Title: Risk of Adolescent Offspring’s Completed Suicide Increases with The History of Their Same-sex Parents’ Death by Suicide
Heading: Suicide of Parent and Same-sex Offspring
Authors’ names and affiliations:
Chi-Chia Jessica Cheng, Ph.D.1; Wen-Jiuan Yen, R.N., Ph.D.2; Wan-Ting Chang, M.Sc.3; Kevin Chien- Chang Wu, M.D., LL.M., Ph.D.4,5, Ming-Chung Ko, M.D., MSc. 3,6,7; and Chung-Yi Li, Ph.D.8,9
1. Department of Public Health, College of Medicine, Fu-Jen Catholic University, New Taipei City, Taiwan
2. College of Nursing, Chung Shan Medical University, Taichung City, Taiwan
3. Department of Health Care Management, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan
4. Department of Social Medicine, School of Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan
5. Department of Psychiatry, National Taiwan University Hospital, Taipei, Taiwan
6. Department of Surgery, Zhong-Xing Branch of Taipei City Hospital, Taipei, Taiwan
7. Institute of Public Health, School of Medicine, National Yang-Ming University, Taipei, Taiwan
8. Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan
9. Department of Public Health, College of Public Health, China Medical University, Taichung, Taiwan
Ming-Chung Ko and Chung-Yi Li contributed to this article equally.
Corresponding author:
Ming-Chung Ko, MD, MSc
Department of Surgery, Taipei City Hospital 145 Zheng Zhou Rd., Taipei, Taiwan 103 e-mail: [email protected]
Tel: 886-2-2552-3234; Fax: 886-2-2375-8291
Funding/support: This study was supported by a grant from the National Scientific Council (NSC101-2314-B-006 -076 -MY3) located in Taipei, Taiwan; and it has no role in both conducting the study and interpreting the results.
Acknowledgments: Nil
ABSTRACT
Backgroud. To investigate the risk of completed suicide in offspring during adolescence in relation to prior history of the same-sex parent’s death by suicide and other causes .
Methods. Overall 500 adolescents who died of completed suicide at age of 15-19 years between 1997 and 2007 were identified from the Taiwan Mortality Registration (TMR). For each case, 30 age- and time-matched controls were randomly selected from all adolescents registered in
Taiwan’s Birth Registry (TBR). Multivariate conditional logistic regression model was used to assess the risks of adolescent completed suicide in relation to their same-sex parent.
Results. Risk of adolescent’s suicide was positively associated with both paternal (Adjusted odds ratio (AOR)=5.38 (95% CI=2.17-13.33) and maternal suicide (AOR=6.59, 95% CI=1.82-23.91).
The corresponding risk estimates associated with paternal and maternal deaths from non-suicidal causes were much lower at 1.88 and 1.94, respectively. The risk of suicide in male youths was significantly associated with prior history of paternal suicidal death (AOR=8.23, 95% CI=2.96- 22.90) , but not with that of maternal suicidal death (AOR=3.50, 95% CI=0.41-30.13). On the other hand, risk of suicid al death in female youths was significantly associated with prior history of
maternal suicide (AOR=9.71, 95% CI=1.89-49.94) , but not with that of paternal suicid al death (AOR=2.42, 95% CI=0.30-19.57). However, the above differences reached no statistical
significance.
Conclusions. Although limited by sample size, our study tends to suggest that an offspring’s suicidal death is associated more with prior history of his/her same-sex parent’s death by suicide.
Key Words. adolescent, case-control studies, suicide, parent
INTRODUCTION
It has been well documented that suicidal behavior runs in families. Mounting evidence suggests that individuals with a family history of suicide were at increased risk of suicidal behavior. The familial transmission of suicide was also found to be independent of transmission of psychiatric disorder per se ( Brent & Melhem, 2008; Kim et al. 2005; Qin et al. 2002; Sørensen et al. 2009;
Runeson & Åsberg, 2003). Both genetic disposition and shared environment are found to be related to suicidal clustering in families (Brent & Melhem, 2008; Brent & Mann, 2005).
Many studies found that parental death, especially from suicide, is a significant risk factor for youth’s psychosocial maladjustment, psychiatric disorder, and suicidal behavior. Compared to those who lost a parent to non-suicidal causes, the youth with a parent who died by suicide were more vulnerable to depression, anxiety, psychological distress, bipolar disorder, and personality disorder, all lead to an increased risk of suicidal attempts and completion (Wilcox et al. 2010;
Brent et al. 2009; Tsuchiya et al. 2005;Agerbo et al. 2002; Pfeffer et al. 2000). But, some other studies reported little difference in child or adolescent outcomes resulting from various causes of parental death (Melhem et al. 2008; Cerel et al. 1999).
