1
Low-level laser treatment on relieving pain and neurological symptoms in
1
patients with carpal tunnel syndrome
2
3
Joe-Air Jiang
4
Department of Bio-Industrial Mechatronics Engineering, National Taiwan University,
5
No. 1, Sec. 4, Roosevelt Road, Taipei, 10617 Taiwan (R.O.C).
6 [E-mail: [email protected]] 7 8 Wen-Dien Chang* 9
Department of Recreation Sports and Health Promotion, Asian-Pacific Institute of Creativity,
10
NO. 110,Syuefu Rd,Toufen Township,Miaoli County 351,Taiwan (R.O.C.).
11 [E-mail: [email protected]] 12 13 Jih-Huah Wu 14
Department of Biomedical Engineering, Ming Chuan University,
15
No.5, Deming Rd., Guishan Township, Taoyuan County 333, Taiwan (R.O.C.).
16
[E-mail: [email protected]]
17
18
Ping Tung Lai
20
Department of Physical Therapy and Rehabilitation, Da Chien General Hospital,
21
No. 6, Shin Guang Street, Miaoli City 360, Taiwan (R.O.C).
22 [E-mail:[email protected]] 23 24 Hung-Yu Lin, 25
Department of Occupational Therapy, I-Shou University,
26
No.8, Yida Rd., Jiaosu Village Yanchao District, Kaohsiung City,Taiwan (R.O.C).
27 [E-mail: [email protected]] 28 29 *Correspondence author: 30
Wen-Dien Chang, Assistant Professor, Ph.D.
31
Department of Recreation Sports and Health Promotion
32
Asian-Pacific Institute of Creativity
33
NO. 110,Syuefu Rd,Toufen Township,Miaoli County 351,Taiwan
34 TEL: 886-37- 605766 35 FAX: 886-37- 605784 36 E-mail: [email protected] 37 38
3 ABSTRACT 39
〔Purpose〕This placebo-controlled study was investigated the therapeutic effects of low-level laser 40
treatment (LLLT) to apply on the transverse carpal ligament of carpal tunnel syndrome (CTS). 41
〔Subjects and Methods〕Idiopathic CTS patients were recruited and were randomly assigned to two 42
groups. The laser group (n = 45) received laser treatment (10 Hz, 60 mW, 9.7 J/cm2, 830 nm), but the
43
placebo group (n = 42) received sham laser treatment. The visual analog scale (VAS), Boston 44
Questionnaire scale, neurological symptoms and nerve conduction study (NCS) were assessed before, 45
immediately after and 5 week follow-up. 46
〔Results〕After LLLT, there was statistically significant decrease for VAS in laser group (p < 0.05). 47
Especially, the effect of LLLT on pain alleviation in the mild CTS group continued after five weeks. 48
Regarding Boston Questionnaire scale, neurological symptoms and NCS, only mild CTS patients in 49
the laser group had statistically significant improvements after treatment (p < 0.05). 50
〔Conclusions〕LLLT with 830 nm diodes laser on transverse carpal ligament had preferable 51
therapeutic effect for mild CTS patients. 52
53
54
55
INTRODUCTION 57
Carpal tunnel syndrome (CTS) is a median nerve lesion due to compression in the carpal tunnel. 58
The median nerve and tendons of the hand pass through the carpal tunnel and the transverse carpal 59
ligament locates on the palm side of the carpal tunnel. The tendons and transverse carpal ligament 60
become inflamed and swollen because of the pressure imposed on the median nerve below it1). The 61
abnormal sensation and weak muscle strength of hands are common clinical symptoms and signs. The 62
diagnosis of CTS is usually based on physical examination and electromyography. These symptoms 63
should be differentiated from the neural paralysis caused by diabetes or other metabolic diseases2). The 64
neurological symptoms are usually caused by high pressure on the median nerve inside the carpal 65
tunnel instead of the neuropathy of median nerve. 66
Many studies suggested that conservative treatments for the initial onset of CTS were safer than 67
surgeries3, 4). Low-level laser treatment (LLLT) is one of the choices of conservative treatments for 68
CTS5). The effects of LLLT in treating CTS were controversial. Some studies demonstrated that it had
