Kaohsiung J Med Sci October 2008 • Vol 24 • No 10
514
Duchenne muscular dystrophy (DMD) takes a slow and arduous course that leads to many serious prob-lems including parental strain. Coping with DMD, depending on the level of a child’s disability, may deplete family energy and resources [1]. In general, families receive professional information about DMD
at the time the child is first diagnosed [2]. Some re-searchers have explored age at diagnosis as a potential mediator or moderator of family function [3], but no study has explored family hardiness, caregiver health, or family support in this regard. In one study, path analysis and structural equation modeling indicated that age at diagnosis, family hardiness, caregiver health and family support all had direct effects on family func-tion [3]. Earlier diagnosis permits greater interacfunc-tion with health professionals, fostering more effective interventions and better family adaptation [3].
Discovering clinical mediators or moderator factors among the variables that affect families with DMD
Received: Aug 25, 2008 Accepted: Nov 18, 2008 Address correspondence and reprint requests to: Dr Jih-Yuan Chen, School of Nursing, Kaohsiung Medical University, 100 Shih-Chuan 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
M
EDIATORS
A
FFECTING
F
AMILY
F
UNCTION IN
F
AMILIES OF
C
HILDREN WITH
D
UCHENNE
M
USCULAR
D
YSTROPHY
Jih-Yuan Chen
School of Nursing, Kaohsiung Medical University, Kaohsiung, Taiwan.
Most families of children with Duchenne muscular dystrophy (DMD) first receive professional information about the disease at the time of their child’s diagnosis. Generally, as the families begin to build a supportive care system for their children, the parents will research DMD on their own or gather formal knowledge about the disease from professionals. However, gaining access to care is a major challenge because they often do not know how to ask the right questions. In particular, vulnerable populations may experience difficulties in assisting their child’s emotional adjustment to the disability and use of available services. The purpose of this study was to test the possible effects of psychosocial mediators of parental health, family hardiness and family support on family function in relation to the age at diagnosis of children with DMD. One hundred and twenty-six Taiwanese parents of children with DMD who are members of the Taiwan Muscular Dystrophy Association filled out questionnaires. Subjects received a phone call before and again within the first week after we mailed them a questionnaire, a stamped return-addressed envelope, and a consent form. The questionnaires included the Family Hardiness Index, Family Assessment Device, Family APGAR, Duke Health Profile and demographic questions. Hierarchical multiple regressions were conducted to test whether family hardiness, parental health, or family support mediated or moderated the association between age at diagnosis and family function. Family hardiness positively mediated the association between age at diagnosis and family function. These findings may help the design of interventions to develop family hardiness in families of children with DMD.
Key Words:Duchenne muscular dystrophy, family functioning, family hardiness, family support, parental health
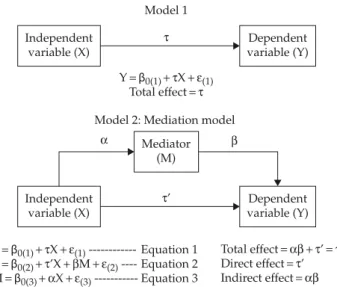
children may help to prepare the families to partici-pate in treatment decisions related to their children. Mediation hypotheses posit how or by what means a causal effect occurs, and how one variable predicts or causes an outcome variable. In contrast, moderators address when or for whom a factor is more strongly related to an outcome. More specifically, a mediator is defined as a potential intervening variable (M) that explains the relation between a predictor (X: inde-pendent variable) and an outcome (Y: deinde-pendent variable) [4,5]. In other words, a hypothesis that a predictor is related to or causes a mediator should have a theoretical rationale [6]. The predictor causes the mediator which, in turn, causes the outcome; the mediator should be something that can be changed. The main purpose of mediator analysis is to examine why an association between a predictor and outcome exists. Understanding such complex relationships among variables can also provide a theory-base for intervention.