In addition to family clustering of suicidal behavior, previous evidence also indicates that gender of parents may be associated with differential risk of offspring suicide. Mothers who died of either suicide or other causes were found to pose greater impacts on risks of offspring
psychiatric disorders and suicide than were fathers (Qin et al. 2002; Brent et al. 2009; Tsuchiya et al. 2005; Agerbo et al. 2002; Lawrence et al. 2006). Some studies also found that the youth who lost a parent, especially mother, to suicide at a younger age tended to experience an even
heightened risk for suicide and suicidal behavior (Wilcox et al. 2010; Brent et al. 2009; Tsuchiya et al. 2005; Agerbo et al. 2002; Garssen et al. 2011). Previous studies suggested that maternal loss, especially to suicide conveyed higher risks to offspring maladjustment and suicide (Brent et al. 2009; Tsuchiya et al. 2005; Agerbo et al. 2002; Kuramoto et al. 2010). Authors of those previous reports argued that loss of mother might mean loss of a primary caregiver and a
significant source of support. Deprivation of adequate care as well as an affectionate attachment figure may result in an increase in risk of suicide in youth.
Previous studies found that father and mother play differential roles in boys and girls’
development (Russell et al. 1997;Steinberg et al. 1987). Each of the dyads of mother-daughter, mother-son, father-daughter, and father-son may be distinct in terms of characteristics of the relationships and child outcomes associated with the relationships. Theoretical accounts such as social learning theory and psychoanalytic theory (Washburn, 1994; Bandura, 1975) often suggest that the same-sex parent is usually the model of identification, and from whom a child learns not only outward behavior but also development of inward sense of self. The sameness of the relations also closely bonds each to the other (Russell et al. 1997). In fact, a study conducted on incarcerated adolescents found that males’ numbers of suicidal attempt were significantly related to father’s affectionless bonding style, but not related to mothers’ bonding style (McGarvey et al.
1999). Abdelnoor & Hollins (2004) found that females who lost their mothers, compared to their fathers, were more likely to undergo traumatic bereavement process. Thompson et al. (2012) found that same-sex parent was also a primary source of help for child and adolescents, who tended to choose their same-sex parent as a target of help-seeking whenever needed. Despite the above evidence, little is known concerning the gender-specific association of suicidality between
parents and offspring (Mittendorfer-Rutz et al. 2008; Lieb et al. 2005). Specifically, it is not clear whether a loss of same-sex parental attachment, in comparison with opposite-sex parental figure, may carry a higher risk for young suicide.
The current study sought to assess whether risk of adolescent completed suicide associated more with parent’s death by suicide than with death by other causes in Taiwan. We also aimed to investigate if there is a gender-specific association of offspring’s suicidal death during
adolescence with prior history his/her same-sex parent’s suicide by death.
METHOD
Source of data
In Taiwan, it is required by law that all live births and deaths be registered within 10 days.
Various birth characteristics including gender, birth weight, gestational age, single/multiple birth, birth order, parental ages, education, marital status, employment and place of birth are available for each live birth in the Taiwan Birth Registry (TBR), which has been evaluated and is
considered valid and complete (Chen et al.2010). Mortality data were obtained from the Taiwan Mortality Registry (TMR). The TMR is considered accurate and complete because it is
mandatory to register all deaths in Taiwan and for physicians to complete all death certificates (Directorate-General Budget, Accounting and Statistics, 1993). We retrieved the information on date of death and underlying cause-of-death (UCOD) for each deceased individual.
Selection of cases and controls
Between 1997 and 2007, totally 500 Taiwanese adolescents aged 15-19 (307 males, 193 females) died of suicide (International Classification of Disease 9th version Clinical Modification (ICD-9-CM): E950-E959) and registered in the TMR. These death records were unselected and were then linked, using individual’s scrambled personal identification number (PIN), to the 1978- 1992 TBR, searching for the birth records of these deceased adolescents. All suicidal cases were successfully linked and were served as cases of this case-control analysis nested within Taiwan’s adolescent population aged 15-19. The age-specific number of cases who died at each age of 15 to 19 was 39, 63, 88, 138, and 172, respectively. There was no significant (p=0.351) difference in
age distribution between male and female cases at the time of suicidal death.
For each case, we randomly selected from the TBR, using individual matching, 30 control subjects who were of the same birth cohort as the case and were alive on the date of the case’
death. If a subject was selected more than once, only the first-time selection was retained, and the subsequent selections were replaced with another random selection until another eligible control was found.
Birth characteristics and family socioeconomic factors
For each case, we retrieved his/her information from TMR on PIN, date of birth, date of death, and underlying-cause-of-death (UCOD). We linked a case’s PIN to the TBR searching for his/her birth characteristics including sex, birth order, singleton/multiple births, gestational week, and birth weight. Information on various family socioeconomic factors was also retrieved from the TBR including location and urbanization level of residential districts, marital status of parents, parental ages and educational attainment at the time of delivery. The above information for controls was also obtained from the TBR. We also calculated the age difference of parents as a family socio-economic indicator ( Chen et al . 2010 ) .The level of urbanization was categorized according to the National Statistics of Regional Standard Classification (Hung & Rabin, 2009).
