A Knowledge Based Systems Framework for Healthcare Institution Clinical
Practice-Literature Review from 2000 to 2007
陳福基
a*, 黃援傑
aFu-Ji Chen
a*, Yuan-Chieh Huang
aa
三軍總醫院資訊管理室
*
通訊作者
:
陳福基
, [email protected]
Abstract
Clinical decision-making is a knowledge intensive activity which can be vastly improved by providing the right knowledge, in the right form, to the right person at the right time. But that goal is not being fully met by current information systems. The purpose of this paper is to highlight the lack of attention paid to knowledge-based systems and the need for further research in this area. Towards that end, this paper analyzes recent research related to knowledge management issues in the healthcare industry, and we adopt Nonaka‘s SECI framework to examine healthcare knowledge-base systems which have been the subject of articles, published between 2000 and 2007, in four medical informatics journals. The result of this effort will eliminate many of the knowledge gaps regarding the process of creating optimized medical knowledge management systems (KMS) applications, and thereby increase both the scope and depth of medical knowledge management research. Keywords: Decision support; Knowledge management; Knowledge-based systems
1、 Introduction
Drucker (1993) argues that in the new economy, knowledge is not just another resource alongside traditional factors of production (i.e. labor, capital, and land), but rather it has become the only meaningful resource today. A ‘knowledge-based perspective’ of the firm has emerged in the strategic management literature (Nonaka & Takechi, 1995), that postulates the services rendered by tangible resources depend on how they are combined and applied, which is in turn a function of the
firm’s know-how (Alavi, 2001). Such know-how is entwined with the firm’s culture, policies, routine procedures and individuals. Naturally, these factors are socially complex and difficult to imitate. Thus the knowledge-based view of the firm posits that those knowledge assets may produce long-term sustainable competitive advantages.
The central issue of knowledge management is not unique to profit organizations, but also influences the healthcare industry. A value of a modern healthcare organization lies more in its intellectual and service capabilities than in its hard assets (traditional production factors), and it is primarily in this base that the potential for competitiveness resides. Therefore, understanding the knowledge creation process and mechanisms of knowledge management is a pivotal issue.
Therefore, we have selected four medical informatics journals for this study, each of which the scientific citation index(SCI)rates with an impact factor of more than 1.9. Those journals are: Journal of the American Medical Informatics Association(JAMIA), International Journal of Medical Informatics(IJMI), Artificial Intelligence in Medicine(AIM),and Journal of Biomedical informatics. The purpose of this study is to analyze the medical informatics literature with regard to knowledge-base systems. Using the Socialization, Externalization, Combination, Internalization framework (SECI model) developed by Nonaka(1995), we will classify each of these huge research articles into one of the four knowledge-creating quadrants. Our objective of the analysis is to raise medical informatics and clinical practitioner awareness of the potentials and implications
of the different knowledge creation processes. 2、 Literature review
2.1.The hierarchical view of data, information, knowledge
The words we use to describe what we know about the world are often entangled and overlap; terms like data, information, and knowledge are often ambiguous in common speech. Some authors have addressed the question of defining knowledge by distinguishing among data, information, and knowledge. A simple way to conceptualize the difference between these terms is to think of a hierarchy of meaning. The hierarchy starts with raw data at the bottom, then moves up through information, and ends at the top with knowledge. Each of these layers builds upon the one below so that meaning increases as we move up the hierarchy (Coiera, 1997).
From the hierarchy perspective ‘data’ is raw numbers and facts(ex. Blood pressure is 127/70 mm HG), whereas information is processed data, and is usually taken to mean data that gains significance in a certain context(ex. The data may inform a clinician that a patient’s blood pressure is under control). Knowledge is authenticated information(ex. Rule “if a patient’s blood pressure is grater that 135/95 mm HG on separate occasions then the patient has high blood pressure”) (Vance, 1997). Through the hierarchy approach we can see how each of the three layers of knowledge is related.
In a less mechanical way knowledge can be described as a medical expert practicing his/her art, someone that has superior long-term and short-term memory as part of their expertise who is capable of perceiving large, meaningful patterns inherent in data and information. The weakness of this purely subjective, tacit approach to knowledge lies in human error; it is possible that inadequate data will be interpreted as meaningful information and then used to support a physician’s decision making. Of course, the optimum approach would be to use both computerized and human knowledge in an interactive way so as to shore-up the
inherent weaknesses in each stage of building a meaningful knowledge building system.