69
better therapeutic effects to treat CTS5, 6, 7). However, one study found that LLLT did not have greater 70
improvements than other conservative treatments8). Recently, some researchers tried to use LLLT to 71
treat CTS and irradiated on the transverse carpal ligament of wrists9). They provided appropriate 72
parameters of LLLT and treatment location, but did not compare the therapeutic effects for different 73
severity of CTS. To go a step further, we tried to imitate the same process of LLLT for mild and 74
5
moderate symptoms of CTS. The purpose of our study was to investigate theclinical outcome and 75
neurophysiological results of the mild and moderate CTS. 76
77
SUBJECTS AND METHODS 78
This study was approved by the Institutional Review Board on Human Subjects Research. 79
Volunteers were the patients from the rehabilitation center of a teaching hospital and recruited from 80
the out-patient clinic. In Table 1, the patients with CTS were diagnosed in accordance with the 81
guideline10). For all patients, nerve conduction studies (NCS) on the ipsilateral ulnar nerve were 82
normal for both the motor and sensory conduction. 83
The inclusion criteria in our experiments were the patients with idiopathic CTS who experienced 84
repeated pain more than a year. The exclusion criteria included that patients had medical history of 85
systemic diseases (rheumatoid arthritis, diabetes, and metabolic diseases), received any surgical 86
operation and other treatments such as anti-inflammatory medicine, acupuncture, and physical therapy. 87
In the sample size of our study, the type I error was set 0.05 (α = 0.05) and power was set 0.8 (β = 0.2). 88
The required the number of samples which was calculated the outcomes based on literatures was at 89
least 14 for each group9). The 90 patients were randomly assigned to two groups based on the criterion 90
of a double blinding experiment. The laser group received LLLT, and the placebo group received 91
sham laser treatment. The sham laser had the same procedure as the laser treatment, but its power 92
supply was cut off and did not generate energy output in order to avoid any psychological effect. 93
The laser instrument (Painless Light PL-830, Advanced Chips & Products Corp., USA) was adopted 94
in this study. The operation parameters of PL-830 were as follows: wavelength = 830 nm; output 95
frequency = 10 Hz, average power = 60 mW (2 × 30mW); and the treatment dosage = 9.7 J/cm2, 96
respectively. The two diodes laser that emitted a laser beam (irradiated area = 370mm2) on the palm
97
side of the wrist (between pisiform and navicular bones). LLLT was executed for 10 minutes, and 5 98
times per week for two weeks. 99
Each patient was assessed before, immediately after the treatment, and in the five weeks follow-ups. 100
Four assessments, such as pain, symptoms, neurological signs, and nerve conduction study, were 101
blinded to one evaluator (test-retest reliability = 0.96). All data after the treatments and in the 102
follow-ups were collected and compared with a baseline before the treatments. 103
(1) Pain assessment: Pain intensity was assessed by a visual analog scale (VAS). The most painful 104
sensation would be scored 10 and painless sensation was scored 0. The patients who participated 105
in the study used their past experience of pain as criterion and scored their pain intensity at 106
present. 107
(2) Symptoms assessment: A self-administered questionnaire, Boston Questionnaire scale, is used to 108
describe the discomfort of CTS11). It consists eleven questions to assess the symptom (Table 2). 109
The symptom at night was assessed by items 1, 2, 9, and 10, and the symptom during the day was 110