Information on the death of parents
The parent’s PINs were retrieved from TBR for both cases and controls. Parental deaths prior to the indexed date (i.e., date of a case’s death), if any, were identified by linking parental PINs to the TMR from 1978 to 2007. Once a parent was found to be deceased, the UCOD of the
deceased parent was recorded.
Statistical analysis
Both birth demographic characteristics and family socioeconomic factors were compared between cases and controls, and differences were tested using Pearson’s χ2 or Fisher’s exact statistic for categorical data, and using Student t-test with equal variance assumed for continuous data. Only the variables significantly different between cases and controls were included in the multivariate conditional logistic regression model to control for their potential confounding.
Using the multivariate conditional logistic regression model, we first analyzed the association of adolescent suicidal death with death of parents, with a particular interest in
examining the relative importance of parent’s death by suicide and death by other causes on risk of adolescent completed suicide. Second, we used two separate models to investigate the
association of male offspring suicidal death with the suicidal death of his father or mother (i.e., father-son and mother-son dyads), as well as the association of female offspring suicidal death with the suicidal death of her father or mother (i.e., father-daughter and mother-daughter dyads) . We used the method proposed by Breslow and Day (1980) to test the heterogeneity between odds ratio s ( ORs) of offspring completed suicide in relation to suicidal and other causes, as well as between ORs of offspring completed suicide associated with paternal and maternal deaths . Similar method was also employed to test the heterogeneity of ORs between father-son and mother-son dyads, as well as between father-daughter and mother-daughter dyads. A p-value of
<0.05 was considered statistically significant, and all analyses were performed with SAS (version 9.1; SAS institute, Cary, NC). Access to the vital statistics data was approved by the Department
of Health. This study was exempt from Institutional Review as all individual’s PIN was encrypted while data linkage was performed.
RESULTS
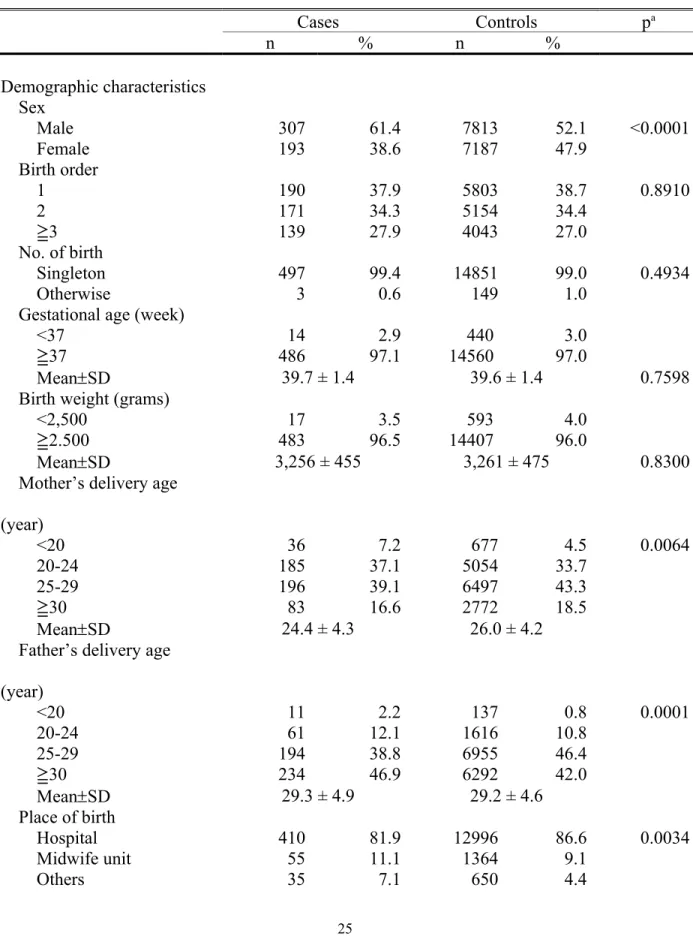
Cases and controls differed in a number of demographic characteristics and social factors.
More males were in cases than in controls (61.4% vs 52.1%). Mothers of cases tended to be significantly younger, and the proportions of younger (<20 years) (2.2% vs 0.8%) and older (>=30 years) (46.9% vs 42.0%) fathers were higher in cases than in controls. Additionally, significantly less proportion of cases than that of controls were born in hospitals (81.9% vs 86.6%) and delivered by physicians (80.9% vs 86.2%). The age difference of parents tended to be greater in cases than in controls. While there was no significant difference in the distribution of maternal education at the time of delivery between cases and controls, the education level was significantly higher in fathers of cases (Table 1).