C
ONSTRUCTION OF ANA
NALYTICALM
ODELWe developed a Model for Stressors, Resources, and Functioning (Figure 1) [3] based on the Resiliency Model of Family Stress, Adjustment, and Adaptation [7]; using correlations among variables, confirmatory factors analyses, and hierarchical multiple regression analysis from predictor variables with dichotomous responses (two categories, usually coded 0 and 1); family income, employment, parent health, family support, family hardiness, child disability, and age at diagnosis were classified into two domains: family
resources and family stressors [3]. These seven vari-ables were termed components of family resources; the other variables (child disability and age at diag-nosis) were termed components of family stressors.
Family stressors include a child’s disability and age at diagnosis, as measured by scales of individual complete dependence (Barthel Index) [8], and reported age when diagnosed with DMD. Family resources in-cluded five potential mediating variables that are all measured with a demographic sheet, the individual Duke Health Profile (Duke) [9], Family APGAR [10], and Family Hardiness Index [11]. These variables are defined below.
Parents’ employment and annual income were the most important variables regarding family character-istics of the family resources in our model. The Duke measures parental health as physical, psychological, social and emotional health of parents. Family support represents the parents’ satisfaction and examines how parents perceived support in the five attributes of adaptation, partnership, growth, affection, and resolve [12]. Family hardiness is conceptualized as the energy resource that includes commitment, challenge, and control [7]. Family function represents families’ abili-ties, including problem solving, communication, role, affective responsiveness, affective involvement, and behavioral control. It is used to evaluate family adap-tation and uses a scale based on the individual Family Assessment Device (FAD) [12].
The objective of this study was to explore the influ-ence of selected family resource variables on family function. The study hypotheses were as follows: family resources, including parental health, family hardiness and family support, might be mediated by or moderate the association between age at diagnosis and family functioning. If this assumption is true, the final effect of family stressors on the reduction of family func-tion will depend on the effect of family characteristics, healthy parent status, family support, and family hardiness on family resources, in the intermediate process.
M
ETHODSStudy design and procedures
This cross-sectional study used hierarchical multiple regression analysis to explore the mediating effects of parental health, family hardiness and family support
Mediating variable Family resources
• Family characteristics (employment, annual income) • Parental health (DUKE) • Family support (FAPGAR) • Family hardiness (FHI) Independent variable Family stressors • DMD child’s disability (Barthel Index) • Age at diagnosis Dependent variable Family functioning • Family Assessment Device (FAD)
Figure 1.Conceptual model for family stressors, resources and function.
on the effects of the variables “age at diagnosis” and “family function” for parents of children with DMD.
The study was approved by the institutional review board of Kaohsiung Medical University, and participating parents with DMD children. A conve-nience sample (203 parents) was recruited from the Taiwan Muscular Dystrophy Association (TMDA) and from patient rolls at Kaohsiung Medical University Hospital. Members of the TMDA received a letter from the association inviting their participation in the study. Subjects who agreed to participate were mailed a packet consisting of two sets of questionnaires and informed consent forms. Follow-up telephone calls were made at 1 and 2 weeks after the questionnaires were mailed to promote the completion and return of the question-naires by each parent. Subjects reported an average time of 40 minutes to complete the questions at home.
Sample
A “family” was defined as a child with DMD living with one or both biological parents. The parents, in-cluding eight single fathers, 26 single mothers, and 46 couples, returned completed questionnaires (62%). Their mean age was 43± 6.1 years (range, 28–61 years). Most of the respondents were female (57%). Respon-dents’ religion was primarily Buddhist (50%) or Taoist (36%), and ethnicity was Taiwanese (76.2%), Hakka (11.9%), or Chinese (10.3%); over half had at least 12 years of education (57.7%) and were employed (56%); most were married (90.5%), and some worked as a laborer or farmer (26%). The families reported an annual income of less than US$10,000 (44%) to over US$30,000 (10%). Forty-eight (60%) families lived in urban areas.
