行政院國家科學委員會專題研究計畫 成果報告
睡眠呼吸障礙與代謝症候群及發炎生化指標的相關性 研究成果報告(精簡版)
計 畫 類 別 : 個別型
計 畫 編 號 : NSC 97-2314-B-040-004-
執 行 期 間 : 97 年 08 月 01 日至 98 年 07 月 31 日 執 行 單 位 : 中山醫學大學醫學系復健科學科
計 畫 主 持 人 : 丁化 共 同 主 持 人 : 楊繼江
計畫參與人員: 碩士班研究生-兼任助理人員:許智超 碩士班研究生-兼任助理人員:陳凱玲
處 理 方 式 : 本計畫可公開查詢
中 華 民 國 98 年 10 月 30 日
行政院國家科學委員會補助專題研究計畫 行政院國家科學委員會補助專題研究計畫 行政院國家科學委員會補助專題研究計畫 行政院國家科學委員會補助專題研究計畫
Beyond Sleep Disordered Breathing, Gender Does Matter Plasma Triglyceride, Uric Acid Levels and Blood Pressure 計畫類別:ˇ 個別型計畫 □ 整合型計畫
計畫編號:NSC 97-2314-B-040-004-
執行期間:97 年 08 月 01 日 至 98 年 07 月 31 日
計畫主持人:丁化 共同主持人:楊繼江
計畫參與人員:陳凱玲、許智超
成果報告類型(依經費核定清單規定繳交):ˇ精簡報告 □完整 報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究 計畫、列管計畫及下列情形者外,得立即公開查詢 □涉及專利或其他智慧財產權,□一年□二年後可公 開查詢
執行單位:中山醫學大學
中 華 民 國 98 年 10 月 30 日
ˇ ˇ ˇ
ˇ 成 果 報 告 成 果 報 告 成 果 報 告 成 果 報 告
□期中進度報告
□期中進度報告
□期中進度報告
□期中進度報告
Beyond Sleep Disordered Breathing, Gender Does Matter Plasma Triglyceride, Uric Acid Levels and Blood Pressure
Hua Ting1, Hsiao-Sui Lo2, Shin-Da Lee3
1Center of Sleep Medicine, Chung-Shan Medical University Hospital, Taichung, Taiwan; 2Department of Neurology, Chung-Shan Medical University Hospital,
Taichung, Taiwan; 3Department of Physical Therapy China Medical University Hospital, Taichung, Taiwan
Abstract
Study Objectives: Sleep-disordered-breathing, more male-prevalent, is associated with systemic inflammation, hypertension and metabolic aberration. Through sexual hormones’ protections, female have metabolic and cardiovascular preferences, speculatively attributed to better upper-airway conductivity and central-breathing control during sleep. The aim of this study is to investigate if above female superiorities exist when adjusted for sleep-disordered-breathing severity.
Design: Retrospective data review analysis.
Participants: 84 randomly-selected eligible sleep-disturbance female patients were enrolled to be matched with a male individually for apnea-hypopnea index (AHImt) or not (nAHImt), besides for age (< and ≥ 50 years [the average menopausal age, Taiwan]; Junior and Senior) and body mass index. Measurements and Results: In Junior/nAHImt (51 pairs), female (35.7±8.3 vs. 35.5±8.1 years, female vs. male; in same sequences as follows) had shorter neck circumference, better sleep architecture, lower AHI (16.2±17.5 vs. 30.3±24.3 events/hr), Epworth Sleepiness Scale score (ESS), blood pressure (BP), serial levels of total cholesterol (TC), triglyceride (TG) (97±51 vs. 147±142 mg/dL) and uric acid (UA) (5.1±1.4 vs. 6.3±1.5 mg/dL). In Junior/AHImt (33 pairs), female (38.6±7.9 vs. 38.9±8.5 years) appeared shorter neck circumference, lower waist/hip ratio (0.85±0.07 vs. 0.91±0.06), ESS, BP, TG(96±43 vs.142±115 mg/dL) and UA (4.7±1.4 vs. 6.4±1.62 mg/dL). While in Senior/nAHImt (51 pairs), female (56.3±5.1 vs. 56.5±5.7 years) had lower AHI, neck circumference, and waist/hip ratio, with lower diastolic BP and UA (5.4±2.0 vs. 6.4±1.7 mg/dL). In Senior/AHImt (33 pairs), female (56.9±5.1 vs. 57.5±5.8 years) had similar waist/hip ratio, sleep architecture, BP, the lipid profile values, C-reaction protein, and UA. UA positively correlated with TG in Junior/male and Senior/female. In two
triple-matched groups, positive correlations were found in UA-systolic BP and UA-TG of both Junior/male and Senior/female; and waist/hip ratio-UA of Junior and Senior/female.
Conclusions: Beyond sleep-disordered-breathing’s attenuating effect, female’s gender preferences on TG, UA and BP persist till menopause age, potentially through central fat evolution.
Key Words: Sleep apnea, gender differences, metabolic syndrome, C-reaction protein
The compelling evidences to date indicated that sleep disordered breathing (SDB) is the independent factor to evoke the systemic inflammation, linking to elevations of various cytokine (e.g. tumor necrosis factor-α) (1) and C-reactive protein(2). An elevation of blood pressure (3) in SDB are multifactorial carry-over effects from the nocturnal events, like an enhanced daytime sympathetic activity, and chemoreception resetting, tonic ‘normoxic’ chemoreception activation, baroreflex and endothelial dysfunction. Further, the SDB patients (4) had significantly higher percentage of hyperglycermia, and dyslipidemia besides of hypertension, and SDB’s severity, defined by apnea-hypopnea index (AHI) value, reflects metabolic syndrome parameters’ number. Taken together, SDB patients are also at increased risk for cardiovascular disease (5) substantially through neurohumeral and hemodynamic mechanisms leading to functional and structural damages within the cardiovascular system. The prevalence of SDB is 25-27% or 10-16% in middle-aged Asian men or women, respectively. No matter differences in races(6,7,8,9), male always more prevalent in SDB that the female. Previous study just indicated that (10)
premenopausal hormonal status protected women from reductions in ventilation and upper airway narrowing and closure during sleep. One the other hand, administration of testosterone to premenopausal women (11) elevates the hypocapnic apnea
threshold and fascilitates the development of central apnea during Non-REM sleep.
Therefore, menopause is a significant risk factor for sleep apnea (12)in women and that hormone replacement appears to be associated with reduced risk.
Menopause-increased cardiovascular disease(particularly coronary heart disease) (13) would be reduced by approximately 30-50 % if estrogen used. The similar situation happened in blood pressure (14) with HRT in majority of postmenopausal women.