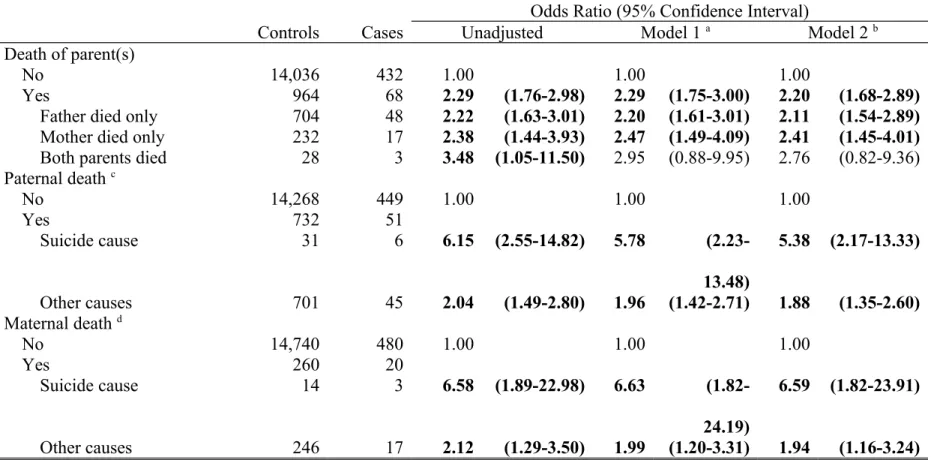
Table 2 shows OR and 95% confidence interval (CI) of adolescent’s completed suicide in relation to prior history of deaths of parents. After controlling for potential confounders,
significantly increased ORs were observed in the study subjects with paternal or maternal death (OR=2.20, 95% CI=1.68 to 2.89), paternal death only (OR=2.11, 95% CI=1.54 to 2.89), and maternal death only (OR=2.41, 95% CI=1.45 to 4.01). An increased but insignificant OR (2. 76, 95% CI=0.82 to 9.36 ) was also observed for death of both parents. After adjustment for birth characteristics and social factors, we noted a stronger association of completed suicide in adolescents with paternal death by suicide (OR=5.38, 95% CI=2.17 to 13.33) than with paternal death by non-suicidal causes (OR=1.88, 95% CI=1.35 to 2.60) ( p =0.0152) . Similar findings were
observed for the association of offspring completed suicide with maternal death (OR=6.59, 95%
CI=1.82 to 23.91 vs OR=1.94, 95% CI=1.16 to 3.24), but the difference in ORs reached no statistical significance ( p =0.0841 ) . In addition, maternal death by suicide conveyed slightly higher , but insignificant ( p =0.9309), risk for offspring suicide than did paternal death by suicide (OR=6.59 vs OR=5.38) .
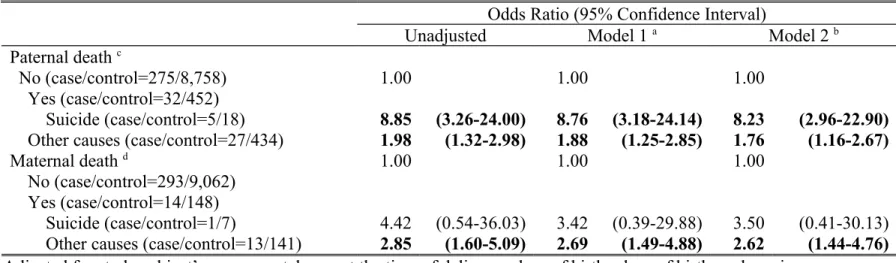
Taking further consideration of offspring gender, analyses were first limited to male cases and their corresponding controls. We noted that male offspring’s death by suicide was
substantially and significantly associated with prior history of paternal death by suicide
(OR=8.23, 95% CI=2.96 to 22.90) , but not with that of maternal death by suicide (OR= 3.50 , 95%
CI=
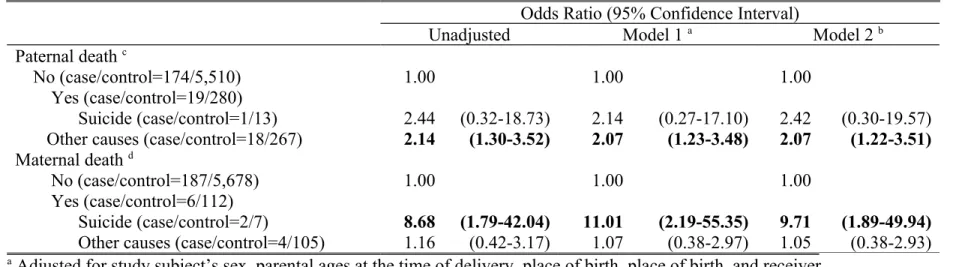
0.41 to 30.13 ) . (Table 3) For female offspring, on the other hand, their deaths by suicide were significantly and positively associated with prior history of maternal death (OR=9.71, 95%
CI=1.89 to 49.94), but not with that of paternal suicidal death (OR= 2.42 , 95% CI= 0.30 to 19.57 ) (Table 4). Despite the above differences of OR between father-son and mother-son dyads, and between father-daughter and mother-daughter dyads, the observed differences were not statistically significant with a p -value of 0.5527 and 0.3139, respectively.
