Correspondence and requests for reprints:Dr. Yung-Ching Liu
Address:Section of Infectious Diseases, Department of Medicine, Shuang-Ho Hospital, Taipei Medical University, No. 291, Road Chung Cheng, Chung Ho City, Taipei County, Taiwan, R.O.C.
Comparison of the AMPLICOR MYCOBACTERIUM Test with Microscopy and Culture for
Diagnosis of Pulmonary Tuberculosis
Chun-Kai Huang
1, Tsi-Shu Huang
2,3, Hsi-Hsun Lin
1,3, Susan Shin-Jung Lee
2,3, and Yung-Ching Liu
4,51
Section of Infectious Diseases, Department of Medicine, E-Da Hospital/I-Shou University, Kaohsiung, Taiwan;
2
Sections of Microbiology and Infectious Diseases, Department of Medicine, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan;
3
National Yang-Ming University, Taipei, Taiwan;
4
College of Medicine, Taipei Medical University, Taipei, Taiwan;
5
Section of Infectious Diseases, Department of Medicine, Shuang-Ho Hospital, Taipei, Taiwan
Abstract
Tuberculosis (TB) is one of the major public health problems in Taiwan. Effective control of TB depends on rapid and correct diagnosis and appropriate treatment. The aim of this study was to evaluate the performance of the Roche AMPLICOR MYCOBACTERIUM (AMPLICOR MTB) test compared with microscopy and culture for diagnosis of pulmonary TB. A total of 123 specimens obtained from 90 suspected pulmonary TB patients were included in this study. All specimens were processed, stained, cultured and assayed using the AMPLICOR MTB test for identification of M. tuberculosis. All patients were followed up for 1 year to confirm or exclude the diagnosis of pulmonary TB. M. tuberculosis was isolated from 29 of these specimens, and final diagnosis of pulmonary TB was identified in 50 patients according to clinical discrepancies. On initial testing, the sensitivity, specificity, positive and negative predictive values of the AMPLICOR MTB test, compared with cultures, were 75.9, 84, 59.5, and 91.9%, respectively. After resolution of discrepancies by the final clinical diagnosis, the sensitivity, specificity, positive and negative predictive values were 72, 98.6, 97.3, and 83.7%, respectively. For smear-positive specimens, the sensitivity was 84.9%, for smear-negative specimens, the sensitivity was 47.1%. Our study demonstrated that the use of the AMPLICOR MTB test was highly sensitive and specific for rapid diagnosis of pulmonary TB. Further studies are needed to determine the cost-effective use of this test with smear-negative specimens. ( J lntern Med Taiwan 2010; 21: 117-124 )
Key Words: AMPLICOR MTB test; Polymerase chain reaction; Mycobacterium tuberculosis
Introduction
Tuberculosis (TB) is currently one of the major public health problems of the world and has been declared a global emergency by the World Health Organization
1. The continuing increase in the number of cases in many countries, the association with HIV/AIDS and the difficulties linked with multidrug-resistant strains give rise to concern. Although the incidence of bacteriologically proven tuberculosis has been steadily declining in Taiwan since 1957, it is still substantially higher than that in the United States
2,3. In 2007, the in- cidence of all TB in Taiwan was 63.2 cases per 100,000 population, whereas in the United States it was 4.4 cases per 100,000 population
3,4. The drawbacks of conventional Mycobacterium tu- berculosis detection techniques are that direct staining for acid-fast bacilli lacks sensitivity and specificity and mycobacterial culture is very time- consuming. The rapid and correct detection of M.
tuberculosis in clinical samples is especially important in Taiwan for clinicians to start timely and efficient treatment.
In the past years, many investigators have described various methods of amplification, especially by polymerase chain reaction (PCR), which enables rapid detection of M. tuberculosis
5-7. However, the reliability of these PCR methods in the clinical setting remain poorly defined
8,9. Commercially available PCR kits with specific procedures and controls may help to reduce interla- boratory variation. Several reports have compared the results of commercialized kits with conventional mycobacteriological methods including cultures and microscopy
10-12. Our previous study has shown that the Roche AMPLICOR MYCOBACTERIUM test (AMPLICOR MTB; Roche Diagnostic Sys- tems, Somerville, N.J.) appears to be more sensitive and specific than the Digene system
13. The diagno- sis of pulmonary TB can be very difficult if we
consider the isolation of organism as the only definitive diagnosis. A substantial percentage of patients cannot be diagnosed based on bacteriology.
