行政院國家科學委員會補助專題研究計畫期末報告
※※※※※※※※※※※※※※※※※※※※※※※※※※
※
※
※
糖尿病對頸動脈構造及功能之影響
※
※
※
※※※※※※※※※※※※※※※※※※※※※※※※※※
計畫類別:□個別型計畫 □整合型計畫
計畫編號:NSC 90-2320-B-002-178-
執行期間:90 年 08 月 01 日至 91 年 07 月 31 日
計畫主持人:蘇大成 醫師
共同主持人:鄭建興 醫師
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
執行單位:台大醫學院
中華民國九十一年十月三十一日
行政院國家科學委員會補助專題研究計畫期末報告
糖尿病對頸動脈構造及功能之影響
計畫類別:□個別型計畫 計畫編號:NSC 90-2320-B-002-178- 執行期間:90 年 08 月 01 日至 91 年 07 月 31 日 計畫主持人:蘇大成 醫師 台大醫學院 共同主持人:鄭建興 醫師 台大醫學院一、中文摘要
研究背景:糖尿病是冠狀動脈心臟病及腦 中風之主要危險因子。近年隨著經濟發展 生活富裕,國人常有營養過度及肥胖之趨 勢,國人糖尿病的盛行率有逐年上昇之 勢,糖尿病對國人健康的威脅絕不可忽 視。材料及方法:本研究藉由具人群代表 性的社區心臟血管研究--金山社區長期 追 蹤 的 族 群 中 , 使 用 病 例 對 照 組 於 1994-1995 年金山社區第三次追蹤的世代 中,空腹血糖超過 126mg/dl 者,或是有 糖尿病病史正在接受治療者,其年齡現在 在 45-65 歲者共 192 位,選為病例組,而 經由性別及年齡配對後,選出對照組 192 位,總共 384 位納入此次研究通知對象。 我們用高解析度的 B 模式的頸動脈超音波 來測量,並以總頸動脈最厚的內皮+中皮 厚度(IMT),及顱外頸動脈硬化塊分數, 來表示顱外頸動脈硬化的程度及頸動脈 血管直徑大小在收縮期及舒張期的變化 來看頸動脈彈性。。結果:於 2001 年共 有 108 位有糖尿病病史及 135 位對照組參 與頸動脈硬化及彈性之檢查。我們發現糖 尿病患者頸動壁脈增厚及動脈硬化塊的 嚴重程度與對照組並無顯著差異,但頸動 脈血管彈性則明顯變差。即使用多變項迴 歸分析來檢驗頸動脈血管彈性指標,我們 用擴張參數(distensibility coefficient, DC) 來表達時,發現糖尿病病史、年齡、收縮 壓、平均動脈壓、脈壓差皆是擴張參數的 重要影響因子。結論:糖尿病明顯的影響 頸動脈的動脈彈性。我們的發現更加強了 糖尿病在動脈硬化的病理形成上扮演一 主要的角色的理論。二、英文摘要
Backgrounds: With the current trend of
aging population in Taiwan, it is urgent to pay more attention to early detection of atherosclerosis to prevent the atherosclerotic diseases. Diabetes mellitus (DM) is one of the well- known and major risk factors for coronary and carotid arteries atherosclerosis.
Mater ial and Methods: One hundred and
eight DM patients and 135 non-DM control subjects from the Chin-Shan Community Cardiovascular Cohort participated in this study in 2001. The carotid atherosclerosis was measured by high-resolution B-mode ultrasonography and expressed as maximal intima-media thickness of the common carotid artery (CA), internal CA, carotid
bulb, and extracranial CA plaque score. The carotid arterial compliance was measured using common CA diameter changes, and was defined as Distensibility Coefficient (DC)= (2(systolic diameter - diastolic diameter)/ systolic diameter)/(systolic BP-diastolic BP). Results of measurements of carotid atherosclerosis showed no significant difference between DM and control. However, DC decreased in DM group while comparing with control. Further analysis using multivariate lineal regression model revealed that DM, age, blood pressure components (SBP, DBP, MAP, and PP) are important determinants of DC. Conclusions : Patients with DM decreased carotid arterial distensibility though no significant difference in carotid atherosclerosis. Our findings support that DM is important in the pathogenesis of atherosclerosis in middle-aged population.
