Ethambutol-Induced Optic Neuropathy: A Nationwide Population-based Study from Taiwan
Hsin-Yi Chen1, 2, Shi-Wei Lai3,4, Chih-Hsin Muo5, Pei-Chun Chen1,5,6*, I-Jong Wang7*
1 Graduate Institute of Clinical Medical Science, China Medical University, Taichung, Taiwan
2 Department of Ophthalmology, China Medical University Hospital, Taichung, Taiwan
3 School of Medicine, China Medical University, Taichung, Taiwan
4 Department of Family Medicine, China Medical University Hospital, Taichung, Taiwan
5 Management Office for Health Data, China Medical University and Hospital, Taichung, Taiwan
6 Graduate Institute of Epidemiology and Preventive Medicine, National Taiwan University College of Public Health, Taipei, Taiwan
7 Department of Ophthalmology, National Taiwan University Hospital, Taipei, Taiwan
Running Title: EMB optic neuropathy, Taiwan.
*Total word count: 2253, total number of pages: 20 .
* Financial Disclosure(s): The authors have no commercial or proprietary interest in any of the materials discussed in this article.
* This work was supported by Taiwan National Sciences Council (NSC 98-2621-M-039-001), Department of Health Clinical Trial and Research Center of Excellence (DOH100-TD-B-111-004), and the China Medical University Hospital (1MS1). * Corresponding author: Pei-Chun Chen, PhD, email: [email protected], and I-Jong Wang MD, PhD, email: [email protected]
Contributorship Statement:
Dr. Chen Hsin-Yi: conception and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, critical revision of the manuscript for important intellectual content, obtaining funding.
Dr.
Shih-Wei Lai : conception and design, analysis and interpretation of data, critical revision of the manuscript for important intellectual content
Chih-Hsin Muo: statistical expertise, conception and design, critical revision of the manuscript for important intellectual content.
Dr. Pei-Chun Chen: statistical expertise, conception and design, critical revision of the manuscript for important intellectual content, obtaining funding.
Dr. I-Jong Wang: critical revision of the manuscript for important intellectual content, supervision.
Abstract
Aim: To investigate the risk factors and co-morbidities associated with
ethambutol-induced optic neuropathy (EON).
Method: Using the Taiwan Longitudinal Health Insurance Database, we conducted
a study within a nationwide representative cohort of patients treated with ethambutol (EMB). We identified 231 patients newly diagnosed with EON between 2000 and 2008 and 924 control subjects. Adjusted odds ratios (OR) by estimating the risk of EON in relation to co-morbidities and EMB prescription protocol was determined.
Results: Compared to control group, EON patients were at risk with older age,
hypertension (adjusted OR=1.62, 95% confidence interval [CI]=1.16-2.26) and renal diseases (without end-stage renal diseases [ESRD], adjusted OR=2.11, 95% CI=1.02-4.35; with ESRD, adjusted OR=3.73, 95% CI=1.79-7.74). Patients with an EMB prescription duration longer than 3 months were not at elevated risk compared with those whose prescription less than 3 months (OR=1.35, 95% CI: 0.99-1.83, adjusted for age, sex, hypertension and renal diseases). Patients whose average daily dose was greater than 1200 mg, compared with the other two groups (800 ~1199 mg, less than 800 mg) were not at increased risk for EON.
Conclusion: Age, hypertension and renal diseasess are risk factors for EON in
Taiwanese population.
Introduction
Although EMB is well-known to be the most common cause of toxic optic neuropathy,1,2 it is still commonly used in medical practice due to increasing drug-resistance of tuberculosis treatment.1,4 The incidence of EON, its clinical characteristics and risks factors, and its dosage information have been poorly described and characterized in many previous studies.2-6 However, the causes of EON and its risk factors remain to be determined. Some previous studies showed that EON is dose-related and reversible,7 but others revealed a controversial result.8-12 Because these ambiguities, the reported incidence of the toxicity varies widely across studies, ranging from 0.5% to more than 35%.Unfortunately, with the increase in the number of cases reporting irreversible EON3-6, an urgency exists to identify the potential risk factors associated with EMB. To better understand the risk factors related to EON in our population, we conducted this study using an eight-year population-based dataset from the Taiwan National Health Insurance (NHI) Program.
