FRAILTY AND ITS ASSOCIATED FACTORS IN AN ELDERLY TAIWANESE METROPOLITAN POPULATION
Cheng-Chieh Lin, MD, PhD, 1,2,3 Chia-Ing Li, PhD,2,3 Nai-Hsin Meng, MD,4 Chiu-Shong Liu, MPH, MD,1,2,3 Chih-Hsueh Lin, MD, 1,2 Chiu-Kai Chang, MD,4 Yih-Dar Lee, MD,5,6
Cheng-Chun Lee, MD,1,7 Tsai-Chung Li, PhD *8,9
1 Department of Family Medicine, China Medical University Hospital, Taichung, Taiwan 2 School of Medicine, College of Medicine, China Medical University, Taichung, Taiwan 3 Department of Medical Research, China Medical University Hospital, Taichung, Taiwan 4 Department of Physical Medicine and Rehabilitation, China Medical University Hospital,
Taichung, Taiwan
5 Department of Psychiatry, Medical College, National Cheng-Kung University, Tainan, Taiwan
6 Bristol-Myers Squibb (Taiwan) Ltd, Global Development & Medical Affairs, Taipei, Taiwan
7 Department of Neurology, China Medical University Hospital, Taichung, Taiwan 8 Graduate Institute of Biostatistics, College of Public Health, China Medical University,
Taichung, Taiwan
9 Institute of Health Care Administration, College of Health Science, Asia University, Taichung, Taiwan
* Correspondence to: Tsai-Chung Li, China Medical University, 91 Hsueh-Shih Road, Taichung, 40421, Taiwan, Tel: 886-4-2205-3366 ext 6605, Fax: 886-4-22078539, e-mail: [email protected]
To the Editor: Frailty is considered to confer a high risk for adverse health outcomes,
including disability, falls, hospitalization and mortality.1-3 The overall prevalence of frailty in the community-dwelling population of Western countries has been reported to be around 6%– 40% using different definitions of frailty.3-7 The most commonly used definition of frailty was proposed by Fried et al.,4 and has shown its ability to predict physical disability, hospitalization, and mortality in a sample of community-dwelling older persons. Taiwan is facing the greatest of gerontological challenges because it has the fastest ageing population in the world. However, there are limited studies estimating the prevalence of frailty in Taiwan.18 In this study, we aimed to estimate the prevalence of frailty, as proposed by Fried et al., 4 and to explore its associated factors in a sample of a general elderly population in a Taiwanese metropolitan area.
This was a population-based cross-sectional study. The target population consisted of all residents who resided in community and aged 65 and over in eight administrative
neighborhoods of Taichung City, Taiwan in June, 2009. There were a total of 2,750 elderly were eligible, and 1,347 agreed to participate with the overall response rate of 49.0%. After excluding those elders with missing data, 1,009 subjects were included in the present data analysis. This study was approved by the Human Research Committee of China Medical University Hospital. Written informed consent was obtained from each participant.
We adopted the definition of frailty proposed by Fried et al., 4 which was composed of 5 components: shrinking, weakness, poor endurance and energy, slowness, and low physical activity level. Four of five frailty components were exactly the same as those proposed by Fried. Only weight loss was adapted. Those with none of the above components were considered as robust, whereas those with 1 or 2 components were considered as pre-fail and those with more than 2 components were hypothesized to be frail.
More than half of the elders were female, aged 65-74 years, with an educational attainment of 7 years or more, married, and with hypertension, pain problems and sleep
impairment. The overall prevalence of frailty in the study sample was 13.8% (95% confidence level [CI]: 10.9%-16.8%) for men and 13.7% (95% CI: 10.7%-16.8%) for women. The prevalence of frailty in men was 7.0% in those aged 65-74 years, 17.4% for those aged 75-84 years and 36.5% for those aged 85 and over; in women, the prevalence was 7.0% in those aged 65-74 years, 22.9% for those aged 75-84 years and 34.5% for those aged 85 and over. The weighted prevalence of frailty in men, women and overall was 14.8%, 15.6%, and 15.3%, respectively. Elders with diabetes, stroke, and pain problem were at significantly higher risk of having frailty after multivariate adjustment (odd ratio [OR]=2.21, 95% CI: 1.33, 3.68, OR=7.57, 95% CI: 3.99-14.33, and OR=2.01, 1.26, 3.21, respectively).
