行政院國家科學委員會專題研究計畫 成果報告
抗精神病藥物導致體重增加及代謝異常之機制及治療 研究成果報告(精簡版)
計 畫 類 別 : 個別型
計 畫 編 號 : NSC 94-2314-B-038-065-
執 行 期 間 : 94 年 08 月 01 日至 96 年 07 月 31 日 執 行 單 位 : 臺北醫學大學精神科
計 畫 主 持 人 : 盧孟良
共 同 主 持 人 : 邱智強、陳俊興
計畫參與人員: 專科畢-專任助理:林憶芬
處 理 方 式 : 本計畫可公開查詢
中 華 民 國 96 年 10 月 23 日
行政院國家科學委員會補助專題研究計畫 成 果 報 告
□期中進度報告
(計畫名稱)
抗精神病藥物導致體重增加及代謝異常之機制及治療
計畫類別: 個別型計畫 □ 整合型計畫 計畫編號:NSC94-2314-B-038-065
執行期間: 94 年 8 月 1 日至 96 年 7 月 31 日
計畫主持人:盧孟良
共同主持人:陳俊興,邱智強 計畫參與人員: 林憶芬
成果報告類型(依經費核定清單規定繳交):精簡報告 □完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢 執行單位: 臺北醫學大學精神科
中 華 民 國 96 年 10 月 23 日
中文摘要
背景: 非典型抗精神病藥物對於精神分裂症之治療具有良好之療效,因此被視為是治療
精神分裂症的第一線藥物。但是近來由於可能會有增加罹患糖尿病或其他新陳代謝異常之 風險而受到注意。本研究將針對 olanzapine 及 risperidone 對於精神分裂症患者之胰島細胞 所出現之急性反應進行研究。
方法: 參與研究之精神分裂症患者將分成兩組,一組接受每天 10 毫克之 olanzapine 藥物
治療,另一組則接受每天 2 毫克之 risperidone 藥物治療,研究期間為 14 天。個案將在第 0 天及第 14 天利用 intravenous glucose tolerance test 方式來檢查胰島素分泌及反應,並檢驗空 腹血糖、胰島素、血脂肪、及 leptin 濃度。
結果: 兩組個案在研究開始時的各項基本資料及實驗室數值均無明顯差異。在兩週的治
療後,兩組在治療前後之體重、BMI、空腹血糖、胰島素、膽固醇、及 leptin 濃度亦無明顯 差異。olanzapine 藥物治療組則在 triglyceride 濃度出現顯著增加。在兩週的治療後,兩組 在治療前後之胰島素敏感性及阻抗性均無顯著差異。olanzapine 藥物治療組則在胰島素分泌 出現顯著減少。
結論: 在接受兩周之 olanzapine 治療後,精神分裂症患者會出現胰島素分泌減少之情形,
顯示 olanzapine 可能會對於胰島細胞功能有直接之影響。
關鍵字:非典型抗精神病藥物,精神分裂症,olanzapine,risperidone,胰島素分泌。
Abstract
Background: Atypical antipsychotics, such as risperidone, olanzapine, and quetiapine, are
effective treatment for schizophrenia and considered as first line therapy. Recently, increasing attention has been drawn to the potential diabetogenic effect of novel antipsychotics. The goal of this prospective study is to evaluate the acute effect of olanzapine and risperidone treatment on pancreatic β-cell function in atypicals-naïve schizophrenic patients.
Methods: Subjects were assigned to therapy with olanzapine (10 mg/day; n=13) or risperidone
(2 mg/day; n=13) for 14 days. The metabolic parameters were quantitatively assessed at baseline and the end of study period by using the intravenous glucose tolerance test. The levels of fasting glucose, fasting insulin, cholesterol, triglyceride, high-density lipoprotein, low-density
lipoprotein, and leptin were also assessed.
Results: There were no significant within-group changes in weight or body mass index for
both groups after 2 weeks treatment. The levels of fasting glucose, fasting insulin, cholesterol, or leptin did not change in both groups. The triglyceride level significantly increased in olanzapine group. Insulin sensitivity index and insulin resistance (insulin/glucose ration and homeostasis model assessment) did not change in both groups. Insulin secretion significantly decreased in olanzapine group.