The DMD children ranged in age from 3 to 25 years (mean, 14.3± 4.6 years). Most were teenagers (41%) and needed wheelchair assistance (73%) or could not raise a hand to their mouth (46%). The mean age when diagnosed with DMD was 6.2± 2.8 years (range, 1–15
years). The DMD children rated a score of 21–60 or 0–20 on the Barthel index, indicating severe depen-dency (47.5%) and complete dependepen-dency (35%), re-spectively. About 73% of the DMD children still received education at home.
Data management and analysis
Steps involved in analyzing the data included creating or transforming predictor and moderator variables (coding categorical variables, centering continuous variables), creating product terms, and structuring the equation. Mean-centered predictor variables (main effect variables before entering them in the model, which center a variable by subtracting the group’s mean from all observations) were used throughout the analysis to eliminate multicollinearity when variables and interaction terms entered the regression equation model. Hierarchical multiple regression analyses were conducted to test whether family hardiness, parental health, and family support mediated or moderated the association between age at diagnosis and family function.
An analysis resulted in an α of 0.05, and power of 0.86 was reached for the sample size of 126 subjects with a medium (0.15) effect on the regression [13]. There was high internal consistency and reliability using Cronbach’s α coefficients that ranged from 0.81 to 0.92 (Table 1) for the instruments in the present study. The construct validity of the FAD was appropriate [14]. FAD provided adequate evidence for the concurrent validity.
R
ESULTSRelationships among predictor variables
and dependent variables
Based on the correlations, age at diagnosis of DMD showed a significant trend in its association with family
Table 1.Normative data of the instruments in the current study
Instruments Items α Range Theoretical range Mean± SD
Barthel Index* 10 0.88 10–100 0–100 38.65± 25.40
Duke Health Profile 17 0.81 29.41–100 0–100 67.48± 15.79
Family Hardiness Index 20 0.81 12–58 0–60 41.20± 7.90
Family APGAR 5 0.89 0–10 0–10 6.63± 2.86
Family Function 60 0.92 1.33–2.97 1–4 2.11± 0.30
hardiness (r= −0.21, p = 0.02) and family function (r = 0.20, p= 0.02), but not with parental health (r = 0.01, p=0.88) or family support (r=−0.01, p=0.94), indicating that age at diagnosis was a significant predictor of family hardiness and family function. The results indicated that child disability (r= 0.06, p = 0.52), family annual income (r= 0.17, p = 0.06) and employment (r= −0.06, p = 0.48) were not significant predictors for family function. Inverse relationships were found for healthy family function of the parents with higher family hardiness (r= −0.743, p = 0.00), greater family support (r= −0.66, p = 0.00), and better parental health (r= −0.60, p < 0.01). These results indicate that these four variables were predictive of each other and had a theoretically positive correlation. Family hardiness and family support were significant predictors of parental health.
Mediation test
The most commonly used hierarchical multiple regres-sion test for mediator effects involves three criteria for determining mediation, as shown in Figure 2 [15,16]. The first step in the process is to determine whether there is a significant association between a predictor and an outcome variable. A mediating relationship is one in which the path relating X to Y is mediated by a third variable (M). In this study, the correlation between age at diagnosis and family hardiness was −0.209, which was significant at p=0.019. But the author hypothesized that this relationship was mediated by family hardiness, such that, if the child with DMD was younger at age of diagnosis, the family would have
greater family hardiness, which would, in turn, lead to improved family function.
The author developed three equations (Figure 2) to test the hypothesis. The results are shown in Figure 3. First, testing showed that, for the mediation hypothesis to be true, the regression for each step had to be sig-nificant. Family function was regressed on age at diag-nosis and family hardiness. Second, family hardiness was regressed on age at diagnosis to establish α in the mediator chain. In the third equation, family function was regressed on age at diagnosis and family hardi-ness. This provided a test of whether family hardiness was related to family functioning (β) as well as an estimate of the association between age at diagnosis and family function, controlling for family hardiness (τ’) [16,17]. Results indicated that age at diagnosis was the best predictor for family function (β = 0.202, p= 0.023, Equation 1: Family function = 1.975 + 0.202 × age at diagnosis+ 0.009) (Figure 3A).