estimated by items 3~8 and 11. The scale of each item was quantified to range from 1 (mildest) 111
to 5 (most severe), and all scales of individual items were calculated and averaged. 112
7
(3) Neurological signs: Two clinical tests for CTS were used. 113
Phalen’s sign test 114
The patients in this test bend their wrists by back-hand to back-hand against each other for 60 115
seconds. If there was a pricking or abnormal sensation in the radial side of the thumb, index finger, 116
middle finger and ring finger, then the test result would be positive. 117
Tinel’s sign test 118
Physician tapped the top of the carpal tunnel of patients’ wrists. If the patting caused a pricking or 119
abnormal sensation in the radial side of the thumb, index finger, middle finger and ring finger, then the 120
test result would be positive. 121
(4) Nerve conduction study 122
The NCS was performed with a portable electromyograph (Medelec Synergy, Oxford, UK), and the 123
stimulating electrodes were placed at the wrist proximal to the carpal tunnel. Accounting the 124
recommendations10), a pair of surface recording electrodes was placed on the abductor policis muscle
125
to record compound muscle action potentials. The distal motor latency and sensory peak latency of the 126
median nerve were measured by stimulating the nerve action potential. The room temperature 127
remained at around 26~29 °C. The NCS for the CTS patients were conducted and diagnosed by the 128
same physician, and the treatments were conducted by the same physical therapist. Both were blinded 129
in this study. 130
All data collected from the patients was analyzed by SPSS13.0, and each statistical parameter in 131
both groups was calculated. Because the distributions of all parameters using the 132
Kolmogorov-Smirnov test were not normal (p > 0.05), so non-parametric tests were used in our 133
statistical analysis. Mann-Whitney U Test was used to test the difference between the parameters of 134
the basic data before the treatment. For comparing the differences in VAS, symptom, neurological 135
signs, and NCS values of distal motor latency and sensory peak latency between both groups, the 136
Wilcoxon test was used. Mann-Whitney U Test was also used to analyze the differences of 137
assessments before and after the treatment, and in follow-ups. For categorical variables of Phalen’s 138
and Tinel’s sign tests, the Fisher exact test was used to compare the score before the treatment with 139
that after the treatment, and the scores in follow-ups. In all of the analyses, a two-tailed test was 140
adopted and the α value was set at 0.05. 141
142
RESULTS 143
In this study, there were 90 patients with CTS, but 3 patients of placebo group dropped out 144
during the experiment. In the laser group (n = 45), 27 patients were diagnosed as mild CTS, and 18 145
patients as moderate CTS. In the placebo group (n = 42), 27 patients were diagnosed as mild CTS and 146
15 patients as moderate CTS. In the baseline of age, duration, VAS, symptom, neurological signs, and 147
NCS, there were no statistically significant differences between two groups before the treatment (p > 148
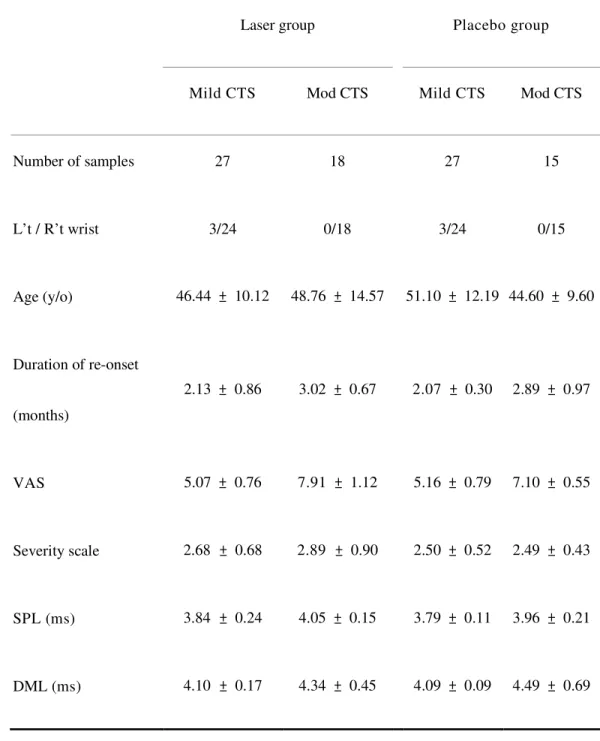
0.05). The basic data were summarized in Table 3. 149
9
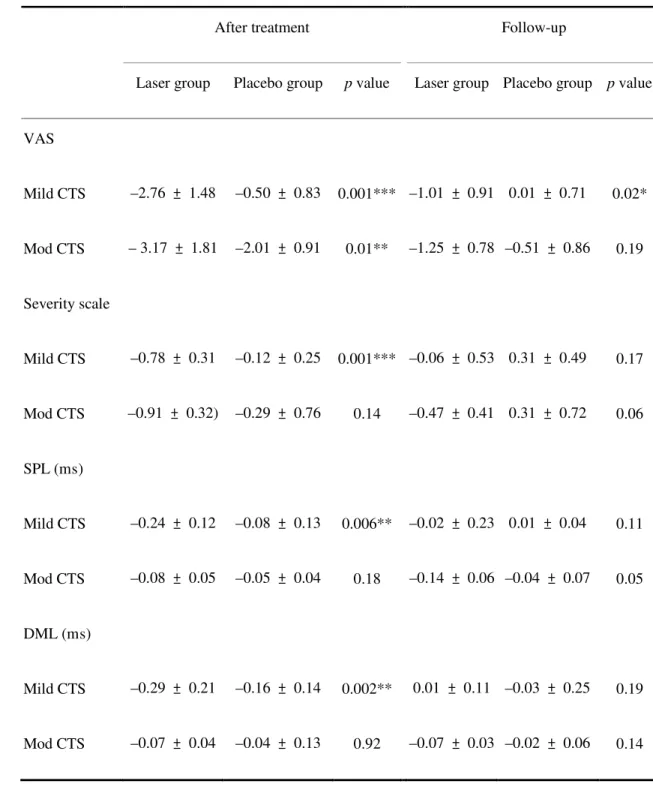
For the patients with either mild or moderate CTS, there was an obvious statistical difference (p < 150
0.05) in VAS decrease between the laser group and the placebo group after the treatment. In addition, 151
there was a significantly statistical difference (p < 0.05) in pain relief for the mild CTS patients during 152
follow-ups. 153
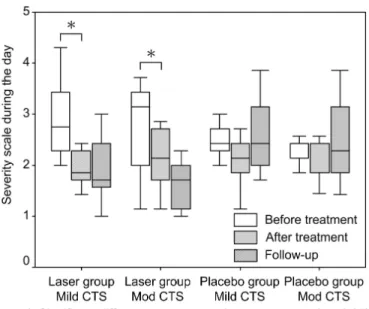
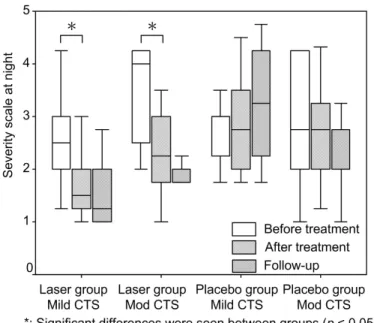
According to the statistical results, the decrease of the severity in the Boston Questionnaire scale 154