三、研究背景及緣由 Backgrounds
and Intr oduction
Studies have shown that atherosclerosis related diseases such as stroke, cardiovascular disease (CVD) and diabetes mellitus (DM) have ranked as the second, fourth and fifth leading cause of death in Taiwan [1]. With the current trend of aging population in Taiwan, it is therefore urgent to pay more attention to prevent the atherosclerotic diseases. More significantly, early detection of atherosclerosis and its associated risk factors is a must to prevent the occurrence and progression of these diseases.
This research was designed to demonstrate the relationships between DM and carotid arterial compliance, and carotid atherosclerosis. The carotid ultrasound will be used to detect atherosclerosis and carotid compliance. Carotid ultrasound is reliable, reproducible and non-invasive technique that allows easy measurement of the overt atherosclerosis in the carotid arteries [2-4] that is strongly associated with cardiovascular risk factors [5-7], and cardiovascular morbidity and mortality [8-9]. We also had demonstrated in CCCC study in Taiwan that hypertension is the major determinant for carotid atherosclerosis [7].With the aging of the population and the increasing prevalence of obesity that might lead to an increasing prevalence of DM and thereby atherosclerosis, present study will be of significant in early detection the abnormalities in carotid arteries of DM patients.
四 、 材 料 與 方 法 Mater ials and
Methods
Subjects
The Chin-Shan Community Cardiovascular Cohort (CCCC) Study is a prospective and longitudinal study that evaluates the incidences, prevalence, mortality and risk factors of cardiovascular and cerebrovascular diseases in a northern Taiwan community since 1990 [7,10-12].
In present study, we will recruit patients with diabetes mellitus and fulfill the criteria of history of diabetes mellitus or
fasting blood sugar ≥126 mg/dl from the third biennial follow-up in 1994-1995 from the CCCC Study. One hundred and ninety two with DM aged 45-64 will be chosen as cases and another 192 control were randomly selected from non-diabetes frequency matched for gender and age. Home-visit or telephone will contact all participants. After obtaining inform consent, participants will be arranged for atherosclerosis measurements.
Arterial Stiffness and Atherosclerosis
Assessments
1. Arterial stiffness
High resolution 2-D, M-mode, and pulse-Doppler ultrasonography will be used to measure the following parameters at bilateral extracranial carotid arteries for each participant. The following methods will be used for carotid arterial stiffness measurements [13].
(1). Vascular wall stiffness (β) = ln (Ps/Pd)Dd / (Ds-Dd) [14]. (2). Distensibility Coefficient (DC)=(2(Ds-Dd)/Ds)/(sbp-dbp) (3). The pulsatility index (PI)= (peak systolic velocity -end diastolic velocity) / mean velocity (4). Resistance index (RI)= (peak systolic velocity -end diastolic velocity) / peak systolic velocity.
2. Carotid Atherosclerosis
Carotid Ar ter y Intima-Media Thickness (IMT)
The maximal IMTs on the common carotid artery (CCA), bulb, and internal carotid artery (ICA) bilaterally will be measured using high-resolution B-mode ultrasonography. A Hewlett Packard SONO
4500 ultrasound system (Andover, MA, U.S.A.), equipped with a 10.0 MHz real-time B-mode scanner and a 5.6 MHz pulsed-Doppler mode scanner, will be used for evaluation. We had studied the reliability of repeat measurements of CCA IMTs according to the inter-observer and intra-observer groups in previous study. The inter-observer correlation coefficients were 0.80 to 0.93 and the intra-observer correlation coefficients were 0.71 to 0.90 [15].
