國立臺灣大學電機資訊學院生醫電子與資訊學研究所 碩士論文
Graduate Institute of Biomedical Electronics and Bioinformatics College of Electrical Engineering and Computer Science
National Taiwan University Master Thesis
慢性疾病照護作業流程之個案管理資訊系統建置與評估 Development and Evaluation of a Workflow-based Chronic
Disease Case Management Information System
王逸帆 Yi-Van Wang
指導教授:賴飛羆 博士 Advisor: Feipei Lai, Ph.D.
中華民國 101 年 1 月
January 2012
誌謝
來台大兩年半,說長不長,說短…將近一千個日子就這樣過了。遙想當初剛 進入研究所,還只是個剛從大學畢業連程式是什麼都一知半解的笨蛋。很幸運的 是我進入了 賴飛羆老師的實驗室。老師常常帶給我很多創新的想法,同時也提供 我們在研究上最大限度的支持,在研究的過程中不斷地讓我學習到不只是學術上 的事情,更學到待人處事的道理。
老師,謝謝您對學生一直以來不厭其煩的細心指導,謝謝!
謝謝俐瑾學姐,雖然我們時常有意見上的分岐,但是你每次給我的意見都字 字珠璣,讓我在學習如何作研究上獲益良多,謝謝。
謝謝家平學長,讓我學會很多研究以外的事情,增加了不少社會歷練,謝謝。
謝謝浩準、麒文以及煌仁學弟,有你們這些資工強者能夠讓我一直重複地問 笨問題,除了十分的感謝,還是感謝。
感謝鈺昇、景崴、亞霖,緯志學弟以及所有實驗室的成員,在最後這一段當 學生的日子裡,能和你們當同學,是我莫大的幸運。
謝謝我在社團的朋友們。來台北能認識你們,真好。
最後,要謝謝我的父母及妹妹一直以來的支持,謝謝。
中文摘要
所謂慢性病,是指會長期影響身心健康,而且難以根治的疾病。然而慢性病 是可以被控制的,藉由良好的飲食、規律的運動以及持續的自我管理就夠穩定病 情。至於要如何持續的控管就要靠個案管理的協助。個案管理是一種共同合作的 過程,在醫療健康方面,藉由不斷的預估、計畫、促進、協調、評估等步驟,以 及合作關係,讓病人的健康狀況維持穩定的控制。然而隨著資訊系統的發展,個 案管理的工作流程也會需要資訊系統的輔助。以臺大醫院的糖尿病及愛滋病的照 護為例子,在這兩種慢性病的個案管理上,我們發現了有許多工作流程上所必須 處理的部分,都能夠靠資訊系統來協助並得到解決。隨著系統的完成及上線,我 們想知道個案管理資訊系統到底解決了多少問題以及效益的程度,使用者滿意度 以及接受度等等。因此本篇論文將會進行以系統評估的為主,系統發展為輔的研 究。
關鍵字:系統評估、個案管理、資訊系統、疾病管理
ABSTRACT
The chronic diseases are not only affecting physical and mental health, but also difficult to cure. However, the chronic can be controlled to stable by including indicated appropriate food intake, regular exercise habit and self-monitoring. And, how to control continually can be done by assistance from case management. Case management is a kind of collaborative process. In health care, through ongoing assessment, planning, facilitation, coordination, and evaluation and cooperation with patients whose health can be maintained in stability. With the development of information systems, the workflow of case managements can be improved. Taking the care of diabetes and HIV in National Taiwan University Hospital as an example, we found parts of workflow were handled manually which could be resolved by assistance from information systems. After the completion and online of the care management information system, we know how many problems can be resolved as well as the efficiency scale, user satisfaction and system acceptability can be evaluated; therefore, this research was carried out to do system evaluation and system development is not our major focus.
Keywords: System evaluation, case management, information systems, disease management
CONTENTS
口試委員會審定書 ... # 誌謝 ... I 中文摘要 ... II ABSTRACT ... III CONTENTS ... IV LIST OF FIGURES ... VI LIST OF TABLES ... VII
CHAPTER 1 INTRODUCTION ... 1
1.1 FOREWORD ... 1
1.2 MOTIVATION AND OBJECTIVE ... 3
1.3 THESIS ORGANIZATION ... 3
CHAPTER 2 BACKGROUND AND RELATED WORK ... 5
2.1 WHAT IS CASE MANAGEMENT? ... 5
2.2 CASE MANAGEMENT IN CHRONIC ... 8
2.3 INFORMATION SYSTEM REQUIREMENT FOR CASE MANAGEMENT ... 9
2.3.1 HIV/AIDS CASE MANAGEMENT ... 9
2.3.2 DIABETES MELLITUS CASE MANAGEMENT ... 10
CHAPTER 3 SYSTEM DEVELOPMENT ... 15
3.1 MVC ARCHITECTURE ... 15
3.2 SYSTEM ARCHITECTURE ... 18
3.3 SYSTEM STATUS IN PRESENT ... 21
CHAPTER 4 METHODOLOGY ... 24
4.1 SYSTEM EVALUATION CONCEPT ... 24
4.2 SYSTEM EVALUATION METHODOLOGY ... 25
4.3 EVALUATION ITEMS ... 28
CHAPTER 5 RESULT AND DISCUSSION ... 31
5.1 RESULT ... 31
5.1.1 SYSTEM SUPPORT IN CASE MANAGEMENT ... 31
5.1.2 USER SATISFACTION AND SYSTEM ACCEPTABLE ... 33
5.2 DISCUSSION ... 37
CHAPTER 6 CONCLUSION AND FUTURE WORK ... 39
6.1 CONCLUSION ... 39
6.2 FUTURE WORK ... 39
REFERENCE ... 41
APPENDIX ... 45
LIST OF FIGURES
Figure 2.1 Case manager’s work-flow in case management. ... 7
Figure 2.2 The HIV case management work-flow data and data transfer direction. ... 10
Figure 2.3 The diabetes case management work-flow data and data transfer direction.12 Figure 3.1 MVC architecture ... 16
Figure 3.2 The system architecture and data flow. ... 19
Figure 3.3 HIV care information system architecture ... 20
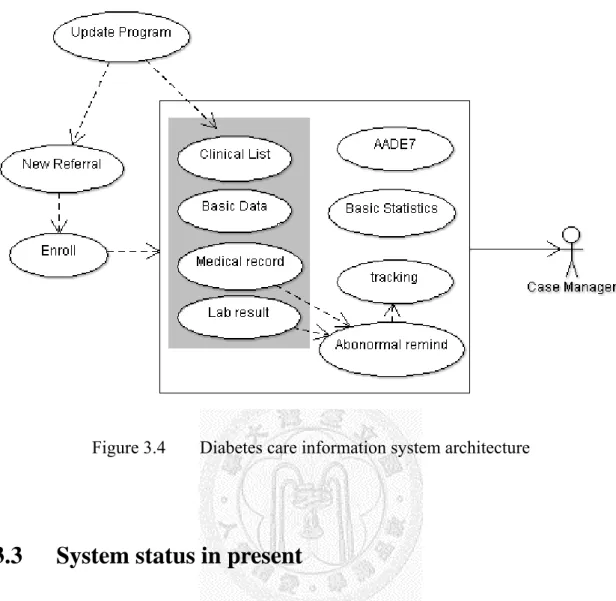
Figure 3.4 Diabetes care information system architecture ... 21
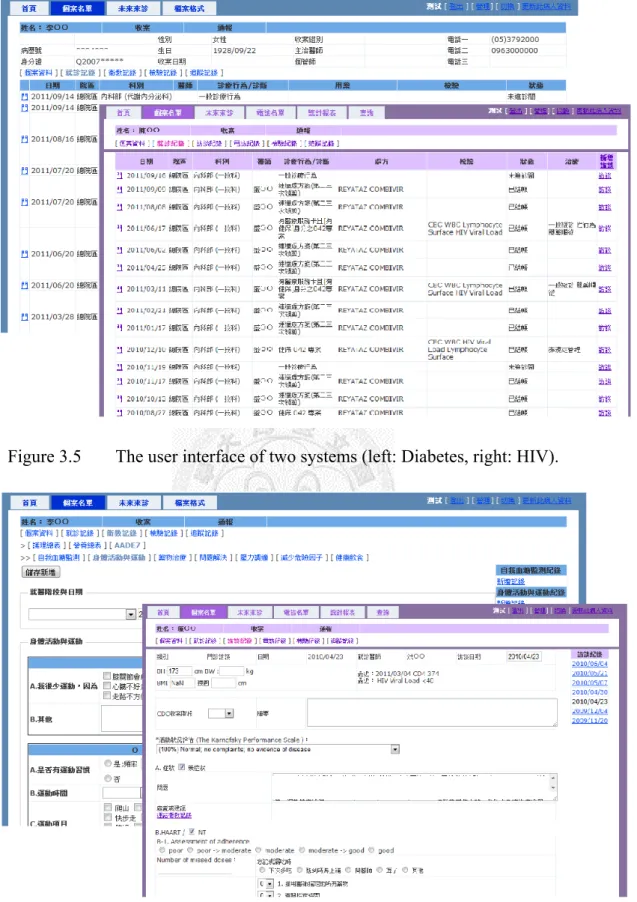
Figure 3.5 The user interface of two systems (left: Diabetes, right: HIV)... 23
Figure 3.6 The interview of HIV system (right) and AADE7 health education table of Diabetes system (left). ... 23
LIST OF TABLES
Table 1 HIV and Diabetes case management work content. ... 13
Table 2 Timeline in development of two systems [6] ... 22
Table 3 The updating program schedule. ... 22
Table 4 The general ways of collection original resource [24]. ... 27
Table 5 Summary to three questionnaire evaluated items. ... 30
Table 6 The list workflow items support by system. ... 32
Table 7 The basic data of case managers. ... 34
Table 8 The user requirement of system. (Cronbach's α value is 0.833) ... 35
Table 9 The user satisfaction of system. (Cronbach's α value is 0.94) ... 36
Table 10 The user acceptability of system. (Cronbach's α value is 0.908) ... 37
Chapter 1 Introduction
1.1 Foreword
Chronic diseases, which are unable to self-recover, must be controlled by some methods. In Taiwan, along with the improvement of public health and medical service, people’s life has been extended. But at the same time, chronic diseases threatened people’s life by complications like neuropathy, cardiovascular disease and kidney disease. For example, the statistics of the causes of death announced by the Department of Health, Taiwan in year 2010, showed that besides the accident death, the top ten were all related with chronic diseases [1]. Actually, chronic disease statuses can be controlled by some ways, including indicated appropriate food intake, regular exercise habit and self-monitoring. However, if a patient just sees his doctor regularly to maintain the health condition and doesn’t have a good self-management, the effect is limited because chronic diseases require continually trace to keep stable. How to control the patient’s health condition is the key point of the health care workers including physicians and nurses, patients’ families and patients themselves.