Conclusions: After 2-weeks of olanzapine treatment, schizophrenic patients decreased insulin
secretory response to a hyperglycemic challenge. The results of this study support the hypothesis that olanzapine directly impair pancreatic β-cell function.
Keywords: atypical antipsychotics, schizophrenia, olanzapine, risperidone, insulin secretion.
報告內容
The atypical antipsychotics, such as olanzapine, risperidone, quetiapine, and ziprasidone, are effective in eliciting both the positive and negative symptoms in schizophrenia (Emsley and Oosthuizen 2003; Kelleher et al 2002; Mortimer 2003). Compared with traditional antipsychotics, atypical antipsychotics cause a lower incidence of extrapyramidal symptoms and minimal
perturbation of prolactin levels. These advantages have led to an increasing use of atypical antipsychotics as the first line therapy for schizophrenia. The atypical antipsychotics act as antagonists at multiple receptors, including members of the dopaminergic, serotonergic, adrenergic, muscarinic, and histaminergic families (Tandon et al 1999). Although the precise mechanism of action remains uncertain, the relatively high affinity for serotonergic receptors and the relatively low dopaminergic D2activity are believed to contribute to the improved efficacy and increased tolerability of atypical antipsychotics (Reynolds 2004).
Compared with the general population, life expectancy in schizophrenic patients is shorter by as much as 20%, attributable to higher rates of suicide, accidental deaths, and natural causes such as cardiovascular disease (Goff et al 2005; Harris and Barraclough 1998; Simpson and Tsuang 1996). Recently, atypical antipsychotics have been linked to several forms of morbidity, including obesity, hyperlipidemia, and type 2 diabetes mellitus (Bergman and Ader 2005; Jin et al 2004;
Melkersson and Dahl 2004; Newcomer 2004; Wirshing 2004). While metabolic abnormalities induced by atypical antipsychotics have been frequently reported, the mechanisms responsible for such an association remain unclear.
Evidence linking atypical antipsychotics to metabolic dysregulation is largely based on case reports and retrospective analyses, which note a disproportionately greater number of patients developing fasting hyperglycemia and new-onset diabetes after the initiation of atypical
antipsychotic treatment (Bergman and Ader 2005; Haupt DW and Newcomer 2001; Henderson et al 2000; Jin et al 2004; Koro et al 2002). Although methodological issues related to nonrandom prescribing patterns and insensitive or non-uniform ascertainment of hyperglycemia or diabetes make these results difficult to interpret, clozapine and olanzapine have been most strongly implicated in pharmacoepidemiological studies. Sowell et al. (Sowell et al 2002) studied insulin secretion using hyperglycemic clamp technique in normal subjects after 15-17 days treatment of olanzapine, risperidone, or placebo. There was a significant change in insulin sensitivity in the olanzapine group and not the risperidone group. The authors ascribed this change to weight gain, based on regression analysis (Sowell et al 2002). In another prospective randomized study in healthy volunteers, the authors found no significant changes in insulin sensitivity or insulin secretion after 3 weeks of treatment with olanzapine or risperidone (Sowell et al 2003). However, their subjects were a normal population instead of patients with schizophrenia. Accordingly, first-episode, drug-naïve patients with schizophrenia have impaired fasting glucose tolerance and are more insulin resistant and have higher levels of plasma glucose, insulin, and cortisol than healthy comparison subjects (Ryan et al 2003). Recently, Henderson et al. (Henderson et al 2005) evaluated the glucose metabolism in antipsychotics-treated schizophrenic patients using a
frequently sampled intravenous glucose tolerance test. They found that both non-obese clozapine- and olanzapine-treated groups displayed significant insulin resistance and impairment of glucose effectiveness compared with risperidone-treated subjects (Henderson et al 2005). Since drug
treatment was not randomized and assessment was cross-sectional, the finding of an association between clozapine and olanzapine and impairment of glucose metabolism cannot be conclusively established as a causal relationship.
While the incidence of new-onset diabetes appears to be increasing in schizophrenic patients treated with certain atypical antipsychotics, it remains unclear whether atypical antipsychotics are directly affecting glucose metabolism or simply increasing known risk factors for diabetes, such as obesity, lipid abnormalities, and decreased physical activity secondary to sedative effects (Henderson 2002). Identification of mechanisms contributing to putative increased risk of diabetes with atypical agents may help to explain apparent inconsistencies in results between pharmacoepidemiological studies and allow identification of patients at risk.
