applied to study the correlations between pain withdrawal threshold and expressions of 223
immunoreactivities, A p value of <0.05 was considered to be statistically significant. All data 224
was analyzed using SPSS version 10.0 for Windows (SPSS Inc., IL, USA). 225
226 227
Results 228
229
Effect of HA on CFA-induced edema 230
The serial alterations of the percentage of edema (mean ± SEM) throughout the whole 231
experiment for each group are shown in figure 2A. After a day of CFA-induction, all animals 232
developed severe monoarthritis in the injected paw. There were no significant differences in 233
the non-injected intact paw on circumference among pre- and post-arthritic, and 234
post-treatment conditions for each group (p > 0.05, data not shown). The edema of the 235
CFA-injected paw gradually increased, reaching a maximal swelling of 65.51%, whereas 236
there were significant differences on edema between pre- and post-arthritic conditions (p < 237
0.001). 238
After treatment, the significant time-dependent differences on edema development 239
were observed in each group (HA group: p < 0.001; SA group: p < 0.001; No-tr group: p < 240
0.001). However, there was no difference in the edema of the arthritic paws among HA, SA, 241
and No-tr groups after treatments of 1D (p = 0.22), 3D (p = 0.41) and 3D6d (p = 0.31). 242
Therefore, intra-articular injections of HA, regardless of different dosages for 1D, 3D, and 243
3D6d, did not ameliorate joint swelling compared with either SA or No-tr groups. 244
245
Effect of HA on CFA-induced inflammatory mechanical nociception 246
The serial alterations of the paw withdrawal threshold (mean ± SEM) throughout the 247
whole experiment for each group are shown in figure 2B. The mean threshold was 25.07 ± 248
4.68 g at pre-arthritic condition. However, after CFA-induction, it decreased to 9.32 ± 3.16 g. 249
There was significant difference with pre-arthritic condition (p < 0.001). 250
The significant differences on paw withdrawal threshold were shown among HA, SA, 251
and No-tr groups after treatment of 1D (p = 0.008), 3D (p < 0.001), and 3D6d (p <0001). 252
Significantly lower threshold existed after treatment of 1D, 3D, and 3D6d in SA and No-tr 253
groups compared with those in HA groups (HA vs. SA, p = 0.04; HA vs. No-tr, p = 0.01 for 254
1D; HA vs. SA, p < 0.001; HA vs. No-tr, p < 0.001 for 3D; HA vs. SA, p < 0.001; HA vs. 255
No-tr, p = 0.001 for 3D6d). The analysis also showed that there was significantly lower 256
threshold found in No-tr group compared with SA group after treatment of 3D (p =0.03) and 257
3D6d (p = 0.01). However, no significant difference was observed between these groups after 258
treatment of 1D (p =1.0). 259
There were significant difference among three dosages in HA group (p < 0.001), but 260
not in both SA (p = 0.84) and No-tr (p = 0.56) groups. After HA treatment, the paw 261
withdrawal threshold showed significant increase in 3D and 3D6d treatments compared with 262
1D treatment (1D vs. 3D, p < 0.001; 1D vs. 3D6d, p < 0.001). However, no difference was 263
observed between the 3D and 3D6d of HA treatments (p = 0.05). 264
Histopathological assessments 266
Widening of the synovial cavity, infiltration of inflammatory cells, thickening of the 267
synovial membrane, a narrowing of the synovial space, disruption of the cartilaginous tissue, 268
and bone erosion were apparent in control rats of No-tr group (figures 3A, 3a) and SA group 269
(figures 3B, 3b). The tibiotarsal joints of rats treated with 1D, 3D, and 3D6d of HA were less 270
inflamed, as revealed by decreased number of inflammatory cells, synovial membrane 271
thickening and cartilage destruction (figures 3C, 3c). There were significant differences in 272
lymphocytic infiltration and aggregate score of non-parametric criteria observed among ankle 273
joint synovium from HA and SA and No-tr groups treated with 1D, 3D, and 3D6d (Table 2, p 274
< 0.05). Lymphocytic infiltrations in synovium were significantly reduced after HA
275
treatment when compared with those treated with SA or No-tr (HA vs. SA, HA vs. No-tr, p < 276
0.05 in all doses). There were no significantly differences in intimal hyperplasia, subintimal 277
fibrosis and vascularity among the three groups (p > 0.05). 278
279
Immunohistochemical assessments on location of HIF-1α, iNOS, and MMP3 280