DISCUSSION
Our research found that offspring completed suicide was significantly associated with prior history of maternal and paternal deaths, especially from suicide cause. Consistent with previous research (Qin et al. 2002;Sørensen et al. 2009;Agerbo et al. 2002; Garssen et al. 2011), our study also tended to suggest that offspring suicide risk associated more with maternal suicide than with paternal suicide. Despite a lack of significant difference , our study findings tended to suggest that a n offspring’s suicid al death was significantly and positively associated with prior history of suicidal death of his/her same-sex parent, but not with that of his/her opposite-sex parent .
Parental death is one of the most traumatic life events for child and adolescents. An early deprivation of parental care and also the changing environment associated with parental loss, such as economic hardship, inadequate care of surviving parent, might result in child
maladjustment (Kuramoto et al. 2009; Hung & Rabin, 2009). However, the impact of parental death of suicide on youth might be more traumatic and damaging than that of parental death of other causes. Past research found that the youth bereaved by parental suicide had higher risk of developing post-traumatic stress disorder, depression, anxiety, and suicidal behavior, compared to those bereaved by non-suicidal causes (Wilcox et al. 2009; Brent et al. 2010; Tsuchiya et al.
2005; Agerbo et al. 2002; Pfeffer et al.2000; Brent et al.1996). Huang and Rabin (2009)argued that suicide-bereaved children not only need to adjust to parental loss, but also need to make meaning of the self-directed nature of suicide in their parents. The grief process might be disastrous and enduring. Children bereaved by parental suicide usually undergo a devastating feeling of being abandoned, shame, self-blame, or hatred (Ratnarajah & Schofield, 2011). In
addition, the aftermath associated suicide, such as social stigma, the unspoken secret in the family, or social isolation, tend to make children’s adjustment particularly difficult. These all pose heightened risks for maladjustment.
The size of OR estimated in our research appeared to be relatively larger than that in past research. In the study by Agerbo et al. (2002), in which the age range of the participants was relatively comparable to that in our study, the covariate adjusted OR of youth suicide completion with maternal and paternal suicide completion was 4.75 and 2.30, respectively, while they were 6.59 and 5.38 in our study. The corresponding estimates in Qin et al. (2002) were even lower at 3.38 and 2.03. The heightened risk found in our study might be partially explained by our study’s inadequate adjustment for potential confounder such as familial psychiatric disorders. Besides, a wide confidence interval associated with the OR estimate noted in our study also limited the interpretation of the different ORs between previous studies and ours.
Our study suggested gender-specific risk associations between offspring completed suicide and history of parental deaths by suicide. Risk of completed suicide for female adolescents was significantly associated with maternal suicide, but not with paternal suicide. The opposite was true for male adolescents. In particular, after taking gender of offspring into consideration, the risk magnitude between parental and offspring suicides of the same-sex was much increased. On the contrary, the links between parent and children of the opposite-sex were reduced and no longer significant.
Buist et al. (2002) found that same-sex attachments generally were gre a ter than were
opposite-sex attachments, and that the level of attachment in both male and female adolescents to
their same-sex parent was similar during adolescence. Thus, a compromised relation with same- sex parent might likely be more destructive than that with opposite-sex parent. Israelashvili et al.
(2006) suggested that suicidal females were in lack of mothers as a positive role model to learn from her ways of coping. According to the social learning theory, imitative learning is augmented when the model is closely identified by the observers. A few studies implied that family
transmission of suicide may be a result of imitation (Mittendorfer-Rutz et al. 2008; Lieb et al.
2005; Burke et al.2010). As same-sex parent is usually the figure a child closely identifies with, the parent’s ways of coping, including self-harming behavior will be more readily imitated by his/her children. Thus, the association between parental and offspring suicides was only observed for same-sex dyads, but not for opposite-sex dyads. Findings of our study tended to support the hypothesis that attachment to the same-sex parents is of particular importance with regard of young suicide, while that to the opposite-sex parent is not.
Previous studies found that the familial transmission of suicide might be a result of imitation (Brent et al. 2005; Mittendorfer-Rutz et al. 2008; Lieb et al. 2005; Burke et al.2010). Past research, however, did not find this inquiry being sufficiently supported (Insel & Gould, 2008).