Although treatment with many psychotropic medications may be temporally associated with weight gain, reports of severe hyperglycemia with ketoacidosis in the absence of weight gain or shortly after initiation of treatment have led to speculation that some of the atypical
antipsychotics may have a rapid and direct effect that impairs insulin secretion or insulin action (Baptista et al 2002; Henderson 2002; Mir and Taylor 2001). A number of hypothetical
mechanisms for such an effect have been postulated based on the receptor binding profiles of the medications, including drug-related decreases in insulin secretion or insulin sensitivity (Baptista et al 2002; Jin et al 2004).
The objective of this prospective study was to test whether atypicals-naïve schizophrenic subjects treated with olanzapine or risperidone experienced decreased insulin secretion, as
assessed by intravenous glucose tolerance test (IVGTT). The IVGTT is a well-established method for assessing glucose metabolism and has been widely used in the medical fields of diabetes and obesity research. A prospective randomized design in atypicals-naïve schizophrenic patients was chosen to allow comparison of the differences between risperidone- and olanzapine-treated groups.
Methods and Materials
Study Subjects
Thefacility’sinstitutionalreview board approved thisprospective,randomized,open-label study.
After providing a description of the study to the patients, written informed consent was obtained.
Subjects were male or female between 18-60 years of age, with body mass index (BMI) between 20-27 kg/m2, fasting glucose level of 110 mg/dl or less, and no personal or family history of diabetes. Research psychiatrists evaluated patients after a thorough medical and neurological workup. The Structured Clinical Interview for DSM-IV (American Psychiatric Association1994) was conducted for the diagnosis. All enrolled patients fulfilled the DSM-IV diagnosis of schizophrenia. None were receiving atypical antipsychotics prior to this study. None of the
patients had been pretreated with depot antipsychotics during at least 6 months before study entry.
Patients with Axis I diagnosis other than schizophrenia or medical or neurological illness were excluded. Subjects were excluded for medical conditions that could confound metabolic assessments. Medications (e.g., lithium, carbamazepine, valproic acid, propranolol, tricyclic antidepressants, or other SSRIs) that may influence body weight, glucose/lipid metabolism, or drug disposition were not allowed (Zimmermann et al 2003).
Study Design
Screening studies, physical examination, and laboratory tests were administered, and medical history was collected to determine eligibility for study enrollment. A total of 26 inpatients were included into this study and were randomized into two treatment groups: olanzapine therapy (10 mg/day) and risperidone therapy (2 mg/day). Glucose metabolism was studied using intravenous glucose tolerance tests. Before the baseline IVGTT, subjects were admitted to an inpatient facility for diet stabilization with an isocaloric diet (25-35 kcal/kg). The tests were performed in the morning after an overnight fast both before and 2 weeks after the start of atypical antipsychotics.
Glucose (0.5 g/kg body weight) was administered intravenously. Blood samples for measurement of glucose and insulin were taken from the opposite arm at t = -15, 0, 5, 10, 15, 20, 30, 40, 50, and 60 minutes. The glucose disappearance rate (kG) was calculated by linear regression from the log-transformed glucose values of t = 10 to 30 minutes. A kGvalue below 0.8 mmol/L per minute was considered as abnormal, between 0.8 and 1.2 mmol/L per minute as indeterminate, and above 1.2 mmol/L per minute as normal (Bergman RN 1985; Elmer et al 1994).
Insulin secretion, the secretion response to a glucose load, was calculated as area under the curve using a linear trapezoidal technique from the serum value at each time point after subtraction of the t = 0 value (increment). Insulin resistance was calculated using the
insulin/glucose ratio, homeostasis model assessment (HOMA-R: fasting glucose [mmol/L] * fasting insulin [mU/L] /22.5), and quantitative insulin sensitivity check index (QUICKI:
1/[log(fasting insulin) + log(fasting glucose)]) (Avignon et al 1999; Katz et al 2000; Matthews et al 1985).
Laboratory Assay
Laboratory assays were performed by the chemistry laboratory of Taipei Institute of Pathology.
The serum levels of glucose, triglyceride, cholesterol, low-density lipoprotein (LDL),
high-density lipoprotein (HDL) were measured by using the Olympus AU400 chemistry analyzer.