Given that SDB is a risk factor for hypertension and cardiovascular diseases, one could speculate that the reduction of cardiovascular morbidity/mortality in post menopausal women with HRT might be related, at least in part, to the reduction of SDB in this population. The possible mechanisms In contrast to 8:1 (6) or greater ratio of male to female sleep apnea cases seen in clinical population, only a 2-3: 1 ratio was seen in community samples (7). The different clinical presentation
especially in women might play the role in this difference. However, (GOM, I-3d) the relative risk for SDB between the sexes is still not clear, nor is it clear whether the consequences of this syndrome are the same in the two sexes. We hypothesized that when SDB severity is similar in SDB men and women, the sleep characters,
pro-inflammatory state and metabolic situation are not necessarily the same, perhaps explaining the sex hormones’ effects cross chronological menopausal age.
Thus, we retrospectively compared their sleep characters, variables of
po-inflammatory state and metabolic situation from the gender pairs with SDB, who were individually matched for AHI or not, besides for age, body mass index (BMI).
Therefore, at cutting age set on chronological average age in menopause, the above parameters we compared in two subgroups might realize age-related gender discrepancy.
METHODS
Subjects
With a chief complaint of sleep disturbance, two hundred and sixty-three patients with a wide spectrum of sleep disorders were recruited in the previous study (16), based on 460 patients continuously attended in the Sleep Clinic, Chung-Shan Medical
University Hospital from September 5, 2003 to April 1, 2004. After being approved by Institutional Review Board (IRB), the study was completely described to all subjects and all subjects signed written informed consent before participation.
All the subjects had received venous blood sampling for various biochemical study to surveying the likelihood of metabolic syndrome and systemic inflammatory situation, in the next morning post an overnight sleep polysmnographic study.
Inclusion criteria were patients diagnosed with sleep-disordered breathing (SDB) which refers to a wide spectrum of sleep-related breathing abnormalities including snoring, sleep apnea-hypopnea syndrome and upper airway resistance syndrome.
Upper airway resistance syndrome is a sleep-disordered breathing syndrome characterized by complaints of daytime fatigue and/or sleepiness, increased upper airway resistance during sleep, frequent transient arousals, and no significant hypoxemia.
Patients were excluded if they were current smoker or had regular exercise program or were taking benzodiazepines, narcotic educations, or alcohol at the time of the study. Further, all diagnosed diseases before the current study were excluded such as cardiovascular diseases, cerebrovascular diseases, neurological diseases,
neuromuscular diseases, pulmonary diseases, liver diseases, renal diseases, cardiomegaly and metabolic diseases. Thereafter, the patients on systemic steroid treatment, on medication for hypoglycemia, anti-hyperlipidemia and/or
antihypertension medication or major GYN surgery or on hormone replacement therapy in female were also excluded. To minimize the possible confounding bias, the subjects, having a regular exercise habit or experiencing smoking were not enrolled.
In addition, SDB patients whose duration of total sleep time was less than two hours in sleep laboratory were also excluded.
Questionnaire and Anthropometric Measurement
All patients were requested to arrive at our sleep laboratory between 8:00 and 9:00 pm and to complete a Epworth Sleep Scale (ESS) (17) scoring and life style questionnaire including smoking and exercise habits. The assessments of anthropometric parameters were performed in all patients with loose-fitting clothing. Body weight and height were measured by an electronically calibrated scale and a calibrated stadiometer, respectively. Neck, waist and hip circumferences were measured in standing position at the end of gentle expiration by calibrated plastic tapes. Waist circumference was measured midway between the lower costal margin and iliac crest, and the hip circumference as the maximal girth at the greater trochanters. BMI was calculated as weight divided by height squared (kg/m2).
Blood Pressure Measurements
Pre-overnight sleep BPs were measured in wakeful status with at least 15 min quiet supine position before sleep, and post-overnight sleep BPs were measured just before getting out of bed using a Phillips V24E modular monitor with noninvasive blood pressure readouts on the right arm in supine position. Mean arterial blood pressure was calculated in the usual manner from the systolic and diastolic blood pressures (i.e., mean blood pressure = 1/3 systolic blood pressure + 2/3 diastolic blood pressure).
Polysomnography and Sleep Scoring
A 12-channel polysomnographic recording system (Rembrandt, Medcare, Amsterdam, Netherlands) was used to assess sleep, respiratory and cardiac variables. The recordings of electroencephalography (C3/A2, C4/A1), electrooculography, and submental electromyography were used to assess sleep state. These signals were used to determine the sleep stage for each 30 s interval of the polysomnographic record, according to conventional criteria (18). Oxyhemoglobin saturation (pulse oximetry), nasal airflow, nasal pressure (nasal cannulae and pressure sensor), rib cage and abdominal motion were measured to assess episodes of sleep-disordered breathing.
Sleep staging and sleep-disordered breathing were subsequently scored using standard techniques. Sleep stages and respiratory events were assessed by trained technicians and reviewed by sleep specialists. All assessed criteria were based on the American Academy of Sleep Medicine Manual. Cessation of airflow for at least 10 s was defined as an episode of apnea. Hypopnea was defined as the nasal pressure signal excursions drop by at least 30% from the sleeping baseline level for 10 s or more that was associated with at least a 4% decrease in arterial oxyhemoglobin saturation.
The AHI was defined as the average number of episodes of apnea and hypopnea per hour. Arousals (19) were defined as a sudden rise in EEG frequency to alpha or theta activity lasting at least 3s but less than 15s preceded by at least 10 s of sleep. Sleep polysomnographic parameters included total sleep time, AHI, arousal index, lowest
oxygen saturation, and duration of O2 saturation less than 90%, as well as the percentage of total sleep time spent in rapid eye movement (REM) sleep (REM, %), non-REM stage 1 and 2 (NREM 1+2, %), and non-REM stage 3+4 (NREM 3+4, %).
Blood Sampling and Biochemical Study
Overnight fasting blood samples in patients were drawn from 7:00 to 9:00 am by a trained phlebotomist via a venipuncture of an antecubital vein. The blood samples were drawn and immediately used for metabolic analysis and enzyme assay. Serum glucose, triglyceride, cholesterol, high density lipoprotein (HDL) cholesterol, and low density lipoprotein (LDL) cholesterol were immediately measured from freshly drawn blood samples. The serum glucose, triglyceride, cholesterol, and HDL were measured by a glucose oxidase autoanalyzer (Analytial Technologies, Farnborough, UK), a triglyceride enzyme autoanalyzer (Bayer Corporation, Tarrytown, NY, USA), a cholesterol oxidase autoanalyzer (Bayer Corporation) and HDL cholesterol (Sigma Diabnostics, St. Louis, MO, USA) on an ADVIA_ 1650 chemistry system (Bayer Corporation, Tarrytown, NY, USA) with reagents and calibrators. Low density lipoprotein (LDL) cholesterol was derived using the Friedwald equation. Serum CRP was assayed with a high-sensitivity assay of Immulite high sensitivity CRP (Immulite 2000 Analyzer). The hsCRP, as a skewed variable, was log transformed to achieve a distribution close to normality. Serum uric acid levels were assessed spectrophotometrically using enzymatic methods using Hitachi 747 analyzer (Boehringer Mannheim, Mannheim, Germany).