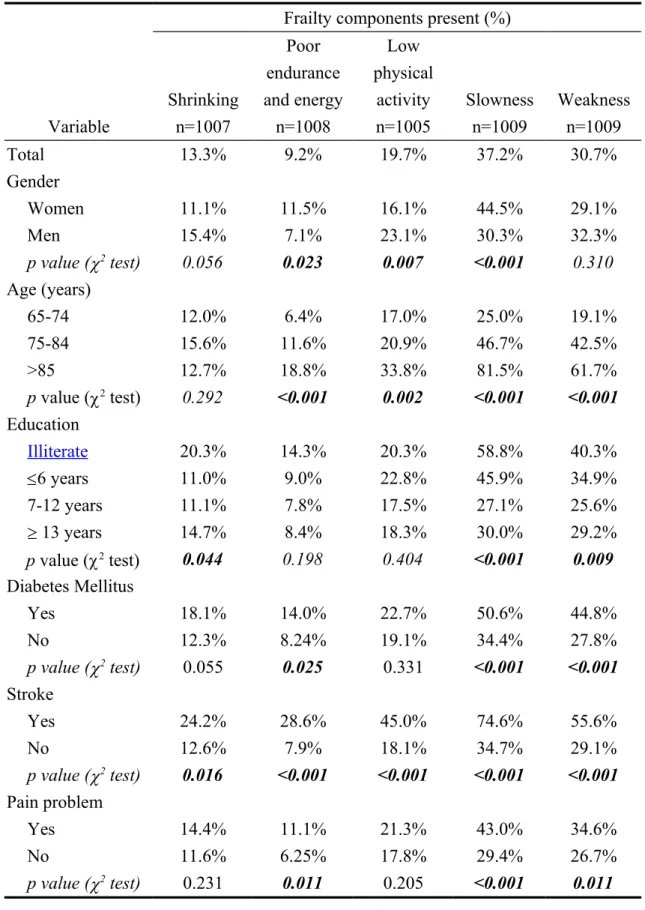
The overall prevalence of individual components of frailty stratified by gender, age, educational level, diabetes, stroke, and pain problem is shown in Table 1. A higher
prevalence of slowness and weakness was observed (37.2% and 30.7%, respectively). A higher prevalence of slowness and weakness was observed in older age, less education attainment elders, and elders with diabetes, stroke, and pain.
We used the criteria proposed by Fried et al. to evaluate the prevalence of frailty in an elderly non-institutionalized civilian population of a metropolitan area in Taiwan. Frailty was more common in women, and older age groups. Slowness and weakness were the most common frailty components in this population. These findings suggest that frailty is prevalent among the elderly Taiwanese population, and has become a serious public health challenge in Taiwan metropolitan areas.
A few surveys have been conducted in diverse community-dwelling populations to estimate the prevalence of frailty. 3,7, 8, 9 In general, our prevalence findings were lower than those in Spain (27.3%) and Italy (23.0%), closer to those in Greece (14.7%), France (15.0%), Germany (12.1%), the Netherlands (11.3%) and Denmark (12.4%), but higher than those in Austria (10.8%), Switzerland (5.8%), Sweden (8.6%) and England (6.3%).9 Most of these studies used the definition proposed by Fried et al.4 Those studies using study-specific criteria
of frailty reported prevalence ranging from 14% to 30%.10
In conclusion, frailty was present in 17% of the elderly Taiwanese population in a metropolitan area. Efforts such as exercise, comprehensive geriatric assessment and
interventions targeting frailty components are needed to reduce adverse effects in this elderly population.
ACKNOWLEDGMENTS
Conflict of Interest: The editor in chief has reviewed the conflict of interest checklist provided by the authors and has determined that the authors have no financial or any other kind of personal conflicts with this paper. This study was supported by grants from the National Health Research Institutes of Taiwan (NHRI-EX98-9838PI), China Medical University (CMU98-S-11 & CMU 99-S-27), and the Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH100-TD-B-111-004).
