Glutathione S-Transferase, incense burning, and asthma in children
I-Jen Wang*# ¶, Ching-Hui Tsai†, Chang-Hao Chen§, Kuan-Yen Tung† and Yungling L. Lee †f AFFILIATIONS
*
Department of Pediatrics, Taipei Hospital, Department of Health, Taipei, Taiwan; #
College of Public Health, China Medical University, Taichung, Taiwan; ¶
School of Medicine, Fu Jen Catholic University, Taipei, Taiwan; †
Institute of Epidemiology and Preventive Medicine, National Taiwan University College of Public Health, Taipei, Taiwan;
§
Guangfu Township Health Office, Hualien County Health Bureau, Hualien, Taiwan; and f
Research Center for Genes, Environment and Human Health, College of Public Health, National Taiwan University, Taipei, Taiwan
Short title: GSTT1, incense burning, and childhood asthma
CORRESPONDENCE
Yungling Leo Lee, MD, PHD, Institute of Epidemiology and Preventive Medicine, College of Public Health, National Taiwan University, Taipei 100, Taiwan.
Fax: 886-2-2392-0456 E-mail: [email protected]
STATEMENT OF INTEREST
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
Incense burning is a popular practice in many families and temples. However, little is known about the effects of indoor incense burning and genetic polymorphisms on asthma. This study evaluated the effects of indoor incense burning and glutathione S-transferase (GST) genetic polymorphisms on asthma and wheeze.
In 2007, 3764 seventh-grade schoolchildren were evaluated using a standard questionnaire for information about respiratory symptoms and environmental exposures. Multiple logistic regressions were performed to assess the association between GST polymorphisms and incense burning frequency on asthma and wheeze, after adjusting for potential confounders.
The frequency of incense burning at home was associated with increased risk of current asthma (p=0.05), medication use (p=0.03), and exercise wheeze (p=0.001). Glutathione S-transferase theta-1 (GSTT1) null genotypes were associated with current asthma (OR=1.43, 95% CI=1.00~2.04) and medication use (OR=1.46, 95% CI=1.01~2.22). GSTT1 showed significant interactive effect with incense burning on current asthma, current wheeze, and nocturnal wheeze. The frequency of incense burning was associated with increased risk of current asthma, medication use, lifetime wheeze, nocturnal wheeze, and exercise wheeze in an exposure-response manner among children with GSTT1 null genotype (p<0.05).
Incense burning is a risk factor for asthma and wheezing, especially in GSTT1 genetically susceptible children.
INTRODUCTION
The prevalence of asthma in Asia differs from that of western countries [1,2]. Culture, lifestyle, and residential environment are all potential risk factors that contribute to such difference [3]. Incense burning and its effect on respiratory health is worth exploring because exposure to incense smoke may be comparable to exposure to tobacco smoke because incense burning is a traditional and popular practice among many families and temples [4,5]. In addition to burning huge amounts of incense in temples during major Chinese or religious festivals, many believers also burn incense when they worship at home or in temples.
The physical characteristics of the incenses are similar. Typical Chinese incense is composed of 35% fragrance material, 33% bamboo stick, 21% herbal and wood powder by weight, and 11% adhesive powder [6]. The emitted smoke contains particulate matter (PM), diethylphthalate (DEP), gas products, and many other organic compounds. Due to its slow and incomplete combustion, incense burning produces continuous smoke that generates toxic gases and chemical particles such as polycyclic aromatic hydrocarbons (PAHs), carbon monoxide, isoprene, and benzene that can easily accumulate inside houses with inadequate ventilation [6]. It is reported that PAHs and airborne PM from incense burning constitute potential health hazards, which are related to respiratory symptoms, asthma, elevated cord blood IgE levels, contact dermatitis, and cancer [7,8]. Therefore, exploring the health effects of exposure to incense smoke in children is warranted.
The Glutathione S-transferase (GST) super-family includes a number of susceptibility genes. Several members, including glutathione S-transferase mu 1 (GSTM1), glutathione S-transferase theta-1 (GSTT1), and glutathione S-transferase pi 1 (GSTP1), are expressed in the respiratory tract and involved in asthma pathogenesis, including oxidant defenses, xenobiotic metabolism, and detoxification of hydroperoxides [9]. The GSTT1 null genotype has been shown to be significantly associated with atopy [10]. Among GSTT1 deficient
children, in utero exposure to smoke is also reportedly associated with significant decrements in lung function [11]. Furthermore, Saadat et al. report that both GSTT1 and GSTM1 null genotypes lack protection against asthma development in adults with positive history of smoking [12]. Evidence suggests that variants in the GSTM1 and GSTP1 loci may contribute to the occurrence of childhood asthma and increase susceptibility to adverse effects of air pollution [13]. Asthmatic children with GSTM1 null and GSTP1 Val/Val genotypes also appear more susceptible to developing respiratory symptoms related to ozone exposure [14]. However, whether or not polymorphism of the GST genotypes can modify the effects of incense smoke on asthma requires investigation. Thus, the purpose of this study was to
METHODS
Study population
Between September and October 2007, 5082 middle-school children were recruited from public schools in 14 Taiwan Children Health Study (TCHS) communities. The focus
population was on 3764 seventh-grade school-aged children who completed the standard questionnaire. Each student took home an informed consent form and a standard
questionnaire to be answered by parents with additional questions concerning the effect of incense burning on asthma symptoms [15]. Questions in the questionnaire included basic demography, residential environmental factors (e.g. environmental tobacco smoke [ETS], pets and cockroaches at home, dampness of the house, fungus on the house wall, air cleaner, air conditioner, dehumidifier, and carpets at home), and family history of atopic diseases. All of the selected subjects were of the same ethnic origin. The Institutional Review Board (National Taiwan University Hospital Research Ethics Committee; Number: 200902042R) approved the study protocol, which is as previously described [15].