Methods
available and are sent to the National Health Research Institute, which collaborates with the NHI to construct the National Health Insurance Research Database.16 For research purpose, the Longitudinal Health Insurance Database was established. This dataset , which comprising of one million beneficiaries randomly selected from all people enrolled in NHI between 1996 and 2000, include files of registration, ambulatory care claims, inpatient claims, and prescription drugs and provides information on health care utilization.
Cases and Controls
This study consists of 11,753 subjects who were dispensed EMB between 1996 and 2008. The cohort was comprised of patients who were 20 years of age or older and who were diagnosed with EON between 2000 and 2008 on either an inpatient or an outpatient basis. All cohort participants were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9) code 377. A control group was randomly selected from the remaining subjects who did not experience EON but were on EMB during the specified time period. This resulted in a case-to-control ratio of 1:4. The index date of the case subject was the date of their EON diagnosis. For each control subject, we assigned an index date frequency matching the index year and the month associated with each of the case subjects. Study subjects with missing information on sex and birth date were excluded.
Finally, a total of 231 patients with EON (cumulative incidence, 2% [231/6369]; incidence density: 36.3 per 1000 person-years) and 924 control group subjects were included.
Variables
We scanned diagnosis information on outpatient and inpatient claims before the index date to identified some comorbidities, including diabetes mellitus (ICD-9 250.XX), obesity (ICD-9 278.0, 278.00, and 278.01), hypertriglyceridemia (ICD-9 272.1), alcoholism (ICD-9 303, 305.00, 305.01, 305.02, 305.03, and v11.3), gallstones (ICD-9 574.00, 574.01, 547.10, 574.11, 574.20, and 574.21), hepatitis B (ICD-9 V02.61, 070.20, 070.22, 070.30, and 070.32), hepatitis C (ICD-9 V02.62, 070.41, 070.44, 070.51, and 070.54), hypertension (ICD-9 401-405), renal diseases (ICD-9 585, 586, 588.8, and 588.9), systemic lupus erythematosus (SLE, ICD-9 710.xx), Reiter’s syndrome (ICD-9 711.1x), rheumatoid arthritis and other inflammatory polyarthopathies (ICD-9 714.xx), palindromic rheumatism (ICD-9 719.3x), polymyalgia rheumatica (ICD-9 725), and malignant illness (ICD-9 140 – 208). To assess whether the risk of EON increases in patients with advanced stage renal diseases, we further classified this group into two subgroups (end-stage renal diseases, ESRD &non-ESRD). Patients with ESRD were identified using the Catastrophic Illness Registry. In the NHI program, patients with ESRD were eligible
to apply for a catastrophic illness certification, which allows for the waiver of copayments for medical care related to ESRD. In both the EON case group and the controls, prescription duration and average daily dosage of EMB were calculated from the date of the participant’s first prescription until the index date. Average daily dose was calculated by dividing total number of milligrams prescribed by total number of days supplied during the year before the index date. According to the standard prescription guideline for EMB,18 we stratified the average daily dosage into three categories: 1) less than 800 mg, 2) 800-1199 mg, 3) greater than 1200 mg. The compliance in these patients is assessed under directly observed therapy by health care personnel.
Statistical Analysis
We compared the differences in sex, age, and comorbidities between case group and control group using Pearson’s chi-square test. The logistic regression model, which estimated the odds ratio (OR) and a 95% confidence interval (CI), was used to evaluate the association between age, sex, comorbid disease, and the risk of EON. The logistic regression analyses did not include the comorbidities in which the prevalence rates were similar between case group and the controls or the comorbidities in which the prevalence rates were very low in both groups. We did not select the comorbidities for inclusion relying on p values due to the small
number cases with comorbidities. We further examined whether patients with coexisting hypertension, diabetes, and renal diseases were at a greater risk of EON. Odds ratios for optic neuropathy in relation to duration of EMB prescription and average daily dosage were calculated too. All analyses were performed using SAS statistical software (Version 9.1 for Windows; SAS Institute, Inc., Cary, NC, USA). We used a two-tailed test for all analyses and the significance level was set at a p
value < 0.05.