In these cases, the diagnosis was made by chest radiograph and therapeutic trial. Therefore, we further conducted a prospective study to evaluate the performance of AMPLICOR MTB test compar- ed with microscopy and culture for diagnosis of pulmonary TB.
Methods
Patients and samples. In a prospective study from May to July 2005, we investigated 123 spe- cimens from 90 consecutive patients who were suspected of having pulmonary TB on the basis of pulmonary infiltrates on their chest X-ray at the Kaohsiung Veterans General Hospital. Of these patients, none were infected with the human immunodeficiency virus type 1. Specimens were limited to expectorated and induced sputa, bro- nchoalveolar lavages, and bronchial washings.
Specimens which could not be processed imme- diately upon receipt were stored at 2 to 6℃ for no longer than 72 hours. All specimens were analyzed for growth of mycobacteria using the BACTEC 460 system (Becton Dickinson Diagnostic Instrument Systems, Towson, Maryland, USA) according to the manufacturer's instructions. Specimens were digested and decontaminated with 2% NaOH in 0.5% N-acetyl-L-cysteine and then concentrated
14. Following digestion, decontamination, and con- centration, all specimens were divided, with one half used for culture and one half stored at -70℃
for the preparation of DNA.
Smear examination. Acid-fast smears of the digested and decontaminated specimens were stained with Rhodamin-Auramine and Ziehl- Neelsen stain and examined by standard proce- dures
14.
Culture and identification. Culture for my-
cobacterium was performed by inoculation of the digested, decontaminated and concentrated materials into one BACTEC 12B bottle and tested with the BACTEC 460 instrument (Becton Dickinson Diagnostic Instrument Systems). The p-nitro-α-acetyl-amino-β-hydroxypropiophenone (NAP) test was performed when the bottle was detected as positive (growth index >50). A dec- reasing or unchanging growth index is presumptive for M. tuberculosis.
AMPLICOR MYCOBACTERIUM system.
The Roche AMPLICOR MTB test was conduct- ed according to the manufacturer's instructions.
Specimens were prepared by addition of 100μl of digested, decontaminated and concentrated spe- cimen to 0.5 ml of wash buffer and followed by centrifugation at 12,000 rpm (11,600 x g) for 10 min. The supernatant was aspirated, and 100 μl of lysis reagent was added to the sediment. After vortexing, the suspension was incubated for 45 min at 60℃ to complete lysis of the mycobacteria. The lysed material was then neutralized by the addition of 100 μl of neutralization reagent.
AMPLICOR MTB amplifies a 584-bp region of the 16S rRNA gene sequence common to all mycobacteria. Carryover contamination was pre- vented by incorporation of dUTP in place of dTTP in the amplification reaction and utilization of uracil-N-glycosylase (AmpErase) to enzymatic- ally cleave any contaminating amplicon carried over from previous reactions. AmpErase was su- bsequently inactivated at the temperatures used for thermal cycling. For amplification, 50 μl of neutralized specimen was added to 50 μl of master mix. The tray containing specimens and controls was then placed in a TC-2400 thermal cycler (Perkin-Elmer, Norwalk, Conn.) and amplified according to the following program: held at 50℃
for 2 min; 2 cycles of 98℃ for 20 s, 62℃ for 20 s, and 72℃ for 45 s; 35 cycles of 94℃ for 20 s, 62℃
for 20 s, and 72℃ for 45 s; held at 72℃ for 5 min;
and held at 72℃ indefinitely.