Extr acr anial Carotid Atherosclerotic (ECCA) Plaque
The plaque scoring quantified method has been mentioned elsewhere [7,16]. In this study, the examination will include the proximal CCA (>20 mm proximal to the bulb bifurcation), distal CCA, bulb, internal carotid artery, and external carotid artery bilaterally. The plaque score will be computed by summing the plaque grades at each of the segments of the ECCA.
The velocity criteria and the real-time B-mode images will be used to assess carotid stenosis. Carotid stenosis >50% will be also defined in the presence of peak systolic velocity >1.25 m/s. Reproducibility of plaque grade scoring showed perfect agreement with kappa value of 0.701 in our previous study.
Assessment of Vascular Risk Factors
BP measurements were performed with mercury sphygmomanometer in a standardized fashion cuff size adjusted to the circumference of the arm. BP was recorded using the means of twomeasurements taken after 5 minutes of rest in the supine position. Data on alcohol use and smoking were obtained by self-reported questionnaire. DM was defined as fasting serum glucose ≥126mg/dl in at least two different measurements and/or a history of use of medication.
Lipid and Lipoprotein Assays
Blood samples of 9-12 hours overnight fasting for lipid and glucose determination were drawn from antecubital vein with patient in a seated position. Serum levels of lipid profiles, including total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglycerides, Apolipoprotein (Apo) A1 and B were analyzed in a central laboratory and described previously [7,10-12].
Statistical Analyses
In the data analysis, clinical features and cardiovascular risk factors of study subjects were compared between DM and control. Continuous variables are expressed as the mean ±1 standard deviation. Chi-square tests was used to make comparisons between two groups. The average carotid artery IMT measurements at CCA, bulb, ICA on both sides were compared between DM and control. The total scores of ECCA plaques were compared also between DM and control. Multivariate lineal regression analysis was used to test the significant predictors for carotid arterial distensibility, which expressed as DC.
五、結果 Results
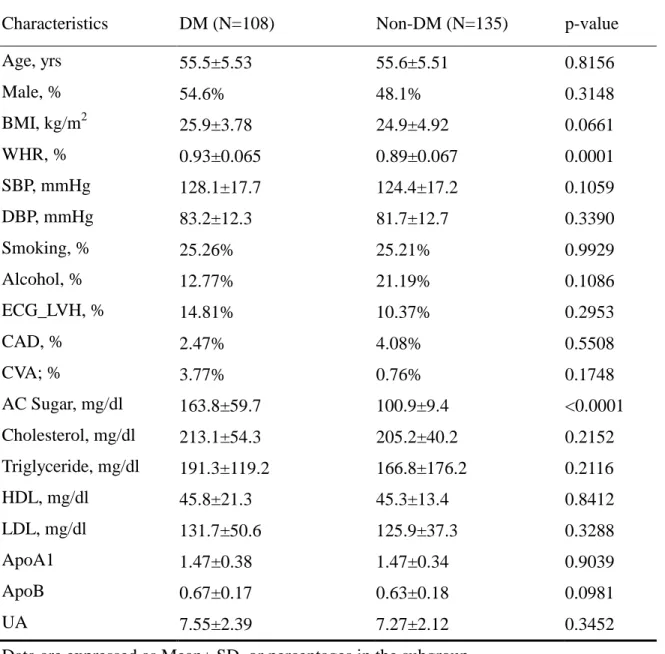
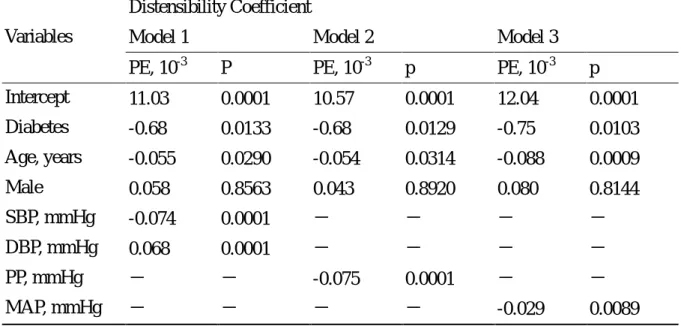
Table 1 showed that obesity indexes and fasting sugar were the major difference between groups of DM and control. There were no significant difference regarding other CV risk factors. Table 2 showed the measurement of carotid atherosclerosis in DM had no significant difference compared with control. Carotid arterial compliance parameters expressed as DC and β decreased in DM patients while compared with control in Table 3. The multiple regression model was used to find out the significant determinants of carotid arterial DC in Table 4. Results revealed diabetes, aged, and blood pressure components (SBP, DBP, PP, and MAP) were predictors of DC.