Health effects assessment
The parents’ questionnaire responses were used to categorize children’s asthmatic and wheezing status as previously described [15]. Children were considered as having lifetime asthma if the answer to the question “Has a doctor ever diagnosed this child as having asthma?” was a yes. Current asthma was defined as physician-diagnosed asthma with any asthma-related symptoms or illnesses in the past 12 months. Medication use was defined as use of any inhaled, oral, or intravenous medication in the past 12 months. Lifetime wheeze was determined by a positive response to the question, “Has your child ever had wheeze or whistling in the chest at any time in the past when he/she did not have a cold or the flu?” Those who reported attacks in the past 12 months were identified as current wheeze. Exercise wheeze was determined by a positive response to the question, “Has your child ever had
wheeze or shortness of breath triggered by exercise?” Incense exposure
Since children were exposed to incense smoke mostly in their homes, incense smoke dosage was determined from the question, “How often is incense burned in the household when the child is in the room during the past 12 months?” The frequency of incense burning was divided into 3 categories: never, less than daily (2 times per month or in major festivals), and daily (all day long, every day, and morning and night every day).
Analysis of genetic polymorphisms
Cotton swabs containing oral mucosa were collected and stored at -80°C before analysis. Genomic DNA was isolated using the phenol/chloroform extraction method [16]. Genetic polymorphisms of the GSTM1 and GSTT1 genes were recognized by polymerase chain reaction (PCR) while the GSTP1 was detected by PCR-restriction fragment length
polymorphisms (PCR- RFLP) method as previously described [16]. The laboratory staff was blinded to each subject’s clinical status. Genotype assignments were based on two consistent experimental results. About 15% of the randomly selected samples were sequenced and all were consistent with the initial genotyping results.
Statistical analysis
Multiple logistic regression models adjusted for major covariates were made to examine the effects of incense burning with GST genotypes on asthma and wheezing. To further assess gene-environmental interaction, the combined association of incense burning and GST
genotypes was examined by stratifying into four groups: no incense GSTT1 or GSTM1 present, no incense GSTT1 or GSTM1 null, with incense GSTT1 or GSTM1 present, and with incense GSTT1 or GSTM1 null. As regards GSTP1, the genotypes were also stratified into four groups: no incense GSTP1 Ile-Ile, no incense GSTP1 Ile-Val or Val-Val, incense GSTP1 Ile-Ile, and incense GSTP1 Ile-Val or Val-Val. Bonferroni correction was used to
address the problem of multiple comparisons.
Gene-environmental interaction was tested by adding a product term in the regression model. For categorical variables with more than two categories, the gene-environmental interaction was evaluated using the likelihood ratio test, comparing the model with indicator variables for the cross-classified variables with a reduced model containing indicator variables for the main effects only. Within genotype category, a one degree of freedom trend test was used to evaluate the possible exposure-response relationship across categories of the incense burning variables.
Odds ratio (OR) and 95% confidence interval (CI) were adjusted for important potential confounders in all analyses. Selection of confounders that were included in the model was based on a priori consideration and standard statistical procedure of 10% change in point estimates. Subjects with missing covariate information were included in the model using missing indicators. All hypothesis testing was two-sided at the significance level of 0.05 and performed using the SAS software version 9.1 (SAS Institute, Inc., Cary, NC).
RESULTS
Of the 3764 children with complete questionnaire and genotyping data enrolled in this study, 26 were excluded due to active smoking. Of the 3738 participants included in the final analysis, 63.0% had residential incense smoke exposure. Table 1 provided the demographic characteristics of the study population. The characteristics were almost identical between those with and without genotyping. The overall allele frequencies were 48.1% null GSTT1 polymorphisms, 56.9% null GSTM1 polymorphisms, and 65.4% Ile GSTP1-105
polymorphisms.
