Prescriptions of Traditional Chinese Medicine, Western
Medicine, and Integrated Chinese-Western Medicine for
Allergic Rhinitis under the National Health Insurance in
Taiwan
Sheng-Kang Huang a,b , Yu-Ling Ho c , Yuan-Shiun Chang a, *
a Department of Chinese Pharmaceutical Sciences and Chinese Medicine Resources,
China Medical University, Taichung 40402,, Taiwan
b Chang-Hua Hospital, Ministry of Health and Welfare. Changhua County 51341,
Taiwan
c Department of Nursing, Hung Kuang University, Taichung 43302, Taiwan.
Background: According to the study on 1996-2001 National Health Insurance Research Database (NHIRD) based on the claim data from National Health Insurance in Taiwan, respiratory diseases account for the majority of outpatient traditional Chinese medicine treatment, and allergic rhinitis accounts for the majority of respiratory diseases. Analysis on the prescription difference of traditional Chinese medicine and western medicine treatments would be helpful to clinical guide and health policy decision making.
Methods: Patients diagnosed as allergic rhinitis with diagnostic code 470~478 (ICD-9-CM) were selected as subjects from 2009-2010 NHIRD. This retrospective study used Chi-Square test to test the effects of gender and age on visit of traditional Chinese medicine, western medicine, and integrated Chinese-Western medicine treatments.
Results: A total of 45,804 patients diagnosed as allergic rhinitis with ICD-9-CM 470~478 were identified from 2009-2010 NHIRD. There were 36,874 subjects for western medicine treatment alone, 5,829 subjects for traditional Chinese medicine treatment alone, and 3,101 subjects for integrated Chinese-Western medicine treatment.
Female patients were more than male in three treatments. 0-9 years children had the highest visit frequency in western medicine and
integrated Chinese-Western medicine groups, while 10-19 years young-age rank the highest in traditional Chinese medicine group.
The Chi-square test of independence showed that the effects of gender and age on visit of three treatments were significant.
Conclusions: The prescription drugs of western medicine treatment alone were almost for relieving the symptoms of allergic rhinitis. That leads to the little difference between 2009 and 2010. The same phenomenon occurs in integrated Chinese-Western medicine. However, the prescription drugs of traditional Chinese medicine treatment vary considerably. It is implied that differential symptoms and treatments used in traditional Chinese medicine treatment have an inclination for personal therapy.
Keywords: allergic rhinitis, prescription difference, personal therapy
Introduction
Following the change of lifestyle, the global asthma population has been increased by 45% yearly. It is estimated that about three hundred million people are suffering from asthma. Allergic rhinitis is considered one of the dangerous factors of asthma, because it very often coexists with asthma in the same patient according to the findings of epidemiological research. [1] Allergic rhinitis has long been a global health problem. As previous researches showed, the incidence of respiratory allergies is about 20-30% with a global growth trend associated with the quick changes of industrial progress, modern lifestyle, and ecological environment. [2] Moreover, allergic rhinitis has the highest prevalence of all allergic respiratory diseases and affects over 12 million people (20%) of the UK population and 400 million people (5.6%) worldwide. [3] As for the incidence of allergic rhinitis in Taiwan, the prevalence is approximately 20% - 30% and increases annually. [4]
The clinical definition of allergic rhinitis is a nasal symptom induced by IgE antibody mediated inflammatory reaction by exposing to allergens. Even if allergic rhinitis is generally not a severe disease, it will interfere with patients’ quality of life and performance of work and learning. Modern medical researches have developed a considerable knowledge of allergic rhinitis and have found efficacious treatments for the disease. In addition to avoiding exposure to allergens, controlling diet and environmental, western medicine treatments include medical treatment, hyposensitization treatment, and surgical treatment. [5] As for traditional Chinese medicine treatment, differential symptoms and treatments have been proven efficacious against allergic rhinitis. In addition, previous researches show that integrated Chinese-Western