六、討論 Discussions
Atherosclerosis shares an important role in the development of coronary heart disease and stroke, and DM is one of the well- known and major risk factors for coronary and carotid arteries atherosclerosis. Recent studies have shown that DM in Taiwan have a higher prevalence rate as compared with the Western countries and the rate is progressively increased in aged over 35 [12]. In addition, one line of research has demonstrated that the incidence rate, based on the United State population standardized non-insulin dependent diabetes mellitus (NIDDM), is 9.3/1000 for men and women in Taiwan[4]. Studies have shown that the fasting glucose level, a symptom of establish diabetes, is
associated with common carotid artery (CCA) intima-media thickness (IMT) that may suggest a chronic hyperglycemia and metabolic abnormalities and sequentially an increased risk for atheroscelerosis [18-19].
In pathophysiological mechanism, obesity was considered as an important trigger factor of diabetes[7]. It is also a significant risk factor for cardiovascular disease (CVD), and is especially at higher risk for overweight men and women [20-21]. Due to the obesity associated multiple worse metabolic effects on CVD and its undeviating association with CVD, the American Heart Association (AHA) has claimed obesity as a major CVD risk since 1998 [22]. Body mass index (BMI) was proposed as a reliable indicator for assessing abdominal obesity and surrogate for CVD in most population.
In our preliminary work, we found that BMI presented in the case of obesity was significantly associated with dyslipidemia (increased cholesterol, LDL-C, TG, and Apo-B) in the female cohort [11]. In addition, hyperinsulinemia was also associated with higher BMI and dyslipidemia was presented in both gender. Our results showed that obesity was associated with relative risk of 5.5 for hyperinsulinemia [13]. Obesity also is one of presentation of insulin resistance syndrome[23]. Diabetes and hyperinsulinemia may be considered as an important risk, a metabolic syndrome with detrimental effects on dyslipidemia and carotid artrial compliance.
In conclusions, patients with DM decreased carotid arterial distensibility though no significant difference in carotid
atherosclerosis. Our findings support that DM is important in the pathogenesis of atherosclerosis in middle-aged population.
七、參考文獻 References
1. Department of Health, Executive Yuan: Health and Vital Statistics II of the Republic of China, 1998, Taipei, Republic of China.
2. Persson J, Wikstrand J, Israelsson B, Formgren J, Berglund G. Noninvasive quantification of atherosclerotic lesions. Reproducibility of ultrasonographic measurement of arterial wall thickness and plaque size. Arteriosclereo Thromb. 1992;12:261-266.
3. Li R, Cai J, Tegeler C, Sorlie P, Metcalf PA, Heiss G. Reproducibility of extracranial carotid atherosclerotic lesions assessed by B-mode ultrasound: the Atherosclerosis Risk In Communities Study. Ultrasound Med Biol. 1996;22:791-799.
4. Su TC, Jeng JS, Chien KL, Torng PL, Sung FC, Lee YT. Measurement reliability of common carotid artery intima-media thickness by ultrasonographic assessment. J Med Ultrasound 1999; 7:73-79.
5. Heiss G, Sharett AR, Barnes R, Chambless LE, Szklo M, Alzola C, ARIC Investigators. Carotid atherosclerosis measured by B-mode ultrasound in populations: associations with cardiovascular risk factors in the ARIC study. Am J Epidemiol 1991;134:250-256.
6. Determinants of carotid intima-media thickness: a population-based ultrasonography study in eastern Finnish men. J intern Med 1991; 229:225-231.