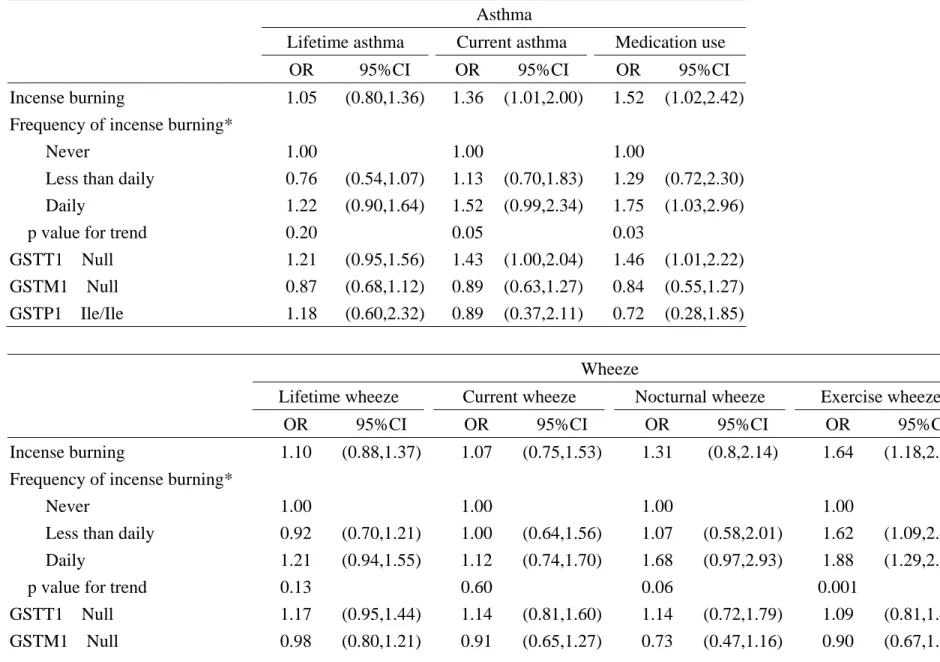
Results showed that incense burning at home was associated with increased risk of current asthma (OR=1.36, 95% CI=1.01~2.00, p=0.05), medication use (OR=1.52, 95% CI=1.02~2.42, p=0.03), and exercise wheeze (OR=1.64, 95% CI=1.18~2.28, p=0.001) (Table 2). The GSTT1 null genotypes were associated with current asthma (OR=1.43, 95%
CI=1.00~2.04) and medication use (OR=1.46, 95% CI=1.01~2.22). The GSTT1 null genotype had a positive relationship with wheeze, but did not reach statistical significance (Table 2). Both the GSTM1 null and the homozygous GSTP1 Ile-105 were not significantly associated with asthma and wheeze.
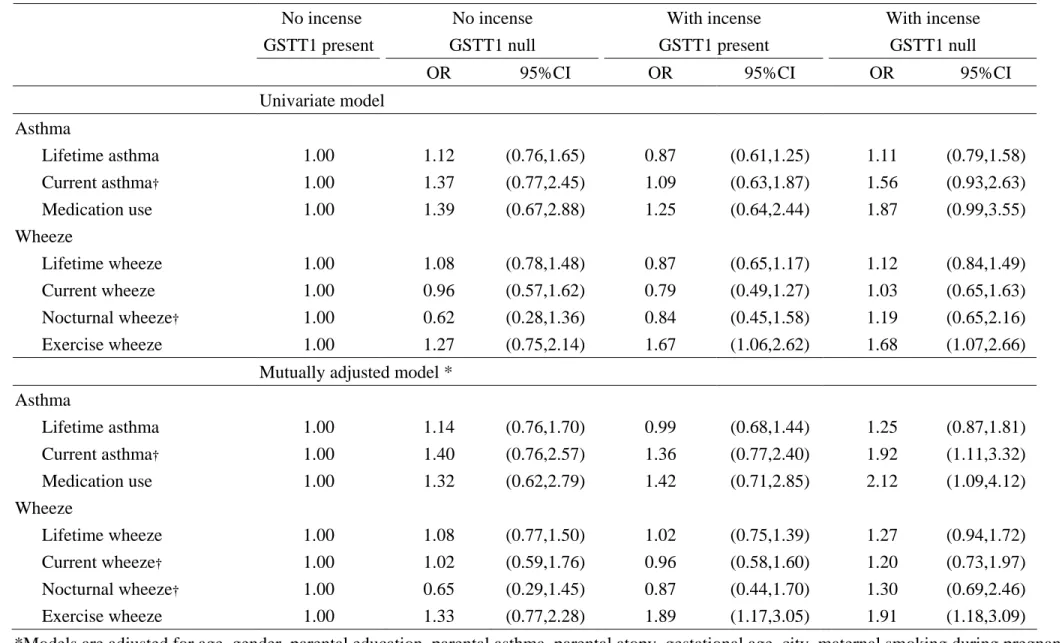
Since only the GSTT1 null genotype was associated with asthma, the association between incense burning and GSTT1 genotype on asthma and wheeze was further examined. In a mutually adjusted model of potential confounders, the GSTT1 null genotype showed
significant interaction with incense burning on current asthma, current wheeze, and nocturnal wheeze (p<0.05) (Table 3). However, analyses of GSTM1 and GSTP1 did not show
significant interactive effects (Supplement Tables). Incense burning and GSTT1 had a synergistic effect on current asthma, with OR=1.40 (95% CI=0.76-2.57) for no incense
exposure GSTT1 null genotype, OR=1.36 (95% CI=0.77-2.40) for incense exposure GSTT1
genotype (Table 3).
