行政院國家科學委員會專題研究計畫 成果報告
補充精氨酸對頂尖跆拳道選手運動表現與 nitric oxide 的
影響
計畫類別: 個別型計畫 計畫編號: NSC92-2413-H-028-004- 執行期間: 92 年 08 月 01 日至 93 年 07 月 31 日 執行單位: 國立臺灣體育學院運動管理學系 計畫主持人: 張振崗 共同主持人: 曾泓富 計畫參與人員: 余欣嶸、卓佩佩 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 93 年 11 月 3 日
行政院國家科學委員會專題研究計畫成果報告
計畫編號:NSC-92-2413-H-028-004
執行期限:92 年 8 月 1 日至 93 年 7 月 31 日
主持人:張振崗,國立台灣體育學院運動管理學系
共同主持人:曾泓富,輔英科技大學護理管理系
計畫參與人員:余欣嶸、卓佩佩
中文摘要 研究顯示 L-精胺酸,尿素循環的中間 產物之一,可能可以促進運動表現。本研 究探討口服補充精胺酸對 5 分鐘間歇運動 期間最大功率與疲勞產生的影響,以頂尖 男性柔道選手為研究對象。運動後血漿氨 與乳酸濃度的增加幅度在精胺酸與安慰劑 組無顯著差異,與安慰劑組相比較,精胺 酸組在第 3、13、14、15 階段的功率輸出 下降比例較低,疲勞指數改變比例精胺酸 組在第 1、3 階段較安慰劑組顯著為低。本 研究顯示,口服精胺酸補充劑可減緩男性 頂尖柔道選手在 5 分鐘間歇划船器運動測 試末期的功率消退,可能有助於提升柔道 選手運動表現,但機轉可能與血漿乳酸與 氨的移除無關。 關鍵詞:精胺酸、柔道、間歇性運動、尿 素、乳酸 AbstractIt has been shown that L-arginine, an intermediate of urea cycle, could increase exercise performance. The objectives of this study are to investigate the effect of oral arginine supplementation on peak power and development of fatigue in a 5-min intermittent rowing test in elite judo athletes. The exercise-induced changes of lactate and ammonia were similar in arginine and placebo groups. The decline in power output was smaller in arginine group, compared to placebo, in the 3rd, 13th, 14th, and last stages. The change of fatigue index was smaller in the arginine group than the control at the first and 3rd stages. This study suggested that acute oral supplementation of arginine could
delay fatigue and enhance power output in an intermittent rowing test in male judo athletes. The mechanism is independent from metabolism of lactate and ammonia
Keywords: arginine, judo, intermittent exercise, ammonia, lactate
Introduction
It has been shown in several studies that L-arginine, an intermediate of urea cycle, could reduce exercise-related accumulations of lactate and ammonia in blood. Schaefer et al. suggested that 3 g L-arginine hydrochloride given intravenously resulted in significantly lower blood lactate and ammonia concentrations compared to a placebo after graded exercise to reach maximum power output on a cycle ergometer in recreationally active subjects [1]. The reduction in exercise-induced blood ammonia accumulation may be associated with the increased ureagenesis as ornithine, an intermediate of urea cycle, was significantly elevated after the supplementation. The reduction in blood lactate accumulation may be partly resulted from increased NO production as citrulline, a by-product of NO synthesis, was significantly increased after exercise.
The acute oral supplementation of arginine could also decrease exercise-induced ammonemia. Eto et al. suggested that the intake of 20 g arginine 30 min prior to the exercise at 75-80% V&O2max for 30 minutes
could diminish the elevation in blood ammonia [2].
supplementations also showed similar effects on exercise. After supplemented with arginine aspartate for 10 days, the increase of blood ammonia was significantly lower than the placebo group after exercising at 80%
V&O2max for 15 minutes [3].
The accumulations of lactate and ammonia have been shown to be involved in the development of muscular fatigue due to the increased muscular acidity [4-6]. However, the research on the ergogenic effect of arginine in trained athletes is limited. Stevens et al. suggested that acute oral supplementation of 6 g arginine monohydrochloride along with 2 g glycine and 3.2 g -ketoisocaproic acid dicalcium could delay the fatigue in concentric and eccentric exercise [7]. The role of arginine in this study could not be identified because the two other components may also contribute to the delay of fatigue.