Matching of Gender Pairs
350 patients with SDB were eligible for gender pairs matching. To show the impact of SDB severity (defined by AHI) on gender differences in various indicators of metabolic syndrome, uric acid (UA) and pro-inflammatory surrogate factor (hs-CRP), we randomly selected gender pairs matched on AHI (AHImt) or not (nAHImt), along with on age and BMI. For matching more precisely, 5 stratified BMI ranges in each 10-year age portions (i.e., 20-29, 30-39, 40-49 and 50-60 years of age) and further 4 severity levels of SDB (i.e., 0-4.9, 5.0-14.9, 15.0-29.9, and ≥ 30 events/hr in AHI for non- [or upper airway resistance syndrome], mild, moderate and severe SDB, respectively) were used (Table 1).
From this our clinical database, random cases of women and matched men were selected to ensure that at least 30 cases could be analyzed for each clinical feature.
This was done to ensure sufficient statistical power. Because menopausal is a continuous process for women in their female sexual hormone decay (20) at age around 50 years old (49.7 ± 4.3 years) in Taiwan (21). To investigate the effects cross-menopausal age on this gender issue, we separate two age groups (Junior and Senior) at the cutting age of 50 years.
Analysis and Statistics
Data are expressed as mean ± standard deviation. Statistical analysis was performed
with paired student t tests for each variable. The Person’s correlation was used to examine between each parameter of the same group. A value of p < 0.05 was considered statistically significant.
A log transformation was used if variables were not normally distributed.
Table 1 The gender pairs' distributions in Junior and Senior groups, matched for stratified age and BMI alone (nAHImt) or for Apnea Hypopnea Index further (AHImt)
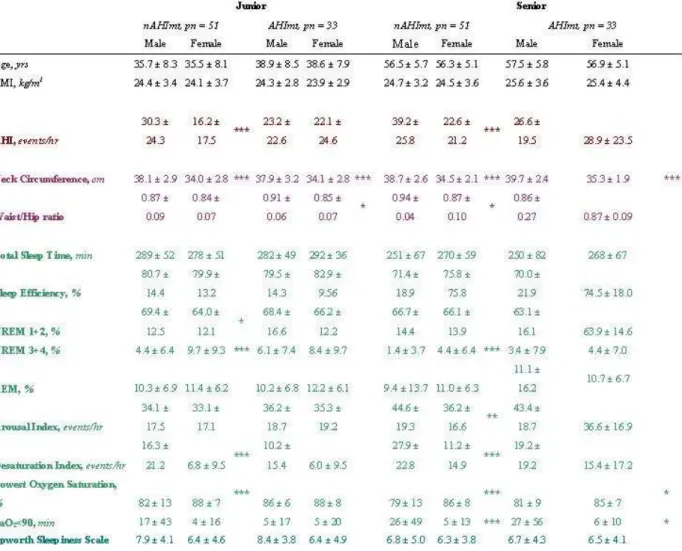
Table 2 The differences of anthropometric characteristics, sleep polysomnography's parameters and ESS questionnaire score in counterparts of Junior and Senior gender-pairs, matched for stratified age and BMI alone (nAHImt) and for Apnea Hypopnea Index further (AHImt)
Table 3 The differences of blood pressures and biochemical characteristics in counterparts of Junior and Senior gender-pairs, matched for stratified age and BMI alone (nAHImt) and for Apnea Hypopnea Index further (AHImt)
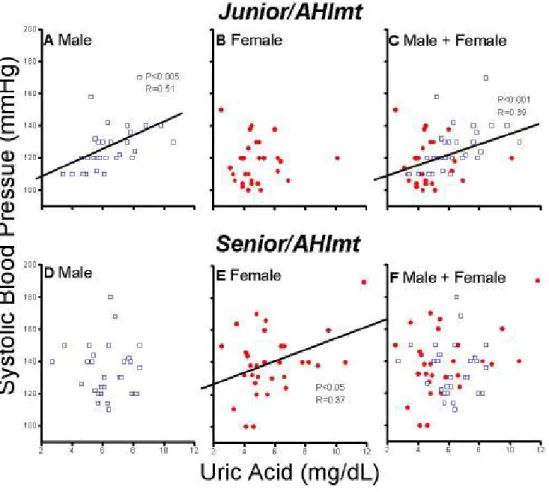
Fig. 1 Pearson’s correlation between plasma uric acid level and systolic blood pressure in male (A,D), female (B,E) and both together (C,F) in Junior/ (A,B,C) and Senior/AHImt (D,E,F) groups.
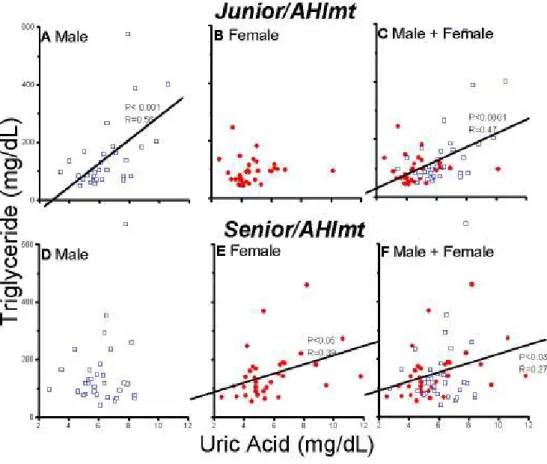
Fig. 2 Pearson’s correlation between plasma uric acid level and plasma triglyceride level in male (A,D), female (B,E) and both together (C,F) in Junior/
(A,B,C) and Senior/AHImt (D,E,F) groups.
Fig. 3 Pearson’s correlation between waist/hip ratio and plasma uric acid level in male (A,D), female (B,E) and both together (C,F) in Junior/ (A,B,C) and Senior/AHImt (D,E,F) groups.
RESULTS
As the result of gender pairing, the pair numbers in Junior/nAHImt, Junior/AHImt, Senior/nAHImt, and Senior/AHImt were 51, 33, 51, and 33 (Table 1), respectively.
In Junior/nAHImt group (Table 2), the female had lower AHI value (16.2 ± 17.5 vs. 30.3 ± 24.3 events/hr in female vs. male, p < .005; in same sequences as follows), shorter neck circumference (34.0 ± 2.8 vs. 38.1 ± 2.9 cm, p < .005), but similar waist/hip ratio (0.84 ± 0.07 vs. 0.87 ± 0.09, p > .05) in comparison with age (35.5 ± 8.1 vs. 35.7 ± 8.3 yrs) and BMI (24.1 ± 3.7 vs. 24.4 ± 3.4 kg/m2) matched male. In polysomnographic study, female had significantly a shorter stage 1+2 (64.0 ± 12.1 vs.