7. Su TC, Jeng JS, Chien KL, et al. Hypertension is the major determinant of carotid atherosclerosis - a community-based study in Taiwan. Stroke 2001; 32:2265-2271.
8. O'leary DH, Polak JF, Kronmal RA, kronmal RA, Manolid TA, Burke GL, Wolfson SK, for the Cardiovascular Health Study collaborative research group. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. N Engl J Med 1999;340:14-22.
9. Bots ML, Hoes AW, Hofman A, Witteman JCM, Grobbee DE. Cross-sectionally assessed carotid intima-media thickness related to long-term risk of stroke, coronary heart disease and death as estimated by available risk functions. J Int Med 1999;245:269-276.
10. Chien KL, Lee YT, Sung FC, Su TC, Hsu HC, Lin RS. Hyperinsulinemia and related atherosclerotic risk factors in the population at risk: community-based study. Clin Chem. 1999; 45:838–846. 11. Torng PL, Su TC, Sung FC, Chien KL,
Huang SC, Chow SN, Lee YT. Effects of menopause and obesity on lipid profiles in middle-aged Taiwanese women— The Chin-Shan Community Cardiovascular Cohort Study. Atherosclerosis. In press 2000.
12. Lee YT, Lin RS, Sung FC, Yang CY,
Chien KL, Chen WJ, Su TC, Hsu HC, Huang YC. Chin-Shan Community Cardiovascular Cohort in Taiwan— baseline data and five-year follow-up morbidity and mortality. J Clin Epidemiol. 2000;53:838–846. 13. Gamble G, Zorn J, Sanders G, et al.
Estimation of arterial stiffness, compliance, and distensibility from M-mode ultrasound measurements of common carotid artery. Stroke. 1994;25:11-16.
14. Kawasaki T, Sasayama S, Yagi S, et al. Non-invasive assessment of the age related changes in stiffness of major branches of the human arteries. Cardiovasc Res 1987;21:678-687.
15. Su TC, Jeng JS, Chien KL, Torng PL, Sung FC, Lee YT. Measurement reliability of common carotid artery intima-media thickness by ultrasonographic assessment. J Med Ultrasound. 1999;7:73-79.
16. Jeng JS, Chung MY, Yip PK, Hwang BS, Chang YC. Extracranial carotid atherosclerosis and vascular risk factors in different types of ischemic stroke in Taiwan. Stroke. 1994;25:1989-1993. 17. Wang SL, Pan WH, Hwu CM, Ho LT,
Lo CH, Lin SL, Jong YS. Incidence of NIDDM and the effects of gender, obesity and hyperinsulinemia in Taiwan. Diabetologia 1997;40:1431-1438.
18. Pujia A, Colonna A, Gnasso A, Mattioli PL, Irace C. Carotid IMT is enlarged in subjects with NIDDM compared with age- and sex-matched control subjects. Diabetes Care. 1994;17:1330-1336. 19. Grundy SM, Benjamin IJ, Burke GL,
Chait A, Eckel RH, Howard BV, Mitch W, Smith SC, Sowers JR. Diabetes and cardiovascular disease. A statement for healthcare professionals from the American Heart Association. Circulation. 1999;100:1134-1146.
20. Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham heart study. Circulation. 1983;67:968-977.
21. Manson JE, Colditz GA, Stampfer MJ, Willett WC, Rosner B, Manson RR, et al. A prospective study of obesity and risk of coronary heart disease in women. N Engl J Med. 1990;322:882-889.
22. Eckel RH, Krauss RM. American Heart Association call to action: Obesity as a major risk factor for coronary heart disease. AHA Nutrition Committee. Circulation. 1998;97:2099-2100.
23. Reaven GM, Lithell H, Landsberg L. Hypertension and associated metabolic abnormalities- the role of insulin resistance and the sympathoadrenal system. N Engl J Med. 1996;334:374-381.
Table 1 Baseline Char acter istics of Par ticipants.