Detection of M. tuberculosis complex or- ganisms was accomplished by hybridization of the amplified product to a DNA probe specific for organisms of the M. tuberculosis complex. Fo- llowing amplification, 100 μl of denaturation solution were added to all tubes; which was then followed by a 10-min room temperature incubation to allow complete denaturation of the double- stranded products. One hundred microliters of hybridization buffer were added to a microwell plate coated with a DNA probe specific for me- mbers of the M. tuberculosis complex. Twenty- five microliters of denatured amplicon were then added, and hybridization was carried out at 37℃
for 90 min. Detection of hybridized duplex was accomplished with an avidin-horseradish peroxidase conjugate-tetramethylbenzidine substrate system.
The reaction was stopped by addition of dilute hydrosulfuric acid; and the optical density at A
450was measured by the Behring ELISA Processor II (Behringwerke AG Diagnostica, Marburg, Germany). A result was considered positive if the absorbance was greater than or equal to 0.35.
Clinical diagnosis of pulmonary TB. For
the clinical diagnosis of pulmonary TB, patients
were followed up for 1 year. Clinical assessment
included the patient's history, symptoms, chest
X-ray, laboratory results, and follow-up observation
(including response to treatment) as well as the
results obtained from other specimens submitted
to the mycobacteriology laboratory. A case was
defined as pulmonary tuberculosis if any one of
the following criteria was met: (1) culture-positive
for M. tuberculosis, (2) culture-negative but with
compatible chest radiograph findings (i.e. Ghon
complex, cavitary lesion etc.) and response to
antituberculous treatment, (3) typical histological
findings including Langerhans' giant cells, caseous
necrosis and acid-fast bacilli seen on biopsied lung
tissues.
Results
Among 123 clinical specimens from 90 patients, 29 specimens (from 20 patients) were positive by culture, 37 (from 27 patients) were positive by the AMPLICOR MTB test, and 34 (from 22 patients) were positive by microscopy.
Nontuberculous mycobacteria (NTM) were isolated from 3 specimens (from 3 patients). The overall performance of the AMPLICOR MTB test indicated that compared with that of culture, 22 clinical specimens (from 15 patients) were positive and 79 (from 67 patients) were negative by both culture and AMPLICOR MTB test, 15 (from 12 patients) were culture-negative, AMPLICOR MTB-positive, and 7 (from 7 patients) were culture-positive, AMPLICOR MTB-negative (Table 1). Overall, the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the AMPLICOR MTB test were 75.9, 84, 59.5, and 91.9%, respectively. For smear-positive specimens (n=34), the AMPLICOR MTB test had a sensitivity of 91.3% and specificity of 36.4 %. The sensitivity and specificity for smear-negative specimens (n=89) were 16.7 and 90.4%, respectively. It also
showed that 23 specimens (from 15 patients) were positive and 83 (from 68 patients) were negative by both culture and microscopy, 11 (from 7 patients) were culture-negative, smear-positive, and 6 (from 5 patients) were culture-positive, smear-negative.
The sensitivity, specificity, PPV and NPV for the microscopy compared with culture per specimen were 79.3, 88.3, 67.7, and 93.3%, respectively.
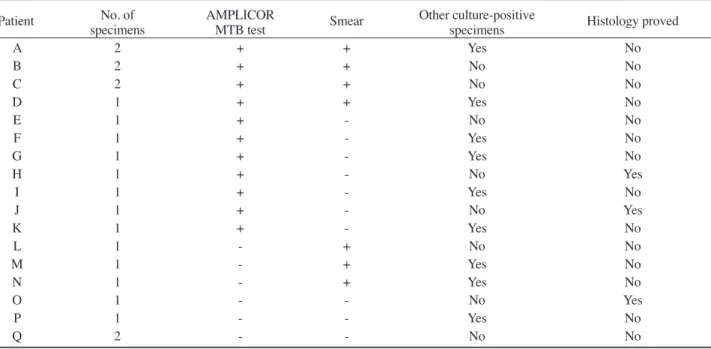
Table 2 compares the AMPLICOR MTB results with final results, based on specimens which grew M. tuberculosis on culture or were obtained from a patient with a clinical diagnosis of pulmonary TB. The diagnosis of pulmonary TB was ascertained according to the definition described in the method section. Fifty pulmonary TB-positive (from 34 patients) and 73 pulmonary TB-negative specimens were defined. Table 3 lists the 21 specimens that were culture-negative for M.
tuberculosis but were obtained from patients with a clinical diagnosis of pulmonary TB. Based on these data, the sensitivity of the AMPLICOR MTB test, microscopy, and culture (using clinical diagnosis as standard) were 72, 66, and 58%, respectively. The specificity of all three tests was higher than 98%.