Case managements in a disease management model can coordinate resources to elevate cost-effectiveness and quality, and improve in management process [2]. Many studies indicate the case managements not only care effectively with improved
outcomes of disease management, patient education and self-care also resulted in better quality of life [3], which also reduce the patient’s readmission times and cost [4].
In order to maintain patient’s quality of life, National Taiwan University Hospital (NTUH) provides the case managements and consultation services for the patients of diabetes mellitus and human immunodeficiency virus (HIV or acquired immunodeficiency syndrome, AIDS). The Diabetes Health Education Center of NTUH provided diabetes related managements and special nurses (case managers) to handle HIV care.
When serving the two diseases case management routine work, we figure out some problems in their work-flow. For example, first, after case managers recorded the health education interview work in paper-based medical record, they had to use addition time to key in the record to the Hospital Information System (HIS). Second, when different case managers wrote the same medical record that could lead to inconsistency. And third, case managers must keep track of a lot of patients’ situation continually at the same time.
While the amount of data increases with the number of patients, some repeating extra manpower work such as preparing paper-based medical record and filing record to National Health Insurance are very time-consuming. However, the above-mentioned problems can be resolved by an information system.
1.2 Motivation and Objective
As mentioned in section 1.1, we could develop a new information system that is able to help the original NTUH HIS and the case managers’ common daily workflow, including reducing the time in inputting data to computer, increasing the consistence of the interview record written by different case managers and help case managers decrease the amount of repeating work and the errors [5].
As previous study, we build a new model architecture for the information system [6], however, the system usability of our users (case managers) is unknown. In this study we will focus on the evaluation of improved work-flow supported and user satisfaction, so, after development of the information system, we would know the system usability for case managers such as the routine daily work, the support provided to the work-flow, and the user’s satisfaction to our system by questionnaire.
1.3 Thesis Organization
The rest of this thesis is divided into four chapters as follows. Chapter 2 provides introductions to case managements in disease management, and reviews the cases for diabetes and HIV related requirement as well. Chapter 3 covers the system development process, including program architecture, supported functions and system in present. Chapter 4 indicates the system evaluation method, including the work-flow
support evaluation and user satisfaction. Chapter 5 presents the current system status, the result of the evaluation by users; satisfaction and the functionality of our system.
Finally, a conclusion and future work are in the last chapter.
Chapter 2 Background and Related Work
2.1 What is Case Management?
The concept of case management came from early 1900s and original from integration of the community public health nursing and social work services [7]. After long-term development and evolvement, case management has been changed to a kind of service measurement for patients that need long-term care and assistance [8].
Traditionally, the object of case management systems is to serve patients that need long term care, especially those serious psychological barriers patients, chronic disease patients, old people, long-term abused children and patients with functional developmental disabilities. For these groups, each of which has different development of history in case management. The definition of case management is still very different until now. According to Orwin et al., they consider the case management is when a case manager contacts and interacts with the case routinely, giving continually care to patients and providing long-term and integrated service [9]. Case management is considered an interdisciplinary and vertical integration work, because case managers must provide different forms of service simultaneously at the same time and ensure the service content they provide conform to case’s different requirements.
According to the American Case Management Association (ACMA), the definition
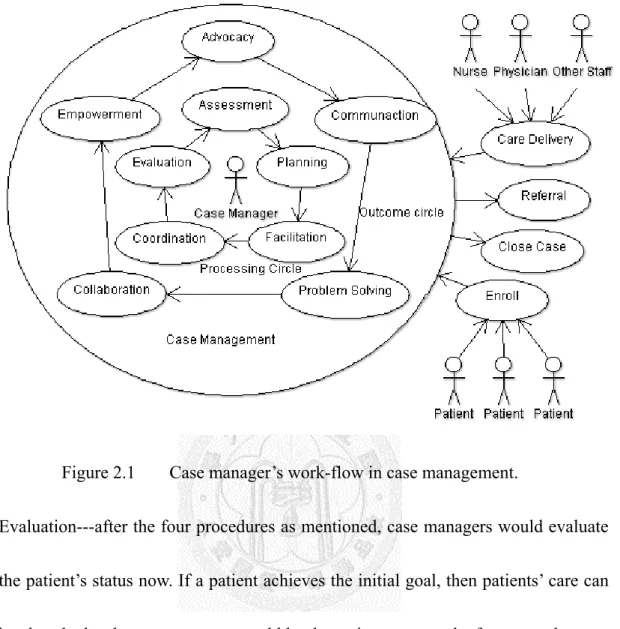
of health/hospital-based case management is “a collaborative process of assessment, planning, facilitation, care coordination, evaluation, and advocacy for options and services to meet an individual’s and family’s comprehensive health needs through communication and available resources to promote quality cost-effective outcomes [10].” Figure 2.1 shows case manager’s work-flow and roles. In the circle inside, case manager could serve the roles of:
1. Assessment---collecting and assessing patient’s information, confirming the cause of patient’s problem that need to be solved and why causing this problem, any methods could solve this problem and the obstruction may be encountered.
2. Planning---after assessment process, case managers could use the collecting resources to assist patients solving the problem in actual activity. Planning form must include four procedures: goal of establishing, ordering priority, selecting method that can achieve goal and certain assessment time.
3. Facilitation---Case managers must maintain patient’s situation in planning, correcting the plan through patient’s situation.
4. Coordination---Case managers could coordinate multiple aspects of care to ensure the patient’s progress. Otherwise, case managers should be a coordinator between the patient and other resources.
Figure 2.1 Case manager’s work-flow in case management.
5. Evaluation---after the four procedures as mentioned, case managers would evaluate the patient’s status now. If a patient achieves the initial goal, then patients’ care can be closed; else the case manager would let the patient re-enter the four procedures.