Adding family hardiness to the equation did not increase the explained variance (R2= 0.547, F
(2, 123)=
76.576, p= 0.00). The mediator function of family har-diness was substantiated first by the reduction of the path coefficient from 0.202 to 0.049 (Table 2), but age at diagnosis did not significantly decrease in the equation [β = 0.049, p = 0.425 (Figure 3A), Equation 2: Family function =3.192+0.049×age at diagnosis −0.733×family hardiness+0.110; Equation 3: Family hardiness =44.82− 0.209× age at diagnosis + 1.651] (Figure 3A). Third, the interaction between age at diagnosis and family hardiness (R2=0.549, F(3, 122)=51.670, p=0.00; F change=
1.382, p= 0.242) was entered to assess its significance (Table 2).
A mediator model is supported if the model with a direct path between age at diagnosis and family functioning does not provide better fit to the data. With exclusion of age at diagnosis in the third step, the explained variance in family function significantly decreased for age at diagnosis (β = 0.066, p = 0.242) (Table 2). Keeping in mind that lower family function scores reflect better function, diagnosis at a later age was associated with lower family function. In addition, given the inverse scoring of FAD for family function (with lower scores indicating better function), these findings indicate that, as family hardiness scores in-creased, family function also increased. The causal model did not engage moderation because the path from the interaction of age at diagnosis and family hardiness to family functioning was not significant [18].
Model 1
Y= β0(1)+ τX + ε(1)
Total effect= τ Model 2: Mediation model
Y= β0(1)+ τX + ε(1) --- Equation 1 Y= β0(2)+ τ’X + βM + ε(2) ---- Equation 2 M= β0(3)+ αX + ε(3) --- Equation 3 Total effect= αβ + τ’ = τ Direct effect= τ’ Indirect effect= αβ α β τ’ Independent variable (X) Dependent variable (Y) Dependent variable (Y) Independent variable (X) Mediator (M) τ
Figure 3.Mediator model: age at diagnosis influences family function through family hardiness. (A) Mediator model
Independent variable
β = 0.202, p = 0.023
Step 1: Age at diagnosis Family function
Family function Family hardiness
β = −0.733, p = 0.000 β = −0.209, p = 0.019
Step 2: Age at diagnosis
Dependent variable β = 0.049, p = 0.425 (B) Non-mediator model Family function Parental health β = −0.601, p = 0.000 β = 0.014, p = 0.879
Step 2: Age at diagnosis
β = 0.21, p = 0.003 (C) Non-mediator model Family function Family support β = −0.659, p = 0.000 β = −0.007, p = 0.941
Step 2: Age at diagnosis
β = 0.198, p = 0.003
Table 2.Family function regressed on child’s age at diagnosis, family hardiness, parental health, and family support β values
Step 1 Step 2 Step 3
Age at diagnosis 0.202* 0.049 0.066
Family hardiness −0.733† −0.884†
Age at diagnosis× family hardiness 0.171
R2 0.041 0.547 0.549
F 5.286* 76.576† 51.670†
F change 5.286* 141.862† 1.382
Age at diagnosis 0.202* 0.210† −0.275
Parental health −0.601† −0.859†
Age at diagnosis× parental health 0.565
R2 0.041 0.402 0.416
F 5.286* 41.368† 28.996†
F change 5.286* 74.326† 2.945
Age at diagnosis 0.202* 0.198† 0.206†
Family support −0.659† −0.662†
Age at diagnosis× family support 0.090
R2 0.041 0.475 0.483
F 5.286* 55.578† 37.962†
F change 5.286* 101.584† 1.909
We found that age at diagnosis had an indirect effect on family function through the mediator family hardiness. The size of the indirect effect was the product of the age at diagnosis and family hardiness, and family hardiness and family function effects, that is −0.209 × −0.733 (0.153). The direct effect was 0.049 and the total effect of age at diagnosis on family function was the sum of the indirect effect and the direct effect, which was 0.202 (Figure 3A). The strength of the mediation effect was estimated using the ratio of the indirect effect to the total effect, which equaled 75.5% for the proportion of mediated effect. The true indi-rect effect was estimated by the Sobel Test [z value = a× b/SQRT(b2× s
a2+a2×sb2), z=2.278, p =0.022]. This
CI0.95 {0.023, 0.283} did not contain 0, so the null
hypothesis of no indirect effect of family hardiness was rejected at α = 0.05 [19].