The plasma glucose level was measured with a hexokinase method. The plasma levels of triglyceride and cholesterol were measured with enzymatic colormetric method. Plasma HDL level was determined by homogeneous liquid selective detergent. Plasma low-density
lipoprotein-cholesterol was calculated from the Friedewald equation (Friedewald et al 1972).
Plasma insulin and leptin were determined using the radioimmunoassay kit and quantified using a Packard Cobra Quantum Gamma Counter.
Statistical Methods
Descriptive statistics are represented as meanSD. The Kolmogorov-Smirnov testing revealed a trend toward normality of distribution for the variables. Subgroups were compared using t-test for continuous variables and chi-square test for categorical variables. A p-value of less than 0.05 was considered to have statistical significance.
Results
Twenty-six subjects signed informed consents and entered the study. Overall, the procedure was well tolerated, and all subjects were able to complete all aspects of the study.
For the entire sample, the meanSD age was 37.3 8.3 years. All subjects were Taiwanese and 18 (69%) were male. The two treatment groups did not differ in age, sex, BMI, weight, or duration of illness or medication treatment.
Baseline Assessment
There were no significant between-treatment group differences in the baseline levels of glucose, insulin, total cholesterol, triglyceride, HDL, LDL, and leptin.
Glucose Metabolism and Lipid
Intravenous glucose tolerance test was performed at baseline and after 14 days of
antipsychotics treatment. In the risperidone group, weight, BMI, fasting glucose, fasting insulin, triglyceride, total cholesterol, HDL, LDL, and leptin did not change significantly at the end point.
Insulin resistance, calculated by the HOMA-R and insulin/glucose ratio, remained similar after 2-week risperidone treatment. Insulin sensitivity index and insulin secretion also remained the same in the risperidone group.
In the olanzapine group, weight, BMI, fasting glucose, fasting insulin, total cholesterol, HDL, LDL, and leptin did not change significantly at the end point. The triglyceride level increased significantly from baseline to end point in olanzapine group. The insulin sensitivity index and insulin resistance remained the same after 2-week olanzapine treatment. In response to a glucose load, the insulin secretion decreased significantly in the olanzapine group.
The weight, BMI, fasting glucose, fasting insulin, triglyceride, total cholesterol, HDL, LDL, and leptin did not differ significantly between groups at the end of study. Although there was no significant difference between groups for insulin sensitivity index or insulin resistance, there was a significant group difference in insulin secretion (p=0.04).
Discussion
In this first prospective study to evaluate glucose metabolism in atypical-naïve schizophrenic patients after 2weeks of atypical antipsychotics administration, we investigated the different effect of olanzapine or risperidone treatment on pancreatic β-cell function. The insulin secretion decreased significantly in patients treated with olanzapine, but not risperidone.
Accumulating clinical evidence indicates that the atypical antipsychotics olanzapine and clozapine have an increased risk of triggering hyperglycemic events in schizophrenic patients (Haupt DW and Newcomer 2001; Lindenmayer et al 2001), which can occur independently of the weight gain associated with these compounds (Koller and Doraiswamy 2002; Ramankutty 2002).
The level of hyperglycemia is often severe and can be attributed to drug treatment, as cessation of use often leads to a full or partial reversal of the hyperglycemia (Koller and Doraiswamy 2002;
Ragucci and Wells 2001). While it is accepted that these atypical antipsychotics harbor an increased risk of disruption glucose regulation, the pharmacological basis for the differences in diabetic liability that exists within the antipsychotics class is not known. Of the commonly used atypical antipsychotics, clozapine and olanzapine appear to have the greatest diabetogenic effect (Bergman and Ader 2005; Jin et al 2004).
The presence of a significant decrease in insulin secretion during olanzapine treatment is in contrast to results reported by previous studies. Previous studies performed with schizophrenic
patients have shown elevated fasting blood glucose concentrations together with
hyperinsulinemia and body weight gain after active olanzapine treatment (Newcomer 2005).
However, the design of these studies is not comparable to ours. Some previous studies applied retrospective or cross-sectional designs that could not establish a causal relationship between olanzapine treatment and metabolic disturbances (Henderson et al 2005; Osser et al 1999). Other studies used healthy volunteers, animals, or culture cells as study subjects that could not reflect the real situation of schizophrenic patients (Ader et al 2005; Melkersson et al 2001; Robinson et al 2005; Sowell et al 2003; Sowell et al 2002). Our study applied the prospective design to evaluate the effect of olanzapine and risperidone on glucose homeostasis in atypicals-naïve schizophrenic patients. The results of this study suggest that olanzapine has an acute and direct effect that impairs insulin secretion.