69.4 ± 12.5 %, p <.05), a longer stage 3+4 (9.7 ± 9.3 vs. 4.4 ± 6.4%, p <.005) in non-REM sleep and less Desaturation Index (6.8 ± 9.5 vs. 16.3 ± 21.2 events/hr, p<.005), a higher value of Lowest Oxygen Saturation (88 ± 7 vs. 82 ± 13 %, p < .005), and a lower ESS score (6.4 ± 4.6 vs. 7.9 ± 4.1, p < .05) compared with male, albeit no differences were found in values of Total Sleep Time, Sleep Efficiency, REM%, Arousal Index, and SaO2 < 90% period. Further, the female in this subgroup (Table 3) had significantly lower systolic blood pressure (116 ± 14 vs. 125 ± 16 mmHg, p < .05) and lower mean blood pressure (90 ± 18 vs. 99 ± 14 mmHg, p < .05) and lower serum levels of total cholesterol (174 ± 38 vs. 190 ± 37 mg/dL, p < .05), triglyceride (97 ± 51 vs. 147 ± 142 mg/dL, p < .05) and uric acid (5.09 ± 1.39 vs. 6.30
± 1.46 mg/dL, p < .005), compared with the male. In these gender counterparts, they had similar values of diastolic blood pressure, serum levels of fasting glucose, HDL, LDL and hs-CRP and its log transformed value.
In Junior/AHImt group (Table 2) based on age (38.6 ± 7.9 vs. 38.9 ± 8.5 yrs), BMI (23.9 ± 2.9 vs. 24.3 ± 2.8 kg/m2) and AHI (22.1 ± 24.6 vs. 23.2 ± 22.6 events/hr) matching, the female still significantly had lower values of neck circumference (34.1
± 2.8 vs, 37.9 ± 3.2 cm, p < .005) and waist/hip ratio (0.85 ± 0.07 vs. 0.91 ± 0.06, p
< .05) and lower ESS score (6.4 ± 4.9 vs. 8.4 ± 3.8 p< .05) than the male, while no differences in polysomnographic variables were noted. Moreover, the female in this group (Table 3) had significantly lower systolic (117 ± 13 vs. 128 ± 17 mmHg, p
< .01), diastolic (80 ± 13 vs. 89 ± 12 mmHg, p < .005) and mean blood pressures (92
± 12 vs. 102 ± 13 mmHg, p < .01) and lower serum values of triglyceride (95 ± 43 vs.
142 ± 115 mg/dL, p < .05) and uric acid (4.73 ± 1.40 vs. 6.41 ± 1.62 mg/dL, p < .005) than the male. Again, no differences in between are values of fast glucose, total cholesterol, HDL, LDL and hs-CRP and its log transformed value.
When focus shifting to Senior subject (Table 2), without AHI matching
(Senior/nAHImt), the female (56.3 ± 5.1 vs. 56.5 ± 5.7 yrs and 24.5 ± 3.6 vs. 24.7 ± 3.2 kg/m2 in age and BMI, respectively; both p > .05), compared with male, was characterized by a lower values of AHI (22.6 ± 21.2 vs. 39.2 ± 25.8 events/hr, p
< .005), neck circumference (34.5 ± 2.1 vs. 38.7 ± 2.6 cm, p < .005) and waist/hip ratio (0.87 ± 0.10 vs. 0.94 ± 0.04, p < .05) and shorter NREM 3+4 (4.4 ± 6.4 vs. 1.4 ± 3.7%, p <.005), lesser arousal index (36.2 ± 24.6 vs. 44.6 ± 19.3 events/hr, p < .01) and less severe O2 desaturation (11.2 ± 14.9 vs. 27.9 ± 22.8 events/hr, 86 ± 8 vs. 79 ± 13%, and 5 ± 13 vs. 26 ± 49 min in Desaturation Index, Lower Oxygen Saturation and SaO2< 90%, respectively; all p < .005), though had similar Total Sleep Time, Sleep Efficiency, NREM 1+2, REM and Epworth Sleepiness Scales scores. In variables of blood pressure (Table 3), metabolic state and pro-inflammatory situation, all above mentioned ones were similar but diastolic blood pressure, again female less than male (86 ± 12 vs. 90 ± 12 mmHg, p < .05).
Further with AHI matching in Senior/AHImt group (56.9 ± 5.1 vs. 57.5 ± 5.8 yrs, 25.4 ± 4.4 vs. 25.6 ± 3.6 kg/m2, and 28.9 ± 23.5 vs. 26.6 ± 19.5 events/hr in age, BMI and AHI, respectively; all p > .05) (Table 2), the female still had shorter neck
circumference (35.3 ± 1.9 vs. 39.7 ± 2.4 cm, p < .005), lower Lowest Oxygen Saturation (85 ± 7 vs. 81 ± 9%, p < .05) and shorter period in SaO2<90% (6 ± 10 vs.
27 ± 56 min, p< .05) with equal values of rest parameters for objective and subjective sleep quality to the male. Interestingly, all the parameters related to blood
pressure (Table 3), metabolic situation and pro-inflammatory state were all of no differences in between gender-paired counterparts.
Let’s focus on variables like systolic blood pressure, triglyceride uric acid and waist/hip ratio in these two triple-matching groups (i.e., Junior/AHImt and
Senior/AHImt). In Junior group, uric acid levels were positively correlated with systolic blood pressure (Fig. 1A) and triglyceride (Fig. 2A) in Male and with waist/hip ratio (Fig. 3B, C) in Female and Male + Female. Whereas, in Senior groups uric acid was positively correlated with systolic blood pressure (Fig. 1E), triglyceride (Fig. 2E) and waist/hip ratio (Fig. 3E) in Female. In Senior group again, uric acid levels were also positively correlated with triglyceride (Fig. 2F) and waist/hip ratio (Fig. 3F) in Male + Female. Paradoxically, waist/hip ratio (Fig. 3D) was negatively correlated with uric acid in male. Further, in Junior Male + Female, waist/hip was positively correlated with systolic blood pressure (p< .05), whereas, in Senior Male + Female, there was a similar trend existed (p= .054) (both not shown by figure).
Discussion
In current gender difference study, the female preferences of daytime alertness, lower blood pressure, and lower serum values of uric acid and triglyceride are shown significantly at chronological
premenopausal ages but not postmenopausal ones, independent of SDB severity. These results might be accounted for putatively by concentration changes in sex hormones and by their related central fat evolution. Low systemic inflammation, surrogated by elevated serum CRP values, appears not affected by SDB severity and of no gender difference. Additional AHI matching, besides of age and BMI matching, is meaningful in attenuating gender discrepancies in sleep architecture, serum levels of total cholesterol and uric acid in pre- and post-menopausal age groups, respectively but not in blood pressure, serum values of fast glucose, HDL and LDL, daytime sleepiness and pro-inflammatory state.