Table 1. Comparison of AMPLICOR MTB test with culture for detection of M. tuberculosis No. of specimens (%)
Specimen type (No.) Culture positive (n = 29) Culture negative (n = 94)
PCR(+) PCR(-) PCR(+) PCR(-) Sensitivity Specificity
All (n = 123) 22 (18) 7 (6) 15 (12) 79 (64) 75.9% 84%
Smear positive (n = 34) 21 (17) 2 (2) 7 (6) 4 (3) 91.3% 36.4%
Smear negative (n = 89) 1(1) 5 (4) 8 (7) 75 (61) 16.7% 90.4%
Table 2. Comparison of AMPLICOR MTB test with clinical daignosis for detection of tuberculosis*
No. of specimens (%)
Specimen type (No.) Tuberculosis-positive Tuberculosis-negative (n = 50) (n = 73)
PCR(+) PCR(-) PCR(+) PCR(-) Sensitivity Specificity
All (n = 123) 36 (29) 14 (11) 1 (1) 72 (59) 72% 98.6%
Smear positive (n = 34) 28 (23) 5 (4) 0 (0) 1 (1) 84.9% 100%
Smear negative (n = 89) 8(7) 9 (7) 1 (1) 71 (58) 47.1% 98.6%
*The combination of culture results yielding M. tuberculosis and clinical diagnosis of pulmonary tuberculosis was
considered the gold standard.
The sensitivity, specificity, PPV and NPV of the Amplicor MTB test were 72, 98.6, 97.3, and 83.7%
respectively. For smear-positive specimens, the sensitivity and specificity of the AMPLICOR MTB test was 84.9 and 100%, whereas the sensitivity and specificity for smear-negative specimens were 47.1 and 98.6%. Only 1 of 15 culture-negative, AMPLICOR MTB-positive specimens was found to be false-positive. This patient was a case of healthcare associated pneumonia, which resolved completely after adequate antimicrobial therapy. He was followed up for one year without any evidence of pulmonary TB. The three specimens that yielded nontuberculous mycobacteria were negative by
both smear and the AMPLICOR MTB test. The overall performance of the AMPLICOR MTB test, culture and microscopy compared with final clinical diagnosis is listed in Table 4.
Discussion
When the performance of a new micro- biological test system is evaluated, culture has always been considered to be the gold standard. For the detection of M. tuberculosis, the specificity of culture is always considered to be 100%. The sensitivity, however, is often reported to be less than 90%. In a study of 261 patients, Krasnow and Wayne found that only 30% of the patients yielded Table 3. Analysis of 17 patients (21 specimens) who had clinical and radiographic evidences of pulmonary tuberculosis
but had negative culture for M. tuberculosis
Patient No. of AMPLICOR Smear Other culture-positive Histology proved
specimens MTB test specimens
A 2 + + Yes No
B 2 + + No No
C 2 + + No No
D 1 + + Yes No
E 1 + - No No
F 1 + - Yes No
G 1 + - Yes No
H 1 + - No Yes
I 1 + - Yes No
J 1 + - No Yes
K 1 + - Yes No
L 1 - + No No
M 1 - + Yes No
N 1 - + Yes No
O 1 - - No Yes
P 1 - - Yes No
Q 2 - - No No
Table 4. Overall performance of the AMPLICOR MTB test, culture and microscopy compared with final clinical diagnosis
No. of samples with test results
Methods Tuberculosis-positive* Tuberculosis-negative* Sensitivity Specificity Predictive value (n = 50) (n = 73) (%) (%) (%) Positive Negative Positive Negative Positive Negative
Culture 29 21 0 73 58 100 100 77.7
Microscopy 33 17 1 72 66 98.6 97.1 80.1
AMPLICOR MTB test 36 14 1 72 72 98.6 97.3 83.7
*Tuberculosis-positive and negative were defined according to final clinical diagnosis.
sputum positive on a single collection
15. If the diagnosis of pulmonary tuberculosis was made exclusively by the isolation of organisms, some patients would be missed. Thus we compared our results with both microbiologically and clinically proven pulmonary TB.