Mechanisms postulated to account for antipsychotics-induced metabolic disturbances include primary damage to the pancreatic islet cells and/or sympathetic nervous system dysfunction, and a secondary phenomenon related to weight gain and insulin resistance (Goldstein et al 1999).
Some cases of olanzapine-induced pancreatitis have been published since 2000 (Doucette et al 2000; Hagger et al 2000; Waage et al 2004). In this study, the olanzapine-induced decrease in insulin secretion might be related to direct damage of pancreatic cells. The regulation of insulin secretion from pancreatic β-cells is a complex physiological process controlled by a number of interacting signaling components (Chey and Chang 2001). In a placebo-controlled study of olanzapine and risperidone in dogs, olanzapine resulted in marked hepatic insulin resistance and impairment in the compensatory upregulation of β-cell sensitivity to glucose (Ader et al 2005).
Recently, Johnson et al explored how antipsychotics impact both fuel and neurohumorally mediated insulin secretion from isolated perifused rat islets (Johnson et al 2005). Their results suggest that inhibition of cholinergic-stimulated insulin secretion is a possible contributing factor in the disruption of glucose homeostasis by olanzapine. Besides the antimuscarinic properties, it is clear that additional mechanisms contribute to the increased diabetic liability of olanzapine.
Another mechanism that may work in synergy with muscarinic antagonist activity is 5-HT2A
receptor antagonism. It has been demonstrated that specific 5-HT2Aagonists can rapidly stimulate glucose uptake in skeletal muscle by a mechanism which does not depend upon components that participate in the insulin signaling pathway (Hajduch et al 1999).
In our present study, triglyceride levels were higher in the olanzapine group compared with the risperidone group. Elevated triglyceride concentrations have also been observed in
olanzapine-treated patients (Osser et al 1999). In this study, olanzapine-induced increases in triglyceride levels occurred prior to the weight gain and other lipid levels changes. Multiple studies of atypical antipsychotics have not found a strong association between the increases in serum triglyceride levels and weight gain (Meyer 2001) and proposed the possibility of a direct effect on lipid levels by some as yet unknown mechanism (Newcomer 2005).
Two limitations of the current study warrant specific comment. First, schizophrenic subjects without exposure of atypical antipsychotics were enrolled in this study. As the prevalence of diabetes in schizophrenic patients appears to exceed that in the general population (Dixon et al 2000; Goff et al 2005), it could be argued that schizophrenic subjects possess higher
susceptibility to pancreatic β-cell dysfunction during treatment with antipsychotics. The study subjects had previous exposure of typical antipsychotics for 8.54.9 years. The cumulative
effect of type and length of typical antipsychotic treatment might play a role in the development of pancreatic dysfunction (Arranz et al 2004). Another potential limitation is the relatively short duration of drug exposure employed in the study. The main objective of this study was to evaluate the potential acute direct effect of olanzapine or risperidone on insulin secretion. There were several studies reported that changes in glucose metabolism might occur within 1-2 weeks of atypical antipsychotic treatment (Chae and Kang 2001; Sowell et al 2002). Therefore, we believed that 2 weeks would provide adequate exposure, particularly with the use of highly sensitive intravenous glucose tolerance test. The results of the current study cannot address potential effects of olanzapine or risperidone after long-term treatment or with higher doses of these medications.
In summary, atypicals-naïve schizophrenic subjects treated with olanzapine or risperidone for 2 weeks exhibited different changes in insulin secretion. In olanzapine treated subjects, the changes of insulin secretion happen prior to the changes of body weight and insulin sensitivity. Overall, the results of our study support the hypothesis that olanzapine has an acute and direct effect to decrease insulin secretion.
References
Ader M, Kim SP, Catalano KJ, et al (2005): Metabolic dysregulation with atypical antipsychotics occurs in the absence of underlying disease: a placebo-controlled study of olanzapine and risperidone in dogs. Diabetes 54:862-71.
American Psychiatric Association(1994):Diagnostic and Statistical Manual of Mental Disorders,Fourth ed.Washington, DC:American Psychiatric Association.