Results
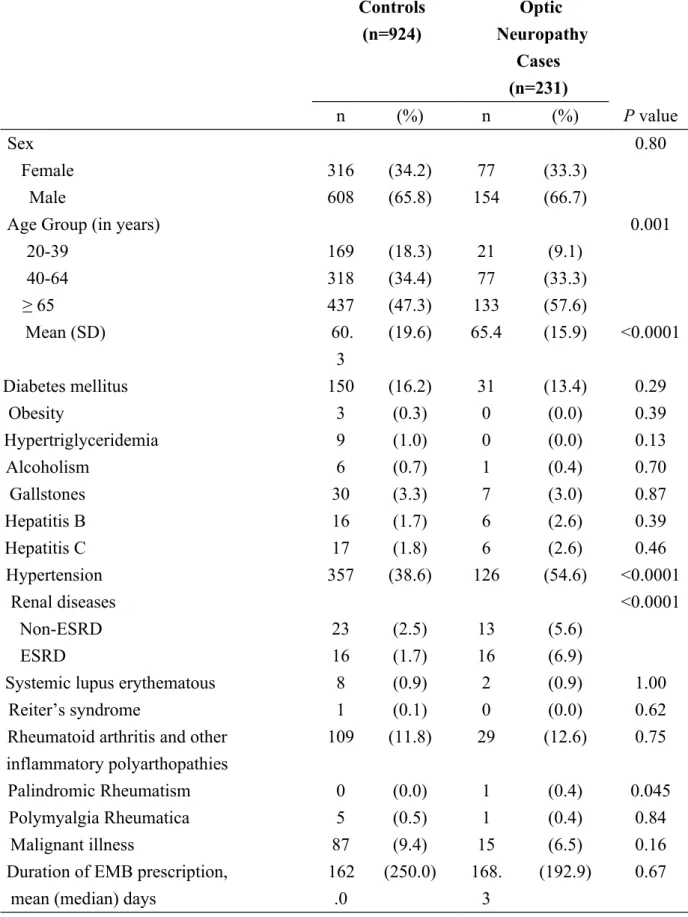
In both the EON group (case) and the non-EON group (control), patients taking EMB were more likely to be male (Table 1). The patients in the EON group (65.4 ± 15.9 years) were older than the controls (60.3 ± 19.6 years). Compared to the control group, the EON group was more likely to have hypertension (54.6% vs. 38.6%) and renal diseases (non-ESRD, 5.6% vs. 2.5%; ESRD, 6.9% vs. 1.7%, P<0.0001).
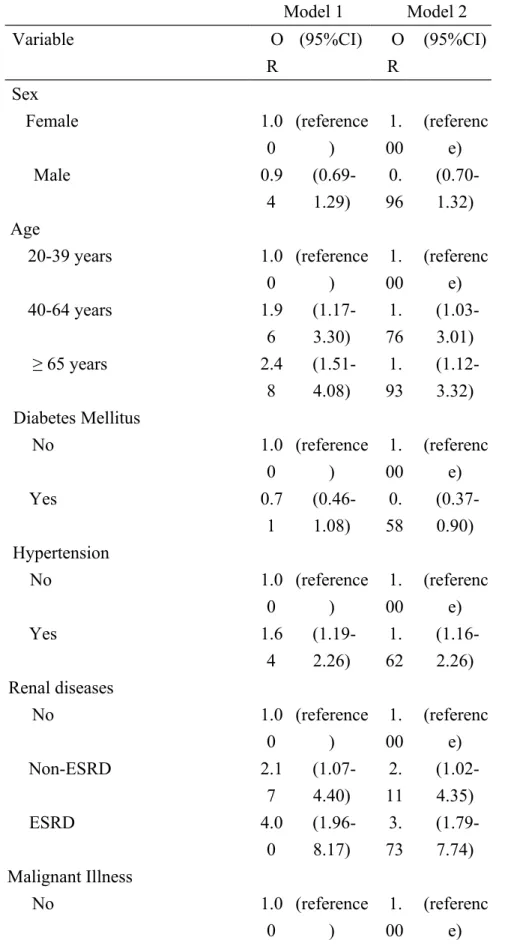
In the logistic regression models adjusted for age, sex, diabetes, hypertension, renal diseases, and malignant illness, the OR for EON in patients aged 40-64 years, compared with patients in the 20-39 year age range, was 1.76 (Table 2, Model 2). The adjusted OR increased to 1.93 for patients aged 65 years and older. Hypertension was associated with an increased risk of EON (OR=1.62).