Arginine supplementation could increase exercise capacity in various types of patients by enhancing NO production at rest and during exercise by serving as a substrate for NO synthase [8]. Regular exercise training has been shown to increase basal NO
production, resulting in endothelium-dependent vasodilation in
animal aorta [9-12] and human forearms [13]. This mechanism has been suggested to be one of the reasons responsible for the cardiovascular protective effect of regular exercise [14]. The vasodilation effect of oral arginine became significant after approximately 60 min, when mean pulmonary arterial pressure and pulmonary vascular resistance began to fall [15]. It has been shown that oral supplementation of arginine at the doses of 5.6-12.6 g/d for 6 weeks enhanced exercise capacity in patients with congestive heart failure, resulting from improved endothelial-dependent vasodilation [16]. In addition, after arginine supplementation for 1 week at 1.5 g/10 kg body weight/d, significantly increased
V&O2max in pulmonary hypertensive subjects
[15]. Short-term oral supplementation of arginine has also been shown to improve exercise capacity in patients with other cardiopulmonary diseases, such as coronary
artery disease [17], stable angina pectoris, and myocardial infarction [18, 19], at least partially through the increase of NO production and vasodilation [20]
The objectives of this study are to investigate the effect of oral arginine supplementation on peak power and development of fatigue in a 5-min intermittent rowing test in elite judo athletes. In addition, the effect of acute oral arginine supplementation on blood lactate, ammonia, and NO after the rowing test in elite judo athletes
Methods Subjects
Twelve male judo athletes will be
recruited from 台灣體育學院. All subjects
have been participated in regular judo training for at least 3 years and have competed in national or international level. All subjects must be non-smokers and non-drinkers and generally healthy.
Study design
This is a randomized, cross-over, placebo-controlled study. Each subject underwent two exercise tests, separated by a 2-week wash-out period, receiving either 5 g arginine or an empty pill (placebo) orally. All subjects were randomly selected to receive the arginine or placebo pill first. After an overnight fast, all subjects will consume the arginine or placebo pill 60 min prior to each exercise test.
Exercise test
In the 5-min intermittent rowing test, subjects put their knees on the pedals of a rowing machine (Concept II) with the seat being fixed at the appropriate position. It allowed the subjects to only use the upper body to pull the string. The test is composed of 15 continuous 20-sec stages. In each stage, the subjects were asked to perform with their greatest effort for 10 sec, then rest for 10 sec. Average power and fatigue index [(highest average power - average power of certain stage)/highest average power x 100%] were calculated for each stage.
Statistical analysis
placebo was analyzed with paried t-test. A p-value less than 0.05 is considered statistically significant.
Results
Plasma lactate and ammonia concentrations before and after a 5-min intermittent rowing test after consumption of arginine and placebo were presented in Table 1. The exercise-induced changes of lactate and ammonia were similar in arginine and placebo groups.
Figure 1 showed percentage difference between arginine and placebo in power output in each stage during a 5-min intermittent rowing test. The decline in power output was smaller in arginine group, compared to placebo, in the 3rd, 13th, 14th, and last stages.
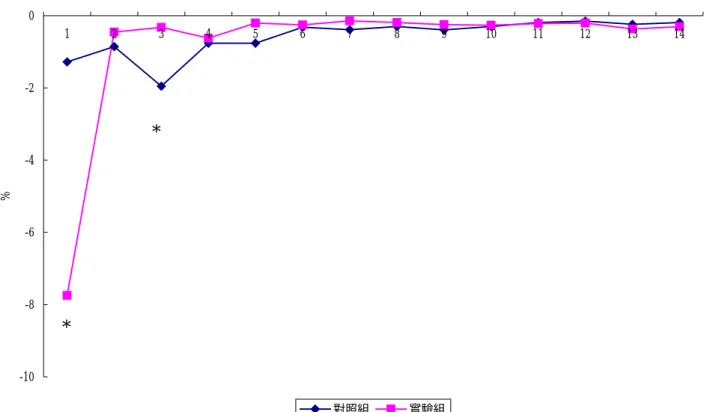
Figure 2 showed percentage difference between arginine and placebo in fatigue index in each stage during a 3-min intermittent rowing test. The change was smaller in the arginine group than the control at the first and 3rd stages.
Discussion
In this study, we showed that acute oral arginine supplementation could increase power output in the later stages of a 5-min intermittent rowing test. The mechanism is unlikely through the enhancement of urea cycle and lactate removal as ammonia and lactate concentrations were similar in arginine and placebo groups.
The intermittent rowing test was designed to mimic the real competition condition of a judo contest. During the test, the seat was fixed so that only upper body strength and endurance were measured. Our study showed that arginine supplementation could increase power output in the final 3 stages of the test. Therefore, arginine may improve judo performance, especially in the final minute of the competition.
In addition, fatigue index, the decline of power output compared to the highest stage was smaller in arginine group in the first and 3rd stage. Therefore, power output in
the initial stages could be enhanced by arginine supplementation. Muscular fatigue could be less apparent in the initial stages of the competition.
Muscular fatigue has been suggested to be related to ammonia and lactate accumulation. However, this study did not show any effect of arginine on exercise-induced ammonia and lactate elevation. The possible mechanism of performance enhancement could be mediated by nitric oxide production. Arginine is the substrate for nitric oxide synthase. NO is a potent vassal dilator. It is likely that the elevated NO production, resulted from arginine supplementation caused the vessels that supply working muscles to dilate. Thus, more blood and oxygen can be delivered to the working muscle.
In summary, this study suggested that acute oral supplementation of arginine could delay fatigue and enhance power output in an intermittent rowing test in male judo athletes. The exact mechanism responsible for the ergogenic effect warrants further investigation.