Author Contributions: Study concept and design: CC Lin, TC Li. Analysis and
interpretation of data: TC Li, CI Li, CS Liu. Critical revision of the manuscript for important intellectual content: NH Meng, CH Lin, CK Chang, YD Lee, CC Lee. Wrote the paper: CC Lin, TC Li.
References
[1] Hamerman D. Toward an understanding of frailty. Ann Intern Med 1999;130:945-950. [2] Walston J, Hadley EC, Ferrucci L et al. Research Agenda for Frailty in Older Adults:
Toward a Better Understanding of Physiology and Etiology: Summary from the
American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J Am Geriatr Soc. 2006;54(6):991-1001.
[3] Fried LP, Ferrucci L, Darer J et al. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci 2004;59(3):255-263.
[4] Fried LP, Tangen CM, Walston J et al. Frailty in older adults: evidence for a phenotype.
J Gerontol A Biol Sci Med Sci 2001;56(3):M146-M156.
[5] Avila-Funes JA, Helmer C, Amieva H, et al. Frailty among community-dwelling elderly
people in France: the three-city study. J Gerontol A: Biol Sci Med Sci 2008;63:1089-1096.
[6] Fernandez-Bolaños M, Otero A, Zunzunegui MV et al. Sex differences in the prevalence
of frailty in a population aged 75 and older in Spain. J Am Geriatr Soc 2008;56:2370-2371.
[7] Chen CY, Wu SC, Chen LJ et al. The prevalence of subjective frailty and factors
associated with frailty in Taiwan. Arch Gerontol Geriatr 2010;50 (Suppl 1): S43-S47.
[8] Syddall H, Roberts HC, Evandrou M et al. Prevalence and correlates of frailty among
community-dwelling older men and women: findings from the Hertfordshire Cohort Study. Age Ageing2010;39(2):197-203.
[9] Santos-Eggimann B, Cuénoud P, Spagnoli Jet al. Prevalence of frailty in middle-aged
and older community-dwelling Europeans living in 10 countries. J Gerontol A Biol Sci
[10] Jones DM, Song X, Rockwood K. Operationalizing a frailty index from a standardized comprehensive geriatric assessment. J Am Geriatr Soc 2004;52(11):1929-1933.
Table 1. Prevalence of frailty components according to demographic characteristics
Frailty components present (%)
Shrinking Poor endurance and energy Low physical
activity Slowness Weakness
Variable n=1007 n=1008 n=1005 n=1009 n=1009 Total 13.3% 9.2% 19.7% 37.2% 30.7% Gender Women 11.1% 11.5% 16.1% 44.5% 29.1% Men 15.4% 7.1% 23.1% 30.3% 32.3% p value (2 test) 0.056 0.023 0.007 <0.001 0.310 Age (years) 65-74 12.0% 6.4% 17.0% 25.0% 19.1% 75-84 15.6% 11.6% 20.9% 46.7% 42.5% >85 12.7% 18.8% 33.8% 81.5% 61.7% p value (2 test) 0.292 <0.001 0.002 <0.001 <0.001 Education Illiterate 20.3% 14.3% 20.3% 58.8% 40.3% £6 years 11.0% 9.0% 22.8% 45.9% 34.9% 7-12 years 11.1% 7.8% 17.5% 27.1% 25.6% ³ 13 years 14.7% 8.4% 18.3% 30.0% 29.2% p value (2 test) 0.044 0.198 0.404 <0.001 0.009 Diabetes Mellitus Yes 18.1% 14.0% 22.7% 50.6% 44.8% No 12.3% 8.24% 19.1% 34.4% 27.8% p value (2 test) 0.055 0.025 0.331 <0.001 <0.001 Stroke Yes 24.2% 28.6% 45.0% 74.6% 55.6% No 12.6% 7.9% 18.1% 34.7% 29.1% p value (2 test) 0.016 <0.001 <0.001 <0.001 <0.001 Pain problem Yes 14.4% 11.1% 21.3% 43.0% 34.6% No 11.6% 6.25% 17.8% 29.4% 26.7% p value (2 test) 0.231 0.011 0.205 <0.001 0.011