Overexpressions of HIF-1α, iNOS, and MMP3 immunoreactivity were found within 281
the synovial tissue in No-tr (figures 4A, 5A, 6A) and SA groups (figures 4B, 5B, 6B). At 282
higher-power magnification, it is evident that these positive immunoreactivities were clearly 283
localized in both nucleus and cytoplasm of arthritic synovium (figures 4a, 5a, 6a; 4b, 5b, 6b). 284
The primary cells exhibiting specific HIF-1α, iNOS, and MMP3 immunoreactivity were 285
morphologically consistent with macrophages, mainly in inflammatory infiltrate and invasive 286
pannus of the inflamed synovial joint. Synovial lining cells and some chondrocytes were also 287
found to be HIF-1α, iNOS and MMP3 positive. After treatment with HA, HIF-1α, iNOS and 288
MMP3 immunoreactivity were reduced (figures 4C, 5C, 6C) concurrent with reduced 289
immunoreactivities localized in both nucleus and cytoplasm of arthritic synovium at 290
higher-power magnification (figures 4c, 5c, 6c). 291
292
Quantitative analysis on extents of HIF-1α, iNOS, and MMP3 293
After treatment, the significant differences on extents of HIF-1α, iNOS, and MMP3 294
immunoreactive expression were shown among HA, SA, and No-tr groups after treatment of 295
1D (HIF-1α: p < 0.001; iNOS: p < 0.001; MMP3: p < 0.001), 3D (HIF-1α: p < 0.001; iNOS: 296
p < 0.001; MMP3: p < 0.001), and 3D6d (HIF-1α: p < 0.001; iNOS: p < 0.001; MMP3: p <
297
0.001). Significantly lower expressions of HIF-1α, iNOS, and MMP3 immunoreactivity 298
existed after treatment of 1D in HA groups (HIF-1α: HA vs. SA, p < 0.001; HA vs. No-tr, p 299
< 0.001 [figure 4D]; iNOS: HA vs. SA, p < 0.001; HA vs. No-tr, p < 0.001 [figure 5D];
300
MMP3: HA vs. SA, p < 0.001; HA vs. No-tr, p < 0.001 [figure 6D]). The analysis also 301
showed there were no significant differences on HIF-1α, iNOS, and MMP3 immunoreactivity 302
between SA and No-tr groups for 1D dosage (HIF-1α: SA vs. No-tr, p = 0.14; iNOS: p = 0.45; 303
MMP3: p = 1.0, [figures 4D, 5D, 6D]). Similar results were also found on HIF-1α, iNOS, and 304
MMP3 immunoreactivity for treatments of 3D and 3D6d (figures 4D, 5D, and 6D). 305
Significant difference on extents of HIF-1α, iNOS, and MMP3 immunoreactive 306
expression were shown among 1D, 3D, and 3D6d dosages in HA group (HIF-1α: p < 0.001; 307
iNOS: p = 0.004; MMP3: p < 0.001), but not in both SA (HIF-1α: p = 0.56; iNOS: p = 0.85; 308
MMP3: p = 0.81) and No-tr (HIF-1α: p = 0.16; iNOS: p = 0.50; MMP3: p =0.99) groups. 309
After 3D and 3D6d of HA treatment, the extents of HIF-1α and iNOS immunoreactive 310
expression significantly reached maximum reduction compared with those of 1D treatment 311
(HIF-1α: 3D vs. 1D, p < 0.001; 3D6d vs. 1D, p =0.03 [figure 4D]; iNOS: 3D vs. 1D, p = 312
0.01; 3D6d vs. 1D, p = 0.03 [figure 5D]). However, no difference was exhibited between the 313
3D and 3D6d of HA treatments (HIF-1α: 3D vs. 3D6d, p = 0.15; iNOS: 3D vs. 3D6d, p = 314
1.0). For expression of MMP3 immunoreactivity, significant reduction was found after 3D 315
treatment (3D vs. 1D, p = 0.001; 3D vs. 3D6d, p < 0.001 [figure 6D]). However, the 316
expression of MMP3 immunoreactivity recovered after 3D6d treatment (3D6d vs. 1D, p = 317
1.0). 318
319
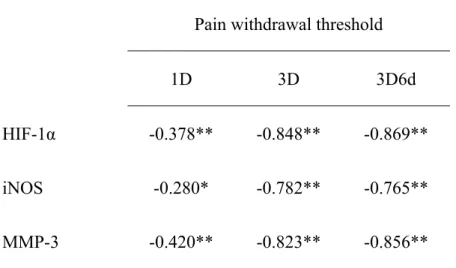
Association of pain withdrawal threshold with immunoreactivity results 320
A significant linear correlation was found between pain withdrawal threshold and 321
immunoreactivity of HIF-1α, iNOS and MMP3 (Pearson correlation coefficients, p <0.05, 322
Table 1). There were strong negative association of pain withdrawal threshold with HIF-1α, 323
iNOS and MMP3 after 3D treatment and those with HIF-1α and MMP3 after 3D6d treatment 324
(0.75 <|Pearson γ| < 1). 325
Discussion 326
327
The results of this study demonstrate that lymphocytic/plasmocytic infiltration in the 328
synovium and accumulation of HIF-1α, iNOS, and MMP3 were suppressed after 329
intra-articular administration of HA at the early phase of adjuvant-induced inflammation. The 330
extent of HIF-1α, iNOS, and MMP3 immunoreactivity was consistent with the results of pain 331
behavioral assessment, which demonstrated elevation of the mechanonociceptive threshold 332
after administration of HA. These findings have never been reported by other researchers. 333
In this model, the early phases of adjuvant-induced arthritis seem to be characterized 334