SDB is an important disorder because of both its prevalence and its diffused cardiovascular and neurocognitive sequale (22,23). Overwhelming evidences indicated that SDB would induce systemic inflammation (2), elevate cytokine levels (e.g., tumor necrosis factor-α(1) or CRP (2)) and increase insulin resistance (24). Moreover, through acute elevated sympathetic activities and chronic neurohumoral effects, SDB might trigger or aggravate vascular pathogenicity (25). Further, the AHI value, an indicator of SDB severity, was proved as the predictor of number of metabolic syndrome parameters (26); and potentially SDB and metabolic syndrome may share a common path mechanism (26). In gender issue, male have been proved greater prevalent in SDB in either community, laboratory, or ethnicity (6,7,8,9) base, whereas, (12) menopause appeared a risk factor for female’s SDB. This gender discrepancy might be caused by greater wakeful genioglossus activity (10) in female, greater increase in NREM sleep airway resistance in male (27) and other unknown mechanisms. Apparently, sex hormones (28) may play the major role: Administrating testosterone (11) to premenopausal women elevates the hypocapnic apnea threshold and facilitates the development of central apnea during NREM sleep; whereas, estrogen and progesterone supplementation (29) diminishes SDB severity in
healthy/nonobese/postmenopausal women. Thus, at considering gender discrepancy in various cardiovascular risk factors, SDB should be rationally looked as a confounding factor, besides of age and obesity. Moreover, menopause, although not absolutely a turning point, appears actually a dominant physiological watershed in female life (20). To our acknowledgement, few studies have
investigated if gender differences still the same after excluding the impacts of SDB, and if after adding menopause effects further. Possibly, this study might be the first one in investigating gender effects on systemic inflammation, hypertension and metabolic aberration at matching of age, BMI and AHI, besides of life-style confounding such as alcohol, smoking and exercise habits (30).
Interestingly, a recent study of pre- and post-menopausal female compared with age- and either AHI- or BMI-matched male, Yukawa et al. (31) reported that female (pre- and post-menopousal ages together) had lower AHI levels, supposedly contributing to lower ESS sores. Lower ESS score is also found in our Junior/nAHImt/Female group but not Senior one. However, their study could not show if gender difference in ESS scores were chronologic or physiologic menopause independent. Further, the subjects they recruited were older and fatter and had higher ESS scores than ours. Defined by receiving antihypertensive medication or systolic and diastolic blood pressures > 140 and 90 mmHg, respectively, hypertension in their study was associated with BMI, AHI and presence of both hyperlipidemia and diabetes mellitus, but not with gender. Apparently, their findings were not consistent with our results that gender effect on hypertension exists at premenopausal ages,
independent from BMI and AHI. We presume it might too premature to conclude if gender affecting hypertension, when multiple potential bias not excluded such as BMI, AHI, smoking, alcohol, exercise habits, diabetes mellitus and others. From compelling studies, estradiol played the role in
vessel-protection through several mechanisms, such as fatty streak protection, cytokine modulating and nitric oxide bioactivity elevation and prostacycline production increasing (32). Moreover, through diffused and sophisticated, central and peripheral mechanisms, depletion of estrogen with a
concomitant increase in androgens, like postmenopausal situation, would lead to increased peripheral resistance and elevated blood pressure (33). The results of present study further, indicate female sexual hormones have a “direct effect” in lower blood pressure effect, beyond concomitant effects on SDB prevention, till postmenopausal ages.
Each additional apnea or hypopnea event per sleep hour in SDB patients, has been proved to increase fasting insulin level and HOMAIR (34) by about 0.5%. In same cohort study, insulin resistance was confirmed as a significant predictor for hypertension. Their findings suggest that SDB is independently associated with insulin resistance (34), but not fasting glucose level.
Without insulin values, we can not compare our results with theirs. However, their findings were quite consistent with ours that after matching age and BMI, no matter AHI matched further or no, there are no gender differences in serum fast glucose levels in both Junior and Senior groups.
Coughlin et al. (35) had shown that SDB patients had lower HDL, higher total cholesterol/HDL ratio and higher TG than control. Those dyslipidemia would be improved by continuous positive airway pressure (CPAP) application, a gold therapeutic strategy for SDB (36,37). In animal studies,
(38) intermittent hypoxia would induce increases of liver TG and phospholipids by upregulating genes of lipid biosynthesis in lean mice. Moreover, SDB has the potential to induce not only quantitative, but also qualitative (or functional) changes (39) in plasma lipids. On the other hand, premenopausal women have a less atherogenic lipid profile (40) and gender dimorphism in lipid metabolism determined by (41) both sex steroid hormones and body fat distribution. Further, estrogen
administration (42) may decrease hepatic lipase activity and increase HDL even in postmenopausal women. Again, these previous studies did not take gender and gender-related SDB severity together into consideration. In tri-matching groups of our study just showed just TG, but not HDL, LDL or total cholesterol levels is significantly low in female than male in Junior group and these lipid profile are similar in values between female and male in Senior group. It just reflects that TG are more affected than HDL, LDL and total cholesterol by female sex hormone beyond by age, BMI and SDB.
In SDB patients, CPAP therapy (37), independent of total body fat, would reduce significantly intraabdominal fat. This visceral fat, but not total body fat, was confirmed (43) as an important determinant of hepatic lipase activity content. Thus, the presence of SDB is conducive to
accumulation of visceral fat and thereby contributes to the occurrence of components of the metabolic syndrome, through alterations in the secretion of adipokines (44). On the other hand, (45)
premenopausal women with less visceral fat are more insulin sensitive than men, whereas
postmenopausal women have insulin sensitivity similar to men, however, SDB severity not excluded.
Further, (46) waist/hip ratio had been found as a good alternative for non-smoking men and women in predicting metabolic disorders. In our Junior/AHImt groups, male have a wider neck
circumference, a higher waist/hip ratio, higher values of BP, serum TG level and serum UA levels than the sex counterparts. However, at Senior/AHImt groups, there are no gender differences in above variables except neck circumferences. Thus, these findings might indicate beyond SDB, sex (or sex hormone) effects are still meaningful in visceral fat accumulation, in turn, affecting blood pressure, uric acid, (potentially insulin sensitivity) and some lipid profile (explained latter). Although, not regarding to serum UA concentration at all (47), Saito H et al had pointed out that in SDB patients, overnight increase in urinary UA/ creatinine ratio and plasma adenosine level during sleep might reflect the severity of tissue hypoxia. When tissue hypoxia occurs, a net degradation of adenosine triphosphate would lead to the release of purine intermediates (adenosine, inosine, hypopxathine, and xanthine) and the purine catabolic end product, UA. Hyperuricemia clearly demonstrated an increased risk of coronary heart and stroke (48) and was associated with hypertension, menopause, metabolic syndrome (49,50,51,52) and atherothrombosis (53,54) in a metabolic syndrome-independent manner.