for the laser group is statistically greater than that for the placebo group, either during the daytime or 155
at night (p < 0.05, Fig. 1 and 2). After the treatment, there was a statistically significant decrease in the 156
total symptom scale for the patients with mild CTS in the laser group (p < 0.05), but not for the 157
placebo group (Table 4). 158
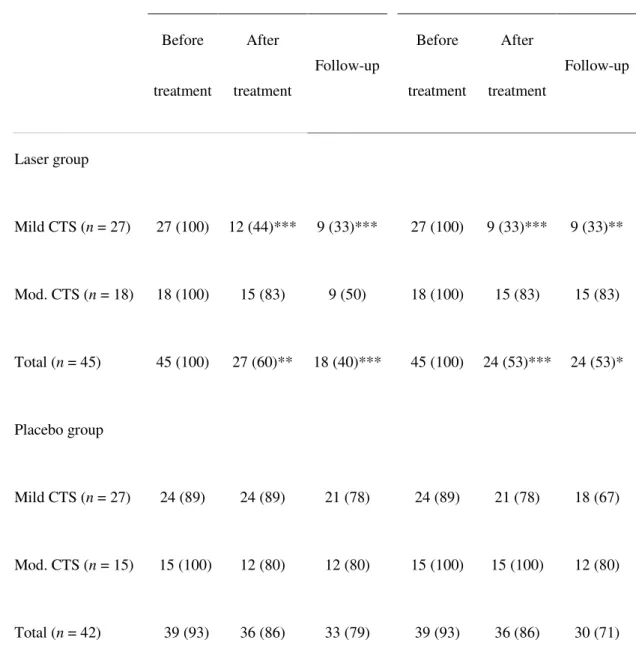
In the neurological signs for CTS (i.e., Phalen’s sign and Tinel’s sign), if those signs occurred 159
after the treatment, the assessment would be marked as a positive one. And if no signs occurred, the 160
assessment would be scored as a negative one. After the statistical analysis, as shown in Table 5, we 161
found that the amount of positive neurological signs in the Phalen’s sign and Tinel’s sign for the laser 162
group was reduced greater than that for the placebo group after the treatment and in the follow-ups. 163
This difference was statistically significant (p < 0.05). The laser group with mild CTS was particularly 164
statistically reduced in Phalen’s sign and Tinel’s sign. (p < 0.05). In the NCS for mild CTS, there was 165
a statistically difference between the laser group and the placebo group after the treatment (p < 0.05). 166
During the whole course of this study, no patient complained about any side effect and dropped 167
out from LLLT. 168
DISCUSSION 169
This research was a controlled study that tried to treat CTS via providing contact band irradiation 170
on transverse carpal ligament. After two weeks of LLLT with 830 nm laser, the VAS of the mild CTS 171
patients in the laser group was decreased to 2.32 ± 0.78. The VAS of the moderate CTS patients was 172
decreased to 3.76 ± 1.81. The results of our study were similar to the previous researches3, 5) and 173
confirmed immediate pain alleviation of LLLT. We also found that LLLT could not maintain this 174
effect for the next five weeks, and thus further research with longer follow-up periods were required. 175
The analgesic effect of LLLT is still controversial, but the clinical effect is confirmed4, 9). Many 176
researchers have discovered that LLLT could promote the production of adenosine triphosphate from 177
the mitochondria5, 7, 9, 12), and enhance the respiration metabolism of the cells13). Those metabolisms 178
reduce the wastes from the inflammation including leukotrienes and metabolite which could improve 179
the healing process. Fulop et al. found that the pain alleviation might be caused by serotonin and 180
endorphins14) which could effectively raise the pain threshold15). The CTS patients who had 181
neurological symptoms and pain due to the inflammation and swelling of the wrist often interfered 182
with functional hand activities. In the result of our study, we found that a decrease of symptoms in the 183
Boston Questionnaire scale accompanied a reduction of VAS. Although our study did not provide a 184
direct proof regarding the changes of biochemical reaction in the affected wrist, we believed that 185
LLLT had a positive effect on CTS. 186
11
The inflammation effect of the CTS wrist often causes neurological signs and median nerve 187
injury. In the electromyography, the mechanism of pain alleviation was better understood and the 188
reduction of pain could also be explained. In the previous research, LLLT was found to enhance the 189
conduction velocity of sural nerve after diode laser irritation on the normal nerve16).Our research found 190
that after the 830 nm LLLT, the NCS values of distal motor latency and sensory peak latency were 191
reduced. We conjectured that nerve conduction velocity increased due to the repair of nerves. This 192
contention is same as that in the past research17). Applied to clinical treatments of CTS, LLLT was 193