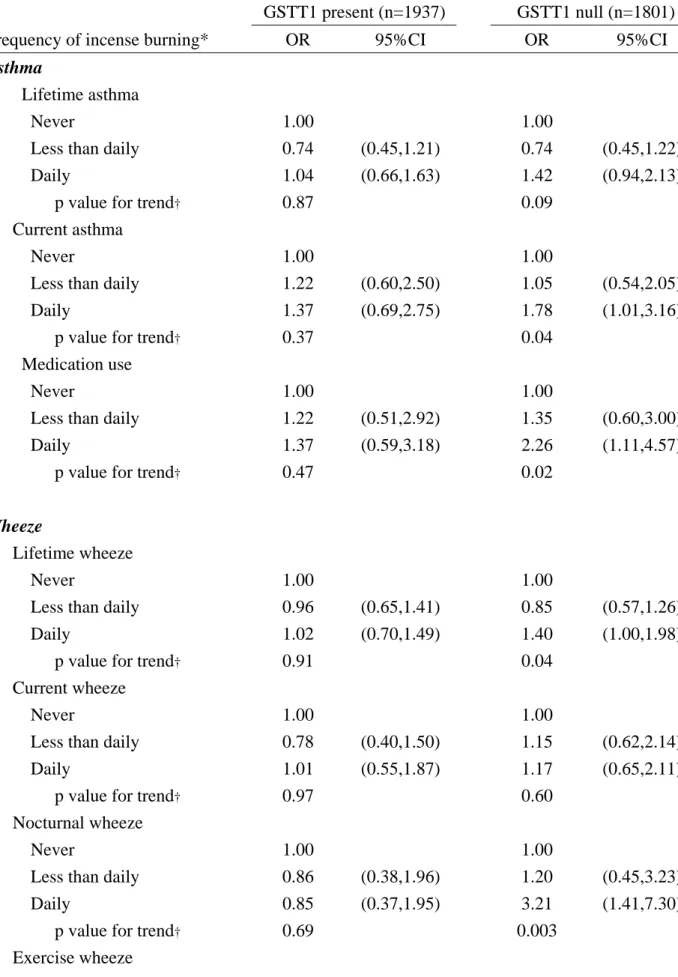
After stratification by GSTT1 genotype, the frequency of incense burning was associated with increased risk of current asthma (p=0.04), medication use (p=0.02), lifetime wheeze (p=0.04), nocturnal wheeze (p=0.003), and exercise wheeze (p=0.01) in an exposure-response manner for children with GSTT1 null genotype (Table 4). However, there were no significant relationships between incense burning and GSTM1 and GSTP1 genotypes on asthma and wheeze (Online Supplementary Tables).
DISCUSSION
This study is a contribution to literature on the potential association among genetic
polymorphisms, incense burning, and pediatric asthma. The combination effects of GSTT1 polymorphisms and incense smoke exposure on the risk of childhood asthma have not been previously studied. Asthma and wheezing are positively associated with the frequency of incense burning. In addition, children carrying the GSTT1 null genotype are most susceptible to the adverse effects of incense smoke.
The factors examined - age, gender, parental education, family income, parental history of atopy, gestational age, residence, maternal smoking, pre- and post-natal ETS exposure, pets and cockroaches at home, dampness of the house, fungus on the house wall, and carpets at home - may all confound the results. As such, they are all considered as potential confounders in this survey and those who made 10% change in point estimates in the statistical procedures have been adjusted. Those with smoking habits have also been eliminated as study subjects to avoid the confounding effect of active smoking. In addition, the subjects were all Han
Chinese, with the premise that they are rather homogeneous. Therefore, the confounding effect of ethnicity is less.
Since the frequencies of incense burning are associated with increased risk of current asthma and medication use instead of lifetime asthma, it is suspected that incense burning may play a more important role in exacerbating asthmatic symptoms among GSTT1 null children. Consistent with a previous epidemiologic study, Al-Rawas et al. also report that incense burning is a common trigger of worsening of wheezing among asthmatic children but is not associated with the prevalence of asthma [18]. Furthermore, Yang et al. have also discovered that incense burning and mosquito repellant burning are significantly associated with acute cough symptoms in primary school children [19].
and respiratory symptoms among primary school children and their non-smoking mothers in Hong Kong [20]. The age of the study population and the constituents of incense from different countries are all be possible contributors to discrepancies in findings.
The biological mechanisms by which the toxic effects of incense burning results in asthma are not well understood. It was reported that molecules emitted from burning incense include CO, CO2, NO2, SO2, DEP, and PMs. Exposures to NO2 and SO2 can lead to
respiratory illness, reduced pulmonary function, and alterations in the lung's defense system [21]. Incense burning also produces volatile organic compounds (VOCs) like benzene, toluene, isoprene, xylenes, aldehydes, and PAHs [6]. These compounds may lead to nose and throat irritation, asthma exacerbation, and cancer.
Aside from irritated respiratory tracts, Lin et al. also report that incense burning may cause elevated cord blood IgE [22]. It is plausible that PMs stimulate dendritic cells and T cells to produce Th2 cytokines and activate pro-inflammatory genes in a process mediated by free radical and oxidative stress mechanisms [23]. Since exposure to lead can stimulate IgE production, it is speculated that lead emitted from incense burning first attaches to PMs, subsequently transferring to fetal blood and modulating the fetal immune system with IgE production [22,24]. Furthermore, incense smoke also causes morphologic changes of
pneumocytes and infiltrates of neutrophils in rat alveoli [25]. Activation of inflammatory cells may lead to amplification of various mediators, ending in inflammatory changes and airway remodeling [26].