Epidemiologically age-related increases in serum UA in women are due to menopause (55), which may get reversed or attenuated by hormone replacement therapy (56). Further, two studies in either Taiwan (57) or Japan (58) showed that elderly women appeared centrally obese and the size of intra-abdominal visceral fat is positively correlated with serum UA and negatively correlated with UA clearance. Moreover,(59) the gender difference in serum UA levels decreased along with aging (60,61,62,63). The findings of these studies were somewhat similar to ours that waist/hip ratio is
positively correlated with UA values in Junior and Senior/AHImt/Female or Female+Male (Fig. 3).
Further, in a non-obese, -hypertensive and -alcoholic male study, Collantes EE (64) had found asymptomatic hyperuricemia, frequently associated with mixed hyperlipidemia or hypertriglyceridemia, from which they speculated purine metabolism flowing triglyceride pathways.
Interestingly, even in our case controlled study the above phenomena still appear in our Junior/AHImt/Male, Junior/AHImt/Male+Female, Senior/AHImt/Female, and
Senior/AHImt/Male+Female (Fig. 2). This gender effect on UA-TG relationship appears substantially dependent on chronological menopausal age. In other words, young male’s
high-androgen/low-estrogen related UA-TG association seems shifting to senior female as the result of postmenopausal hormonal changes, possibly the similar mechanisms on UA-systolic BP too (Fig, 1).
Conversely, the linkages of systolic BP and TG to hyperurecemia are absent in
Junior/AHImt/Female and Senior/AHImt/Male. We supposed that there might be same compensatory mechanisms that counteract or attenuate the associative relationship in between. Paradoxically, in Senior/AHImt/Male, waist/hip ratio is negatively correlated with serum UA levels. This is hard to explain. We hypothesize that in these senior men, through long term central obesity effect on an increase of cardiac output (65) even during sleep, which likely mitigates the tissue hypoxia impact from SDB; i.e., the greater waist/ hip ratio, the lower the serum UA levels. On the other hand, that visceral fat still affects BP and lipid profile, will diminish SBP-UA and TG-UA association in Senior/AHImt/Male. However, to confirm these, further studies are needed.
Shepertycky et al. (66) had reported that women with SDB are more likely to be treated for depression, to have insomnia and to have hypothyroidism than are age, BMI, AHI, and ESS score matched men. In general population, the presence of excessive daytime sleepiness is strongly associated with depression, obesity, diabetes and SDB, age, exercise habit and other covariates.
Recently, Basta et al (30) has shown that in obese subjects (BMI 35-40 kg/m2), predictors of moderate sleepiness (ESS score ≅ 13.5) for both sexes were depression and log AHI. However, gender difference of excessive daytime sleepiness, after controlling age, BMI, AHI and exercise, is still unknown. The results of our study just indicated that in relatively slim subjects on sleep clinic base, the female of premenopausal ages have lower ESS score than the male. This gender difference was not found when they got older than chronological menopausal ages. Further study in this agenda should be needed.
Serum CRP levels, a potential early marker of cardiovascular disease (67,68,69,70), will be elevated by aging, smoking, obesity/visceral obesity, insulin resistance, hypertension (71) or total/
partial sleep deprivation (72). In the clinical SDB subjects, Guilleminault et al (73) had reported that only BMI was significantly associated with high CRP values, no matter men and women considered separately. However, the linkage between SDB severity and CRP values was not consistent in other studies (71,74). Lui et al (71) recently had shown that in their male SDB patients, the CRP level was significantly predicted by each value of AHI, waist circumference, and serum TG level. In our study, after age- and BMI-matching, no gender difference of serum CRP levels is found, no matter AHI
matching or not, in both Junior and Senior groups. This result is likely supporting Guilleminault et al.’s finding; but actually still not against Lui et al.’s, because CRP-AHI association is not examined in either gender or total group in our study. In SDB subjects, it is quite frequently that sleep is
fragmented accompanied with total sleep time reduced and sleep efficiency diminished. Thus, in present study, no gender disparity in both total sleep time and sleep efficiency, in either AHImt or nAHImt of both Junior and Senior groups, possibly plays a role at least in part, in attenuating male’s dominant effects of AHI, blood pressure and waist/hip ratio on CRP values.
AHI matching further in our study, is quite meaningful in attenuating gender discrepancies in sleep architecture, serum levels of total cholesterol and uric acid in pre- and post-menopausal age groups, respectively. This result just demonstrates that gender impact seems stronger than SDB in certain cardiovascular factors such as BP, TG, UA, visceral fat accumulation and daytime sleepiness, although fading away when people get older. On the other hand, BMI matching potentially diminish gender differences in some portion of lipid profile and pro-inflammatory state. In clinical
implication, our study might somehow show up the different impact weighting of gender, BMI, SDB, waist/hip ratio and age on various cardiovascular risk factors.
Limitations
This is a clinical base, rather than a population base study. Due to the gender differences in clinical pictures (66), it might be limited to extend our results exponentially to general population. Besides, craniofascial character is a dominant predictor for SDB in Asian against BMI in Caucasian counterparts. Potentially, our patients are relatively lower in BMI values than are those in Western studies. Therefore, it should be cautious when our results would be generalized to other ethic groups.
Conclusion
In this retrospective, clinical based, gender pairing, case control study, several conclusions might be noteworthy:
1. At chronological premenopausal age, female has actually preferences against age- and
BMI-matched male, in daytime alertness, blood pressure, and serum levels of triglyceride and uric acid, which persists even beyond sex related sleep disordered breathing.
2. The fact that female preferences fade away cross the physiological watershed of menopause might be accounted for, at least in part, by central fat evolution.
3. Additional AHI matching, besides of age and BMI matching, is meaningful in attenuating gender discrepancies in sleep architecture, serum levels of total cholesterol and uric acid in pre- and post-menopausal age groups, respectively.
Acknowledgements
The study was partly supported by National Science Council in Taiwan (NSC97 2314-B-040-004- ) and Chung Shan Medical University Hospital ( CS 07161)
REFENCES
1.Elevated production of tumor necrosis factor-alpha by monocytes in patients with obstructive sleep apnea syndrome. Minoguchi K. Tazaki T. Yokoe T. Minoguchi H.
Watanabe Y. Yamamoto M. Adachi M. Chest. 126(5):1473-9, 2004
2. Elevated levels of C-reactive protein and interleukin-6 in patients with obstructive sleep apnea syndrome are decreased by nasal continuous positive airway pressure.
Yokoe T. Minoguchi K. Matsuo H. Oda N. Minoguchi H. Yoshino G. Hirano T.
Adachi M. Circulation. 107(8):1129-34, 2003
3. Chronic orthostatic intolerance: part of a spectrum of dysfunction in orthostatic cardiovascular homeostasis? Narkiewicz K. Somers VK. Circulation. 98(20):2105-7, 1998
4. ?