Reference
1. Schaefer A, Piquard F, Geny B, et al. L-Arginine reduces exercise-induced increase in plasma lactate and ammonia. Int J Sports Med 23: 403-407, 2002. 2. Eto B, Peres G, Le Moel G. Effects of an
ingested glutamate arginine salt on ammonemia during and after long lasting cycling. Arch Int Physiol Biochim Biophys 102: 161-2, 1994. 3. Denis C, Dormois D, Linossier MT, et al.
Effect of arginine aspartate on the exercise-induced hyperammoniemia in humans: a two periods cross-over trial. Arch Int Physiol Biochim Biophys 99: 123-7, 1991.
4. Spodaryk K, Szmatlan U, Berger L. The relationship of plasma ammonia and lactate concentrations to perceived exertion in trained and untrained women. Eur J Appl Physiol Occup Physiol 61: 309-12, 1990.
EA. Effect of muscle acidity on muscle metabolism and fatigue during intense exercise in man. J Physiol 495: 587-96, 1996.
6. Favero TG, Zable AC, Colter D, Abramson JJ. Lactate inhibits Ca(2+) -activated Ca(2+)-channel activity from skeletal muscle sarcoplasmic reticulum. J Appl Physiol 82: 447-52, 1997.
7. Stevens BR, Godfrey MD, Kaminski TW, Braith RW. High-intensity dynamic human muscle performance enhanced by a metabolic intervention. Med Sci Sports Exerc 32: 2102-8, 2000.
8. Moncada S, Higgs A. The L-arginine-nitric oxide pathway. N Eng J Med 329: 2002-12, 1993.
9. Wang J, Wolin MS, Hintze TH. Chronic
exercise enhances endothelium-mediated dilation of
epicardial coronary artery in conscious dogs. Circ Res 73: 829-38, 1993.
10. Sessa WC, Pritchard K, Seyedi N, Wang J, Hintze TH. Chronic exercise in dogs increases coronary vascular nitric oxide production and endothelial cell nitric oxide synthase gene expression. Circ Res 74: 349-53, 1994.
11. Muller JM, Myers PR, Laughlin MH. Vasodilator responses of coronary resistance arteries of exercise-trained pigs. Circulation 89: 2308-14, 1994. 12. Laughlin MH. Endothelium-mediated
control of coronary vascular tone after chronic exercise training. Med Sci Sports Exerc 27: 1135-44, 1995.
13. Lewis TV, Dart AM, Chin-Dusting JP, Kingwell BA. Exercise training increases basal nitric oxide production from the forearm in hypercholesterolemic patients. Arterioscler Thromb Vasc Biol 19:
2782-7, 1999.
14. Gielen S, Schuler G, Hambrecht R. Exercise training in coronary artery disease and coronary vasomotion. Circulation 103: E1-6, 2001.
15. Nagaya N, Uematsu M, Oya H, et al. Short-term oral administration of L-arginine improves hemodynamics and exercise capacity in patients with
precapillary pulmonary hypertension. Am J Respir Crit Care Med 163: 887-91, 2001.
16. Rector TS, Bank AJ, Mullen KA, et al.
Randomized, double-blind, placebo-controlled study of supplemental oral L-arginine in patients with heart failure. Circulation 93: 2135-41, 1996.
17. Bednarz B, Wolk R, Chamiec T, et al. Effects of oral L-arginine supplementation on exercise-induced QT dispersion and exercise tolerance in stable angina pectoris. Int J Cardiol 75: 205-10, 2000.
18. Ceremuzynski L, Chamiec T, Herbaczynska-Cedro K. Effect of supplemental oral L-arginine on exercise capacity in patients with stable angina pectoris. Am J Cardiol 80: 331-3, 1997.
19. Fujita H, Yamabe H, Yokoyama M. Effect of L-arginine administration on myocardial thallium-201 perfusion during exercise in patients with angina pectoris and normal coronary angiograms. J Nucl Cardiol 7: 97-102, 2000.
20. Cheng JW, Baldwin SN, Balwin SN. L-arginine in the management of cardiovascular diseases. Ann Pharmacother 35: 755-64, 2001.
5
Table 1. Plasma lactate and ammonia concentrations before and after a 3-min intermittent rowing test after consumption of arginine and placebo.
Lactate (mM) Ammonia (mM)
Pre Post Pre Post
Arginine 0.22±0.01 7.83±1.22 0.12±0.01 4.22±0.25 Placebo 0.21±0.01 8.01±0.95 0.13±0.01 4.10±0.31 mean±SD. -0.25 -0.2 -0.15 -0.1 -0.05 0 0.05 0.1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 % 對照組 實驗組
Figure 1. Percentage difference between arginine and placebo in power output in each stage during a 3-min intermittent rowing test.
* * *
6 -10 -8 -6 -4 -2 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 % 對照組 實驗組
Figure 1. Percentage difference between arginine and placebo in fatigue index in each stage during a 3-min intermittent rowing test.
*