by acute cytokines-induced inflammation [25]. Due to infiltration of the injured tissues 335
caused by immune cells and responses, swelling is a major sign during acute inflammation 336
and it might also be considered an important parameter on evaluation the potential 337
anti-inflammatory effects of compounds [26]. However, as shown in the results of our study, 338
The levels of edematous swelling were not changed after HA treatment in acute inflammation 339
at the early phase of adjuvant-induced arthritis, suggesting the weaker activity against edema 340
of HA in acute inflammatory animal model. This result is consistent with the animal study 341
with collagen-induced arthritis [27] and human study with OA [28]. The reason is probably 342
due to HA inducing swelling adverse effects which primarily occurs in the HA injected site. 343
Previous studies revealed that HA may act either as a primary irritant or an inflammatory 344
mediator to induce acute adverse events characterized by transient swelling of the injected 345
joint in some patients [28, 30, 31]. The prevalence of adverse effects was noted in 47% of 346
patients after HA supplementation and in 22% of patients treated with saline injections (32). 347
In this study, the observation time of edema measurement started 3 h post-HA administration 348
after HA administration when an adverse effect of a transient increase in swelling at the 349
injection site occurred. Therefore, the further study with long-term observations of joint 350
swelling after ceasing HA was needed for clarifying the effect of exogenous HA on resolving 351
RA-induced joint edema. 352
It has been well-established by animal behavioral and human clinical studies that 353
elastoviscous solutions of HA could have an analgesic effect when injected into arthritic 354
joints and if appropriately applied to patients with acute arthritic pain [33]. There was 355
significantly less bradykinin found in the crystal-induced arthritic joint after the injection of 356
HA [34]. Electrophysiological studies also demonstrated that the rate of neural discharges of 357
the nociceptive afferent fibers innervating the synovial tissue were significantly attenuated 358
and reached a constant rate 2–3 h after injection [33, 35, 36]. Treatment of HA showed an 359
analgesic effect after the onset of cartilage destruction and pain in a rabbit OA model [37]. 360
Our behavioral study is the first report on the analgesic effect of HA at decreased mechanical 361
allodynia in a rat RA model, which is also consistent with the findings of previous studies. 362
The intra-articular injection of HA also resulted in elevation of mechanonociceptive threshold, 363
which was in accordance with those of data determined by immunohistochemistry in this 364
study. 365
HA has been demonstrated to possess a therapeutic effect on OA studied by many 366
researchers. Macroscopic and microscopic evaluations revealed that HA has 367
chondroprotective effects in a rabbit model of OA [38]. Our results showed that HA reduced 368
the pathohistological sign including the degree of infiltration of the synovial membrane by 369
plasma and lymphocytes in CIA animals which is consistent with findings from previous 370
study (39). The tendency for decreased cellular infiltration during early phase of arthritis 371
supports the assumption that HA provides a temporary protecting barrier over the cartilage, 372
and thereby protects it against CFA insults. HA has also been shown to significantly suppress 373
NO production and inhibit interleukin-1 beta (IL-1ß)-induced MMP3 production from OA 374
synovial tissue in vitro and in vivo [40-43]. As far as we know in English literature, few 375
studies regarding the role of HA on suppression of HIF-1α-mediated hypoxic and 376
inflammatory responses have been conducted in OA models. Due to less inflammation in OA 377
synovial tissue, there is minor HIF-1α expression in these tissues [5]. However, there is 378
relatively higher expression of HIF-1α immunohistochemistry in RA synovial tissues 379
compared with OA tissues due to the nature of the tissue being inflammatory and angiogenic 380
in RA [7]. Therefore, HIF-1α has the potential to serve as an anti-rheumatic drug activity 381
biomarker in the clinic and is expected to significantly affect/accelerate the clinical 382
development of treatment for RA. 383