The action in the outcome circle represents the outcome achieved; for example, advocating plan and communication with patients, facilitating patients to solve problem, collaborating with patients and, the end goal, evaluating patients whether got empowerment.
2.2 Case Management in Chronic
Many studies indicated the case management model in chronic care has better effectiveness. About the health service in Somalia, they provide malaria case management that improving the health sector in availability of drugs and diagnostic kit, scaling up malaria control [11]. For diabetes mellitus patients, we evaluate the result of 2 groups; case management and non-case management, after long-term follow-up, case management group has better Glycated hemoglobin (A1C) and Low density lipoprotein-cholesterol (LDL-C) improvement than the non-group [12]. In HIV/AIDS, a brief case management is very effective using resource that can be offered to HIV-infected clients soon after their HIV diagnosis for the improvement in viral load [13]. Case managements also improve adherence for HIV-positive patients to achieve established goals and referrals [14]. Overall, case management is positive-direction, cost-efficient and decreasing patient’s hospitalized length/days [15].
However, with pushing toward electronic health records (EHR), chronic disease case management also needs assistance from information system [16]. There are several researches about supporting by information system. For patients with poorly controlled diabetes, using the information system can have better result in A1C than the non-use group [17]. An ambulatory care for HIV-infected patient was managed by an electronic health system in Kenya, the CD4 (cluster of differentiation 4) and VL (Viral Load) are
more stable in use-group then the non-use [18]. For the work-flow related assistance, using an information system to help chronic case management can get better outcome, such as decreasing error rate in medical record or out of reach [19].
In NTUH, case managements chronic disease care for HIV, diabetes and heart failure has been in progress for many years. However the support from NTUH HIS to case management related functions is not enough. So we first attempted to design an information system for HIV and Diabetes care that can help case managers in daily work.
2.3 Information System Requirement for case management
2.3.1 HIV/AIDS Case Management
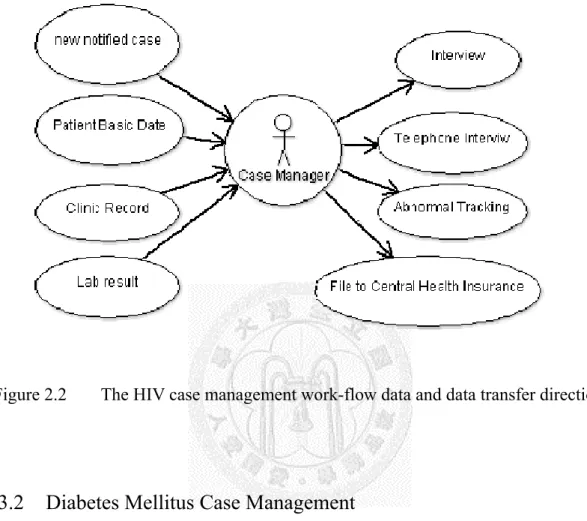
Compared to other chronic diseases, HIV/AIDS belongs to mandatory reporting communicable disease. The enrolled must be notified to Centers for Disease Control, Taiwan (CDC), and because HIV is a sensitive disease, maintaining HIV-infected patient’s privacy is especially important. Figure 2.2 shows what the information case managers should handle. In generally, a HIV case manager would track every patient with related information when they come to clinic, such as laboratory results, which include CD4 and viral load, interview in last clinic to compare patient’s status and telephone interview to grasp patient’s latest situation. Therefore, the system must
provide case managers an interface that can immediately support the information in the left-half of Figure 2.2 side and reduce the time to enter the right-half side information.
Figure 2.2 The HIV case management work-flow data and data transfer direction.
2.3.2 Diabetes Mellitus Case Management
Diabetes is classified as a typical chronic disease, in addition to general health evaluation, and the food intake should also be recorded. The American Association of Diabetes Educators (AADE) was advocating actively the concept of AADE7TM to change self-care behaviors in patients. AADE7TM includes the seven evaluation items [20]:
1. Healthy eating---By making appropriate food intakes to control patients weight and achieve optimal blood glucose levels.
2. Being active--- With appropriate levels of exercise, those at risk for type 2 diabetes can not only reduce risk and improve glycemic control, but also help improve body mass index (BMI), enhance weight loss, help control lipids and blood pressure and reduce stress.
3. Monitoring---Daily self-monitoring of blood glucose provides people with diabetes the information they need to assess how food, physical activity and medications affect their blood glucose levels.
4. Taking medication---Case managers can demonstrate how to inject insulin or explain how diabetes pills work and when to take them. Effective drug therapy in combination with healthy lifestyle choices can lower blood glucose levels, reduce the risk for diabetes complications and produce other clinical benefits.
5. Problem solving---A person with diabetes must keep their problem-solving skills sharp because on any given day, a high or low blood glucose episode or a sick day will require them to make rapid, informed decisions about food, activity and medications.
6. Reducing risks---Effective risk reduction behaviors such as smoking cessation, and regular eye, foot and dental examinations reduce diabetes complications and maximize health and quality of life. An important part of self-care is learning to understand, seek and regularly obtain an array of preventive services.
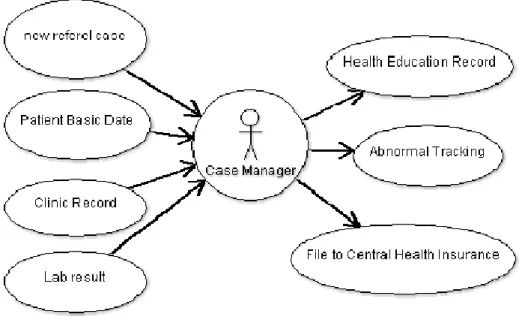
Figure 2.3 The diabetes case management work-flow data and data transfer direction.
7. Healthy coping---Health status and quality of life are affected by psychological and social factors. Psychological distress directly affects health and indirectly influences a person’s motivation to keep their diabetes in control. When motivation is dampened, the commitments required for effective self-care are difficult to maintain.
When barriers seem insurmountable, good intentions alone cannot sustain the behavior. Coping becomes difficult and a person’s ability to self-manage their diabetes deteriorates.
AADE7 is the best evaluation direction for diabetes, and which also applies to other chronic diseases [21]. Figure 2.3 shows the Diabetes Case manager’s work-flow.
Similar to HIV work-flow, case managers must know the patient’s latest information,
and key in the health education record (just AADE7) [22] (Subjective, Objective, Assessment, Plan and additional Evaluation, SOAPE record method) format. So the information system must be able to support the work.
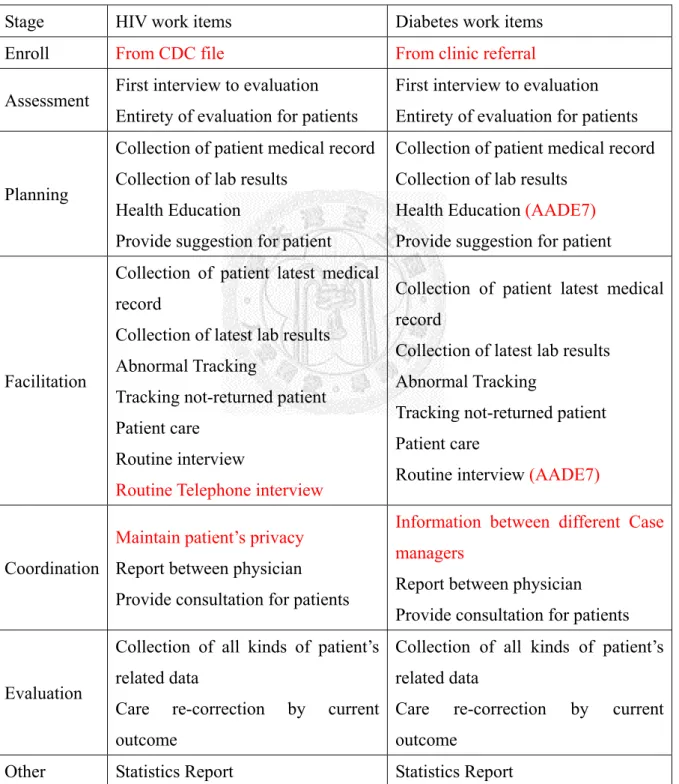
Table 1 HIV and Diabetes case management work content.