By indicating a significant risk link between parent-child dyads of the same-sex, our study tended to demonstrate that suicide modeling might occur with same-sex parent, with whom youth more closely identify. The same-sex parent could be an important source of identification for child and adolescents to develop a sense of self. The sameness between them also closely bonds each to the other. When children are bereaved by parental suicide in an early age, the misfortune will be more readily incorporated into their personality and identity (Hung & Rabin, 2009; Ratnarajah &
Schofield, 2011). Thus, there might be a strong tendency for child and adolescents to model
same-sex parents’ ways of problem-solving, including self-killing, when they encounter life hardship. Still, more research is needed to see if the findings could be reproduced with samples from other countries and other type of suicidal behavior, such as suicidal attempt.
There are several methodological strengths in our study. First, this study used a nationwide population based registry data, which ensures the representativeness of the study subjects.
Additionally, linkage between birth and death registries also effectively reduces the likelihood of sample attribution, which provides reassurance of limited selection bias. Moreover, we used the nested case-control design, which further provides reassurance for a limited likelihood of selection bias. Second, the study sample consisted of 500 cases of suicidal cases and 1,500 controls, which makes it possible for performing detailed sex-stratifications. Thirdly, most of the previous research probed for suicidal ideations and attempts. Our research reported that the impact of parental death on adolescents could be as deleterious as suicide completion. Such information is of great public health implication as suicidal death in adolescent can cost a great loss of years of potential life and economic loss.
Despite the above strengths, several limitations should be mentioned here. First, we were unable to control for psychiatric histories of participants and their parents. Statham et al. (1998) argued that the r isk of persistent suicidal thoughts and attempts is determined by a complex interplay of psychiatric history, neuroticism, traumatic life experiences, genetic vulnerability specific for suicidal behavior and socio-cultural risk or protective factors. In addition, the study by
Sørensen et al . (2009) showed that parental history of suicide is a risk factor for suicide in offspring, but primarily in offspring without psychiatric hospitalization. Past research suggested that familial psychiatric history was associated with family socio-economic factors; and the risk
of familial psychiatric history was associated with increased poverty in the families (Agerbo et al. 2002). Since our research did control for family socio-economic factors, the potential influences of psychiatric history had been partially controlled for. Inadequate adjustment for potential confounding by study subject’s psychiatric disorder might result in overestimation of the relationship between offspring completed suicide and parent’s suicide by death. Second, our study noted a lack of significant association of completed suicide in female offspring with paternal death by suicide, as well as a lack of significant association of completed suicide in male offspring with maternal death by suicide, which are likely to be caused by very limited sample size in those gender-specific analyses. In fact, there was only one male suicide case whose mother also died by suicide; and there was only one female suicide case whose father died by suicide. Third, because the study findings were entirely based on birth and death registries, we are not aware whether the parents were together with the children at the time of suicide; it might be possible that if the father was out of the child's life that his suicide would have less impact.
Additionally, some adolescents might have witnessed the suicide personally; some might just have been told; and some might never have been told that their parents died from suicide. A lack of detailed information on the scene of suicide makes it very difficult to assess the intensity of exposure of parental suicide on their offspring. Another limitation is that findings of risk links between parent-child dyads are only true for completed suicide.
This study extends our knowledge of the familial transmission of suicide by exploring associations of adolescent completed suicide with paternal and maternal death by suicide separately in an Asian country. Risk of completed suicide in adolescents was positively associated with parental death, especially the death by suicide. One of the potential novel
contributions by our study is that our data tended to reveal that familial transmission of suicide completion was true only for same-sex parent-child dyads, suggesting that same-sex
identification and modeling as well as same-sex parental bonding might play crucial roles in explaining the associations between parental suicide and adolescent completed suicide.
Nonetheless, firmed conclusion about the above-mentioned relationships was limited due to small sample size in the stratified analyses. Future studies with larger sample sizes would help elucidate whether the familial transmission of completed suicide for same-sex parent-child dyads truly exist. If it indeed exists, more attention needs to be paid to identification and modeling issues in designing suicide prevention and treatment plans for adolescents. In particular, child or adolescents who lost the same-sex parent to suicide need to receive particular attention, since a heighted risk of suicide modeling is likely to occur with them.
REFERENCES
Abdelnoor, A. & Hollins, S. (2004). The effect of childhood bereavement on secondary school performance. Educational Psychology in Practice 20, 43-54.
Agerbo, E., Nordentoft, M. & Mortensen, P.B. (2002). Familial, psychiatric, and socioeconomic risk factors for suicide in young people: nested case-control study. British Medical Journal 325, 74.
Brent, D.A., Melhem, N., Donohoe, M.B., Walker, M. (2009). The incidence and course of depression in bereaved youth 21 months after the loss of a parent to suicide, accident, or sudden natural death. American Journal of Psychiatry 166,786-794
Brent, D.A. & Melhem, N. (2008). Familial transmission of suicidal behavior. The Psychiatric Clinics of North America 31,157-177.