The possible important role of HIF-1α in RA has been extensively discussed [44, 45]. 384
The presence of both hypoxia and inflammatory proteins in RA synovium, which both lead to 385
HIF-1α stabilization and subsequent HIF-1 activation, seems to highlight the important role 386
of HIF-1α [45]. Elevated synovial angiogenesis is a key event during the course of RA. The 387
modulation and blockade of angiogenesis via drug interventions has been shown to contribute 388
to therapeutic efficacy in rat models of arthritis [46]. HIF-1α probably has an essential 389
involvement in the angiogenic process of synovium in RA by regulation of its target gene, 390
vascular endothelial growth factor (VEGF) (44). Inhibition of HIF-1α protein expression and 391
VEGF production by SMP-114, a disease-modifying anti-rheumatic drug (DMARD), has 392
been shown of therapeutic benefit in RA [47]. Oral administration of the inhibitor of heat 393
shock protein 90 (Hsp90) which has been shown to potently reduce HIF-1α-related signaling 394
and VEGF production has also been found to decrease inflammation and cartilage damage in 395
vivo models of RA [48]. Therefore, suppression of HIF-1α may be a key implication on the
396
development of novel therapeutic strategies revolutionizing the treatment of RA. Results 397
showed that HA suppressed the adjuvant-induced overexpression of iNOS and MMP3, which 398
is consistent with findings from previous studies. Our study is the first to report that HA 399
suppresses HIF-1α. This study revealed the reduction of accumulation of HIF-1α expression 400
in synovium of adjuvant-induced RA model after intra-articular HA administration. The 401
suppressive effects on accumulation of inflammation-induced HIF-1α, iNOS, and MMP3 402
expressions in synovium may be involved in the therapeutic mechanism of HA intervention 403
used in treatment of RA. Further molecular studies on expressions of VEGF will be needed 404
for fully supporting the issue of anti-angiogenic effects of HA. 405
406
Conclusions 407
408
Suppression of HIF-1α may be one of the major targets of the therapeutic approach in 409
RA. This study demonstrated that early intervention of HA is an effective protection against 410
accumulation of inflammation-induced HIF-1α, iNOS, and MMP3, which might limit the 411
erosive joint damage of arthritis. The findings suggest that modulation of HIF-1 α as a 412
“master switch” may be used as a therapeutic target in the anti-inflammatory treatment of 413 RA. 414 415 List of abbreviations 416
1D: 1 dose, 3D: three doses, 3D6d: follow-up at the 6th day after 3 doses, CaMKII: 417
Ca2+/calmodulin-dependent kinase II, CFA: complete Freund's adjuvant, DMARD: 418
disease-modifying anti-rheumatic drugs, H&E: hematoxylin and eosin, HA: hyaluronan, 419
HIF-1α: hypoxia-inducible factor-1 alpha, Hsp90: heat shock protein 90, IL-1ß: interleukin-1 420
beta, iNOS: inducible nitric oxide synthase, MMP3: matrix metalloproteinase-3, MMPs: 421
matrix metalloproteinases, NO: Nitric oxide, NOS: nitric oxide synthases, OA: osteoarthritis, 422
RA: rheumatoid arthritis, SD: Sprague-Dawley, SPSS: Statistical Package for the Social 423
Sciences, VEGF: vascular endothelial growth factor. 424
425
Competing interests: The authors have declared no conflictsof interest. 426
427
Authors’ contributions 428
LWC conceived the study, and participated in data analysis, and drafted the manuscript. JW 429
participated in the histopathology and scored the immunohistology. PLC participated in the 430
establishment of animal model, immunohistology and animals’ functional evaluations. YLH 431
conceived the study, performed the statistical analysis, and drafted the manuscript. All 432
authors read and approved the final manuscript. 433
434
Acknowledgements and Funding 435
The authors gratefully acknowledged the technical expertise of Mr. Shih-Chung Chen for 436
counting of immunohistochemical-labeled cells and Ms. Pin-Wen Tu for recording of data of 437
the animals’ functional evaluations in this study. This work was supported by a grant of 438
China Medical University and Hospital (grants CMU-98-S-10 to YLH. and DMR-96-073 to 439 LWC), Taiwan. 440 441 References 442
1. Peters CL, Morris CJ, Mapp PI, Blake DR, Lewis CE, Winrow VR: The transcription 443
factors hypoxia-inducible factor 1alpha and Ets-1 colocalize in the hypoxic 444