medicine treatments for allergic rhinitis are effective measures without obvious side effect. [6] Some researches even suggest that the performance of integrated Chinese-Western medicine treatments is better than western medicine treatments. [7,8] According to the study on 1996-2001 National Health Insurance Research Database (NHIRD), which is based on the claim data of National Health Insurance (NHI) in Taiwan, respiratory diseases account for the majority of outpatient traditional Chinese medicine treatment. [9]
Taiwanese have always believed traditional Chinese medicines have slower effects but more safety, while western medicines have quicker effects but more side effects. [10,11,12] Accordingly, patients with chronic or recurrent diseases frequently seek not only western medicine treatment but also traditional Chinese medicine treatment or integrated Chinese-Western medicine treatments. The dual-track treatment has become prevalent ever since Taiwan’s NHI included reimbursement of traditional Chinese medicines in 1995. Taiwan’s NHI initiated by central government in 1995 is compulsory for the whole population to have an equal chance to join and to meet the demand of health. As a preceding research on the habit of medicine consumption of outpatients of medical centers in Taiwan showed, 72.7% patients accepted both traditional Chinese medicine treatments and western medicine treatments. [13] However, the study conducted research by questionnaire survey and did not evaluate the influence factors and difference of medications prescriptions of traditional Chinese medicine treatments and western medicine treatments. Furthermore, many researches have conducted epidemiology study or utilization of traditional Chinese medicine by exploring NHIRD in recent years. [9,14-15] Unfortunately, these study did not simultaneously compare traditional Chinese medicine treatments alone, western medicine treatments alone, and integrated Chinese-Western medicine treatments. This study would like to explore the three treatments for allergic rhinitis to know if there exist specific treatment guidelines for prescribed medications or inclination for personal therapy.
Methods
On the basis of the claim data from Taiwan’s NHI, the National Health Research Institutes (NHRI) constructed NHIRD in 1998 to support academic and non-profit organizations to undertake medical researches. This study used allergic rhinitis patients of 2009-2010 NHIRD as research sample. We classified allergic rhinitis patients into three groups: traditional Chinese medicine treatment alone, western medicine treatment alone, and integrated Chinese-Western medicine treatment. This study analyzed the distinctions of demographic characteristic and medical use patterns among the three groups. Because
Taiwan’s National Health Insurance only reimburses extract Chinese medicines, prescription patterns analysis of this study excluded raw medicinal substances and other herb medicines.
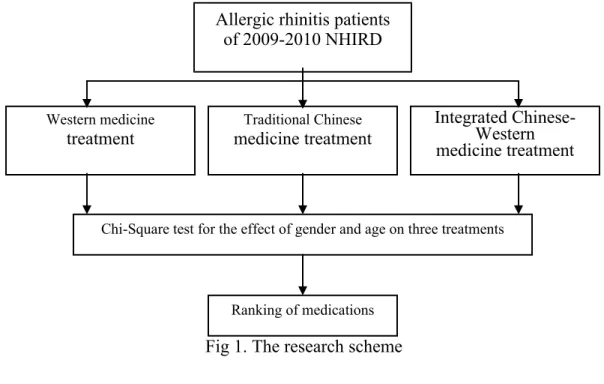
Patients diagnosed as allergic rhinitis with diagnostic code 470~478 (ICD-9-CM) were selected as subjects. The statistical analysis software SAS 9.13 was employed for data analysis. Chi-Square test was utilized to test the effects of gender and age on visit of traditional Chinese medicine treatment, western medicine treatment, and integrated Chinese-Western medicine treatment. Finally, medications prescribed by the three treatments were ranked and compared. The research scheme of this study is shown as Fig 1.
Fig 1. The research scheme
Results and Discussion
A total of 45,804 patients diagnosed as allergic rhinitis with ICD-9-CM 470~478 were selected from 2009-2010 NHIRD. There were 36,874 subjects for western medicine treatment alone, 5,829 subjects for traditional Chinese medicine treatment alone, and 3,101 subjects for integrated Chinese-Western medicine treatment.
The average age of western medicine treatment group was 32.79 ± 21.77, with 17,205 male (46.66%) and 19,669 female (53.34%). Among traditional Chinese medicine group, the average age was 30.15 ± 18.55, with 2,589 male (44.42%) and 3,240 female (55.58%). As for integrated Chinese-Western medicine group, the average age was 26.90 ± 19.57, with 1,477 male (47.63%) and 1,624 female (52.37%). A chi-square test
Western medicine treatment Integrated Chinese-Western medicine treatment Traditional Chinese medicine treatment
Chi-Square test for the effect of gender and age on three treatments
Ranking of medications
Allergic rhinitis patients of 2009-2010 NHIRD
of independence was performed to examine the effect of gender on treatments. The relation between these two variables was significant (p = 0.0024) shown as Table 1.