Arranz B, Rosel P, Ramirez N, et al (2004): Insulin resistance and increased leptin concentrations in noncompliant schizophrenia patients but not in antipsychotic-naive first-episode
schizophrenia patients. J Clin Psychiatry 65:1335-42.
Avignon A, Boegner C, Mariano-Goulart D, Colette C, Monnier L (1999): Assessment of insulin sensitivity from plasma insulin and glucose in the fasting or post oral glucose-load state.
Int J Obes Relat Metab Disord 23:512-7.
Baptista T, Kin NM, Beaulieu S, de Baptista EA (2002): Obesity and related metabolic
abnormalities during antipsychotic drug administration: mechanisms, management and research perspectives. Pharmacopsychiatry 35:205-19.
Bergman RN, Ader M (2005): Atypical antipsychotics and glucose homeostasis. J Clin
Psychiatry 66:504-14.
Bergman RN FD, Ader M, (1985): Assessment of insulin sensitivity in vivo. Endocr Rev 6:45-86.
Chae BJ, Kang BJ (2001): The effect of clozapine on blood glucose metabolism. Hum
Psychopharmacol 16:265-271.
Chey WY, Chang T (2001): Neural hormonal regulation of exocrine pancreatic secretion.
Pancreatology 1:320-35.
Dixon L, Weiden P, Delahanty J, et al (2000): Prevalence and correlates of diabetes in national schizophrenia samples. Schizophr Bull 26:903-12.
Doucette DE, Grenier JP, Robertson PS (2000): Olanzapine-induced acute pancreatitis. Ann
Pharmacother 34:1128-31.
Elmer DS, Hathaway DK, Shokouh-Amiri H, Hughes T, Gaber AO (1994): The relationship of glucose disappearance rate (kG) to acute pancreas allograft rejection. Transplantation 57:1400-5.
Emsley R, Oosthuizen P (2003): The new and evolving pharmacotherapy of schizophrenia.
Psychiatr Clin North Am 26:141-63.
Friedewald WT, Levy RI, Fredrickson DS (1972): Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin
Chem 18:499-502.
Goff DC, Cather C, Evins AE, et al (2005): Medical morbidity and mortality in schizophrenia:
guidelines for psychiatrists. J Clin Psychiatry 66:183-94; quiz 147, 273-4.
Goldstein LE, Sporn J, Brown S, et al (1999): New-onset diabetes mellitus and diabetic ketoacidosis associated with olanzapine treatment. Psychosomatics 40:438-43.
Hagger R, Brown C, Hurley P (2000): Olanzapine and pancreatitis. Br J Psychiatry 177:567.
Hajduch E, Rencurel F, Balendran A, Batty IH, Downes CP, Hundal HS (1999): Serotonin (5-Hydroxytryptamine), a novel regulator of glucose transport in rat skeletal muscle. J
Biol Chem 274:13563-8.
Harris EC, Barraclough B (1998): Excess mortality of mental disorder. Br J Psychiatry 173:11-53.
Haupt DW NJ, D. W., Newcomer JW (2001): Hyperglycemia and antipsychotic medications. J
Clin Psychiatry 62 Suppl 27:15-26; discussion 40-1.
Henderson DC (2002): Atypical antipsychotic-induced diabetes mellitus: how strong is the evidence? CNS Drugs 16:77-89.
Henderson DC, Cagliero E, Copeland PM, et al (2005): Glucose metabolism in patients with schizophrenia treated with atypical antipsychotic agents: a frequently sampled intravenous glucose tolerance test and minimal model analysis. Arch Gen Psychiatry 62:19-28.
Henderson DC, Cagliero E, Gray C, et al (2000): Clozapine, diabetes mellitus, weight gain, and lipid abnormalities: A five-year naturalistic study. Am J Psychiatry 157:975-81.
Jin H, Meyer JM, Jeste DV (2004): Atypical antipsychotics and glucose dysregulation: a systematic review. Schizophr Res 71:195-212.
Johnson DE, Yamazaki H, Ward KM, et al (2005): Inhibitory effects of antipsychotics on carbachol-enhanced insulin secretion from perifused rat islets: role of muscarinic antagonism in antipsychotic-induced diabetes and hyperglycemia. Diabetes 54:1552-8.
Katz A, Nambi SS, Mather K, et al (2000): Quantitative insulin sensitivity check index: a simple, accurate method for assessing insulin sensitivity in humans. J Clin Endocrinol Metab 85:2402-10.