Frequency of incense burning is associated with increased risk of asthma in an
exposure-response manner in this study. After stratification by GSTT1 genotypes, the effect of incense burning remains only in the GSTT1 null genotype. The GSTT1 also shows
significant synergistic interaction with incense burning on current asthma, with OR=1.40
CI=0.77-2.40) for incense exposure GSTT1 present genotype, and OR=1.92 (95%
CI=1.11-3.32) for incense exposure GSTT1 null genotype. Previously, however, variants in the GSTM1 and GSTP1 loci reportedly contribute to the occurrence of childhood asthma, thereby increasing susceptibility to adverse effects of tobacco smoke [10,14]. The differences in genotype findings compared to other studies can be due to ethnic compositions and various distributions of genotype frequencies. There is a higher frequency of GSTT1 genotype in this study population than in Caucasians (48.1% vs. 25.0%) [27]. Such inconsistent results may underscore the inherent weakness of single-gene analyses for the study of gene-environment interactions for a multi-gene disease like asthma. Since different polymorphisms of the GSTT1 gene have different effects on the detoxification ability of an individual, an incense
smoke-induced airway injury is different in children carrying different GSTT1
polymorphisms. The statistically suggested interactions in this study add to the plausibility of
a biological interaction between the GSTT1 enzyme and incense smoke in the detoxification
process of reactive metabolic intermediates and reactive oxygen species (ROS) [28,29].
Furthermore, Cornelis et al. report that consumption of cruciferous vegetables is associated
with lower risk of myocardial infarction only among those with a functional GSTT1 allele,
which suggests that GSTT1 carriers can protect against oxidative stress or DNA damage
[28,30].
Consistent with previous studies, the GSTT1 null genotype is associated with increased risk of asthma [11,31]. A possible explanation for this is that GST enzymes, largely expressed in human lung cells, act as detoxifying enzymes and serve as markers of putative oxidative stress [32]. Furthermore, altered anti-oxidant defenses, lipid peroxidation, and
anti-inflammation pathways are important in asthma pathogenesis [33]. It can be speculated that asthma caused by incense smoke partially contributes to DNA damage, which can occur from the lack of detoxification of reactive smoke metabolites by the GSTT1 enzyme [27,34].
However, evidence for an association between GSTs and asthma is inconsistent. The findings
of Minelli et al. do not support a substantial role of GST genes alone in the development of
asthma [35]. Future large scale studies about interactions of GST genes with environmental
oxidative exposures and other genes involved in antioxidant pathways among genetically
susceptible individuals are necessary.
This study has some potential limitations that may influence the interpretation of the results. First, the degree of ventilation of the room where incense was burned is not known. The amount of incense smoke inhaled will be biased because incense exposure has been calculated based on the questionnaire. There is also no good quantitative biomarker for incense burning presently. Exposure assessments from the questionnaire are regarded as appropriate surrogate measurements of incense smoke exposure, which may be subject to misclassification bias. Furthermore, the study subjects are likely to be exposed to other sources of incense aside from their own houses. If incense smoke exposure from temples or other places are included in the analyses, the current amount of incense smoke used will most likely double or triple. Misclassification bias will then shift the results toward the null.
Another possible limitation is recall bias as regards respiratory outcomes. The recall of
asthma status was assessed in a subset of the study population and found that the concordance of parental reports of asthma and medical records’ documentation of asthma was good.
One of the strengths of this study is its inclusion of a large and socio-demographically diverse population of children in Taiwan. Unbiased observations of the association between genetic polymorphisms and outcomes are expected. In addition, the association between incense burning has been investigated with many respiratory outcomes. By current knowledge, the interaction of genetic polymorphisms and incense burning on respiratory manifestations has not been previously reported. The results here suggest that genotyping for the GSTT1 polymorphism, a simple and inexpensive assay, may be a suitable biomarker for identifying
genetically susceptible children.
In conclusion, household incense exposure has adverse effects on children carrying the GSTT1 null genotypes. These findings not only help understand the etiology of asthma but also guide potential control measures in the future. The diverse detoxification ability of incense smoke depends on variations of GSTT1 polymorphisms. Since incense smoke is a complex mixture of chemicals and other metabolic genes may be involved, additional long-term research is warranted to explore the relative role of other genes in determining genetic susceptibility to adverse respiratory outcomes.
ACKNOWLEDGEMENTS
The authors thank all of the field workers who supported the data collection, the school administrators and teachers, and especially the parents and children who participated in this study. This study was supported by the grant #98-2811-B-002-137 and #96-2314-B-006-053 from Taiwan National Science Council and Department of Health in Taiwan. The funding source had no role in the design or analysis of the study.