synovium of inflamed joints in adjuvant-induced arthritis. Arthritis Rheum 2004, 445
50:291-296. 446
2. Boyd HK, Lappin TR, Bell AL: Evidence for impaired erythropoietin response to 447
anaemia in rheumatoid disease. Br J Rheumatol 1991, 30:255-259. 448
3. Oliver KM, Taylor CT, Cummins EP: Hypoxia. Regulation of NFkappaB signalling 449
during inflammation: the role of hydroxylases. Arthritis Res Ther 2009, 11:215. 450
4. Paleolog EM: Angiogenesis in rheumatoid arthritis. Arthritis Res 2002, 4 (Suppl 451
3):S81-S90. 452
5. Brouwer E, Gouw AS, Posthumus MD, van Leeuwen MA, Boerboom AL, Bijzet J, Bos 453
R, Limburg PC, Kallenberg CG, Westra J: Hypoxia inducible factor-1-alpha 454
(HIF-1alpha) is related to both angiogenesis and inflammation in rheumatoid 455
arthritis. Clin Exp Rheumatol 2009, 27:945-951. 456
6. Giatromanolaki A, Sivridis E, Maltezos E, Athanassou N, Papazoglou D, Gatter KC, 457
Harris AL, Koukourakis MI: Upregulated hypoxia inducible factor-1alpha and 458
-2alpha pathway in rheumatoid arthritis and osteoarthritis. Arthritis Res Ther 2003, 459
5:R193-201. 460
7. Hollander AP, Corke KP, Freemont AJ, Lewis CE: Expression of hypoxia-inducible 461
factor 1alpha by macrophages in the rheumatoid synovium: implications for 462
targeting of therapeutic genes to the inflamed joint. Arthritis Rheum 2001, 463
44:1540-1544. 464
8. Jeon CH, Ahn JK, Chai JY, Kim HJ, Bae EK, Park SH, Cho EY, Cha HS, Ahn KS, Koh 465
EM: Hypoxia appears at pre-arthritic stage and shows co-localization with early 466
synovial inflammation in collagen induced arthritis. Clin Exp Rheumatol 2008, 467
26:646-648. 468
9. Oyanagui Y: Nitric oxide and superoxide radical are involved in both initiation and 469
development of adjuvant arthritis in rats. Life Sci 1994, 54:PL285-289. 470
10. Hashimoto K, Fukuda K, Yamazaki K, Yamamoto N, Matsushita T, Hayakawa S, 471
Munakata H, Hamanishi C: Hypoxia-induced hyaluronan synthesis by articular 472
chondrocytes: the role of nitric oxide. Inflamm Res 2006, 55:72-77. 473
11. Ahn JK, Koh EM, Cha HS, Lee YS, Kim J, Bae EK, Ahn KS: Role of 474
hypoxia-inducible factor-1alpha in hypoxia-induced expressions of IL-8, MMP-1 475
and MMP-3 in rheumatoid fibroblast-like synoviocytes. Rheumatology (Oxford) 476
2008, 47:834-839. 477
12. Farrell AJ, Blake DR, Palmer RM, Moncada S: Increased concentrations of nitrite in 478
synovial fluid and serum samples suggest increased nitric oxide synthesis in 479
rheumatic diseases. Ann Rheum Dis 1992, 51:1219-1222. 480
13. Cawston T: Matrix metalloproteinases and TIMPs: properties and implications for 481
the rheumatic diseases. Mol Med Today 1998, 4:130-137. 482
14. Tetlow LC, Wolley DE: Comparative immuno-localization studies of collagenase-1 483
and collagenase 3 production in the rheumatoid lesion, and by human 484
chondrocytes and synoviocytes in vitro. Br J Rheumatol 1998, 37:64-70. 485
15. Yoshihara Y, Nakamura H, Obata K, Yamada H, Hayakawa T, Fujikawa K, Okada Y: 486
Matrix metalloproteinases and tissue inhibitors of metalloproteinases in synovial 487
fluids from patients with rheumatoid arthritis or osteoarthritis. Ann Rheum Dis 488
2000, 59:455-461. 489
16. Keyszer G, Lambiri I, Nagel R, Keysser C, Keysser M, Gromnica-Ihle E, Franz J, 490
Burmester GR, Jung K: Circulating levels of matrix metalloproteinases MMP-3 and 491
MMP-1, tissue inhibitor of metalloproteinases 1 (TIMP-1), and MMP-1/TIMP-1 492
complex in rheumatic disease. Correlation with clinical activity of rheumatoid 493
arthritis versus other surrogate markers. J Rheumatol 1999, 26:251-258. 494
17. Fraisl P, Aragones J, Carmeliet P: Inhibition of oxygen sensors as a therapeutic 495
strategy for ischaemic and inflammatory disease. Nat Rev Drug Discov 2009, 496
8:139-152. 497
18. Chen W, Ostrowski RP, Obenaus A, Zhang JH: Prodeath or prosurvival: two facets of 498
hypoxia inducible factor-1 in perinatal brain injury. Exp Neurol 2009, 216:7-15. 499
19. Miltner O, Schneider U, Siebert CH, Niedhart C, Niethard FU: Efficacy of 500
intraarticular hyaluronic acid in patients with osteoarthritis--a prospective clinical 501
trial. Osteoarthritis Cartilage 2002, 10:680-686. 502
20. Schimizzi AL, Massie JB, Murphy M, Perry A, Kim CW, Garfin SR, Akeson WH: 503
High-molecular-weight hyaluronan inhibits macrophage proliferation and 504
cytokine release in the early wound of a preclinical postlaminectomy rat model. 505
Spine J 2006, 6:550-556.