more effective than other conservative treatments18, 19). It was apparent based on their results as well as 194
ours, especially for the improvement in symptom severity and neurological signs. Elwakil et al. 195
compared LLLT with the standard open carpal tunnel release surgery, and found that LLLT could 196
improve hand weakness and the atrophy of thenar muscles7). The velocity of neural conduction also 197
showed statistical significance after the treatment (p < 0.05). Some studies found that LLLT performed 198
better than other conservative treatments in reducing neurological signs and nerve conduction 199
velocity18, 19). Although the effect on neural tissues generated by LLLT is not clear yet, the NCS of 200
CTS were found to be related to the degree of severity of the symptoms in our research. In our study, 201
irradiation area of LLLT was not the distribution of median nerve. We also found that the NCS of the 202
laser group were statistically less than those of the placebo group after applying LLLT to transverse 203
carpal ligament (p < 0.05). Accordingly, this result indicated that using the LLLT with an 830 nm 204
diodes laser on the injured nerve is effective. 205
In an animal research, Gigo-Benato et al. used laser irradiation (wavelength: 808 nm; dosage: 29 206
J / cm2; duration: 39 seconds) for the end-to-side neurorrhaphy of mouse, and irradiated directly on the 207
exposed axon of median nerve. They found that this approach could enhance the growth and healing 208
of the injured nerve20). However, it is difficult to apply to CTS patients. Because of median nerve of 209
human beings is located at the palm side of the wrist, and LLLT should target and reach the nerve in 210
the soft tissue under the skin. Thus, the laser energy might be absorbed by the soft tissue, and 211
insufficient energy reaches the injured nerve. Bakhtiary and Rashidy-Pour tried to use an 830 nm 212
point-like LLLT (1.8 J / point) to irradiate 5 points on the distribution of median nerve8), and they 213
obtained anunsuccessful result. The reason was that the nerve dispersion is different from each patient, 214
and this method is very hard to provide an appropriate dosage for the injured section of the nerve21). 215
Naeser et al. also tried to mark the hand and wrist with a square cm grid to treat each marked area with 216
the same dosage, and it resulted in an average dosage on each squares6). They found that the patients
217
experienced a pain alleviation of 50 %, but statistical difference was not seen (p > 0.05). Naeser et al. 218
asserted the reason for no obvious statistically difference in the assessment might be that the injured 219
nerve did not absorb enough treatment dosages6). Hence, the approach of point-like LLLT seemed 220
ineffectively to treat the CTS. Chang et al. thought that the main pathophysiology for CTS is the 221
inflammation and swelling of transverse carpal ligament, and essayed a beam-like diodes laser to 222
irradiate on transverse carpal ligament9). An identical 830 nm LLLT (9.7 J/cm2) on the injured 223
transverse carpal ligament wereimitated in our study. We also found that the pain alleviation for the
13
mild CTS patients was higher than that for the moderate CTS patients, and the reduction of symptoms 225
for the laser group was higher than that for the placebo group after two weeks of LLLT. As mentioned 226
in the previous research, it would take 4 to 5 weeks of LLLT to treat the mild and moderate CTS in 227
order to achieve statistically significant reductions of neurological symptoms (p < 0.05)6). We 228
considered that 830 nm diodes LLLT (9.7 J / cm2) is a referable parameter for CTS, and a beam-like
229