Table 1. Distribution and chi-square test of allergic rhinitis patients treated by western medicines, traditional Chinese medicines, and integrated Chinese- Western medicines on gender in 2009-2010 Western medicine (N =36,874) Traditional Chinese medicine (N =5,829) Integrated Chinese-Western medicine (N =3,101) Total (N=45,804) χ2
Gender Count % Count % Count % Count %
12.0769 p= 0.0024 Male 17,205 46.66 2,589 44.42 1,477 47.63 21,271 46.44
Female 19,669 53.34 3,240 55.58 1,624 52.37 24,533 53.56
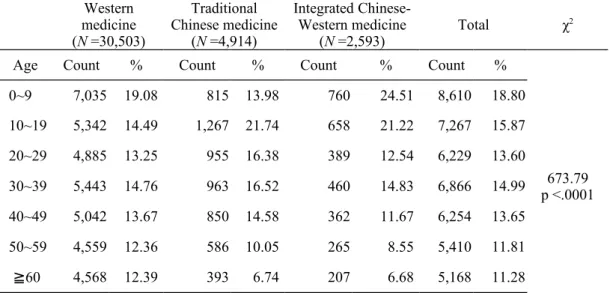
The peak age of allergic rhinitis patients treated by western medicines was 0-9 years of age (19.08 %), followed by 10-19 years of age (14.49 %). The peak age of allergic rhinitis patients treated by traditional Chinese medicines was 10-19 years of age (21.74 %), followed by 30–39 years of age (16.52%). The peak age of allergic rhinitis patients treated by integrated Chinese-Western medicines was 0-9 years of age (24.51 %), followed by 10-19 years of age (21.22 %). A chi-square test of independence was performed to examine the effect of age on treatments. The relation between these two variables was significant (P<0.0001), shown as Table 2.
Table 2. Distribution and chi-square test of allergic rhinitis patients treated by western medicines, traditional Chinese medicines, and integrated Chinese-Western medicines on age in 2009-2010 Western medicine (N =30,503) Traditional Chinese medicine (N =4,914) Integrated Chinese-Western medicine (N =2,593) Total χ 2
Age Count % Count % Count % Count %
0~9 7,035 19.08 815 13.98 760 24.51 8,610 18.80 673.79 p <.0001 10~19 5,342 14.49 1,267 21.74 658 21.22 7,267 15.87 20~29 4,885 13.25 955 16.38 389 12.54 6,229 13.60 30~39 5,443 14.76 963 16.52 460 14.83 6,866 14.99 40~49 5,042 13.67 850 14.58 362 11.67 6,254 13.65 50~59 4,559 12.36 586 10.05 265 8.55 5,410 11.81 ≧60 4,568 12.39 393 6.74 207 6.68 5,168 11.28