Kelleher JP, Centorrino F, Albert MJ, Baldessarini RJ (2002): Advances in atypical antipsychotics for the treatment of schizophrenia: new formulations and new agents. CNS Drugs
16:249-61.
Koller EA, Doraiswamy PM (2002): Olanzapine-associated diabetes mellitus. Pharmacotherapy 22:841-52.
Koro CE, Fedder DO, L'Italien GJ, et al (2002): An assessment of the independent effects of olanzapine and risperidone exposure on the risk of hyperlipidemia in schizophrenic patients. Arch Gen Psychiatry 59:1021-6.
Lindenmayer JP, Nathan AM, Smith RC (2001): Hyperglycemia associated with the use of atypical antipsychotics. J Clin Psychiatry 62 Suppl 23:30-8.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985):
Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412-9.
Melkersson K, Dahl ML (2004): Adverse metabolic effects associated with atypical antipsychotics: literature review and clinical implications. Drugs 64:701-23.
Melkersson K, Khan A, Hilding A, Hulting AL (2001): Different effects of antipsychotic drugs on insulin release in vitro. Eur Neuropsychopharmacol 11:327-32.
Meyer JM (2001): Effects of atypical antipsychotics on weight and serum lipid levels. J Clin
Psychiatry 62 Suppl 27:27-34; discussion 40-1.
Mir S, Taylor D (2001): Atypical antipsychotics and hyperglycaemia. Int Clin Psychopharmacol 16:63-73.
Mortimer AM (2003): Antipsychotic treatment in schizophrenia: atypical options and NICE guidance. Eur Psychiatry 18:209-19.
Newcomer JW (2004): Abnormalities of glucose metabolism associated with atypical
antipsychotic drugs. J Clin Psychiatry 65 Suppl 18:36-46.
Newcomer JW (2005): Second-generation (atypical) antipsychotics and metabolic effects: a comprehensive literature review. CNS Drugs 19 Suppl 1:1-93.
Osser DN, Najarian DM, Dufresne RL (1999): Olanzapine increases weight and serum triglyceride levels. J Clin Psychiatry 60:767-70.
Ragucci KR, Wells BJ (2001): Olanzapine-induced diabetic ketoacidosis. Ann Pharmacother 35:1556-8.
Ramankutty G (2002): Olanzapine-induced destabilization of diabetes in the absence of weight gain. Acta Psychiatr Scand 105:235-6; discussion 236-7.
Reynolds GP (2004): Receptor mechanisms in the treatment of schizophrenia. J
Psychopharmacol 18:340-5.
Robinson KA, Yacoub Wasef SZ, Buse MG (2005): At therapeutic concentrations, olanzapine does not affect basal or insulin-stimulated glucose transport in 3T3-L1 adipocytes. Prog
Neuropsychopharmacol Biol Psychiatry.
Ryan MC, Collins P, Thakore JH (2003): Impaired fasting glucose tolerance in first-episode, drug-naive patients with schizophrenia. Am J Psychiatry 160:284-9.
Simpson JC, Tsuang MT (1996): Mortality among patients with schizophrenia. Schizophr Bull 22:485-99.
Sowell M, Mukhopadhyay N, Cavazzoni P, et al (2003): Evaluation of insulin sensitivity in healthy volunteers treated with olanzapine, risperidone, or placebo: a prospective, randomized study using the two-step hyperinsulinemic, euglycemic clamp. J Clin
Endocrinol Metab 88:5875-80.
Sowell MO, Mukhopadhyay N, Cavazzoni P, et al (2002): Hyperglycemic clamp assessment of insulin secretory responses in normal subjects treated with olanzapine, risperidone, or placebo. J Clin Endocrinol Metab 87:2918-23.
Tandon R, Milner K, Jibson MD (1999): Antipsychotics from theory to practice: integrating clinical and basic data. J Clin Psychiatry 60 Suppl 8:21-8.
Waage C, Carlsson H, Nielsen EW (2004): Olanzapine-induced pancreatitis: a case report. Jop 5:388-91.
Wirshing DA (2004): Schizophrenia and obesity: impact of antipsychotic medications. J Clin
Psychiatry 65 Suppl 18:13-26.