Stage HIV work items Diabetes work items Enroll From CDC file From clinic referral Assessment First interview to evaluation
Entirety of evaluation for patients
First interview to evaluation Entirety of evaluation for patients
Planning
Collection of patient medical record Collection of lab results
Health Education
Provide suggestion for patient
Collection of patient medical record Collection of lab results
Health Education (AADE7) Provide suggestion for patient
Facilitation
Collection of patient latest medical record
Collection of latest lab results Abnormal Tracking
Tracking not-returned patient Patient care
Routine interview
Routine Telephone interview
Collection of patient latest medical record
Collection of latest lab results Abnormal Tracking
Tracking not-returned patient Patient care
Routine interview (AADE7)
Coordination
Maintain patient’s privacy Report between physician Provide consultation for patients
Information between different Case managers
Report between physician Provide consultation for patients
Evaluation
Collection of all kinds of patient’s related data
Care re-correction by current outcome
Collection of all kinds of patient’s related data
Care re-correction by current outcome
Other Statistics Report Statistics Report
Upload data to NHI (National Health Insurance) and CDC (Centers for Disease Control)
Upload data to NHI (National Health Insurance)
We classify the works that case manager should do. Table 1 summarizes the workflows. In Table 1, we can find the work items between two diseases and most of them are the same, only small parts like enrolled resource, we must pay attention to HIV patient’s privacy and for Diabetes the related information can be shared among different case managers in coordination. The support from NTUH HIS is not enough now, case managers must spend much time in workflow. So we decide to develop a new information system to cover the deficiency part of HIS to provide assistance for case managers.
Chapter 3 System development
This chapter describes the development of information system, including system architecture and design pattern.
3.1 MVC architecture
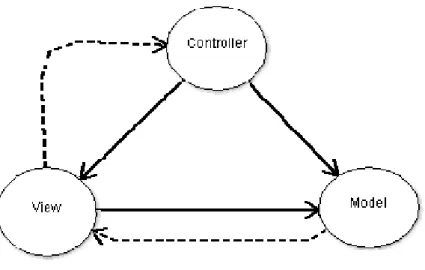
In system implementation, in order to ensure the flexibility of the program model and easy follow-up maintenance, after multi-aspect evaluation we used the Model-View-Controller (MVC) concept to design. MVC concept was provided by Trygve Reenskaug in 1974 which was a software design model invented from program language Smalltalk in Xerox PARC [23]. The purpose of MVC model in implementation of dynamic program design is easy to modify a program and simply extend functions, and it is possible to re-use the same part of a program. Besides, this model allows the program structure to be more intuitive through simplification. By separating each part of the program, at the same time, every basic part is given the function that should be. Figure 3.1 shows MVC model. The solid line represents a direct association, the dashed indicates an indirect association.
The definition of Model-View-Controller is as follows:
Figure 3.1 MVC architecture
1. Model: Managing the behavior and data of the application domain, it responds to requests for information about its state (usually from the view), and responds to instructions to change state (usually from the controller).
In event-driven systems, the model notifies observers (usually views) when the information changes so that they can react.
2. View: Rendering the model into a form suitable for interaction, typically a user interface element. Multiple views can exist for a single model for different purposes. A view port typically has a one-to-one correspondence with a display surface and knows how to render to it.
3. Controller: Controller receives user input and initiates a response by making calls on model objects. A controller accepts input from the users and instructs the model and a view port to perform actions based on that
input.
The MVC structure has several advantages. It forces to separate basically the data layer code like database searching script from the expression layer code like HTML.
Despite the MVC needs extra work to build the MVC application, it still has more benefits. First, several views can share a model; the same model can be re-used by different views, it greatly promotes the code re-usability. Second, the controller is a self-contained object; it is relatively independent from the view and model, so it can easily change the data layer and work method in the application, for example, changing database from MySQL to MSSQL, it only needs to replace the controller. Once practicing controller correctly, whatever the data come from MySQL or MSSQL, the view can display them right way. Finally, the controller can achieve user’s requirement by connecting to different models and views; it can select appropriate model processing type according to users’ demand. Despite the MVC also has defects that include indeterminate result, difficult to comprehend; and because the model and view must seriously separate, this let not only find error difficult but also include more files than before. Nevertheless it will cost much time to build MVC model framework, it can promote software development efficient at a later period.
On long-term perspective, because case management requirements are approximately similar, in order to extend as many disease support, we finally select using the MVC
model to develop our information system.
3.2 System architecture
In this case management (CM) system, we used Microsoft ASP.NET Framework 4.0 and MVC 2.0 to develop, and the database is Microsoft SQL Server 2008 R2. The system used other web-related technique including the web service and Asynchronous JavaScript XML (AJAX).
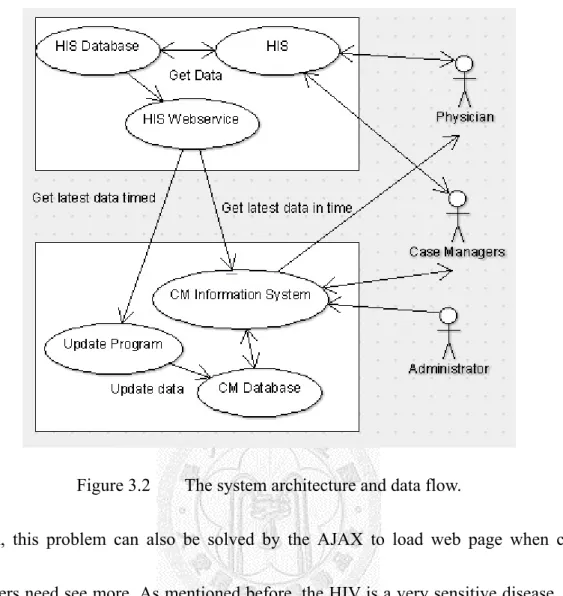
Figure 3.2 displays this system data flow with the staff including case managers and physicians. In data flow of the HIS and case management information system, we use the web services to update the patient’s data. This has several advantages, such as we can only get the minimum amount of data that we need, which not only decreasing the loading for NTUH HIS but also increasing the processing efficiency of data importing to the CM system. In addition, we design another program to update the latest information for the system. For example, the program will get all the data at the specific time in NTUH HIS with low loading. And some data need to be updated timely such as emergency record, so the updating program will get the data at a shorter time. Besides, the system can also immediately get the latest data when case managers need.
About the web-based application of the system, because a large amount of patient list can be included and their data may slow down the case managers in browsing the
Figure 3.2 The system architecture and data flow.
system, this problem can also be solved by the AJAX to load web page when case managers need see more. As mentioned before, the HIV is a very sensitive disease. We also set a simple link to mark the patient’s data when case managers leave the computer they are using temporarily.
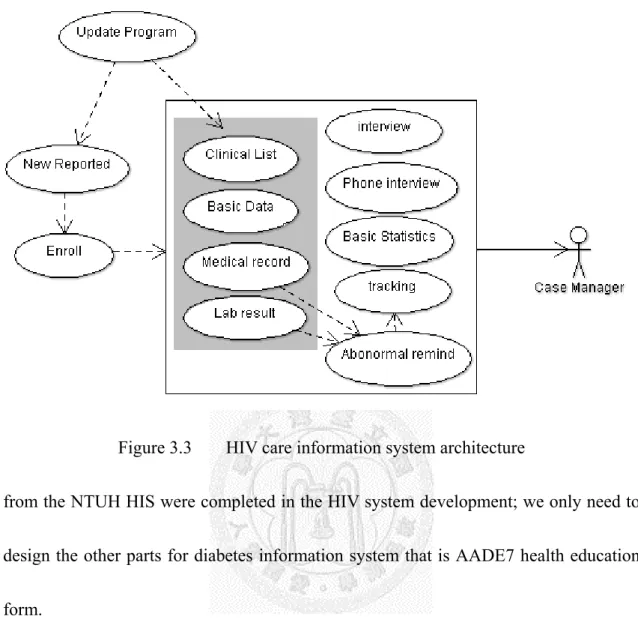
Figure 3.3 and Figure 3.4 show the HIV and diabetes system architecture of the information system. The two case management systems are almost the same; this also explains the reason why we use the MVC model to program. We spent ten months to complete the HIV information system; however, the diabetes information system was done by 5 months by the same manpower. Because most of the functions to fetch data
Figure 3.3 HIV care information system architecture
from the NTUH HIS were completed in the HIV system development; we only need to design the other parts for diabetes information system that is AADE7 health education form.