REFERENCES
1.Yan DC, Ou LS, Tsai TL, Wu WF, Huang JL. Prevalence and severity of symptoms of asthma, rhinitis, and eczema in 13- to 14-year-old children in Taipei, Taiwan. Ann Allergy Asthma Immunol 2005; 95:579-585.
2. Anderson HR, Ruggles R, Strachan DP, et al. Trends in prevalence of symptoms of asthma, hay fever, and eczema in 12-14 year olds in the British Isles, 1995-2002: questionnaire survey. BMJ 2004; 328:1052-1053.
3. Douwes J, Pearce N. Asthma and the westernization 'package'. Int J Epidemiol 2002;31: 1098-1102.
4. Wen CP, Levy DT, Cheng TY, Hsu CC, Tsai SP. Smoking behaviour in Taiwan, 2001. Tob Contro. 2005; 14 Suppl 1:i51-i55.
5. Bureau KHCEP. Reduction of Pollutants in Tamples. In Total Inventory Control of Air Pollutants and the Guidance Program for Reduction. Kao-Hsiung, Taiwan 2003:6-9. 6. Lin TC, Krishnaswamy G, Chi DS. Incense smoke: clinical, structural and molecular
effects on airway disease. Clin Mol Allergy 2008;6:3.
7. Abdul WA, Mostafa OA. Arabian incense exposure among Qatari asthmatic children. A possible risk factor. Saudi Med J 2007;28:476-478.
8. Chiang KC, Liao CM. Heavy incense burning in temples promotes exposure risk from airborne PMs and carcinogenic PAHs. Sci Total Environ 2006;372:64-75.
9. Sampsonas F, Archontidou MA, Salla E, Karkoulias K, Tsoukalas G, Spiropoulos K. Genetic alterations of glutathione S-transferases in asthma: do they modulate lung growth and response to environmental stimuli? Allergy Asthma Proc 2007;28:282-286.
10. Hanene C, Jihene L, Jamel A, Kamel H, Agnès H. Association of GST genes
polymorphisms with asthma in Tunisian children. Mediators Inflamm 2007; 2007:19564. 11. Kabesch M, Hoefler C, Carr D, Leupold W, Weiland SK, von Mutius E. Glutathione S
transferase deficiency and passive smoking increase childhood asthma. Thorax 2004;59:569-573.
12. Saadat M, Ansari-Lari M. Genetic polymorphism of glutathione S-transferase T1, M1 and asthma, a meta-analysis of the literature. Pak J Biol Sci 2007;10: 4183-4189.
13. Piacentini S, Polimanti R, Moscatelli B, et al. Glutathione S-transferase gene
polymorphisms and air pollution as interactive risk factors for asthma in a multicentre Italian field study: A preliminary study. Ann Hum Biol 2010; 37: 427-439.
14. Romieu I, Ramirez-Aguilar M, Sienra-Monge JJ, et al. GSTM1 and GSTP1 and
respiratory health in asthmatic children exposed to ozone. Eur Respir J 2006;28:953-959. 15. Tsai CH, Huang JH, Hwang BF, Lee YL. Household environmental tobacco smoke and
risks of asthma, wheeze and bronchitic symptoms among children in Taiwan. Respir Res 2010;11:11.
16. Lee YL, Hsiue TR, Lee YC, Lin YC, Guo YL. The association between glutathione S-transferase P1, M1 polymorphisms and asthma in Taiwanese schoolchildren. Chest 2005;128:1156-1162.
17. Al-Rawas OA, Al-Maniri AA, Al-Riyami BM. Home exposure to Arabian incense (bakhour) and asthma symptoms in children: A community survey in two regions in Oman. BMC Pulm Med 2009;9:23.
18. Yang CY, Chiu JF, Cheng MF, Lin MC. Effects of indoor environmental factors on respiratory health of children in a subtropical climate. Environ Res 1997;75:49-55. 19. Koo LC, Ho JC, Tominaga S, et al. Is Chinese incense smoke hazardous to respiratory
health? Indoor and Built Environment 1995;4: 334-343.
20. Bernard SM, Samet JM, Grambsch A, Ebi KL, Romieu I. The potential impacts of climate variability and change on air pollution- related health effects in the United States. Environ Health Perspect 2001;109 Suppl 2:199-209.
21. Lin YC, Wen HJ, Lee YL, Guo YL. Are maternal psychosocial factors associated with cord immunoglobulin E in addition to family atopic history and mother immunoglobulin E? Clin Exp Allergy 2004;34:548-554.
22. Donaldson K, Stone V, Borm PJ, et al. Oxidative stress and calcium signaling in the adverse effects of environmental particles (PM10). Free Radic Biol Med
2003;34:1369–1382.
23. Lutz PM, Wilson TJ, Ireland J, et al. Elevated immunoglobulin E (IgE) levels in children with exposure to environmental lead. Toxicolog. 1999;134:63-78.
24. Wegmann M. Th2 cells as targets for therapeutic intervention in allergic bronchial asthma. Expert Rev Mol Diagn 2009;9:85-100.
25. Alarifi SA, Mubarak MM, Alokail MS. Ultrastructural changes of pneumocytes of rat exposed to Arabian incense (Bakhour). Saudi Med J 2004;25:1689-1693.