506
21. Saito S, Momohara S, Taniguchi A, Yamanaka H: The intra-articular efficacy of 507
hyaluronate injections in the treatment of rheumatoid arthritis. Mod Rheumatol 508
2009, 19:643-651. 509
22. Oliveira PG, Brenol CV, Edelweiss MI, Brenol JC, Petronilho F, Roesler R, Dal-Pizzol F, 510
Schwartsmann G, Xavier RM: Effects of an antagonist of the 511
bombesin/gastrin-releasing peptide receptor on complete Freund's 512
adjuvant-induced arthritis in rats. Peptides 2008, 29:1726-1731. 513
23. Brauer R, Kittlick PD, Thoss K, Henzgen S: Different immunological mechanisms 514
contribute to cartilage destruction in antigen-induced arthritis. Exp Toxicol Pathol 515
1994, 46:383-388. 516
24. Smith MM, Cake MA, Ghosh P, Schiavinato A, Read RA, Little CB: Significant 517
synovial pathology in a meniscectomy model of osteoarthritis: modification by 518
intra-articular hyaluronan therapy. Rheumatology (Oxford). 2008 , 47:1172-1178. 519
25. Ferraccioli G, Bracci-Laudiero L, Alivernini S, Gremese E, Tolusso B, De Benedetti F: 520
Interleukin-1beta and Interleukin-6 in arthritis animal models. Roles in the early 521
phase of transition from the acute to chronic inflammation and relevance for 522
human rheumatoid arthritis. Mol Med 2010, 16:552-557. 523
26. Morris CJ: Carrageenan-induced paw edema in the rat and mouse. Methods Mol 524
Biol 2003, 225:115-121.
525
27. Campo GM, Avenoso A, Campo S, Ferlazzo AM, Altavilla D, Calatroni A: Efficacy of 526
treatment with glycosaminoglycans on experimental collagen-induced arthritis in 527
rats. Arthritis Res Ther 2003, 5:R122-131. 528
28. Petrella RJ: Hyaluronic acid for the treatment of knee osteoarthritis: long-term 529
outcomes from a naturalistic primary care experience. Am J Phys Med Rehabil 2005, 530
84:278-83; quiz 84, 93. 531
29. Zhou JL, Liu SQ, Qiu B, Hu QJ, Ming JH, Peng H: Effects of hyaluronan on vascular 532
endothelial growth factor and receptor-2 expression in a rabbit osteoarthritis 533
model. J Orthop Sci 2009, 14:313-319. 534
30. Henderson EB, Smith EC, Pegley F, Blake DR: Intra-articular injections of 750 kD 535
hyaluronan in the treatment of osteoarthritis: a randomised single centre 536
double-blind placebo-controlled trial of 91 patients demonstrating lack of efficacy. 537
Ann Rheum Dis 1994, 53:529-534.
538
31. Puttick MP, Wade JP, Chalmers A, Connell DG, Rangno KK: Acute local reactions 539
after intraarticular hylan for osteoarthritis of the knee. J Rheumatol 1995, 540
22:1311-1314. 541
32. Hamburger MI, Lakhanpal S, Mooar PA, Oster D: Intra-articular hyaluronans: a 542
review of product-specific safety profiles. Semin Arthritis Rheum 2003, 32:296-309. 543
33. Balazs EA: Analgesic effect of elastoviscous hyaluronan solutions and the 544
treatment of arthritic pain. Cells Tissues Organs 2003, 174:49-62. 545
34. Aihara S, Murakami N, Ishii R, Kariya K, Azuma Y, Hamada K, Umemoto J, Maeda S: 546
Effects of sodium hyaluronate on the nociceptive response of rats with 547
experimentally induced arthritis. Nippon Yakurigaku Zasshi 1992, 100:359-365. 548
35. Pozo MA, Balazs EA, Belmonte C: Reduction of sensory responses to passive 549
movements of inflamed knee joints by hylan, a hyaluronan derivative. Exp Brain 550
Res 1997, 116:3-9.
551
36. Gomis A, Pawlak M, Balazs EA, Schmidt RF, Belmonte C: Effects of different 552
molecular weight elastoviscous hyaluronan solutions on articular nociceptive 553
afferents. Arthritis Rheum 2004, 50:314-326. 554
37. Hashizume M, Koike N, Yoshida H, Suzuki M, Mihara M: High molecular weight 555
hyaluronic acid relieved joint pain and prevented the progression of cartilage 556
degeneration in a rabbit osteoarthritis model after onset of arthritis. Mod 557
Rheumatol 2010, 20:432-438.
558
38. Ozkan FU, Ozkan K, Ramadan S, Guven Z: Chondroprotective effect of 559
N-acetylglucosamine and hyaluronate in early stages of osteoarthritis--an 560
experimental study in rabbits. Bull NYU Hosp Jt Dis 2009, 67:352-357. 561
39. Roth A, Mollenhauer J, Wagner A, Fuhrmann R, Straub A, Venbrocks RA, Petrow P, 562
Bräuer R, Schubert H, Ozegowski J, Peschel G, Müller PJ, Kinne RW: Intra-articular 563
injections of high-molecular-weight hyaluronic acid have biphasic effects on joint 564
inflammation and destruction in rat antigen-induced arthritis. Arthritis Res Ther 565
2005, 7:R677-686. 566
40. Tung JT, Venta PJ, Caron JP: Inducible nitric oxide expression in equine articular 567
chondrocytes: effects of antiinflammatory compounds. Osteoarthritis Cartilage 2002, 568
10:5-12. 569
41. Takahashi K, Hashimoto S, Kubo T, Hirasawa Y, Lotz M, Amiel D: Hyaluronan 570
suppressed nitric oxide production in the meniscus and synovium of rabbit 571
osteoarthritis model. J Orthop Res 2001, 19:500-503. 572
42. Lee YT, Shao HJ, Wang JH, Liu HC, Hou SM, Young TH: Hyaluronic acid modulates 573
gene expression of connective tissue growth factor (CTGF), transforming growth 574
factor-beta1 (TGF-beta1), and vascular endothelial growth factor (VEGF) in 575
human fibroblast-like synovial cells from advanced-stage osteoarthritis in vitro. J 576
Orthop Res 2010, 28:492-496.