laser irradiated on transverse carpal ligament is a practical method. Therefore this kind of treatment is 230
effective, especially for mild CTS. 231
Traditionally, the preferred priority treatments for CTS were the conservative methods which aim 232
at pain relief and symptom alleviation3, 4). The successful treatment approaches include splinting, and 233
corticosteroid injection22). The success rate of splinting was 70%, but the rate decreased to a range 234
from 12% to 30% one year later23). The success rate of injection at a specified area for pain alleviation 235
ranged from 51 % to 93.5 %, but the rate declined and fell to a range between 6.5 % and 33 % after 236
one year24). However, we found that the disappearances of the Phalen’s sign and the Tinel’s sign 237
reached 40 % and 47 % respectively after LLLT, and 60% and 47 % after five weeks. However, the 238
comparison between LLLT and other conservative treatments was not investigated in this research, 239
and was still needed to study in the future. 240
241
REFERENCES 242
1) Prakash KM, Fook-Chong S, Leoh TH, et al.: Sensitivities of Sensory Nerve Conduction Study 243
Parameters in Carpal Tunnel Syndrome. Clin Neurophysiol, 2006, 23: 565-567. 244
2) Flak M, Durmala J, Czernicki K, et al.: Double crush syndrome evaluation in the median nerve in 245
clinical, radiological and electrophysiological examination. Stud Health Technol Inform, 2006, 123: 246
435-441. 247
3) Piazzini DB, Aprile I, Ferrara PE, et al.: A systematic review of conservative treatment of carpal 248
tunnel syndrome. Padua L Clin Rehabil, 2007, 21: 299-314. 249
4) Carlson H, Colbert A, Frydl J, et al.: Current options for nonsurgical management of carpal tunnel 250
syndrome. Int J Clin Rheumtol, 2010, 5: 129-142. 251
5) Naeser MA: Photobiomodulation of pain in carpal tunnel syndrome: review of seven laser therapy 252
studies. Photomed Laser Surg, 2006, 24: 101-110. 253
6) Naeser MA, Hahn KA, Lieberman BE, et al.: Carpal tunnel syndrome pain treated with low-level 254
laser and microamperes transcutaneous electric nerve stimulation: A controlled study. Arch Phys 255
Med Rehabil, 2002, 7: 978-988. 256
7) Elwakil TF, Elazzazi A, Shokeir H: Treatment of carpal tunnel syndrome by low-level laser versus 257
open carpal tunnel release. Lasers Med Sci, 2007, 22: 265-270. 258
8) Bakhtiary AH, Rashidy-Pour A: Ultrasound and laser therapy in the treatment of carpal tunnel 259
syndrome. Aust J Physiother, 2004, 50: 147-151. 260
9) Chang WD, Wu JH, Jiang JA, et al.: Carpal tunnel syndrome treated with a diode laser: a controlled 261
treatment of the transverse carpal ligament. Photomed Laser Surg, 2008, 26: 551-557. 262
15
10) Jablecki CK, Andary MT, Floeter MK, et al.: Practice parameter. Electrodiagnostic studies in 263
carpal tunnel syndrome. Report of the American Association of Electrodiagnostic Medicine, 264
American Academy of Neurology, and the American Academy of Physical Medicine and 265
Rehabilitation. Neurology, 2002, 58: 1589-1592. 266
11) Sezgin M, Incel NA, Serhan S, et al.: Assessment of symptom severity and functional status in 267
patients with carpal tunnel syndrome: reliability and functionality of the Turkish version of the 268
Boston Questionnaire. Disabil Rehabil, 2006, 28: 1281-1285. 269
12) Amat A, Rigau J, Waynant RW, et al.: Modification of the intrinsic fluorescence and the 270
biochemical behavior of ATP after irradiation with visible and near-infrared laser light. J 271
Photochem Photobiol, 2005, 81: 26-32. 272
13) Gao X, Xing D: Molecular mechanisms of cell proliferation induced by low power laser 273
irradiation. J Biomed Sci, 2009, 16: 4. 274
14) Fulop AM, Dhimmer S, Deluca JR : A meta-analysis of the efficacy of laser phototherapy on pain 275
relief.Clin J Pain, 2010, 26: 729-736.