26. Nukui T, Day RD, Sims CS, Ness RB, Romkes M. Maternal/newborn GSTT1 null genotype contributes to risk of preterm, low birthweight infants. Pharmacogenetics 2004;14:569-576.
27. Cornelis MC, El-Sohemy A, Campos H. GSTT1 genotype modifies the association between cruciferous vegetable intake and the risk of myocardial infarction. Am J Clin Nutr 2007;86:752-758.
28. See SW, Wang YH, Balasubramanian R. Contrasting reactive oxygen species and transition metal concentrations in combustion aerosols. Environ Res 2007;103:317-324. 29. Dellinger B, Pryor WA, Cueto R, Squadrito GL, Hegde V, Deutsch WA. Role of free
radicals in the toxicity of airborne fine particulate matter. Chem Res Toxicol 2001;14:1371–1377.
30. Vavilin VA, Makarova SI, Liakhovich VV, Gavalov SM. Polymorphic Genes of
Hereditarily Burdened and Nonburdened Children. Russian Journal of Genetics 2002;38:439–445.
31. Ercan H, Birben E, Dizdar EA, et al. Oxidative stress and genetic and epidemiologic determinants of oxidant injury in childhood asthma. J Allergy Clin Immunol
2006;118:1097–1104.
32. Altinisik J, Balta ZB, Aydin G, Ulutin T, Buyru N. Investigation of glutathione S-transferase M1 and T1 deletions in lung cancer. Mol Biol Rep 2010;37:263-267. 33. Popp W, Vahrenholz C, Schell C, et al. DNA single strand breakage, DNA adducts, and
sister chromatid exchange in lymphocytes and phenanthrene and pyrene metabolites in urine of coke oven workers. Occup Environ Med 1997;54:176–183.
34. Minelli C, Granell R, Newson R, et al.Glutathione-S-transferase genes and asthma
phenotypes: a Human Genome Epidemiology (HuGE) systematic review and
TABLE 1 Selected characteristics of participants in the Taiwan Children Health Study
With genotyping (n=3764) All eligible participants (n=5082)
n % n % Demographic information Boy 1848 49.1 2464 48.5 Age, yr (Mean ± SD) 12.26 ± 0.50 12.42 ± 0.65 Parental education, yr† <=12 2319 62 3201 63.4 13~15 740 19.8 964 19.1 >=16 679 18.2 884 17.5 Gestational age† <=37 335 9.1 461 9.3 >37 3342 90.9 4496 90.7 Parental asthma† 114 3.1 140 2.9 Parental atopy† 957 26.4 1263 25.8 Family income*† <=400,000 1249 35.8 1777 37.7 400,001~800,000 1408 40.4 1853 39.3 >=810,000 828 23.8 1080 22.9 Active smoking† 26 0.7 37 0.7
Maternal smoking during
pregnancy† 146 3.9 198 3.9
ETS at home† 1774 47.4 2471 48.9
Incense burning at home†
Never 1326 37.0 1724 35.8
Less than daily 1021 28.5 1398 29.0
Daily 1237 34.5 1699 35.2 Respiratory Outcomes† Asthma Lifetime asthma 292 7.8 375 7.4 Current asthma 114 3.1 140 2.9 Medication use 96 2.6 123 2.4 Wheeze Lifetime wheeze 449 12.0 586 11.6 Current wheeze 150 4.0 186 3.7 Nocturnal wheeze 82 2.2 109 2.2 Exercise wheeze 206 5.5 276 5.5
*New Taiwan dollars per year ($1 USD = $ 33 New Taiwan dollar). †Number of subjects does not add up to total N because of missing data.
TABLE 2 Effects of incense burning at home and GST genotype on sub-categories of asthma and wheeze
Asthma
Lifetime asthma Current asthma Medication use
OR 95%CI OR 95%CI OR 95%CI
Incense burning 1.05 (0.80,1.36) 1.36 (1.01,2.00) 1.52 (1.02,2.42)
Frequency of incense burning*
Never 1.00 1.00 1.00
Less than daily 0.76 (0.54,1.07) 1.13 (0.70,1.83) 1.29 (0.72,2.30)
Daily 1.22 (0.90,1.64) 1.52 (0.99,2.34) 1.75 (1.03,2.96)
p value for trend 0.20 0.05 0.03
GSTT1 Null 1.21 (0.95,1.56) 1.43 (1.00,2.04) 1.46 (1.01,2.22)
GSTM1 Null 0.87 (0.68,1.12) 0.89 (0.63,1.27) 0.84 (0.55,1.27)
GSTP1 Ile/Ile 1.18 (0.60,2.32) 0.89 (0.37,2.11) 0.72 (0.28,1.85)
Wheeze