Using culture as the gold standard, the overall sensitivity of the AMPLICOR MTB test was 75.9%.
After resolution of discrepancies by final clinical diagnosis, the sensitivity was 72% which was not satisfactory. A similar low level of sensitivity of the AMPLICOR MTB test was reported elsewhere
16,17. Possible causes of the disappointing low level of sensitivity of the AMPLICOR MTB test were briefly investigated: (1) the possibility of a low intrinsic level of sensitivity of the Amplicor test system itself and inhibition of the amplification step by clinical DNA extracts, (2) inadequate specimen.
We did not test for the presence of inhibitors in our study, which have been reported to occur in 5-13% of specimens
5,18,19. Only 1 to 5% of sputum specimens were analyzed by PCR, while 50% were analyzed by culture. Such small amount might contribute to the lack of sensitivity. In addition, in this study, there were 4 specimens from 3 patients whose clinical diagnosis was pulmonary tuber- culosis, but culture, the AMPLICOR MTB test, and microscopy of these 4 specimens were all negative. There were 7 AMPLICOR MTB-neg- ative specimens which turned out to be positive after retesting from the specimen taken on another occasion. Some investigators suggested in order to obtain a high degree of sensitivity, PCR should be run as an adjunct to smear and culture with at least three samples for each patient
20. Three consecutive morning sputum were suggested not only for conventional culture and microscopy but also for PCR.
The sensitivity was significantly different between acid-fast microscopy positive and negative specimens (84.9 vs 47.1%). The high sensitivity
in microscopy positive specimens has also been reported elsewhere
13,21. A smear-positive specimen contains >5 x 10
3bacilli. It might be speculated that since there were less organisms in smear-nega- tive specimens, the sensitivity of PCR decreased accordingly. Therefore, the AMPLICOR MTB test can be used to confirm the diagnosis of M. tu- berculosis in microscopy positive specimens since smear could not differentiate M. tuberculosis from other species of mycobacteria. In smear-negative specimens, we could detect nearly half (47.1%) of the specimens to be positive. This still helped with the rapid diagnosis of pulmonary TB and would have impacted on the management of those patients.
When the AMPLICOR MTB test and microscopy were performed at the same time, up to 82% of specimens that were truly positive for tuberculosis could be detected.
The specificity of the AMPLICOR MTB test was 84% using culture as standard and was 98.6%
after adjustment by clinical diagnosis. There were 14 AMPLICOR MTB-positive, but culture-negative specimens that were found to be truly positive for tuberculosis after clinical resolution. Only 1 specimen was really a false positive. When culture is used as the standard, specimens containing non- cultivable bacteria, which may lead to a positive PCR result, are initially identified as false-positive samples. All 3 specimens of NTM were AMP- LICOR MTB-negative in our study. However, false-positive result due to isolation of NTM has been reported in another study
22. Although the AMPLICOR MTB test was shown to have a high specificity in this study, clinicians should be careful to rule out the possibility of NTM in a positive result of the AMPLICOR MTB test. Compared to our previous study
13, when clinical resolution was included as a gold standard, the specificity of the AMPLICOR MTB test was higher, but the sensitivity remained no difference.
The PPV was low for the Amplicor system
before resolution of discrepancy by final clinical diagnosis. In this study, it seemed to be influenced by the sensitivity of the reference method, because most of the AMPLICOR MTB-positive, culture- negative specimens were finally diagnosed as pulmonary TB. Since the prevalence of pulmonary TB remains high in Taiwan, the high PPV indicated that the AMPLICOR MTB test should be a useful and reliable diagnostic tool.