577
43. Waddell DD, Kolomytkin OV, Dunn S, Marino AA: Hyaluronan suppresses 578
IL-1beta-induced metalloproteinase activity from synovial tissue. Clin Orthop Relat 579
Res 2007, 465:241-248.
580
44. Gaber T, Dziurla R, Tripmacher R, Burmester GR, Buttgereit F: Hypoxia inducible 581
factor (HIF) in rheumatology: low O2! See what HIF can do! Ann Rheum Dis 2005, 582
64:971-980. 583
45. 44. Muz B, Khan MN, Kiriakidis S, Paleolog EM: Hypoxia. The role of hypoxia and 584
HIF-dependent signalling events in rheumatoid arthritis. Arthritis Res Ther 2009, 585
11:201. 586
46. Issekutz AC, Sapru K: Modulation of adjuvant arthritis in the rat by 587
2-methoxyestradiol: an effect independent of an anti-angiogenic action. Int 588
Immunopharmacol 2008, 8:708-716.
589
47. Westra J, Brouwer E, van Roosmalen IA, Doornbos-van der Meer B, van Leeuwen MA, 590
Posthumus MD, Kallenberg CG: Expression and regulation of HIF-1alpha in 591
macrophages under inflammatory conditions; significant reduction of VEGF by 592
CaMKII inhibitor. BMC Musculoskelet Disord 2010, 11:61. 593
48. Rice JW, Veal JM, Fadden RP, Barabasz AF, Partridge JM, Barta TE, Dubois LG, Huang 594
KH, Mabbett SR, Silinski MA, Steed PM, Hall SE: Small molecule inhibitors of 595
Hsp90 potently affect inflammatory disease pathways and exhibit activity in 596
models of rheumatoid arthritis. Arthritis Rheum 2008, 58:3765-3775. 597
598
Figure legends 600
Figure 1. Experimental design of the sequence of events for the entire course of the 601
experiment. After the evaluations including measurements of paw edematous swelling and 602
pain threshold, the animals were sacrificed for histology and immunohistochemistry. 1D: one 603
dose; 3D: three doses; 3D6d: follow-up at the 6th day after 3 doses. CFA: complete Freund’s 604
adjuvant; HA: hyaluronan; No-tr: No treatment; SA: saline 605
606
Figure 2. Results of edema (A) and pain behavioral (B) assessments. Data were calculated 607
before treatment at the conditions of pre- and post-CFA-induced arthritis, after treatment at 608
conditions of one injection (1D), three injections (3D) and follow-up 6 d after 3D (3D6d) in 609
treatment (hyaluronan injection, HA), placebo (saline administration, SA) and control (sham 610
injection, No-tr) groups. Each bar represents the mean ± SD in body weight and mean ± SEM 611
in paw circumference and withdrawal threshold. #: p < 0.05, Student’s t-test for comparison 612
of pre- and post-arthritic condition before treatment. *p < 0.05, Bonferroni post hoc test for 613
comparison of difference between groups at dosages of 1D, 3D and 3D6d after treatment. 614
615
Figure 3. Histopathology of arthritis joints. Representative HE sections of the hind paws 616
obtained from adjuvant-induced arthritic animals treated with intra-articular three injections 617
for No-tr (A), SA (B), and HA (C). In rats without any treatment for No-tr group, wherein 618
cartilaginous tissue could not be clearly detected, bone damage was even greater and there 619
was massive inflammatory cells infiltrated in synovium (a). Similar changes were observed in 620
rats treated with SA. Cartilage erosion was more pronounced and the extensively expanded 621
synovial pannus was more densely infiltrated with mononuclear cells (b). In rats treated with 622
HA, the joints were much less inflamed, and lymphocyte accumulation (c) and cartilage 623
damage decreased. There was no sign of bone destruction (cart = cartilage; syn = synovial 624
tissue; see figure 2 for other definitions). 625
626
Figure 4. Representative immunohistochemical sections of HIF-1α immunoreactivity. 627
Sections obtained from the arthritic synovium treated with intra-articular three injections of 628
No-tr (A), SA (B), and HA (C) groups. At higher-power magnification, it is evident that these 629
positive (brown staining) immunoreactivities were clearly localized in both nucleus and 630
cytoplasm of arthritic synovium in the sections from No-tr (a) and SA (b) animals. 631
Administration of HA (c) to adjuvant-induced rat produced a marked reduction in the 632
immunostaining for HIF-1α quantitative analysis (D) of positive-labeled cells in synovium 633
for HIF-1α immunohistochemistry at the early phase of inflammation of each group was 634