5. Bradley G Curr Opn Pulm Med 2002:516-520
6. Sleep apnea, hypopnea and oxygen desaturation in normal subjects. A strong male predominance. Block AJ. Boysen PG. Wynne JW. Hunt LA. New England Journal of Medicine. 300(10):513-7, 1979
7. The occurrence of sleep-disordered breathing among middle-aged adults. Young T.
Palta M. Dempsey J. Skatrud J. Weber S. Badr S. New England Journal of Medicine.
328(17):1230-5, 1993.
8. The gender bias in sleep apnea diagnosis. Are women missed because they have different symptoms?.Young T. Hutton R. Finn L. Badr S. Palta M. Archives of Internal Medicine. 156(21):2445-51, 1996.
9.A community study of sleep-disordered breathing in middle-aged Chinese men in Hong Kong.. Ip MS. Lam B. Lauder IJ. Tsang KW. Chung KF. Mok YW. Lam WK.
Chest. 119(1):62-9, 2001.
10. Influence of gender on waking genioglossal electromyogram and upper airway resistance. Popovic RM. White DP.
American Journal of Respiratory & Critical Care Medicine. 152(2):725-31, 1995.
11.Effect of testosterone on the apneic threshold in women during NREM sleep. Zhou XS. Rowley JA. Demirovic F. Diamond MP. Badr MS. Journal of Applied
Physiology. 94(1):101-7, 2003.
12. Prevalence of sleep-disordered breathing in women: effects of gender. Bixler EO.
Vgontzas AN. Lin HM. Ten Have T. Rein J. Vela-Bueno A. Kales A. American Journal of Respiratory & Critical Care Medicine. 163(3 Pt 1):608-13, 2001.
13. Cardiovascular disease in women: a statement for healthcare professionals from the American Heart Association. Writing Group. Mosca L. Manson JE. Sutherland SE.
Langer RD. Manolio T. Barrett-Connor E. Circulation. 96(7):2468-82, 1997.
14. Laragh JH, Brenner BM, editors. Hypertension, pathophysiology diagnosis, and management. New Tork: Raven Press;1995.
15. Sleep apnea and daytime sleepiness and fatigue: relation to visceral obesity, insulin resistance, and hypercytokinemia. Vgontzas AN. Papanicolaou DA. Bixler EO. Hopper K. Lotsikas A. Lin HM. Kales A. Chrousos GP. Journal of Clinical Endocrinology & Metabolism. 85(3):1151-8, 2000
16. Post- to pre-overnight sleep systolic blood pressures are associated with sleep respiratory disturbance, pro-inflammatory state and metabolic situation in patients with sleep-disordered breathing. Ting H. Lo HS. Chang SY. Chung AH. Kuan PC.
Yuan SC. Huang CN. Lee SD. Sleep Medicine. 10(7):720-5, 2009 17. ESS
18. Rechtschaffen A, Kales A, editors. A manual of standardized terminology techniques and scoring system for sleep stages of human subject. Washington, DC:
Government Printing Office; 1968.
19. arousal 20. Menopausal
21. Effects of menopause and obesity on lipid profiles in middle-aged Taiwanese women: the Chin-Shan Community Cardiovascular Cohort Study. Torng PL. Su TC.
Sung FC. Chien KL. Huang SC. Chow SN. Lee YT. Atherosclerosis. 153(2):413-21, 2000 .
22. Continuous positive airway pressure treatment improves pulmonary
hemodynamics in patients with obstructive sleep apnea. Sajkov D. Wang T. Saunders NA. Bune AJ. Mcevoy RD. American Journal of Respiratory & Critical Care
Medicine. 165(2):152-8, 2002 .
23.Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. Nieto FJ. Young TB. Lind BK.
Shahar E. Samet JM. Redline S. D'Agostino RB. Newman AB. Lebowitz MD.
Pickering TG. JAMA. 283(14):1829-36, 2000 .
24 Effect of high-fat diet and metformin treatment on ventilation and sleep apnea in non-obese rats. Ramadan W. Petitjean M. Loos N. Geloen A. Vardon G. Delanaud S.
Gros F. Dewasmes G. Respiratory Physiology & Neurobiology. 150(1):52-65, 2006 J.
25. Wolk R 2007 Exp Physiol 91:67-78
26. Obstructive sleep apnea syndrome is associated with some components of metabolic syndrome. Kono M. Tatsumi K. Saibara T. Nakamura A. Tanabe N.
Takiguchi Y. Kuriyama T. Chest. 131(5):1387-92, 2007.
27. Gender differences in airway resistance during sleep. Trinder J. Kay A. Kleiman J.
Dunai J. Journal of Applied Physiology. 83(6):1986-97, 1997 Dec.
28 Role of endogenous female hormones in hypoxic chemosensitivity. Tatsumi K.
Pickett CK. Jacoby CR. Weil JV. Moore LG. Journal of Applied Physiology.
83(5):1706-10, 1997 .
29 Progestin and estrogen reduce sleep-disordered breathing in postmenopausal women. Pickett CK. Regensteiner JG. Woodard WD. Hagerman DD. Weil JV. Moore LG. Journal of Applied Physiology. 66(4):1656-61, 1989 .
30. Lack of regular exercise, depression, and degree of apnea are predictors of excessive daytime sleepiness in patients with sleep apnea: sex differences. Basta M.
Lin HM. Pejovic S. Sarrigiannidis A. Bixler E. Vgontzas AN. Journal of Clinical Sleep Medicine. 4(1):19-25, 2008 .
31. Gender differences in the clinical characteristics among Japanese patients with obstructive sleep apnea syndrome. Yukawa K. Inoue Y. Yagyu H. Hasegawa T.
Komada Y. Namba K. Nagai N. Nemoto S. Sano E. Shibusawa M. Nagano N. Suzuki M. Chest. 135(2):337-43, 2009.
32 .Arnal 2007
33. Vascular actions of estrogens: functional implications. Miller VM. Duckles SP.
Pharmacological Reviews. 60(2):210-41, 2008 Jun.
34 Obstructive sleep apnea is independently associated with insulin resistance. Ip MS.
Lam B. Ng MM. Lam WK. Tsang KW. Lam KS. American Journal of Respiratory &
Critical Care Medicine. 165(5):670-6, 2002 .
35.Obstructive sleep apnoea is independently associated with an increased prevalence of metabolic syndrome. Coughlin SR. Mawdsley L. Mugarza JA. Calverley PM.
Wilding JP. European Heart Journal. 25(9):735-41, 2004.
36. Circulating cardiovascular risk factors in obstructive sleep apnoea: data from randomised controlled trials. Robinson GV. Pepperell JC. Segal HC. Davies RJ.
Stradling JR.Thorax. 59(9):777-82, 2004 Sep.