Brent, D.A. & Mann. J.J. (2005). Family genetic studies, suicide, and suicidal behavior.
American Journal of Medical Genetics. Part C, Seminars in Medical Genetics 133C, 13–
24..
Brent, D.A., Moritz, G., Bridge, J., Perper, J. & Canobbio, R. (1996). Long-term impact of exposure to suicide: a three-year controlled follow-up. Journal of the American Academy of Child and Adolescent Psychiatry 35, 646-653.
Bandura, A. (1975). Social Learning and Personality Development. Holt, Rinehart & Winston:
New York.
Thompson, R.B., Cothran, T. & McCall, D. (2012) Gender and age effects interact in
preschoolers' help-seeking: evidence for differential responses to changes in task difficulty. Journal of Child Language 39:1107-1120.
Buist, K.L., Deković, M., Meeus, W. & van Aken, M.A. (2004). The reciprocal relationship between early adolescent attachment and internalizing and externalizing problem behaviour. Journal of Adolescence 27:251-266.
Burke, A.K., Galfalvy, H., Everett, B., Currier, D., Zelazny, J., Oquendo, M.A., Melhem, N.M., Kolko, D., Harkavy-Friedman, J.M., Birmaher, B., Stanley, B., Mann, J.J. & Brent, D.A.
(2010). Effect of exposure to suicidal behavior on suicide attempt in a high-risk sample of offspring of depressed parents. Journal of the American Academy of Child and
Adolescent Psychiatry 49,114-121.
Cerel, J., Fristad, M.A., Weller, E.B. & Weller, R.A. (1999). Suicide-bereaved children and adolescents: A controlled longitudinal examination. Journal of the American Academy of Child and Adolescent Psychiatry 38, 672-679.
Chen CW, Tsai CY, Sung FC, Lee YY, Lu TH, Li CY, Ko MC. (2010). Adverse birth outcomes among pregnancies of teen mothers: age specific analysis of national data in Taiwan.‐ Child: Care, Health and Development 36, 232-240.
Directorate-General Budget, Accounting and Statistics. (1993). National Statistics of Regional
Standard Classification Data from Directorate-General Budget. Accounting and Statistics: Taipei, Taiwan
Garssen, J., Deerenberg, I., Mackenbach, J.P., Kerkhof, A. & Kunst, A.E. (2011). Familial risk of early suicide: variations by age and sex of children and parents. Suicide & Life-
threatening Behavior 41, 585-593.
Hung, N.C. & Rabin, L.A. (2009). Comprehending childhood bereavement by parental suicide: A critical review of research on outcomes, grief processes, and interventions. Death Studies 33,781-814.
Israelashvili, M., Gilad-Osovitzki, S. & Asherov, J. (2006). Female adolescents’ suicidal behavior and mothers’ ways of coping. Journal of Mental Health 15, 533-542.
Insel, B.J. & Gould, M.S. (2008). Impact of modeling on adolescent suicidal behavior. The Psychiatric Clinics of North America 31, 293-316.
Kim, C.D., Seguin, M., Therrien, N., Riopel, G., Chawky, N., Lesage, A.D. & Turecki, G.
(2005). Familial aggregation of suicidal behavior: a family study of male suicide completers from the general population. Am J Psychiatry 162:1017-1019.
Kuramoto, S.J., Stuart, E.A., Runeson, B., Lichtenstein, P., Långström, N. & Wilcox, H.C.
(2010). Maternal or paternal suicide and offspring's psychiatric and suicide-attempt hospitalization risk. Pediatrics 126, e1026-1032.
Kuramoto, S.J., Brent, D.A. & Wilcox, H.C. (2009). The impact of parental suicide on child and
adolescent offspring. Suicide & Life-threatening Behavior 39,137-151.
Lawrence, E., Jeglic, E.L., Matthews. L.T., & Pepper, C.M. (2005-2006). Gender differences in grief reactions following the death of a parent. Omega: Journal of Death and Dying 52, 323-337.
Lieb, R., Bronisch, T., Höfler, M., Schreier, A. & Wittchen, H.U. (2005). Maternal suicidality and risk of suicidality in offspring: findings from a community study. American Journal of Psychiatry 162, 1665-1671.
Lin, C.M., Lee, P.C., Teng, S.W., Lu, T.H., Mao, I.F. & Li, C.Y. (2004). Validation of the Taiwan birth registry using obstetric records. Journal of Formosan Medical Association 103, 297-301.
Lu, T.H., Lee, M.C. & Chou, M.C. (2000). Accuracy of cause-of death coding in Taiwan: types of miscoding and effects on mortality statistics. International Journal of Epidemiology 29, 336-343.
McGarvey, E.L., Kryzhanovskaya, L.A., Koopman, C., Waite, D & Canterbury, R.J. (1999).
Incarcerated adolescents' distress and suicidality in relation to parental bonding styles.