2.2. Knowledge creation process and the knowledge spiral
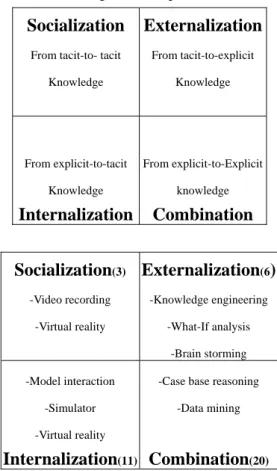
New knowledge is created through the synergistic relationship and interplay between tacit and explicit knowledge ( Nonaka & Takeuchi, 1995 ) , especially through a four step process of socialization, externalization, combination, and internalization(Table 1).
Socialization is the process of sharing with others experiences, technical skills, mental models, and other forms of tacit knowledge. For example, resident physicians work side by side with senior physicians and learn craftsmanship, not just through language, but through observation, imitation, and practice. Externalization is the process of converting tacit knowledge into explicit knowledge. Writing is an act of converting tacit knowledge into articulated knowledge; for example, engaging in techniques such as brainstorming which gathers tacit knowledge into verbalized streams of external text. Combination is the process of combining several types of explicit knowledge into new explicit knowledge. For example, this includes techniques such as the ‘meta analysis’ of literary approaches to uncover new patterns and relationships of explicit knowledge. Internalization is the process of testing and validating the new relationship in the proper context, thereby converting externalized explicit knowledge back into new tacit knowledge. As we will show, this four-step process of knowledge creation can be supported and optimized by targeted knowledge building management.
Table 1 Knowledge creation process
Socialization
From tacit-to- tacitKnowledge
Externalization
From tacit-to-explicit Knowledge From explicit-to-tacit KnowledgeInternalization
From explicit-to-Explicit knowledgeCombination
Socialization
(3) -Video recording -Virtual realityExternalization
(6)
-Knowledge engineering -What-If analysis -Brain storming -Model interaction -Simulator -Virtual realityInternalization
(11)-Case base reasoning -Data mining
Combination
(20)3. Conclusion
In the medical field, medical information systems accumulate enormous numbers of healthcare records daily. By appropriate management, the heterogeneous data can be converted into valuable knowledge. Such knowledge will be useful to a physician’s daily decision-making process, and the enhanced organization of this knowledge will be an intelligent asset to strengthen healthcare institutions performance.
The complete knowledge creation process includes socialization, externalization, combination, and internalization. Our analysis highlights the majority of published knowledge management research. The results show that the portfolio of knowledge management research in the healthcare literature is biased toward explicit knowledge. In particular, tacit to tacit knowledge sharing has been ignored in the medical informatics literature. This implies that tacit knowledge is left largely unexamined (table1 socialization paper count). We further challenge researchers to consider broadening their range of exploration and consider knowledge perspectives
other than the ones with which they are most comfortable. The aim of this endeavor is to eliminate the gaps in understanding regarding the medical knowledge creation processes, and thereby to broaden the scope of medical knowledge management research.
Reference
A. Aamodt, E. Plaza, (1994) ‘Case-base Reasoning: Foundational Issues, Methodological Variations and Systems Approaches’, AI Communication (7), pp.39-59.
Abidi SSR, Manickam S. (2002) ‘Leveraging XML-based electronic medical records to extract experiential clinical knowledge: An automated approach to generate clinical cases for medical case-based reasoning systems’, Int J Med Informatics, No.68, pp.187-203.
Alavi,M. & Leidner,D.E. (2001) ‘Knowledge Management and Knowledge Management Systems : Conceptual Foundations and Research Issues’,MIS Quarterly, 25(1), pp.107-136.
Anderson, J. R. (1983). The architecture of cognition. Cambridge, MA: Harvard University Press.
Bichindaritz, I., Marling, C. (2006) ‘Case-based reasoning in the health sciences: What's next? ’, Artificial Intelligence In Medicine, 36(2), pp. 127-135 .
Duane K. Bowman, (1995) ‘International Survey: Virtual-Environment Research’, IEEE Computer, June, pp.56-65.
Drucker, P. F. (1993). Post-capitalist society. New York: Harper Business.
Edmund C. Payne, Robert C. McArthur, (1990) ‘Developing Expert Systems: A Knowledge Engineering’s Handbook for Rules& Objects’, John Wiley & Sons, INC Press, 1990
Goel, V. Moehr, J. Browman, G.. (1998) ‘The role of group support technology in developing the HEALNet research agenda’, Int J Med Informatics, 51, pp.215-219.
Goodwin, L., VanDyne, M., Lin, S., Talbert, Steven.(2003) ‘Data mining issues and opportunities for building nursing knowledge’, Journal of Biomedical Informatics, 36(4-5), pp. 379-388.
Gourlay, D. Lun, K.C. Lee, Y.N. Tay, J. (2003) ‘Virtual reality for relearning daily living skills’, Int J Med Informatics,60, pp.255-261.