Additionally, patients with renal diseases also showed an elevated risk for EON compared with subjects without renal diseases. For patients who had renal diseases but without ESRD, the adjusted OR was 2.11; the adjusted OR rose to 3.73 for patients with ESRD. However, diabetes was associated with a decreased risk of EON. The risk was not statistically significant in the age-adjusted and sex-adjusted model (Model 1, OR=0.71), but the risk became significant after an adjustment was made for other comorbidities (Model 2, OR=0.58).
Table 3 indicates the adjusted ORs of EON in patients with coexisting diabetes, hypertension, and renal diseases compared with those without these diseases. The OR for patients with hypertension alone was 1.79 and increased to 3.84 for hypertensive patients with renal diseases. The OR for patients having all three of these comorbidities was 3.94. For renal diseases alone, the OR was 2.42, but it was
not statistically significant.
Table 4 presents the OR of EON in relation to duration of the EMB prescription. Patients whose EMB prescription duration were longer than 3 months were found to be at a mild elevated risk of EON compared with those who less than 3 months ( OR=1.38, 95% CI: 1.02-1.86, Model 1, adjusted for age and sex). However, when additionally adjusted for hypertension and renal diseases, there is no
Table 5 shows the result of OR for optic neuropathy in relation to average daily dosage of EMB prescription. For all cases treated with EMB, relative to the group whose average daily dose was less than 800 mg, the other two groups were not with increased risk for EON. Same result was noted in the cases with renal diseases. Mild increased risk for EON was only noted in the group whose average daily dose was between 800-1199 mg in the cases without renal diseases (OR: 1.46, 95 % CI: 1.04-2.06).
Discussion
This study used population-based data to understand the comorbidities associated with EON in Taiwan, which is one of the few studies investigating the roles of multiple systemic factors in EON in a large Chinese cohort. Our results show that patients with EON were found to be older and to have hypertension and renal diseases compared to the controls. Our result is in agreement with the general belief that advanced age and renal diseases are the most common two risk factors for EON. In one recent meta-analysis of 70 EON cases, the authors noted that the majority of patients were over 40 years of age and 40% of them were over 65,4 which is consistent with our result (57.6 %, over 65 years old). However, when the authors further considered the CDC’s statistics on the age distribution of tuberculosis cases, they found that the number of cases of tuberculosis decreased with increasing age
after peaking in the 25–44 age group.19 They postulated that age was an independent risk factor for EON based on the thought that renal function decreases related to aging.19 Although renal tubular function is known to decrease with age,17 the aging effect of EMB clearance is not yet known. Compared with that study, our current logistic analysis model could explain age should be a strong risk factor for EON.
Furthermore, our analysis identified some other interesting findings. First, hypertension was associated with an increased risk of EON (OR=1.62), which has seldom been reported. Secondly, diabetes was associated with non-statistically significant reduction in risk of EON in the age- and sex- adjusted model, and the association became statistically significant after further adjusting hypertension and renal disease. The role that diabetes plays in EON need be further elucidated in a future study. Thirdly, patients with renal diseases were also at an elevated risk for EON compared with subjects without renal diseases. The adjusted OR for patients with renal diseases but without ESRD was 2.11 and this rose to 3.73 for patients with ESRD. This important result confirms the previous belief that poor renal function is an important risk factor for EON.
Because hypertension and renal disease are both risk factors of EON, we further examine the joint effect of these comorbidities on EON risk. To assess the influence of diabetes on the associations, the analysis was also stratified by diabetes.
The adjusted OR for patients with hypertension only was 1.79 and for patients with renal diseases only was 2.42 (not statistically significant). The adjusted OR for patients with hypertension only was 1.79 and increased to 3.84 for those with coexisting renal disease. The OR was at similar strength for patients who were also comorbid for diabetes. This study is the first to notice that hypertension is a potential aggravating factors for EON in patients with renal diseases.