Zimmermann U, Kraus T, Himmerich H, Schuld A, Pollmacher T (2003): Epidemiology,
implications and mechanisms underlying drug-induced weight gain in psychiatric patients.
J Psychiatr Res 37:193-220.
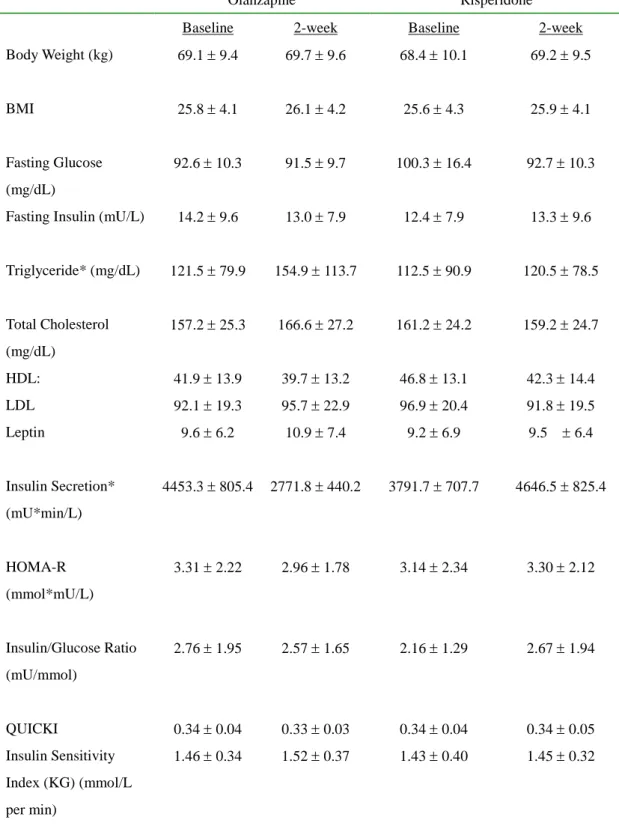
Table 1. Metabolic Profiles of Patients treated with Olanzapine or Risperidone
Olanzapine Risperidone
Baseline 2-week Baseline 2-week
Body Weight (kg) 69.19.4 69.79.6 68.410.1 69.29.5
BMI 25.84.1 26.14.2 25.64.3 25.94.1
Fasting Glucose (mg/dL)
92.610.3 91.59.7 100.316.4 92.710.3
Fasting Insulin (mU/L) 14.29.6 13.07.9 12.47.9 13.39.6
Triglyceride* (mg/dL) 121.579.9 154.9113.7 112.590.9 120.578.5
Total Cholesterol (mg/dL)
157.225.3 166.627.2 161.224.2 159.224.7
HDL: 41.913.9 39.713.2 46.813.1 42.314.4
LDL 92.119.3 95.722.9 96.920.4 91.819.5
Leptin 9.66.2 10.97.4 9.26.9 9.5 6.4
Insulin Secretion*
(mU*min/L)
4453.3805.4 2771.8 440.2 3791.7707.7 4646.5825.4
HOMA-R (mmol*mU/L)
3.312.22 2.961.78 3.142.34 3.302.12
Insulin/Glucose Ratio (mU/mmol)
2.761.95 2.571.65 2.161.29 2.671.94
QUICKI 0.340.04 0.330.03 0.340.04 0.340.05
Insulin Sensitivity Index (KG) (mmol/L per min)
1.460.34 1.520.37 1.430.40 1.450.32
* p < 0.05 within group comparison.
計畫成果自評
1. 本研究由於實驗設計較為煩瑣,參與研究之受試者需要接受密集之抽血檢驗,導致收案 速度較預期緩慢,因此申請延長研究計畫執行期間。
2.
本研究所獲得之初步結果符合原本之預期,同時亦具有相當之學術價值,適合將結果發表於國際學術期刊中。目前已有論文發表 Chiu CC, Chen KP, Liu HC, Lu ML*. The early effect of olanzapine and risperidone on insulin secretion in atypicals-naïve schizophrenic patients. Journal of Clinical Psychopharmacology 2006; 26:504-507 [SCI]
[*correspondence author]
3.
目前針對所獲得之初步成果進行更大樣本及較長追蹤時間之研究,並針對可能之作用機制設計出可行之預防及治療策略,此一研究將可以在研究上及臨床治療上帶來助益。