Figure 3.4 Diabetes care information system architecture
3.3 System status in present
We finally spent 15 months to develop the case management information system [6]. Table 2 shows the two information systems development line. Using the MVC model is actually decreasing the time in development. The information system server is in NTUH Informational Center now. After the information system being online, there are the information system related statistical shown in Table 2. In the HIV information system, there are three case managers who are using the system and dealing with approximate 800 enrolled patient’s related data. And the diabetes information system also supports five case managers and handles approximate 1,300 patients. Figure 3.5
displays the user interface of two systems, most of them are similar. In Figure 3.6, the interview forms of HIV information system and the AADE7 health education table of diabetes information system is the major differences. In order to increase the data readiness, our system updates all patients’ information in a specific time. This is shown in Table 3. Finally, in order to realize the efficiency of system, next chapter will describe the system evaluation
Table 2 Timeline in development of two systems [6]
HIV system Diabetes system
Development Timeline 2010/07~2011/05 2010/03~2011/07
Total Time (month) 10 5
Case Managers (persons) 3 5
Patients (persons) 2,138 1,297
Enrolled Patients (persons) 873 1,297
Table 3 The updating program schedule.
Updating items Updating time
All patient information At 2:00
Emergency records From 7:00 to 18:00, once in 30 minutes Clinic Records From 7:00 to 18:00, once in 1 hour Future clinic records At 7:00
Abnormal Laboratory results At 7:00
Figure 3.5 The user interface of two systems (left: Diabetes, right: HIV).
Figure 3.6 The interview of HIV system (right) and AADE7 health education table of Diabetes system (left).
Chapter 4 Methodology
4.1 System Evaluation Concept
The purpose of the system evaluation is getting the user’s behavior in system usage.
By monitoring and analyzing system efficiency using evaluation result, we can find where to improve. The case management information is to assist work of case managers, the effectiveness of the support from this system in workflow and user’s satisfaction need to be evaluated.
”Evaluation is carefully collecting information about a program or some aspect of a program in order to make necessary decisions about the program.“ Evaluation is defined by McNamara [24], the purpose of system evaluation which is collecting the information about system is to optimize and improve the developed system. The evaluation can be separated to three stages [24]:
1. Goals-based evaluation: Assessing the outcome before system still not operated can help user to allocate time and space; the system designer can also know about the system efficiency and expectative goal.
2. Process-based evaluation: Through outside observation and inside verification to know the processing and behavior of system usage to realize system’s operation. This evaluation could help long-term operation that could improve system efficiency step
by step through progressive observation.
3. Outcomes-based evaluation: After the usage of the system we will keep the usage data and record to do system usage analysis. Through them, we can realize what the user’s product actually.
By the three oriented-evaluations, we can understand the system’s advantages and disadvantages, and get improvement opinion.
4.2 System Evaluation Methodology
In order to evaluate, we need to collect information of system usage. There are some ways to collect. Table 4 lists the general ways of collecting original resource [24], and compares their advantages and disadvantages.
1. Questionnaires: Questionnaire is the most inexpensive, quickly and can collect a lot of samples in a short time. However, because of anonymous, it might get random or non-excepted answer.
2. Interview: Since interview is face to face, all of the related-information can be collected. We can control the information in range and depth. But interview could take much time and cost much, as well as not easy to compare and analyze with other users.
3. Documentation review: In the period of system operation, the left record information
was long-term and widespread. So, we can analyze the records to realize the processing of system operation. However, reviewing the document need more time to analyze; and if the required information was not recorded, we could not get it.
4. Observation: Through direct observation we can realize the behavior of users, how system operation and how system been used. The disadvantages are difficult to categorize observations and may affect the behavior of users.
5. Group meeting to discussion: By grouping members (the users and system designers) together, it can quickly get response through interaction and communication.
However, because of “group meeting”, it must let all members join the group meeting which could be more complicated and difficult to analyze.
6. Case studies: To fully understand all the system related information, we compare to several cases. Finally we can realize the total input, process and results. It costs time in waiting outcome.
The six collection data methods are in common. According to evaluation items and systems different, the method selected was changed. We select several methods to collect the information.
Table 4 The general ways of collection original resource [24].
Method Overall Purpose Advantages Challenges
questionnaires,
when need to quickly and/or easily get lots of information from people in a
non-threatening way
-can complete anonymously -inexpensive to administer
-easy to compare and analyze
-administer many people -can get lots of data -many sample already exist
-might not get careful feedback
-wording can bias client's responses -are impersonal - doesn't get full story
interviews
when want to fully understand someone's impressions or
experiences, or learn more about their answers to questionnaires
-get full range and depth of information
-develops relationship with client
-can be flexible with client
-can take much time -can be hard to analyze and compare
-can be costly
-interviewer can bias client's responses
documentation review
when want impression of how program operates without interrupting the program; is from review of applications, finances, memos, minutes, etc.
-get comprehensive and historical information -doesn't interrupt program or client's routine in program -information already exists
-few biases about information
-often takes much time -info may be
incomplete
-need to be quite clear about what looking for -not flexible means to get data; data restricted to what already exists
observation
to gather accurate information about how a program actually operates, particularly about processes
-view operations of a program as they are actually occurring -can adapt to events as they occur
-can be difficult to interpret seen behaviors -can be complex to categorize observations -can influence
behaviors of program participants
-can be expensive
focus groups
explore a topic in depth through group discussion, e.g., about reactions to an
experience or suggestion, understanding common complaints, etc.; useful in
evaluation and marketing
-quickly and reliably get common impressions -can be an efficient way to get much range and depth of information in a short time
- can convey key information about programs
-can be hard to analyze responses
-need good facilitator for safety and closure -difficult to schedule 6-8 people together
case studies
to fully understand or depict client's
experiences in a program, and conduct comprehensive examination through cross comparison of cases
-fully depicts client's experience in program input, process and results -powerful means to portray program to outsiders
-usually quite time consuming to collect, organize and describe -represents depth of information, rather than breadth
4.3 Evaluation items
We separate the evaluation items to two parts:
1. Work-flow support
As mentioned before, in order to provide assistance for case managers, we develop the case management information system to achieve this goal. So, the evaluation will point at work-flow support (Table 1). This evaluation items belong to process-based evaluation, by observing the users behaviors whatever been supported by the information system. Through process-based evaluation analysis, we can
understand the value of the system that has been used. Hence, we select the workflow support status as evaluation item.
2. User Satisfaction and system acceptability
User satisfaction belongs to outcomes-based evaluation. After the information system being online, we started to support case managers’ workflow. However, the system designers couldn’t know the situation of the usage, for example, system function, user interface and system acceptance etc., those are evaluation items. By the questionnaire designed from Hong-Li Juan [25], we first evaluate the information literacy of case managers to confirm credit, and then using second questionnaire about system requirement (before) and system satisfaction by Jia-Pin Juang [26] and acceptability from Martinez [27, 28] (after). Via the user feedback, we can know more about the advantages and disadvantages of the information system. Table 5 summarizes the three questionnaires.
Table 5 Summary to three questionnaire evaluated items.
Content
Information literacy of nurse [25]
Designed from Hong-Li Juan, Content Validity Index; CVI is 56-92%, average is 80.9%; Cronbach'α value is 0.778.
This questionnaire is separated to two parts.
First part: Basic attribute, computer and network resource and experience.
Second part: Evaluation of information literacy scale, total is 60 questions.
Use the Likert scale 4 point, 1 completely not, 2 partly not, 3 partly can and 4 completely can; the total score is higher represent information literacy better [25].
User requirement and Satisfaction [26]
These questions are separated to two part: The first part is requirement, 26 questions, further separated to “function”
and “maintenance”, Use the Likert scale 5 point.
The second is satisfaction, 26 questions, same as the first part and separated to two parts “function” and
“maintenance”, and extra three questions added:
“Overall, is the case management information system what want?”
“Overall, how much do you feel about the system promoting scale for you work efficient?”
“Overall, how much is your satisfaction to the system?”