Conflicting results about the treatment protocol of EMB on EON were noted.12,13 One recent meta-analysis study has reported that duration of EMB, and dose of EMB were positively correlated with risk of EON.13 Another study in Korea,12 they reported that renal dysfunction and daily dose of EMB, but not duration of EMB treatment, seem to be related to development of EON. To clarify this important issue in our population, we further analyzed the EMB dosing regimen, including the prescription duration and average daily dosage. Interestingly, our result reveals that both prescription duration and average daily dosage do not have significant association with the risk of EON. We believe this most likely represents an idiosyncratic reaction of EMB in our Chinese population. Furthermore, we found the majority of EMB treated cases (about 88%) were on average less than 1200 mg/ per day. According to the treatment guideline of tuberculosis,18 recommended dose was standardized for three or four body weight
bands. It is a great pity that the body weight data were not available in our dataset; therefore, we failed to understand the real daily dose based on weight. This is a major limitation in this study compared to others and constrains a direct comparison with previous studies because of different study design and statistical method. However, this result could be a good basis for future prospective study in EON.
Although the results are quite meaningful, some limitation should be mentioned. First, the EON diagnoses were totally reliant upon claims data (ICD-9 coding from clinicians), which may be less accurate than diagnoses carried out individually through a standardized procedure. Second, other selection biases also inherit in this kind of retrospective study. Because the vision and body weight data were not available in our health insurance database, we were unable to understand the real dose effect on the severity of vision impairment in each patient based on body weight. Even so, this dataset has good sample randomization.18 Furthermore, to avoid miss diagnosis for case group, we ensured that all study cohort should have EON diagnoses in consensus with concurrent and continuous intake of EMB. Forth, because we could not determine compliance in this retrospective study; however, comments on how compliance is assessed in these patients (directly observed therapy, etc) would be useful to have. Additionally, we excluded any tuberculosis case coded with any
optic neuropathy (ON) before EMB use.
In summary, age factor, hypertension and renal diseases were found to be important risk factors for EON. The important issue of dosing regimen of EMB on EON should be clarified in future study. Hope our current work could help patients avoid this vision threatening disease.
Table 1. Characteristics of optic neuropathy cases and control subjects selected from EMB–treated patients
Controls (n=924) Optic Neuropathy Cases (n=231) n (%) n (%) P value Sex 0.80 Female 316 (34.2) 77 (33.3) Male 608 (65.8) 154 (66.7)
Age Group (in years) 0.001
20-39 169 (18.3) 21 (9.1) 40-64 318 (34.4) 77 (33.3) ≥ 65 437 (47.3) 133 (57.6) Mean (SD) 60. 3 (19.6) 65.4 (15.9) <0.0001 Diabetes mellitus 150 (16.2) 31 (13.4) 0.29 Obesity 3 (0.3) 0 (0.0) 0.39 Hypertriglyceridemia 9 (1.0) 0 (0.0) 0.13 Alcoholism 6 (0.7) 1 (0.4) 0.70 Gallstones 30 (3.3) 7 (3.0) 0.87 Hepatitis B 16 (1.7) 6 (2.6) 0.39 Hepatitis C 17 (1.8) 6 (2.6) 0.46 Hypertension 357 (38.6) 126 (54.6) <0.0001 Renal diseases <0.0001 Non-ESRD 23 (2.5) 13 (5.6) ESRD 16 (1.7) 16 (6.9)
Systemic lupus erythematous 8 (0.9) 2 (0.9) 1.00
Reiter’s syndrome 1 (0.1) 0 (0.0) 0.62
Rheumatoid arthritis and other inflammatory polyarthopathies
109 (11.8) 29 (12.6) 0.75
Palindromic Rheumatism 0 (0.0) 1 (0.4) 0.045
Polymyalgia Rheumatica 5 (0.5) 1 (0.4) 0.84
Malignant illness 87 (9.4) 15 (6.5) 0.16
Duration of EMB prescription, mean (median) days
162 .0
(250.0) 168. 3
(192.9) 0.67 Abbreviation: ESRD refers to end-stage renal diseases.