In this study, acid-fast microscopy revealed good sensitivity. In Daniel's investigation, the acid- fast smears of sputum were estimated to be positive in 30-40% of those with a single specimen
23. The auramine-rhodamine fluorochrome method for the detection of acid-fast microorganisms in specimens allows for rapid screening and may be more sen- sitive than the carbolfuchsin techniques
14. Only 1 specimen was false positive in our study. Ho- wever, this method has limitations, as mycobac- terium species cannot be identified by acid-fast microscopy.
The AMPLICOR MTB system was user friendly and well-suited to a clinical laboratory because up to 90 specimens could be amplified in a single run. Following concentration of the samples in the sample preparation area, the total time for completion of the test was about 5 to 6 hours depending upon the numbers of samples processed. The total time consisted of 1.5 hours of amplification and 2 hours of incubation time.
Although the AMPLICOR MTB test is relatively costly, this must be balanced by several factors:
earlier diagnosis resulting in fewer investigations, reduced hospital stay, earlier initiation of correct therapy, less use of inappropriate empirical therapy and a less risk of continued infectivity in or out the hospital.
In summary, the AMPLICOR MTB test can provide rapid and specific diagnosis for pulmonary TB in respiratory specimens. It may also detect cases missed by culture. The sensitivity was good in
smear-positive specimens and it enabled diagnosis of up to nearly 50% of smear-negative specimens.
Acknowledgments
Financial support. No financial support.
Potential conflicts of interest. All authors: no conflicts.
References
1. Raviglione MC, Snider DE, Jr., Kochi A. Global epide- miology of tuberculosis. Morbidity and mortality of a worldwide epidemic. JAMA 1995; 273: 220-6.
2. Annual Incidence and Mortality due to Newly Diagnosed Tuberculosis in Taiwan. Taiwan CDC 2008;<http://www.cdc.
gov.tw/public/Data/87141255971.pdf>.
3. Trends in tuberculosis--United States, 2007. Morb Mortal Wkly Rep 2008; 57: 281-5.
4. Cambanis A, Yassin MA, Ramsay A, Bertel Squire S, Arbide I, Cuevas LE. Rural poverty and delayed presentation to tuberculosis services in Ethiopia. Trop Med Int Health 2005;
10: 330-5.
5. Brisson-Noel A, Aznar C, Chureau C, et al. Diagnosis of tuberculosis by DNA amplification in clinical practice evaluation. Lancet 1991; 338: 364-6.
6. Eisenach KD, Cave MD, Bates JH, Crawford JT. Polymerase chain reaction amplification of a repetitive DNA sequence specific for Mycobacterium tuberculosis. J Infect Dis 1990;
161: 977-81.
7. Cousins DV, Wilton SD, Francis BR, Gow BL. Use of poly- merase chain reaction for rapid diagnosis of tuberculosis. J Clin Microbiol 1992; 30: 255-8.
8. Noordhoek GT, Kolk AH, Bjune G, et al. Sensitivity and specificity of PCR for detection of Mycobacterium tuberculosis: a blind comparison study among seven la- boratories. J Clin Microbiol 1994; 32: 277-84.
9. Noordhoek GT, van Embden JD, Kolk AH. Reliability of nucleic acid amplification for detection of Mycobacterium tuberculosis: an international collaborative quality control study among 30 laboratories. J Clin Microbiol 1996; 34:
2522-5.
10.Carpentier E, Drouillard B, Dailloux M, et al. Diagnosis of tuberculosis by Amplicor Mycobacterium tuberculosis test: a multicenter study. J Clin Microbiol 1995; 33: 3106-10.
11.Wobeser WL, Krajden M, Conly J, et al. Evaluation of Roche Amplicor PCR assay for Mycobacterium tuberculosis. J Clin Microbiol 1996; 34: 134-9.
12.Jan IS, Hsueh PR, Teng LJ, Lee LN, Yang PC, Luh KT.
Evaluation of an automatic polymerase chain reaction assay for identification of Mycobacterium tuberculosis in respiratory specimens. J Formos Med Assoc 1998; 97: 204-9.