Moderation of parental health, family
support and family function by age at
diagnosis
Moderator analyses were performed to examine the interaction effects between family resources and age at diagnosis on family function, after controlling the path from age at diagnosis to family hardiness, parental health or family support (Table 2) [18]. Solving the model to determine a moderating relationship formed a new variable, which was the product of the two predictors. For example, predicting family function (Y) from age at diagnosis (X) and family hardiness (M), created a variable (XM)= X × M, then Y = b1X + b2M+ b3X × M + b0. If the XM term was significant, there was a moderating relationship. Age at diagnosis was revealed as a mediator function. We tested the moderator effect from the interaction of age at diag-nosis and family hardiness to family function (R2=
0.549, F(3, 122)= 51.670, p = 0.00), assessing their
signifi-cance. After excluding age at diagnosis in the third step, the explained variance in family function signif-icantly decreased with age at diagnosis (β = 0.066, p= 0.242, SE = 0.006). The causal model did not engage moderation because the path from the interaction of age at diagnosis and family hardiness to family function was not significant (F change =1.382, p=0.242) (Table 2). Age at diagnosis revealed that the non-mediator function and non-moderator function of parental health was substantiated first by increasing the path coefficient from 0.202 to 0.210. The second change was also significant in the path from age at diagnosis
and parental health to family function. In the second step, age at diagnosis and parental health were also entered into the equation and contributed to explaining the variance in the measurement of family functioning (R2= 0.402, F
(2, 123)= 41.368, p = 0.00) (Table 2). Age at
diagnosis showed a small but significant addition in the equation (β = 0.21, p = 0.003), and the path from age at diagnosis to parental health was not significant (β = 0.014, p = 0.879) (Figure 3B). After statistically con-trolling the path from age at diagnosis to parental health and the path from parental health to family func-tion, the previous relationship between age at diag-nosis and family function became more significant (β = 0.21, p = 0.003) (Figure 3B). In the third step, the interaction between age at diagnosis and parental health was entered to assess its interaction significance (R2= 0.416, F
(3, 122)= 28.996, p = 0.00, F change = 2.945, p= 0.089) (Table 2). With exclusion of age at diagnosis in this third step, the explained variance in family function for age at diagnosis did not significantly decrease (β = −0.275, p = 0.347) (Table 2). When the re-gression coefficient for the interaction term of the age at diagnosis and parental health was entered into the third step of the hierarchical regression, there was no significant contribution to explaining the variance of family functioning (R2change = 0.014). The path from
the interaction of parental health and age at diagnosis to family functioning was non-significant (Table 2).
Age at diagnosis revealed that the non-mediator function and non-moderator function of family sup-port was substantiated first by decreasing the path coefficient from 0.202 to 0.198. The second change was also significant in the path from age at diagnosis and family support to family function. Age at diag-nosis and family support were also entered into the equation and contributed to explaining the variance in the measurement of family function (R2= 0.475,
F(2, 123)= 55.578, p = 0.00) (Table 2). Figure 3C shows that age at diagnosis was significantly suppressed in the equation (β = 0.198, p = 0.003), but the path from age at diagnosis to family support was not significant (β = −0.007, p = 0.941). After statistically controlling the path from age at diagnosis to family support and the path from family support to family function, the previous association between age at diagnosis and family function became more significant (β = 0.198, p= 0.003). In the third step, the interaction between age at diagnosis and family support was entered to assess their significance (R2= 0.483, F
p= 0.00, F change = 1.909, p = 0.023) (Table 2). With the addition of age at diagnosis in the third step, the explained variance in family function significantly increased for age at diagnosis (β = 0.206, p = 0.002) (Table 2). When the regression coefficient for the interaction term of age at diagnosis and family sup-port was entered into the third step of hierarchical regression, there was no significant contribution in explaining the variance of family functioning (R2
change=0.008). The path from the interaction of family support and age at diagnosis to family function was not significant (Table 2).