Table 2. Adjusted odds ratios for optic neuropathy in relation to medical comorbidities Model 1 Model 2 Variable O R (95%CI) O R (95%CI) Sex Female 1.0 0 (reference ) 1. 00 (referenc e) Male 0.9 4 (0.69-1.29) 0. 96 (0.70-1.32) Age 20-39 years 1.0 0 (reference ) 1. 00 (referenc e) 40-64 years 1.9 6 (1.17-3.30) 1. 76 (1.03-3.01) ≥ 65 years 2.4 8 (1.51-4.08) 1. 93 (1.12-3.32) Diabetes Mellitus No 1.0 0 (reference ) 1. 00 (referenc e) Yes 0.7 1 (0.46-1.08) 0. 58 (0.37-0.90) Hypertension No 1.0 0 (reference ) 1. 00 (referenc e) Yes 1.6 4 (1.19-2.26) 1. 62 (1.16-2.26) Renal diseases No 1.0 0 (reference ) 1. 00 (referenc e) Non-ESRD 2.1 7 (1.07-4.40) 2. 11 (1.02-4.35) ESRD 4.0 0 (1.96-8.17) 3. 73 (1.79-7.74) Malignant Illness No 1.0 0 (reference ) 1. 00 (referenc e)
Yes 0.5 8 (0.33-1.03) 0. 63 (0.35-1.13) Abbreviation: ESRD refers to end-stage renal diseases.
Model 1 was adjusted for age and sex.
Table 3. Adjusted odds ratios for optic neuropathy in relation to hypertension, diabetes, and renal diseases Controls (n=924) % Optic Neuropathy cases (n=231) % Odds Ratio (95% CI) Hypertension Diabete s Renal diseases - - - 517(56.0) 94(40.7) 1.00 + - - 231(25.0) 87(37.7) 1.79(1.23-2.58) - + - 42(4.55) 7(3.03) 0.86(0.37-1.98) - - + 6(0.65) 3(1.30) 2.42(0.59-9.98) + + - 95(10.3) 14(6.06) 0.72(0.39-1.33) + - + 20(2.16) 16(6.93) 3.84(1.88-7.83) - + + 2(0.22) 1(0.43) 2.38(0.21-26.83) + + + 11(1.19) 9(3.90) 3.94(1.57-9.90)
Table 4. Odds ratios for optic neuropathy in relation to duration of EMB prescription Controls (n=924) % Optic Neuropathy cases (n=231) %
Odds Ratio (95% CI)
Model 1 Model 2
Duration of prescription, months
≦3 months 436 (47.2) 88 (38.1) 1.00 1.00
> 3 months 488 (52.8) 143 (61.9) 1.38 (1.02-1.86) 1.35 (0.99-1.83)
Model 1 was adjusted for age and sex.
Table 5. Odds ratios for optic neuropathy in relation to average daily dosage of EMB prescription
Controls (n=924) %
Optic Neuropathy cases (n=231) %
Odds Ratio (95% CI)
Average daily dose, mg Model 1 Model 2
All EMB-treated Cases
< 800 439 (47.5) 115 (49.8) 1.00 1.00 800-1199 290 (31.4) 88 (38.1) 1.28 (0.93-1.76) 1.36 (0.98-1.89) ≧1200 195 (21.1) 28 (12.1) 0.68 (0.43-1.09) 0.72 (0.45-1.16)
With Renal diseases
< 800 24 (61.5) 21 (72.4) 1.00 1.00 800-1199 13 (33.3) 7 (24.1) 0.39 (0.11-1.36) 0.40 (0.11-1.40) ≧1200 2 (5.13) 1 (3.45) 0.41 (0.03-5.36) 0.37 (0.03-4.91)
Without Renal diseases
< 800 415 (46.9) 94 (46.5) 1.00 1.00 800-1199 277 (31.3) 81 (40.1) 1.44 (1.02-2.03) 1.46 (1.04-2.06)* ≧1200 193 (21.8) 27 (13.4) 0.79 (0.49-1.28) 0.78 (0.48-1.26)
Model 1 was adjusted for age and sex.
Model 2 was additionally adjusted for hypertension and renal diseases.
Average daily dose was calculated by dividing total number of milligrams prescribed by total number of days supplied during the year before the index date.