Use the Likert scale 5 point; 5 greatly agree, 4 very agree, 3 partly agree, 2 disagree and 1 completely not agree.
System acceptability [27, 28]
8 simple questions to evaluate acceptability.
Use the Likert scale 5 point; 5 greatly agree, 4 very agree, 3 partly agree, 2 disagree and 1 completely not agree.
Chapter 5 Result and Discussion
This chapter describes the evaluation result, and the related outcome and data.
5.1 Result
5.1.1 System Support in Case Management
As mentioned before, we list the work-flow of case managers need. Through processing-based evaluation, the system supporting for case management will demonstrate more clearly. Most workflow items are supported by the information system, except for the “direct care and consultation” or providing suggestions to patients that must be supported by case managers. Other system didn’t completely support items one was “statistics report print and export”. This part must connect to other unit, such as National Health Insurance. We only provide some simple statistics function, for example, calculating the percent of re-clinic, today clinic patient count etc. Table 6 shows all the workflow supported.
Table 6 The list workflow items support by system.
Stage Case management work items System support Enroll From CDC file (HIV)
From clinic referral (Diabetes) Both are supported by system
Assessment First interview to evaluation Entirety of evaluation for patients
Interview can be recorded by system
Entire information can be collected through system
Planning
Collection of patient medical record Collection of lab results
Provide suggestion for patient Health Education (HIV)
AADE7 health education (Diabetes)
Collection part can be handled by system
Health education can be recorded by system
Facilitation
Collection of patient latest medical record
Collection of latest lab results Abnormal Tracking
Tracking not-returned patient Patient clinic care
Routine interview
Routine Telephone interview (HIV)
Besides patient clinic care, all of the others can be supported by system.
Coordination
Information between different Case managers (Diabetes)
Maintain patient’s privacy (HIV) Report between physician (Diabetes) Provide consultation for patients
Besides consultation, this must be done face to face by case manager self; others can be supported by system.
Evaluation
Collection of all kinds of patient related data
Care re-correction by current outcome
Case managers could re-correct the care planning by information supported by system.
Other
Statistics Report
Upload data to National Health Insurance and CDC (HIV)
Partly supported.
5.1.2 User Satisfaction and system acceptable
There are five case managers for diabetes care and three for HIV care. Hence, we sent totally eight questionnaires for the eight case managers. The following is questionnaire results:
1. The basic demographic data of case managers (Table 7):
All case managers are female; the average age is 42.33 years old, S.D. is 4.1;
37.5% of case managers are married; 62.5% of case managers have Master degree; the work year is principle in 10 to 20 years.
2. Information literacy of nurse (not shown): The average score is 202 points; all case managers think the computer was enough in work place.
3. The user requirement (Table 8) :
Most of requirement averages are greater than 4.5 points. The S.D. ranges are from 0 to 1; Cronbach's α value is 0.852; the lowest requirement is “The function of merge-print the management record in system (4.1)”.
The user satisfaction (
4. Table 9):
User satisfaction averages are from 2.8 to 4.4 points. The S.D. ranges are from 0.6 to 1.3; Cronbach's α value is 0.946; the highest user satisfaction is “Can
search by patient's basic information (4.4)”; the lowest is “The function of providing merge-print the management record in system (2.8)”.
5. The user acceptability (Table 10)
Averages are from 3.5 to 4.3, and the S.D ranges are 0.7 to 0.8. Cronbach's α value is 0.925; The highest user acceptability is “The training received is adequate (4.3)”; the lowest is “I feel I provide the right attention to patients using this system (3.1)”.
Table 7 The basic data of case managers.
N=8
Variable Peoples Percent Mean S.D.
Sexual male 0 0%
female 8 100%
Ages <40 years old 2 25.00%
43.33 4.1
>40 years old 6 75.00%
Married Yes 3 37.50%
No 5 62.50%
Education Collage 3 37.50%
Master 5 62.50%
Work Year
<10 years 2 25.00%
14.63 5.63 10~20 years 4 50.00%
>20 years 2 25.00%
Table 8 The user requirement of system. (Cronbach's α value is 0.833)
Items Scores
Function Mean SD
1 The screen visual comfortable of System 4.7 0.45 2 System interface is simple and easy to understand 5.0 0
3 System response time 5.0 0
4 System stability degree 5.0 0
5 The list item of Patients in System main screen 4.9 0.3 6 System provides kinds of search condition 4.7 0.7 6.1 Can search by patient's basic information 5.0 0 6.2 Can search specific record of period by date 4.7 0.5
6.3 Can Search by case status 4.7 0.5
6.4 Can search by days of lost 4.7 0.5
7 The function of registering the management record in system 4.7 0.5 8 The function of reading the management record in system 4.7 0.5 9 The function of providing print the management record in system 4.7 0.5 10 The function of merge-print the management record in system 4.0 0.9 11 The function of providing export a series of the management record in
system 4.4 0.7
12 System can link to information system in hospital 5.0 1 13 The system can feedback the management record to related system in
hospital 4.6 0.7
14 System can provide real-time in searching case 4.4 0.9 15 System can alert actively about tracking 4.7 0.5 16 System can provide statistical analysis 5.0 0
Maintain
1 There have Professional program can maintain system 5.0 0 2 There have appropriate permissions to manage system 5.0 0 3 System has enough storage capacity in hardware 5.0 0
4 Guideline for system operation 4.9 0.3
5 Manual for Standard operating system 5.0 0 6 The requirement for completed time to tracking and review in system 5.0 0
function update and change
Table 9 The user satisfaction of system. (Cronbach's α value is 0.94)
Items Scores Function Mean SD
1 The screen visual comfortable of System 4 0.5
2 System interface is simple and easy to understand 4.1 0.6
3 System response time 4 0.5
4 System stability degree 3.9 1
5 The list item of Patients in System main screen 4.3 0.5 6 System provides kinds of search condition 4 0.8 6.1 Can search by patient's basic information 4.6 0.5 6.2 Can search specific record of period by date 3.9 1
6.3 Can Search by case status 3.1 1.1
6.4 Can search by days of lost 3.3 1.3
7 The function of registering the management record in system 3.9 1 8 The function of reading the management record in system 3.7 0.9 9 The function of providing print the management record in system 3.3 0.9 10 The function of merge-print the management record in system 2.7 1.3 11 The function of providing export a series of the management record in
system 2.9 1.1
12 System can link to information system in hospital 3 1.6 13 The system can feedback the management record to related system in
hospital 3 1.3
14 System can provide real-time in searching case 3.9 1 15 System can alert actively about tracking 3.1 1,2 16 System can provide statistical analysis 3.3 0.9
Maintain 1 There have Professional program can maintain system 3.1 1
2 There have appropriate permissions to manage system 3.9 0.8 3 System has enough storage capacity in hardware 3.7 0.9
4 Guideline for system operation 3 1
5 Manual for Standard operating system 3.1 1.2
6 The requirement for completed time to tracking and review in system
function update and change 3.1 1.4
A Overall, is the case management information system confirming your
requirement? 3.7 0.9
B Overall, how much do you feel about the system promotion scale for you
work efficient? 3.9 0.8
C Overall, how much is your satisfaction for the system? 3.9 0.6 Table 10 The user acceptability of system. (Cronbach's α value is 0.908) System acceptability ( 8questions) Mean SD 1 I am satisfied with the use of the system 4.1 0.6 2 I feel I provide the right attention to patients using this system 3.1 0.8
3 I would use the system again 4.1 0.6
4 I would recommend it to others 3.9 0.6
5 I find the system easy to use 4 0.8
6 I find the use the system is stressing (inverted question) 3.9 0.8 7 The training received is adequate 4.4 0.5 8 The system improves the care provided to patients 3.6 0.7
5.2 Discussion
About workflow supporting for case managers routine work list (Table 6), the system can cover most of “information-related” work, except for statistics report and file to CDC and National Health Insurance (NHI) or other of the “non-information”
works including direct care and providing consultation for patents. Because the system can’t directly connect to the CDC or NHI, so it couldn’t provide the function for filing.
About the statistics report, we only design the excel table export for case management to list patients.