Characteristics DM (N=108) Non-DM (N=135) p-value
Age, yrs 55.5±5.53 55.6±5.51 0.8156 Male, % 54.6% 48.1% 0.3148 BMI, kg/m2 25.9±3.78 24.9±4.92 0.0661 WHR, % 0.93±0.065 0.89±0.067 0.0001 SBP, mmHg 128.1±17.7 124.4±17.2 0.1059 DBP, mmHg 83.2±12.3 81.7±12.7 0.3390 Smoking, % 25.26% 25.21% 0.9929 Alcohol, % 12.77% 21.19% 0.1086 ECG_LVH, % 14.81% 10.37% 0.2953 CAD, % 2.47% 4.08% 0.5508 CVA; % 3.77% 0.76% 0.1748 AC Sugar, mg/dl 163.8±59.7 100.9±9.4 <0.0001 Cholesterol, mg/dl 213.1±54.3 205.2±40.2 0.2152 Triglyceride, mg/dl 191.3±119.2 166.8±176.2 0.2116 HDL, mg/dl 45.8±21.3 45.3±13.4 0.8412 LDL, mg/dl 131.7±50.6 125.9±37.3 0.3288 ApoA1 1.47±0.38 1.47±0.34 0.9039 ApoB 0.67±0.17 0.63±0.18 0.0981 UA 7.55±2.39 7.27±2.12 0.3452 Data are expressed as Mean± SD, or percentages in the subgroup.
Table 2 Measurements of Carotid Ar ter iosclerosis
DM (N=108) Non-DM (N=135) p-value IMT, cm CCA 0.088±0.021 0.086±0.022 0.4604 Bulb 0.100±0.036 0.094±0.033 0.1702 ICA 0.076±0.022 0.094±0.033 0.2672 MEAN 0.088±0.022 0.085±0.020 0.1723 ECCA Plaque Score
Total Score 1.500±2.646 1.119±2.133 0.2257 Data are expressed as Mean±SD.
Table 3. Measurements of Carotid Ar ter ial Compliance DM(N=108) Non-DM(N=134) p-value Ds, cm 0.65±0.06 0.63±0.09 0.0138 Dd, cm 0.60±0.06 0.57±0.08 0.0019 PI 1.29±1.30 1.20±0.33 0.3355 RI 0.66±0.07 0.65±0.07 0.1055 DC, mmHg-1 0.0038±0.0014 0.0046±0.0025 0.0028 Â 5.40±2.16 4.79±2.02 0.0236 Data are expressed as Mean±SD.
Distensibility Coefficient (DC)=(2(Ds-Dd)/Ds)/(sbp-dbp) â=(log(sbp/dbp))×(Dd/(Ds-Dd))
Table 4. Multiple Regression Analysis for Distensibility Coefficient (DC) of Common Carotid Ar ter y Compliance with Respect to Associated Risk Factor s.
Distensibility Coefficient
Model 1 Model 2 Model 3 Variables
PE, 10-3 P PE, 10-3 p PE, 10-3 p Intercept 11.03 0.0001 10.57 0.0001 12.04 0.0001 Diabetes -0.68 0.0133 -0.68 0.0129 -0.75 0.0103 Age, years -0.055 0.0290 -0.054 0.0314 -0.088 0.0009 Male 0.058 0.8563 0.043 0.8920 0.080 0.8144 SBP, mmHg -0.074 0.0001 - - - - DBP, mmHg 0.068 0.0001 - - - - PP, mmHg - - -0.075 0.0001 - - MAP, mmHg - - - - -0.029 0.0089 * Model 1 :R2 =0.2277, adjusted R2=0.1936 . Model 2 :R2=0.2265, adjusted R2=0.1963 . Model 3 :R2=0.1129, adjusted R2=0.0782 .
* All models expressed after adjusted for current smoking, body mass index, low-density lipoprotein cholesterol(LDL), and high-density lipoprotein cholesterol(HDL).
* Abbreviations: PE, parameter estimate; PP, Pulse Pressure, PP=SBP-DBP; MAP, Mean attery pressure, MAP=(SBP+2DBP)/3 .