276
15) Ay S, Doğan SK, Evcik D: Is low-level laser therapy effective in acute or chronic low back pain? 277
Clin Rheumatol, 2010, 29: 905-910. 278
16) Vinck E, Coorevits P, Cagnie B, et al.: Evidence of changes in sural nerve conduction mediated by 279
light emitting diode irradiation. Lasers Med Sci, 2005, 20: 35-40. 280
17) Shooshtari SM, Badiee V, Taghizadeh SH, et al.: The effects of low level laser in clinical outcome 281
and neurophysiological results of carpal tunnel syndrome. Electromyogr Clin Neurophysiol, 2008, 282
48: 229-231. 283
18) Yagci I, Elmas O, Akcan E, et al.: Comparison of splinting and splinting plus low-level laser 284
therapy in idiopathic carpal tunnel syndrome. Clin Rheumatol, 2009, 28: 1059-1065. 285
19) Dincer U, Cakar E, Kiralp MZ, et al.: The effectiveness of conservative treatments of carpal tunnel 286
syndrome: splinting, ultrasound, and low-level laser therapies. Photomed Laser Surg, 2009, 27: 119 287
-125. 288
20) Gigo-Benato D, Geuna S, de Castro Rodrigues A, et al.: Low-power laser biostimulation enhances 289
nerve repair after end-to-side neurorrhaphy: a double-blind randomized study in the rat median 290
nerve model. Lasers Med Sci, 2004, 19: 57-65. 291
21) Evcik D, Kavuncu V, Cakir T, et al.: Laser therapy in the treatment of carpal tunnel syndrome: a 292
randomized controlled trial. Photomed Laser Surg, 2007, 25: 34-39. 293
22) Gerritsen AA, de Krom MC, Struijs MA, et al.: Conservative treatment options for carpal tunnel 294
syndrome: a systematic review of randomised controlled trials. J Neurol, 2002, 249: 272-280. 295
23) Gerritsen AA, de Vet HC, Scholten RJ: Splinting vs surgery in the treatment of carpal tunnel 296
syndrome: a randomized controlled trial. JAMA, 2002, 288: 1245-1251. 297
24) Hui AC, Wong S, Leung CH, et al.: A randomized controlled trial of surgery vs. steroid injection 298
for carpal tunnel syndrome. Neurology, 2005, 64: 2074-2078. 299
17 300
Table 1. Diagnostic criteria of CTS 301
302
Diagnostic items Mild CTS Moderate CTS
Electromyography The sensory peak latency value of
median nerve was above 3.6 ms, and the
distal motor latency value was lower
than 4.3 ms.
The sensory peak latency value
of median nerve was above 3.6
ms, and the distal motor latency
value was above 4.3 ms.
Symptoms The patients also had two or more of the
following symptoms:
(1)Phalen’s sign
(2) Tinel’s sign
(3)wakefulness at night due to the pain
(4) wrist pain
(5)abnormal sensation in the first three
fingers.
The patients also had two or
Table 2. Boston Questionnaire scale 303
Items Scale
1. How severe is the hand or wrist pain that you have at night? 1~5
2. How often did hand or wrist pain wake you up during a typical night in the past
2 weeks?
1~5
3. Do you typically have pain in your hand or wrist during the daytime? 1~5
4. How often do you have hand or wrist pain during the daytime? 1~5
5. How long, on average, does an episode of pain last during the daytime? 1~5
6. Do you have numbness in your hand? 1~5
7. Do you have weakness in your hand and or wrist? 1~5
8. Do you have tingling sensations in your hand? 1~5
9. How severe is the numbness or tingling at night? 1~5
10. How often did hand numbness or tingling wake you up during a typical night
in the past two weeks?