Lifetime wheeze Current wheeze Nocturnal wheeze Exercise wheeze
OR 95%CI OR 95%CI OR 95%CI OR 95%CI
Incense burning 1.10 (0.88,1.37) 1.07 (0.75,1.53) 1.31 (0.8,2.14) 1.64 (1.18,2.28)
Frequency of incense burning*
Never 1.00 1.00 1.00 1.00
Less than daily 0.92 (0.70,1.21) 1.00 (0.64,1.56) 1.07 (0.58,2.01) 1.62 (1.09,2.41)
Daily 1.21 (0.94,1.55) 1.12 (0.74,1.70) 1.68 (0.97,2.93) 1.88 (1.29,2.74)
p value for trend 0.13 0.60 0.06 0.001
GSTT1 Null 1.17 (0.95,1.44) 1.14 (0.81,1.60) 1.14 (0.72,1.79) 1.09 (0.81,1.47)
GSTP1 Ile/Ile 0.96 (0.57,1.61) 0.83 (0.37,1.86) 1.21 (0.37,4) 1.76 (0.7,4.41)
Models are adjusted for age, gender, parental education, parental asthma, parental atopy, gestational age, city, maternal smoking during pregnancy, and ETS at home
TABLE 3 Association between incense burning at home and GSTT1 genotype on sub-categories of asthma and wheeze No incense GSTT1 present No incense GSTT1 null With incense GSTT1 present With incense GSTT1 null
OR 95%CI OR 95%CI OR 95%CI
Univariate model Asthma Lifetime asthma 1.00 1.12 (0.76,1.65) 0.87 (0.61,1.25) 1.11 (0.79,1.58) Current asthma† 1.00 1.37 (0.77,2.45) 1.09 (0.63,1.87) 1.56 (0.93,2.63) Medication use 1.00 1.39 (0.67,2.88) 1.25 (0.64,2.44) 1.87 (0.99,3.55) Wheeze Lifetime wheeze 1.00 1.08 (0.78,1.48) 0.87 (0.65,1.17) 1.12 (0.84,1.49) Current wheeze 1.00 0.96 (0.57,1.62) 0.79 (0.49,1.27) 1.03 (0.65,1.63) Nocturnal wheeze† 1.00 0.62 (0.28,1.36) 0.84 (0.45,1.58) 1.19 (0.65,2.16) Exercise wheeze 1.00 1.27 (0.75,2.14) 1.67 (1.06,2.62) 1.68 (1.07,2.66)
Mutually adjusted model *
Asthma Lifetime asthma 1.00 1.14 (0.76,1.70) 0.99 (0.68,1.44) 1.25 (0.87,1.81) Current asthma† 1.00 1.40 (0.76,2.57) 1.36 (0.77,2.40) 1.92 (1.11,3.32) Medication use 1.00 1.32 (0.62,2.79) 1.42 (0.71,2.85) 2.12 (1.09,4.12) Wheeze Lifetime wheeze 1.00 1.08 (0.77,1.50) 1.02 (0.75,1.39) 1.27 (0.94,1.72) Current wheeze† 1.00 1.02 (0.59,1.76) 0.96 (0.58,1.60) 1.20 (0.73,1.97) Nocturnal wheeze† 1.00 0.65 (0.29,1.45) 0.87 (0.44,1.70) 1.30 (0.69,2.46) Exercise wheeze 1.00 1.33 (0.77,2.28) 1.89 (1.17,3.05) 1.91 (1.18,3.09)
home
25 TABLE 4 Association of frequency of incense burning at home on sub-categories
of asthma and wheeze by GSTT1 genotype
GSTT1 present (n=1937) GSTT1 null (n=1801)
Frequency of incense burning* OR 95%CI OR 95%CI
Asthma
Lifetime asthma
Never 1.00 1.00
Less than daily 0.74 (0.45,1.21) 0.74 (0.45,1.22)
Daily 1.04 (0.66,1.63) 1.42 (0.94,2.13)
p value for trend† 0.87 0.09
Current asthma
Never 1.00 1.00
Less than daily 1.22 (0.60,2.50) 1.05 (0.54,2.05)
Daily 1.37 (0.69,2.75) 1.78 (1.01,3.16)
p value for trend† 0.37 0.04
Medication use
Never 1.00 1.00
Less than daily 1.22 (0.51,2.92) 1.35 (0.60,3.00)
Daily 1.37 (0.59,3.18) 2.26 (1.11,4.57)
p value for trend† 0.47 0.02
Wheeze
Lifetime wheeze
Never 1.00 1.00
Less than daily 0.96 (0.65,1.41) 0.85 (0.57,1.26)
Daily 1.02 (0.70,1.49) 1.40 (1.00,1.98)
p value for trend† 0.91 0.04
Current wheeze
Never 1.00 1.00
Less than daily 0.78 (0.40,1.50) 1.15 (0.62,2.14)
Daily 1.01 (0.55,1.87) 1.17 (0.65,2.11)
p value for trend† 0.97 0.60
Nocturnal wheeze
Never 1.00 1.00
Less than daily 0.86 (0.38,1.96) 1.20 (0.45,3.23)
Daily 0.85 (0.37,1.95) 3.21 (1.41,7.30)
26
Never 1.00 1.00
Less than daily 2.03 (1.16,3.54) 1.28 (0.71,2.31)
Daily 1.86 (1.06,3.28) 1.99 (1.18,3.35)
p value for trend† 0.04 0.01
Models are adjusted for age, gender, parental education, parental asthma, parental atopy, gestational age, city, maternal smoking during pregnancy, and ETS at home *Average days of incense burning at home per month