In the questionnaire outcome, the information literacy of nurse (not shown): The
average score is 203 points, so case managers belonged to high information literacy community [25]. In the user requirement questionnaire, most of the average scores are greater than 4.4 point. This result is also identical to Jia-Pin Juang and M. F. Yen [26, 29]. In case management workflow, the case managers indeed need support from information system. About user satisfaction part, most questions are greater than 3.3 points; the lowest is“The function of merge-printing the management record in system
(2.8)”,“The function of providing export a series of the management record in system
(2.9)” and“System can link to information system in hospital (2.9)”. The reason of the
lowest score is, this system didn’t provide print extra education table and excel file function in HIV care. This also indicated case managers need information function in export or input data. Overall, the results of confirming requirement (3.7 points), promoting work efficiency (3.9), user satisfaction is positive (3.9) and user acceptability (all greater than 3.6) is positive.
The two aspect evaluations (processing-based and outcome-based) help us to find more potential problems. For example, the user acceptability of question 2 “I feel I can pay the right attention to patients using this system” average point is 3.1. The possible reason is the computer used is desktop PC; however, the case managers couldn’t “bring PC” around to provide medical work. If we can provide the information system using tablet PC, this acceptability result could be better.
Chapter 6 Conclusion and Future Work
6.1 Conclusion
By developing case management information system, we successfully support most of information-related workflow; through kinds of information integration, case manager can concentrate more in patient’s care. In system evaluation, we also confirm that the system is positively beneficial to the case managers. However, we still have space for improvements. For example, the system only supports HIV and Diabetes workflow in present; if the other chronic diseases like kidney disease, chronic obstructive pulmonary disease (COPD) and heart failure that long-term affecting patient are integrated to this system, the evaluation could be more multi-aspects, we might process further long-term research such as data-mining or patient outcome improvement researches.
6.2 Future Work
The next stage, we will go for several goals:
1. Mobile information system:
There are more and more information systems specific for mobile platform such as drug consultation [30]. Self-management information system also can be used for
diabetes care and the information can be used more times in mobile platform than in PC [31], the information can be browsed anywhere is the trend.
2. Clinic disease support system (CDSS):
CDSS can promote clinical performance such as drug dosing, simple vital signs abnormal determination for medical staff [32], more advanced system can suggest cancer treatment [33]. In case management, maybe the system could be designed for individualized to assist the primary care.
Reference
1. Taiwan Department of Health (台灣行政院衛生署) 2010國人十大死因統計報 告. 2010.
2. Kersbergen, A.L., Case management: A rich history of coordinating care to control costs. Nursing Outlook, 1996. 44(4): p. 169-172.
3. Ofman, J.J., et al., Does disease management improve clinical and economic outcomes in patients with chronic diseases? A systematic review. The American Journal of Medicine, 2004. 117(3): p. 182-192.
4. Mohagheghi, P., V. Dehlen, and T. Neple, Definitions and approaches to model quality in model-based software development-A review of literature. Information and Software Technology, 2009. 51(12): p. 1646-1669.
5. Jacobs, B., Electronic medical record, error detection, and error reduction: A pediatric critical care perspective. Pediatr Crit Care Med, 2007. 8(2).
6. Li, H.-C., Modeling Information System Architecture for Health Care Case Management. 台灣大學碩士論文, 2011.
7. Sowell, R.L. and T.M. Meadows, An integrated case management model:
Developing standards, evaluation, and outcome criteria. Nursing Administration Quarterly, 1994. 18(2): p. 53.
8. Baldwin, S. and P.A. Woods, Case management and needs assessment: Some issues of concern for the caring professions. Journal of Mental Health, 1994.
3(3): p. 311-322.
9. Orwin, R.G., et al., Pitfalls in evaluating the effectiveness of case management programs for homeless persons. Evaluation Review, 1994. 18(2): p. 153-207.
10. American Case Management Association ( ACMA美國個案管理學會). 2011;
Available from: http://www.acmaweb.org/.
11. Noor, A.M., et al., Health service providers in Somalia: their readiness to provide malaria case-management. Malaria journal, 2009. 8(1): p. 100.
12. Schmittdiel, J., et al., The effectiveness of diabetes care management in managed care. The American journal of managed care, 2009. 15(5): p. 295.
13. Gardner, L.I., et al., Efficacy of a brief case management intervention to link recently diagnosed HIV-infected persons to care. Aids, 2005. 19(4): p. 423.
14. PhD, A.R.W., et al., An adherence-focused case management intervention for HIV-positive patients in a public care setting. Journal of HIV/AIDS & Social Services, 2009. 8(1): p. 80-94.
15. Jiang, L.-Q. Case Management and Health Education. 2008 [cited 2011
05-20]; Available from:
http://health99.doh.gov.tw/Article/ArticleDetail.aspx?TopIcNo=45&DS=1-Artic le.
16. Devine, F., Health Information Technology and What It Means to Case Managers. Professional Case Management, 2010. 15(2): p. 59-61 10.1097/NCM.0b013e3181d2122d.
17. McMahon, G.T., et al., Web-based care management in patients with poorly controlled diabetes. Diabetes Care, 2005. 28(7): p. 1624.
18. Siika, A.M., et al., An electronic medical record system for ambulatory care of HIV-infected patients in Kenya. International Journal of Medical Informatics, 2005. 74(5): p. 345-355.
19. Maass, M.C., et al., Usefulness of a Regional Health Care Information System in primary care: A case study. Computer methods and programs in biomedicine, 2008. 91(2): p. 175-181.
20. American Association of Diabetes Educators (AADE美國糖尿病學會). 2011;
Available from: http://www.diabeteseducator.org.
21. Gonzalez, A., Diabetes education for all! The Diabetes Educator, 2008. 34(3): p.
373-373.
22. How to Write Nursing Notes in SOAP Format. Available from:
http://www.ehow.com/how_8371959_write-nursing-notes-soap-format.html.
23. Reenskaug, T. MVC XEROX PARC 1978-79. 1978-79 [cited 2011 05-25].
24. McNamara, C. Basic Guide to Program Evaluation. Available from:
http://managementhelp.org/evaluation/program-evaluation-guide.htm#anchor15 75679.
25. 洪麗娟, 臨床護理人員資訊素養及其相關因素之研究. 長榮大學護理學研
究所學位論文, 2008(2008 年).
26. 張嘉蘋, et al., 癌症個案管理資訊系統之評值. 醫療資訊雜誌, 2011. 20(1): p.
49-58.
27. de Toledo, P., et al., Telemedicine experience for chronic care in COPD.
Information Technology in Biomedicine, IEEE Transactions on, 2006. 10(3): p.
567-573.
28. A.Mart´ınez, R.R., A. Infante, C. Campillo, and C. Gattini, Bases Metodol´ogicas Para Evaluar la Viabilidad y el Impacto de Proyectos de Telemedicina. Washington: Organizaci´on panamericana de la salud, 2001.
29. Chou), 顏.M.F.Y.周.S.M., 資訊時代中的個案管理. 護理雜誌, 2001. 48(3): p.
33-37.
30. Sadasivam, R.S., et al., Development of a Point-of-Care HIV/Aids Medication Dosing Support System Using the Android Mobile Platform. Journal of medical systems, 2010: p. 1-9.
31. Lin, Y.H., et al., Developing a Web 2.0 Diabetes Care Support System with Evaluation from Care Provider Perspectives. Journal of medical systems, 2011:
p. 1-11.
32. Hunt, D.L., et al., Effects of computer-based clinical decision support systems on physician performance and patient outcomes. JAMA: the journal of the American Medical Association, 1998. 280(15): p. 1339.
33. Hsueh-Chun, L., et al., Development of a real-time clinical decision support system upon the web mvc-based architecture for prostate cancer treatment.
BMC Medical Informatics and Decision Making. 11.