1~5
11. Do you have difficulty with the grasping and use of small objects such as keys
or pens?
1~5
304
305
19 Table 3. The basic data in two groups
307
Laser group Placebo group
Mild CTS Mod CTS Mild CTS Mod CTS
Number of samples 27 18 27 15 L’t / R’t wrist 3/24 0/18 3/24 0/15 Age (y/o) 46.44 ± 10.12 48.76 ± 14.57 51.10 ± 12.19 44.60 ± 9.60 Duration of re-onset (months) 2.13 ± 0.86 3.02 ± 0.67 2.07 ± 0.30 2.89 ± 0.97 VAS 5.07 ± 0.76 7.91 ± 1.12 5.16 ± 0.79 7.10 ± 0.55 Severity scale 2.68 ± 0.68 2.89 ± 0.90 2.50 ± 0.52 2.49 ± 0.43 SPL (ms) 3.84 ± 0.24 4.05 ± 0.15 3.79 ± 0.11 3.96 ± 0.21 DML (ms) 4.10 ± 0.17 4.34 ± 0.45 4.09 ± 0.09 4.49 ± 0.69
All data are expressed as mean ± standard deviation, except for items of samples and L’t / R’t wrist, 308
which are presented as n. 309
VAS: Visual Analog Scale, SPL: Sensory Peak Latency, ML: Motor Latency. 310
Table 4. Mean changes from baseline scores of parameters, and analysis of changes after treatment 312
and five weeks follow-up 313
After treatment Follow-up
Laser group Placebo group p value Laser group Placebo group p value
VAS Mild CTS –2.76 ± 1.48 –0.50 ± 0.83 0.001*** –1.01 ± 0.91 0.01 ± 0.71 0.02* Mod CTS – 3.17 ± 1.81 –2.01 ± 0.91 0.01** –1.25 ± 0.78 –0.51 ± 0.86 0.19 Severity scale Mild CTS –0.78 ± 0.31 –0.12 ± 0.25 0.001*** –0.06 ± 0.53 0.31 ± 0.49 0.17 Mod CTS –0.91 ± 0.32) –0.29 ± 0.76 0.14 –0.47 ± 0.41 0.31 ± 0.72 0.06 SPL (ms) Mild CTS –0.24 ± 0.12 –0.08 ± 0.13 0.006** –0.02 ± 0.23 0.01 ± 0.04 0.11 Mod CTS –0.08 ± 0.05 –0.05 ± 0.04 0.18 –0.14 ± 0.06 –0.04 ± 0.07 0.05 DML (ms) Mild CTS –0.29 ± 0.21 –0.16 ± 0.14 0.002** 0.01 ± 0.11 –0.03 ± 0.25 0.19 Mod CTS –0.07 ± 0.04 –0.04 ± 0.13 0.92 –0.07 ± 0.03 –0.02 ± 0.06 0.14
Data are expressed as mean ± standard deviation. 314
*p < 0.05; **p < 0.01; ***p < 0.001. 315
21
Table 5. Number of participants (%) with positive neurological signs 316
Phalen’s sign test Tinel’s sign test
Before treatment After treatment Follow-up Before treatment After treatment Follow-up Laser group Mild CTS (n = 27) 27 (100) 12 (44)*** 9 (33)*** 27 (100) 9 (33)*** 9 (33)** Mod. CTS (n = 18) 18 (100) 15 (83) 9 (50) 18 (100) 15 (83) 15 (83) Total (n = 45) 45 (100) 27 (60)** 18 (40)*** 45 (100) 24 (53)*** 24 (53)* Placebo group Mild CTS (n = 27) 24 (89) 24 (89) 21 (78) 24 (89) 21 (78) 18 (67) Mod. CTS (n = 15) 15 (100) 12 (80) 12 (80) 15 (100) 15 (100) 12 (80) Total (n = 42) 39 (93) 36 (86) 33 (79) 39 (93) 36 (86) 30 (71)
Data are expressed as number of positive cases (percentage). 317
*p < 0.05; **p < 0.01; ***p < 0.001. 318
319
321
Fig. 1. Changes in the symptom scales during the day in both groups. 322 323 324 325 326 327 328 329 330 331 332 333
23 334
Fig. 2 Changes of symptom scales at night in both groups. 335