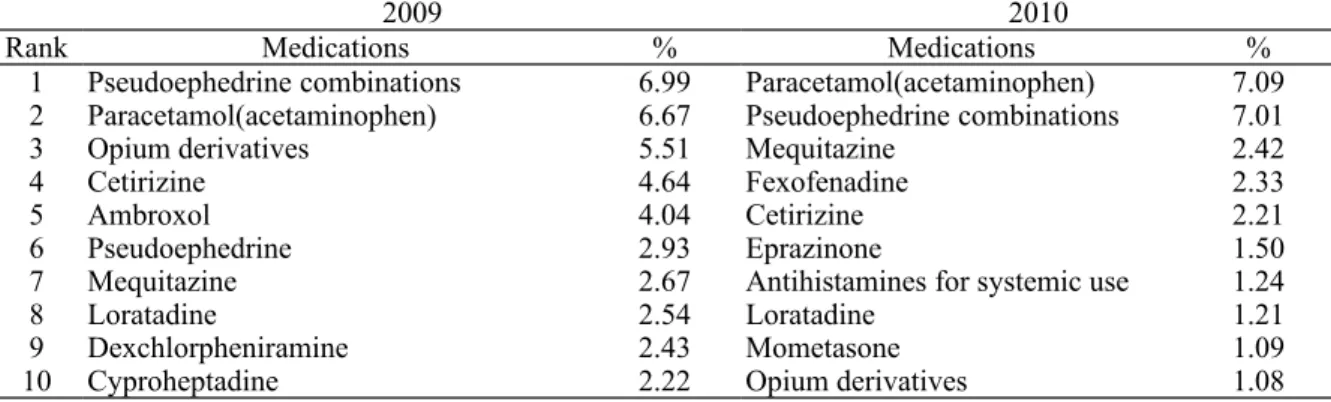
As Table 3 showed, the top 10 prescription drugs of western medicine treatment in 2009 and 2010 were almost decongestant agents (pseudoephedrine) including antihistamine, paracetamol
(acetaminophen), and medications for suppressing cough and dissolving phlegm to relieve the symptoms of allergic rhinitis. Ambroxol, pseudoephedrine, dexchlorpheniramine, and cyproheptadine ranked as 5th, 6th, 9th, and 10th in 2009 dropped out of the top 10 of 2010 rankings. Fexofenadine, eprazinone, antihistamines for systemic use, and mometasone ranked as 4th, 6th, 7th, and 9th in 2010 from outside the top 10 in 2009. Opium derivatives fell to 10th place in 2010 from 3rd place in 2009.
Table 3. The top 10 medications of allergic rhinitis treated by western medicines in 2009-2010
2009 2010
Rank Medications % Medications %
1 Pseudoephedrine combinations 6.99 Paracetamol(acetaminophen) 7.09 2 Paracetamol(acetaminophen) 6.67 Pseudoephedrine combinations 7.01
3 Opium derivatives 5.51 Mequitazine 2.42
4 Cetirizine 4.64 Fexofenadine 2.33
5 Ambroxol 4.04 Cetirizine 2.21
6 Pseudoephedrine 2.93 Eprazinone 1.50
7 Mequitazine 2.67 Antihistamines for systemic use 1.24
8 Loratadine 2.54 Loratadine 1.21
9 Dexchlorpheniramine 2.43 Mometasone 1.09
10 Cyproheptadine 2.22 Opium derivatives 1.08
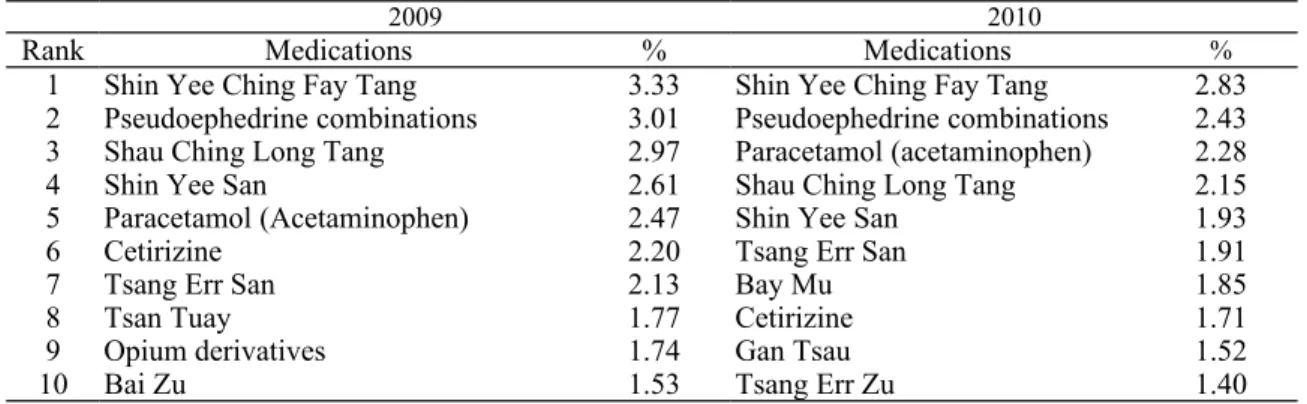
Among the top 10 prescription medicines of traditional Chinese treatment, Shin Yee Ching Fay Tang ranked first (and Bay Mu ranked 10th) in 2009 had surprisingly dropped out of the top 10 of 2010 rankings. Besides, Tsan Tuay and Gan Tsau ranked as 5th and 10th in 2010 from outside the top 10 in 2009 (table 4). It is inferred that because differential symptoms and treatments were used according to traditional Chinese medicine theory, it makes all the difference in medications used.