13.Huang TS, Liu YC, Lin HH, Huang WK, Cheng DL. Com-
以 AMPLICOR MYCOBACTERIUM Test、
鏡檢和培養來診斷肺結核的比較
黃俊凱1
黃采菽
2,3林錫勳
1,3李欣蓉
2,3劉永慶
4,51
義大醫院 內科部感染科/義守大學
2
高雄榮總 內科部感染科及微生物科 3國立陽明大學
4
台北醫學大學醫學院 5雙和醫院 內科部感染科
摘 要
結核是台灣主要的公衛問題之一,要有效地控制結核仰賴著迅速而正確的診斷和適當 的治療。這個研究的目的是比較AMPLICOR MYCOBACTERIUM (AMPLICOR MTB) test、
鏡檢和培養用以診斷肺結核的成效。這個研究包括由90個疑似肺結核病人所採集的123套檢 體,所有檢體經過處理、 染色、培養和使用AMPLICOR MTB test 分析以鑑定結核分枝桿 菌。所有病人並追蹤一年以確定或排除肺結核的診斷。總共有29套檢體分離出結核分枝桿 菌,而根據臨床最後診斷為肺結核者共50個病人。與培養結果比較,AMPLICOR MTB test 的敏感性、特異性、陽性預測率、和陰性預測率分別為75.9,84,59.5,和91.9%。與最終 臨床診斷比較,其敏感性、特異性、陽性預測率、和陰性預測率分別為72,98.6,97.3,和
83.7%。針對抹片陽性檢體,其敏感性為 84.9%,而針對抹片陰性檢體,其敏感性為47.1%。
我們的研究顯示 AMPLICOR MTB test 用於快速診斷肺結核具有高度敏感性與特異性,而針 對抹片陰性檢體是否符合成本效益其仍有待進一步研究。
parison of the Roche AMPLICOR MYCOBACTERIUM assay and Digene SHARP Signal System with in-house PCR and culture for detection of Mycobacterium tuberculosis in respiratory specimens. J Clin Microbiol 1996; 34: 3092-6.
14.Murray PR, Baron EJ, Pfaller MA, Tenover FC, Yolken RH, eds. Manual of clinical microbiology. 6th ed. American Society for Microbiology, Washington, D.C. 1995; 33-51.
15.Krasnow I, Wayne LG. Comparison of methods for tu- berculosis bacteriology. Appl Microbiol 1969; 18: 915-7.
16.Schirm J, Oostendorp LA, Mulder JG. Comparison of Amplicor, in-house PCR, and conventional culture for detection of Mycobacterium tuberculosis in clinical samples.
J Clin Microbiol 1995; 33: 3221-4.
17.D'Amato RF, Wallman AA, Hochstein LH, et al. Rapid diagnosis of pulmonary tuberculosis by using Roche AMPLICOR Mycobacterium tuberculosis PCR test. J Clin Microbiol 1995; 33: 1832-4.
18.Nolte FS, Metchock B, McGowan JE, Jr., et al. Direct de- tection of Mycobacterium tuberculosis in sputum by po-
lymerase chain reaction and DNA hybridization. J Clin Microbiol 1993; 31: 1777-82.
19.Sjobring U, Mecklenburg M, Andersen AB, Miorner H.
Polymerase chain reaction for detection of Mycobacterium tuberculosis. J Clin Microbiol 1990; 28: 2200-4.
20.Devallois A, Legrand E, Rastogi N. Evaluation of Amplicor MTB test as adjunct to smears and culture for direct detection of Mycobacterium tuberculosis in the French Caribbean. J Clin Microbiol 1996; 34: 1065-8.
21.Bergmann JS, Woods GL. Clinical evaluation of the Roche AMPLICOR PCR Mycobacterium tuberculosis test for detection of M. tuberculosis in respiratory specimens. J Clin Microbiol 1996; 34: 1083-5.
22.Beavis KG, Lichty MB, Jungkind DL, Giger O. Evaluation of Amplicor PCR for direct detection of Mycobacterium tuberculosis from sputum specimens. J Clin Microbiol 1995;
33: 2582-6.
23.Daniel TM. Rapid diagnosis of tuberculosis: laboratory techniques applicable in developing countries. Rev Infect Dis. 1989; 11 (Suppl 2): S471-8.