37 Changes in intra-abdominal visceral fat and serum leptin levels in patients with obstructive sleep apnea syndrome following nasal continuous positive airway pressure therapy. Chin K. Shimizu K. Nakamura T. Narai N. Masuzaki H. Ogawa Y. Mishima M. Nakamura T. Nakao K. Ohi M. Circulation. 100(7):706-12, 1999.
38 Chronic intermittent hypoxia upregulates genes of lipid biosynthesis in obese mice.
Li J. Grigoryev DN. Ye SQ. Thorne L. Schwartz AR. Smith PL. O'Donnell CP.
Polotsky VY. Journal of Applied Physiology. 99(5):1643-8, 2005.
39 HDL dysfunction in obstructive sleep apnea. Tan KC. Chow WS. Lam JC. Lam B.
Wong WK. Tam S. Ip MS. Atherosclerosis. 184(2):377-82, 2006 .
40 .Does lipoprotein or hepatic lipase activity explain the protective lipoprotein profile of premenopausal women?. St-Amand J. Despres JP. Lemieux S. Lamarche B.
Moorjani S. Prud'homme D. Bouchard C. Lupien PJ. Metabolism: Clinical &
Experimental. 44(4):491-8, 1995.
41. Regulation of hepatic lipase and serum lipoproteins by sex steroids. Tikkanen MJ.
Nikkila EA. American Heart Journal. 113(2 Pt 2):562-7, 1987.
42 .Effect of estrogen on post-heparin lipolytic activity. Selective decline in hepatic triglyceride lipase. Applebaum DM. Goldberg AP. Pykalisto OJ. Brunzell JD.
Hazzard WR. Journal of Clinical Investigation. 59(4):601-8, 1977.
43 A hepatic lipase gene promoter polymorphism attenuates the increase in hepatic lipase activity with increasing intra-abdominal fat in women. Carr MC. Hokanson JE.
Deeb SS. Purnell JQ. Mitchell ES. Brunzell JD. Arteriosclerosis, Thrombosis &
Vascular Biology. 19(11):2701-7, 1999.
44. Despres JP 2006
1. Abdominal obesity and metabolic syndrome. Despres JP. Lemieux I. Nature.
444(7121):881-7, 2006
45. The metabolically obese, normal-weight individual revisited. Ruderman N.
Chisholm D. Pi-Sunyer X. Schneider S. Diabetes. 47(5):699-713, 1998.
46. Chen Chu-Chih 2009
47. Tissue hypoxia in sleep apnea syndrome assessed by uric acid and adenosine.
Saito H. Nishimura M. Shibuya E. Makita H. Tsujino I. Miyamoto K. Kawakami Y. Chest. 122(5):1686-94, 2002.
48. Hyperuricemia as a risk factor on cardiovascular events in Taiwan: The
Chin-Shan Community Cardiovascular Cohort Study. Chien KL. Hsu HC. Sung FC. Su TC. Chen MF. Lee YT. Atherosclerosis. 183(1):147-55, 2005.
49 Serum uric acid and coronary heart disease. Beard JT 2nd. American Heart Journal.
106(2):397-400, 1983.
50. Cook DG 1986 Serum uric acid, serum glucose and diabetes: relationships in a population study. Cook DG. Shaper AG. Thelle DS. Whitehead TP. Postgraduate Medical Journal. 62(733):1001-6, 1986.
51. Relationship between hyperuricemia and other cardiovascular disease risk factors among adult males in Taiwan. Chu NF. Wang DJ. Liou SH. Shieh SM. European Journal of Epidemiology. 16(1):13-7, 2000.
52. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971-1992. National Health and Nutrition Examination Survey.
Fang J. Alderman MH. JAMA. 283(18):2404-10, 2000.
53. Association between serum uric acid, metabolic syndrome, and carotid atherosclerosis in Japanese individuals. Ishizaka N. Ishizaka Y. Toda E. Nagai R.
Yamakado M. Arteriosclerosis, Thrombosis & Vascular Biology. 25(5):1038-44, 2005.
54 .Atherosclerosis 192 (2007) 131–137, 136a
55. The effect of menopause on serum uric acid levels in non-obese healthy women.
Wingrove CS. Walton C. Stevenson JC. Metabolism: Clinical & Experimental.
47(4):435-8, 1998.
56. Reduction of serum uric acid by hormone replacement therapy in postmenopausal women with hyperuricaemia. Sumino H. Ichikawa S. Kanda T. Nakamura T.
Sakamaki T. Lancet. 354(9179):650, 1999 . 57 .Asia Pac J Clin Nutr 2005;14 (3):285-292
58.Close correlation between visceral fat accumulation and uric acid metabolism in healthy men. Takahashi S. Yamamoto T. Tsutsumi Z. Moriwaki Y. Yamakita J.
Higashino K. Metabolism: Clinical & Experimental. 46(10):1162-5, 1997.
59. Asia Pac J Clin Nutr 2005;14 (3):285-292, 285a.
60. Nutrition and Health Survey in Taiwan 1993-1996; NAHSIT1993-1996 61. Hyperuricemia and gout in Taiwan: results from the Nutritional and Health Survey in Taiwan (1993-96). Chang HY. Pan WH. Yeh WT. Tsai KS. Journal of Rheumatology. 28(7):1640-6, 2001.
62. Serum uric acid levels among thirty-four thousand people in Japan.
Akizuki S. Annals of the Rheumatic Diseases. 41(3):272-4, 1982 .
63.Community-based epidemiological study on diabetes in Pu-Li, Taiwan.
Chou P. Chen HH. Hsiao KJ. Diabetes Care. 15(1):81-9, 1992.
64. Collantes EE 1990 65. obesity
66. Differences between men and women in the clinical presentation of patients diagnosed with obstructive sleep apnea syndrome. Shepertycky MR. Banno K. Kryger MH. Sleep. 28(3):309-14, 2005.
67. Ridker PM 2002
Inflammatory biomarkers, statins, and the risk of stroke: cracking a clinical conundrum.Ridker PM.Circulation. 105(22):2583-5, 2002 .
68. Danesh J 2000 69. Danesh J 2004 70. Pearson TA 2003
71.C-reactive protein is associated with obstructive sleep apnea independent of visceral obesity. Lui MM. Lam JC. Mak HK. Xu A. Ooi C. Lam DC. Mak JC. Khong PL. Ip MS. Chest. 135(4):950-6, 2009.
72. Effect of sleep loss on C-reactive protein, an inflammatory marker of cardiovascular risk.Meier-Ewert HK. Ridker PM. Rifai N. Regan MM. Price NJ.
Dinges DF. Mullington JM. Journal of the American College of Cardiology.
43(4):678-83, 2004.
73. Guilleminault 2004 Sleep
74. C-reactive protein is associated with sleep disordered breathing independent of adiposity . Punjabi NM. Beamer BA. Sleep. 30(1):29-34, 2007.