Table 4. The top 10 medications of allergic rhinitis treated by traditional Chinese medicines in 2009-2010
2009 2010
Rank Medications % Medications %
1 Shin Yee Ching Fay Tang 5.19 Shin Yee San 4.76 2 Shau Ching Long Tang 4.61 Shau Ching Long Tang 3.97 3 Shin Yee San 4.22 Tsang Err San 3.07
4 Tsang Err San 3.62 Bai Zu 2.59
5 Jel Girng 2.63 Tsan Tuay 2.47
6 Gir Girn Tang 2.50 Gir Girn Tang 2.39 7 Yu Shing Tsao 2.38 Tsang Err Zu 2.33
8 Bai Zu 2.31 Yu Shing Tsao 2.17
9 Tsang Err Zu 2.17 Jel Girng 2.02
10 Bay Mu 2.08 Gan Tsau 1.94
As for integrated Chinese- western medicine treatment, Tsan Tuay, opium derivatives, and Bai Zu ranked 8th, 9th, and 10th respectively in 2009 were replaced by Bay Mu (7th), Gan Tsau (9th), and Tsang Err Zu (10th) in 2010 (Table 5).
In recent years, various researches proved that taking Chinese medicines and western medicines at the same time would be at the risk of severe drug interactions. [16] Although many mechanisms of drug-drug interaction between Chinese medicines and western medicines are not clear enough, most of these come from the change of pharmacodynamics (absorption, distribution, and metabolism of drug) to enhance or decrease effects by combing use of Chinese medicines and western medicines. Among integrated Chinese-western medicine, the ranks of medications in 2009 and 2010 have little difference. However, combined use of pseudoephedrine and Mar Huang or Shau Ching Long Tang (containing components of Mar Huang) in Zong Yee Fang Jee will enhance nervous system excitement, accelerated heartbeat, sudden hypertension, and insomnia due to the drug-drug interactions. [17]
Table 5. The top 10 medications of allergic rhinitis treated by integrated Chinese- western medicines 2009-2010
2009 2010
Rank Medications % Medications %
1 Shin Yee Ching Fay Tang 3.33 Shin Yee Ching Fay Tang 2.83 2 Pseudoephedrine combinations 3.01 Pseudoephedrine combinations 2.43 3 Shau Ching Long Tang 2.97 Paracetamol (acetaminophen) 2.28
4 Shin Yee San 2.61 Shau Ching Long Tang 2.15
5 Paracetamol (Acetaminophen) 2.47 Shin Yee San 1.93
6 Cetirizine 2.20 Tsang Err San 1.91
7 Tsang Err San 2.13 Bay Mu 1.85
8 Tsan Tuay 1.77 Cetirizine 1.71
9 Opium derivatives 1.74 Gan Tsau 1.52
10 Bai Zu 1.53 Tsang Err Zu 1.40
Conclusions
While previous research showed that male have a higher probability incurred allergic rhinitis than female [18]. This research on the 2009-2010NHIRD showed that female patients were more than male no matter treated with traditional Chinese medicines (F:M=1.25:1), western medicines (F:M=1.14:1), or integrated Chinese-Western medicines (F:M=1.09:1). Furthermore, 0-9 years old children had the highest visit frequency in western medicine and integrated Chinese-Western medicine groups, while 10-19 years young-ages ranked the highest in traditional Chinese medicine group. It is suggested that younger patients accounted for a greater proportion in allergic rhinitis.
The prescription drugs of western medicine treatment alone were almost for relieving the symptoms of allergic rhinitis. That leads to the little difference between 2009 and 2010. The same phenomenon occurred in integrated Chinese-Western medicine. Except opium derivatives, thee of the four western medicines in 2009 top 10 list, pseudoephedrine combinations, paracetamol (acetaminophen), and cetirizine, were
remained in 2010 top 10 list.