Harris M.R., Judith R. G. R. Harold.(2000) ‘Embedded structure and representation of nursing knowledge’, Journal of American Medical Informatics Association, 7(6) pp: 539-549.
Hogue, Jack T. Hough J. Watson. (1985) ‘An Examination of Decision Maker’s Utilization of Decision Systems Output’, Information & Management, 8(4), pp.205-212.
Hamid R. Nemati , David M. Steiger , Lakshmi S. Iyer , Richard T. Herschel, (2002), ‘Knowledge warehouse: an architectural integration of knowledge management, decision support, artificial intelligence and data warehousing’, Decision Support Systems, 33(2), pp.143-161
Holsapple, C. W. and A. B. Whinston.(1996), Decision Support Systems: A Knowledge Based Approach. Minneapolis, MN: West Publishing, Inc.
Hripcsak, G., Bakken, S., Stetson, Peter D., Patel, Vimla L. (2003) ‘Mining complex clinical data for patient safety research: a framework for event discovery’, Journal of Biomedical Informatics,36(12), pp. 120-130.
I. Nonaka, H. Takeuchi, (1995) ,The Knowledge Creating Company, New York, NY:Oxford University Press. Kushniruk, A. W. (2001) ‘Analysis of Complex
Decision-Making Processes in Health Care: Cognitive Approaches to Health Informatics’, Journal of Biomedical Informatics, 34(5), pp.365-376. Lau, Francis, Robert Hayward. (2000) ‘Building a virtual
network in a community health research training program’, Journal of American Medical Informatics Association, 8(4), pp:361-377.
Lin, F. r. Chou, S.c. Pan, S.m. Chen, Y.m.(2001) ‘Mining Time Dependency patterns in clinical pathways’, Int J Med Informatics, 62: pp.11-25.
Poynton, M. R., McDaniel, Anna M. (2006) ‘Classification of smoking cessation status with a back propagation neural network,’ Journal of Biomedical Informatics, 39(6), pp. 680-686.
Radetzky, A. Rudolph, M. (2001) ‘Simulating tumor removal in neurosurgery’, Int J Med Informatics,64, pp.461-472.
Radetzky, A., Nürnberger, A.(2002) ‘Visualization and simulation techniques for surgical simulators using actual patient’s data,’ Artificial Intelligence in Medicine , 26(3), pp. 255-279.
Romero, C., Ventura, S., Gibaja, E. L., Hervás, C.(2006) ‘Web-based adaptive training simulator system for cardiac life support’, Artificial Intelligence In Medicine, 38(1), pp. 67-78.
S. Achour, M. Dojat, C. Rieux, P. Bierling and E. Lepage.(2001)‘A UMLS-based knowledge acquisition tool for rule-based clinical decision support system development’, Journal of the American Medical Informatics Association,8(4), pp. 351–360.
S. Svacina, R. Hovorka, T. Haas, Z. Masek, J. Kabrt,(1991) ‘Ten Years Of Computer Support of Metabolic Intensive Care Unit. Medical Informatics Europe’, Lecture notes in Medical Informatics 45, Springer Verlag, Berlin, pp.930-933.
Sørensen T. S., Søren V. T., Piotr Makowski, Jørgen L. K. and Erik M. P.(2001) ‘A newvirtual reality approach for planning of cardiac interventions’, Artificial Intelligence in Medicine, 22(3), pp. 193-214.
Su, S. Shih, C. L. (2003) ‘Modeling an emergency medical services system using computer simulation’, Int J Med Informatics,72, pp.57-72.
Sieger, R. S. (1989). ‘Mechanisms of cognitive development’, Annual Review of Psychology, 40, 353-379.
R. Serban, Annette T. T., Frank V. H., Mar M., Cristina Polo-Conde. (2007) ‘Extraction and Use of Linguistic Patterns for Modeling Medical Guidelines’ ,Artificial Intelligence in Medicine, 37, pp.137-149 .
Temkin B, Acosta E, Hatfield P, Onal E, Tong A. (2002) ‘Web-based three-dimensional virtual body structures: W3D-VBS,’ Journal of Medical Informatics Association, 9(5), pp. 425-436.
Vance, D. M.(1997) ‘information, knowledge and wisdom: The Epistemic Hierarchy and Computer-Based Information System’, Proceedings of The Third Americans Conference on Information Systems, B. Perkins and I. Vessey (eds), Indianapolis, IN.
Zack, M. (1998) ‘What Knowledge-Problems Can Information Technology Help to Solve’, Proceedings of the Fourth Americans Conference on Information Systems, pp. 644-646.