D
ISCUSSIONData from this study provide support for part of the concept model of family stressors, family resources, and family function. Parents who reported earlier detection of the disease, and who gained earlier family access to care, were more encouraging, tolerant and hardy in coping with the disease and consequent search for family support, which might maintain parental health associated with family functioning. Consistent with the model of stressors, resources, and functioning, the results showed that age at diag-nosis did not have a direct association with parental health and family support. However, age at diagnosis of DMD had significant effects on family function and family hardiness, supporting decision-making at the time of prenatal or neonatal screening of the disease. Family hardiness was a complete mediator on family function through age at diagnosis because the direct path between age at diagnosis and family function was not significant and the path was zero when family hardiness was included in the model [4,5]. In testing the interaction effect of age at diagnosis and family hardiness, an increase in moderator effect was not detected [5]. The associations between greater family hardiness with positive family adaptation or psychological outcome are consistent with findings from previous studies [4,20]. We can assume that the caregivers learned the skills earlier for taking care of the affected child carefully so that the child could maintain his/her function and quality of life. The reason why greater family hardiness was associated with higher family functioning and to earlier diagnosis may have been because caregivers with greater family hardiness received more support.
The finding that the children’s level of disability was not associated with family function or with any of the other predictor variables was surprising. The main supposition to explain this is that the parents participated in support groups that helped them adapt to the progressive course of the disease. These findings raise several important issues for future research. With respect to family resources, parents in this study reported poorer health status and more anxiety, depression, pain, and disability than members of the general population [21], a finding consistent with previous research on families of children with serious or disabling conditions. Tamplin and Goodyer [22] reported that mental health was highly correlated with all FAD scales for mothers of high-risk children, with only one or two scales for low- and high-risk fathers, respectively. Studies have revealed evidence that depressed adolescents were significantly more likely to be in families that were reported as dysfunc-tional on the FAD [22,23].
Mean family hardiness scores in this study were also lower than those for parents of children with asthma, cardiac conditions, or diabetes, as described in previous studies [7]. The reasons for these differences between parents of children with DMD and other conditions should be explored in future research. The positive association between hardiness and healthy family functioning indicates that parents of children with DMD who had greater hardiness to endure stress-ors also had greater health. In addition, from a health promotion perspective, the findings support the need to develop family hardiness through family support services that could be incorporated into health pro-motion programs in the long term [24].
This study was limited due to the small convenience sample and self-report measures. In using self-reports, the parents could have over-reported hardiness, sup-port and strength, and under-resup-ported their health condition. Addressing only parents in the TMDA, the present study produced findings that may be specific to one association and not generalizable to others. Furthermore, the cross-sectional design of this study limits the exploration of causal relationships among the predictors/mediators and outcome variables. A lon-gitudinal study with a multilevel modeling technique design would allow further investigation of the mul-tiple factors that influence the causal effects. Finally, this study did not account for economic differences between family hardiness and family function. Thus,
future studies might demonstrate other factors that mediate or moderate the associations between pre-dictor and outcome variables. Owing to the dynamic nature of the phenomena examined in this study, qual-itative interviews and other more in-depth, socially grounded research should be conducted in this area in the future.
A
CKNOWLEDGMENTSThe author would like to thank Drs. Susan Instone, Allen Orsi, and Diane Hatton for their contributions to the completion of this research.