However, the prescription drugs of traditional Chinese medicine treatment varied considerably. Especially, Shin, Yee Ching Fay Tang ranked first in 2009 had surprisingly dropped out of the top 10 of 2010 rankings. It is implied that because differential symptoms and treatments were used according to traditional Chinese medicine theory, it makes all the difference in medications used. That means the traditional Chinese medicine treatment has an inclination for personal therapy.
Reference
1. Matthew M., Denise F., Shaun H., Richard B. Developed for the global initiative for asthma. Global burden of Asthma 2003;1-22 2. Bezerra GF, de Almeida FC, Neto da Silva MA, Nascimento AC,
Meireles Guerra RN, Viana GM, Muniz Filho WE, Costa Mdo R, Zaror L, Brandão Nascimento Mdo D. Respiratory allergy to airborne fungi in São Luís--MA: clinical aspects and levels of IgE in a structured asthma program. J Asthma. 2014 Dec 9;51(10):1028-34. 3. Horizon Scanning Centre. House dust mite allergen immunotherapy
tablet (Mitizax) for house dust mite allergy-induced rhinitis and conjunctivitis – third line. 2013 November.
4. Yang, S.H., Chen, H.Y. Phase 3 Study of Qi-tonifying Chinese Herbal Products for Treatment of Allergic Rhinitis, ClinicalTrials.gov identifier: NCT01631032, July 2012.
5. Lee K.L. Immunology and allergy. Otolaryngol Clin North Am. 1985;18: 625-863.
6. Chen FP, Chen TJ, Kung YY et al. Use frequency of traditional Chinese Medicine in Taiwan. BMC Health Serv Res. 2007;7:26. 7. Xue CC, Li CG, Hügel HM et al. Does acupuncture or Chinese
herbal medicine have a role in the treatment of allergic rhinitis? Curr Opin Allergy Clin Immunol. 2006 Jun; 6(3):175-9.
8. Guo H, Liu MP. Mechanism of traditional Chinese medicine in the treatment of allergic rhinitis. Chin Med J (Engl). 2013 Feb;126(4):756-60.
9. Use frequency of traditional Chinese Medicine in Taiwan. BMC Health Serv Res. 2007;7:26.
10. Chen CY, Chang SK, Chi C, Chen SC, Lee JL, Lai JS. The factors which influence people in the utilization of Chinese medicine. Chin Med Coll J. 1999;8:77–88. (in Chinese).
11. Kang JT, Lee KF, Chen CF, Chou P. Factors related to the choice between traditional Chinese medicine and modern western medicine. J Formos Med Assoc. 1994;93:s49–55.
12. Long L, Huntley A, Ernst E. Which complementary and alternative therapies benefit which conditions? A survey of the opinions of 223
professional organizations. Complement Ther Med. 2001;9:178–185. doi: 10.1054/ctim.2001.0453.
13. Chen YC, Chen FP, Chen TJ, Chou LF, Hwang SJ. Patterns of traditional Chinese medicine use in patients with inflammatory bowel disease: a population study in Taiwan. Hepatogastroenterology. 2008;55(82-83):467-70.
14. Chen FP, Kung YY, Chen YC, Jong MS, Chen TJ, Chen FJ, Hwang
SJ. Frequency and pattern of Chinese herbal medicine prescriptions
for chronic hepatitis in Taiwan. J Ethnopharmacol.
2008;117(1):84-91.
15. Lai HY, Chen YC, Chen TJ, Chou LF, Chen LK, Hwang SJ. Intra-articular hyaluronic acid for treatment of osteoarthritis: a nationwide study among the older population of Taiwan. BMC Health Serv Res. 2008;28:8-24
16. Fugh-Berman A. Herb–drug interaction, Lancet 2000; 355:134–138. 17. Muittari A, Mattila MJ. Objective and subjective assessment of
ephedrine combinations in asthmatic outpatients. Ann Clin Res. 1979 Jun;11(3):87-9.
18. deShazo RD, Kemp SF. Allergic rhinitis: Clinical manifestations, epidemiology, and diagnosis. UP TO DATE. 2013/01/30.