presented in the average proportion of labeled neurons (mean ± SEM). * p < 0.05, showed 635
significant differences between groups when either SA or No-tr is compared with HA group 636
using Bonferroni post hoc test. Significant differences were found between HA vs SA groups 637
and HA vs No-tr groups. # p < 0.05, showed significant differences between dosages tested 638
by Bonferroni post hoc test (cart = cartilage; syn = synovial tissue; see figure 2 for other 639
definitions). 640
641
Figure 5. Representative immunohistochemical sections of iNOS immunoreactivity. 642
Sections obtained from the arthritic synovium treated with intra-articular three injections of 643
No-tr (A), SA (B), and HA (C) groups. At higher-power magnification, it is evident that these 644
positive (brown staining) immunoreactivities were clearly localized in both nucleus and 645
cytoplasm of arthritic synovium in the sections from No-tr (a) and SA (b) animals. 646
Administration of HA (c) to adjuvant-induced rat produced a marked reduction in the 647
immunostaining for iNOS. Quantitative analysis (D) of positive-labeled cells in synovium for 648
iNOS immunohistochemistry at the early phase of inflammation of each group was presented 649
in the average proportion of labeled neurons (mean ± SEM). * p < 0.05, showed significant 650
differences between groups when either SA or No-tr is compared with HA group using 651
Bonferroni post hoc test. Significant differences were found between HA vs SA groups and 652
HA vs No-tr groups. # p < 0.05, showed significant differences between dosages tested by 653
Bonferroni post hoc test (cart = cartilage; syn = synovial tissue; see figure 2 for other 654
definitions). 655
Figure 6. Representative immunohistochemical sections of MMP3 immunoreactivity. 657
Sections obtained from the arthritic synovium treated with intra-articular three injections of 658
No-tr (A), SA (B), and HA (C) groups. At higher-power magnification, it is evident that these 659
positive (brown staining) immunoreactivities were clearly localized in both nucleus and 660
cytoplasm of arthritic synovium in the sections from No-tr (a) and SA (b) animals. 661
Administration of HA (c) to adjuvant-induced rat produced a marked reduction in the 662
immunostaining for iNOS. Quantitative analysis (D) of positive-labeled cells in synovium for 663
MMP3 immunohistochemistry at the early phase of inflammation of each group was 664
presented in the average proportion of labeled neurons (mean ± SEM). * p < 0.05, showed 665
significant differences between groups when either SA or No-tr is compared with HA group 666
using Bonferroni post hoc test. Significant differences were found between HA vs SA groups 667
and HA vs No-tr groups. # p < 0.05, showed significant differences between dosages tested 668
by Bonferroni post hoc test (cart = cartilage; syn = synovial tissue; see figure 2 for other 669
definitions). 670
Table 1. Association of pain withdrawal threshold with the 672
immunoreactivity results given as γ-values 673
Pain withdrawal threshold
1D 3D 3D6d
HIF-1α -0.378** -0.848** -0.869**
iNOS -0.280* -0.782** -0.765**
MMP-3 -0.420** -0.823** -0.856**
Correlations were analyzed by Pearson correlation coefficients. 674
**: P<0.01; *:P<0.05. 675
Dose Group Intimal hyperplasia Subintimal fibrosis Lymphocytic infiltration Vascularity Aggregate score 1D HA 2.45±0.11 2.60±0.11 1.50±0.11*# 2.05±0.11 7.80±0.26*# SA 2.60±0.11 2.60±0.11 2.50±0.11 2.10±0.12 9.10±0.31 No-tr 2.65±0.11 2.65±0.10 2.95±0.05 2.20±0.12 9.75±0.24 a
p value among groups p>0.05 p>0.05 p<0.001 p>0.05 p<0.001
3D HA 2.50±0.11 2.70±0.11 1.40±0.13*# 2.20±0.09 8.05±0.31*#
SA 2.80±0.09 2.70±0.10 2.55±0.11 2.15±0.11 9.55±0.28 No-tr 2.80±0.09 2.70±0.11 2.85±0.08 2.20±0.14 9.95±0.32 a
p value among groups p>0.05 p>0.05 p<0.001 p>0.05 p<0.001
3D6d HA 2.50±0.11 2.50±0.11 1.40±0.11*# 2.15±0.11 7.85±0.25*#
SA 2.70±0.11 2.60±0.10 2.77±0.10 2.20±0.14 9.6±0.36 No-tr 2.70±0.11 2.70±0.11 2.85±0.08 2.40±0.11 10.05±0.33 a
p value among groups p>0.05 p>0.05 p<0.001 p>0.05 p<0.001
Values are mean± SEM. a: tested with Kruskal–Wallis test. *: p < 0.05, showed statistically significant differences between HA and SA groups; #