Appendix
護理人員資訊素養研究之問卷 第一部份:基本資料
一、基本屬性:
1、您的出生年月為:民國 年 月
2、您的最高學歷為:□1.博士、□2.碩士、□3.大學 □4.專科,
畢業年度為:民國 年 目前進修中:□是□否 3、您的婚姻狀況:□1.已婚、□2.未婚、□3.離婚、□4.其他 4、是否需要陪同小孩或親人上網:□0.無、□1.有
5、您的護理工作年資: 總共 年
6、您到台大醫院就職時間為:民國 年 月,
7、目前單位到職時間為民國 年 月
8、您的職稱為:□1.約用護理師、□2.護士、□3.護理師、□4.專科護理師、
□5.個案管理師、□6.小組長、□7.護理長(含代理)、□8.其他_________
9、您的護理能力進階層級為:□0.N、 □1.N1、 □2.N2、 □3.N3、□4.N4、
□5.NL 以上
10、您有無兼任資訊相關業務□0.無 有( 請自填 ) 二、相關資源
1、您的住所有無您專屬之電腦:□0.無、□1.有 2、您的工作場所有無您專屬之電腦:□0.無、□1.有 3、您的住所電腦是否能上網:□0.否、□1.是
4、您的工作場所電腦是否能上網:□0.否、□1.是 5、您認為工作場所中的電腦是否足夠護理人員使用:
□0.非常不夠、□1.稍嫌不足、□2.足夠 6、當您碰到電腦問題時通常會怎麼做(可複選):
□1.問家人、 □2.問同事、 □3.問朋友、 □4.問資訊相關人員、
□5.看電腦操作手冊、 □6.看書、 □7.上網查資料、 □8.上網發問 、
□9.其他 7、請問您最常使用電腦或上網的地點為(可複選)
□1.住所、 □2.辦公室、 □3.護理站、 □4 公共設施電腦(圖書館、社教館等)、
□5.網咖、 □6.無線網路、 □7.其他
三、相關經驗
1、請問您每週平均使用電腦(不包括上網)的時數為多久?
□0.沒有使用、□有使用(約 小時)
2、請問您每週平均上網的時數為多久?□0.沒有使用、□有使用(約 小時)。
3、請問您有無使用過下列軟體?使用頻率如何?
(1) Windows 操作:
□0.沒有用過、□1.每年使用 1-2 次、□2.每季使用 1-2 次、
□3.每月使用 1-2 次、□4.每週使用 1-2 次、□5.每天使用 (2) 文書處理如 Word 等:
□0.沒有用過、□1.每年使用 1-2 次、□2.每季使用 1-2 次、
□3.每月使用 1-2 次、□4.每週使用 1-2 次、□5.每天使用 (3) 試算表如 Excel:
□0.沒有用過、□1.每年使用 1-2 次、□2.每季使用 1-2 次、
□3.每月使用 1-2 次、□4.每週使用 1-2 次、□5.每天使用 (4) 簡報軟體如 Power Point:
□0.沒有用過、□1.每年使用 1-2 次、□2.每季使用 1-2 次、
□3.每月使用 1-2 次、□4.每週使用 1-2 次、□5.每天使用 (5) E-mail:
□0.沒有用過、□1.每年使用 1-2 次、□2.每季使用 1-2 次、
□3.每月使用 1-2 次、□4.每週使用 1-2 次、□5.每天使用
4、請問您在學校制式教育中有無參加過下列電腦、網路或資訊等相關課程?
□1.Windows 操作、 □2.文書處理:如 Word 等、 □3.試算表:如 Excel、
□4.簡報軟體:如 Power Point、 □5.E-mail 使用、 □6.資訊搜尋技巧、
□7.實證護理資料查詢、 □8.網路使用、 □9.其他: 、
□0.完全沒有
研習總學分數共: 學分
5、請問您三年內在工作場所或補習班等場所有無參加過下列電腦、網路或資訊等 相關課程?
□1.Windows 操作、 □2.文書處理:如 Word 等、 □3.試算表:如 Excel、
□4.簡報軟體:如 Power Point、 □5.E-mail 使用、 □6.資訊搜尋技巧、
□7.實證護理資料查詢、 □8.網路使用、 □9.其他: 、
□0.完全沒有
研習時數共: 小時
第二部份:資訊素養問卷:
一、 電腦素養(基本技能及應用):請您依下列之敘述,勾選最適合您的狀況
題目
非 常 熟 練
大 部 份 熟 練
大 部 份 不 會
完 全 不 會
1 能做一般的 Windows 開關機 □ □ □ □
2 能操作檔案總管之資料夾新增刪除等功能。 □ □ □ □
3 能操作桌面新增捷徑等設定。 □ □ □ □
4 能設定控制台各種元件的設定如網路連線設定等。 □ □ □ □
5 能做簡易的 Word 文書處理、修改、打字及列印。 □ □ □ □
6 能操作 Word 文書處理排版之功能,字型與段落等進階設
定。 □ □ □ □
7 能操作 Word 製作表格文件能力,框線網底、項目編號等進
階設定。 □ □ □ □
8 能操作 Word 合併列印的能力。 □ □ □ □
9 能操作 Word 文件設定目錄之功能。 □ □ □ □
10 能閱讀 Excel 統計軟體的檔案,做簡單的資料輸入、編輯與
列印。 □ □ □ □
11 能操作 Excel 做資料的排序,常用的函數使用如加總、平均。 □ □ □ □
12 能操作 Excel 做儲存格格式設定之功能。 □ □ □ □
13 能操作 Excel 資料做成單一統計圖表。 □ □ □ □
14 能操作 Excel 做成雙座標之各種統計圖表如柏拉圖等。 □ □ □ □
15 能操作 Excel 做統計函數的運用(如 t-test 等)。 □ □ □ □
16 能閱讀 PowerPoint 簡報軟體的檔案,並能做簡報的播放及
操作 □ □ □ □
17 能簡易的 PowerPoint 簡報檔案,排版及背景與字型設定。 □ □ □ □
18 能操作 Power Point 插入圖片美化及統計圖表工作。 □ □ □ □
19 能操作 Power Point 做各種動畫及特效的展示。 □ □ □ □
20 有 E-mail 電子信箱,能自行閱讀電子郵件。 □ □ □ □
21 具有建立及傳送新郵件能力,能做郵件之回覆轉寄功能。 □ □ □ □
22 寄送 E-mail 會附加檔案及圖片。 □ □ □ □
23 能做 E-mail 之通訊錄之管理。 □ □ □ □
24 能做 E-mail 電子信箱郵件規則之設定。 □ □ □ □
25 熟悉 E-mail [工具][選項]內的各項設定。 □ □ □ □
二、網路素養(資訊搜尋技巧、應用技巧) 請您依下列之敘述,勾選最適合您的狀 況
題目
非 常 熟 練
大 部 份 熟 練
大 部 份 不 會
完 全 不 會
1 您會在操作瀏覽器中時將我的最愛或書籤的內容匯入或匯
出嗎? □ □ □ □
2 您會使用瀏覽器匯入匯出通訊錄的功能嗎? □ □ □ □
3 您會在電腦上進行網路設定(TCP/IP)嗎? □ □ □ □
4 您會使用瀏覽器(如 Netscape、IE、Firefox)來瀏覽網際網路
嗎? □ □ □ □
5 您會使用網路上的搜尋引擎(如 Google、GAIS、Yahoo)來尋
找需要的資料嗎? □ □ □ □
6 您會連上網利用搜尋引擎(如 Google、Yahoo---等)找到需要
的網站或資料庫嗎? □ □ □ □
7 您能利用圖書館資訊系統去尋找所需要的參考資料嗎?(如
OVID、Chanel-等) □ □ □ □
8 您能利用圖書館資訊系統去尋找實証文獻嗎?(如 EBN、
Cohren-等) □ □ □ □
9 您會使用通訊軟體連上電子佈告欄(BBS)嗎? □ □ □ □
10 您參加討論群組(News)來蒐集資訊或與其他人討論嗎? □ □ □ □
11 當您引用他人的作品時,您知道如何加以註明出處嗎? □ □ □ □
12 您曾使用網路會客室、聊天室嗎? □ □ □ □
13 當您進行資料搜尋時,您會使用進階搜尋功能,以擴大或縮
小資料範圍嗎? □ □ □ □
14 您會下載網路上的資料存檔使用或以電子郵件傳送嗎? □ □ □ □
15 您能夠透過內部網站上傳或下載業務相關文件嗎? □ □ □ □
16 您遇到一些簡易的問題能透過網路獲得適當的協助嗎? □ □ □ □
17 您能將收集到的網路資料分類整理成一份報告或文章嗎? □ □ □ □
18 您能預防及處理病毒入侵嗎? □ □ □ □
![Table 2 Timeline in development of two systems [6]](https://thumb-ap.123doks.com/thumbv2/9libinfo/9608139.633768/30.892.145.749.499.749/table-timeline-development-systems.webp)