R
EFERENCES1. Chen JY, Jong YJ. A stress model for parents of children with Duchenne muscular dystrophy. Hu Li Za Zhi 2006; 53:44–51. [In Chinese]
2. Chen JY. Functioning Among Taiwanese Families with a Child Having Duchenne Muscular Dystrophy. Doctoral Dissertation, University of San Diego, San Diego, CA, 2004.
3. Chen JY, Clark MJ. Family function in families of children with Duchenne muscular dystrophy. Fam Community Health 2007;30:296–304.
4. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical consideration. J Pers Soc Psychol 1986;51:1173–82.
5. Frazier PA, Tix AP, Barron KE. Testing moderator and mediator effects in counseling psychology research. J Couns Psychol 2004;51:115–34.
6. Holmbeck GN. Toward terminological, conceptual, and a statistical clarity in the study of mediators and moderators: examples from the child-clinical and pedi-atric psychology literatures. J Consult Clin Psychol 1997; 65:599–610.
7. McCubbin HI, Thompson AI, McCubbin MA. Family Measures: Stress, Coping, and Resiliency—Inventories for Research and Practice. Honolulu, Hawaii: Kamehameha Schools, 2001.
8. Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J 1965;14:61–5.
9. Parkerson GRJ, ed. User’s Guide for Duke Health Measures. Durham, NC: Department of Community and Family Medicine, Duke University Medical Center, 2002. 10. Smilkstein G. The Family APGAR: a proposal for a
family function test and its use by physicians. J Fam Pract 1978;6:1231–9.
11. Gardner W, Nutting PA, Kelleher KJ, et al. Does the family APGAR effectively measure family functioning? J Fam Pract 2001;50:19–25.
12. Miller IW, Keitner GI, Whisman MA, et al. Depressed patients with dysfunctional families: description and course of illness. J Abnorm Psychol 1992;101:637–46. 13. Cohen J. Statistical Power Analysis for the Behavioral
Sciences, 2ndedition. Hillsdale, New Jersey: Lawrence
Erlbaum Associates, 1988.
14. Arpin K, Fitch M, Browne GB, et al. Prevalence and correlates of family dysfunction and poor adjustment to chronic illness in specially clinics. J Clin Epidemiol 1990;43:373–83.
15. MacKinnon DP, Lockwood CM, Hoffman JM, et al. A comparison of methods to test mediation and other in-tervening variable effects. Psychol Methods 2002;7:83–104. 16. MacKinnon DP, Dwyer JH. Estimating mediated effects
in prevention studies. Eval Rev 1993;17:144–58. 17. MacKinnon DP, Warsi G, Dwyer JH. A simulation
study of mediated effect measures. Multivariate Behav Res 1995;30:41–62.
18. Lindley P, Walker SN. Theoretical and methodological differentiation of moderation and mediation. In: Downs FS. Readings in Research Methodology. Philadelphia: Lippincott, 1999:198–203.
19. Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput 2004;36:717–31. 20. Clark PC. Effects of individual and family hardiness
on caregiver depression and fatigue. Res Nur Heal 2002;25:37–48.
21. Patterson JM. Integrating family resilience and family stress theory. J Marriage Fam 2002;64:349–60.
22. Tamplin A, Goodyer IM. Family functioning in adoles-cents at high and low risk for major depressive disorder. Eur Child Adolesc Psychiatry 2001;10:170–9.
23. Miller IW, Kabacoff RI, Epstein NB, et al. The develop-ment of a clinical rating scale for the McMaster model of family functioning. Fam Proc 1994;33:53–69.
24. Chen JY, Instone SL. Family Resilience and Functioning in Child with DMD: Functioning and Resilience in Families with Children with Duchenne Muscular Dystrophy. Saarbrucken: VDM Verlag Dr. Muller, 2008.
收文日期:97 年 8 月 25 日 接受刊載:97 年 11 月 18 日 通訊作者:陳季員醫師 高雄醫學大學護理學系 高雄市三民區十全一路 100 號