Crisis 20,164-170.
Melhem, N.M., Walker, M., Moritz, G. & Brent, D.A. (2008). Antecedents and sequelae of sudden parental death in offspring and surviving caregivers. Archives of Pediatrics and Adolescent Medicine 162, 403-410.
Mittendorfer-Rutz, E., Rasmussen, F. & Wasserman, D. (2008). Familial clustering of suicidal behaviour and psychopathology in young suicide attempters. Social Psychiatry and Psychiatric Epidemiology 43, 28-36.
Pfeffer, C.R., Karus, D., Siegel, K. & Jiang, H. (2000). Child survivors of parental death from cancer or suicide: depressive and behavioral outcomes. Psychooncology 9,1-10.
Qin, P., Agerbo, E. & Mortensen, P.B. (2002). Suicide risk in relation to family history of completed suicide and psychiatric disorders: a nested case-control study based on longitudinal registers. Lancet 360, 1126–1130.
Ratnarajah, D. & Schofield, M.J. (2011). Survivors' narratives of the impact of parental suicide.
Suicide & Life-Threatening Behavior 38,618-630.
Runeson, B. & Åsberg, M. (2003). Family history of suicide among suicide victims. American Journal of Psychiatry 160, 1525-1526.
Russell, A. & Saebel, J. (1997). Mother–son, mother–daughter, father–son, and father–daughter:
Are they distinct relationships? Developmental Review 17,111-147.
Sørensen, H.J., Mortensen, E.L., Wang, A.G., Juel, K., Silverton, L. & Mednick, S.A. (2009).
Suicide and mental illness in parents and risk of suicide in offspring. Social Psychiatry and Psychiatric Epidemiology 44, 748-751.
Statham, D.J., Heath, A.C., Madden, P.A., Bucholz, K.K., Bierut, L., Dinwiddie, S.H., Slutske, W.S., Dunne, M.P. & Martin, N.G. (1998). Suicidal behaviour: an epidemiological and
genetic study. Psychological Medicine 28, 839-855.
Steinberg, L. (1987). Recent research on the family at adolescence: The extent and nature of sex differences. Journal of Youth and Adolescence 16,191-197.
Tsuchiya, K.J., Agerbo, E. & Mortensen, P.B. (2005). Parental death and bipolar disorder: a robust association was found in early maternal suicide. Journal of Affective Disorders 86, 151-159.
Wilcox, H.C., Kuramoto, S.J., Lichtenstein, P., Långström, N., Brent, D.A. & Runeson, B.
(2010). Psychiatric morbidity, violent crime, and suicide among children and adolescents exposed to parental death. Journal of the American Academy of Child and Adolescent Psychiatry 49, 514-523.
Washburn, M. (1994). Reflections on a psychoanalytic theory of gender difference. The journal of the American Academy of Psychoanalysis and Dynamic Psychiatry 22, 1-28.
Table 1. Characteristics of cases and controls
Cases Controls pa
n % n %
Demographic characteristics Sex
Male 307 61.4 7813 52.1 <0.0001
Female 193 38.6 7187 47.9
Birth order
1 190 37.9 5803 38.7 0.8910
2 171 34.3 5154 34.4
≧3 139 27.9 4043 27.0
No. of birth
Singleton 497 99.4 14851 99.0 0.4934
Otherwise 3 0.6 149 1.0
Gestational age (week)
<37 14 2.9 440 3.0
≧37 486 97.1 14560 97.0
MeanSD 39.7 ± 1.4 39.6 ± 1.4 0.7598
Birth weight (grams)
<2,500 17 3.5 593 4.0
2.500
≧ 483 96.5 14407 96.0
MeanSD 3,256 ± 455 3,261 ± 475 0.8300
Mother’s delivery age (year)
<20 36 7.2 677 4.5 0.0064
20-24 185 37.1 5054 33.7
25-29 196 39.1 6497 43.3
≧30 83 16.6 2772 18.5
MeanSD 24.4 ± 4.3 26.0 ± 4.2
Father’s delivery age (year)
<20 11 2.2 137 0.8 0.0001
20-24 61 12.1 1616 10.8
25-29 194 38.8 6955 46.4
≧30 234 46.9 6292 42.0
MeanSD 29.3 ± 4.9 29.2 ± 4.6
Place of birth
Hospital 410 81.9 12996 86.6 0.0034
Midwife unit 55 11.1 1364 9.1
Others 35 7.1 650 4.4
Delivered by
Physician 403 80.9 12930 86.2 0.0001
Midwife 87 17.5 1995 13.3
Others 10 1.6 75 0.5
Socioeconomic factorsb Marital status of parents
Married 498 99.6 14989 99.9 0.0642
Otherwise 2 0.4 11 0.1
Urbanization of residence
Metropolis 171 34.2 4656 31.0 0.2647
Satellite city 153 30.6 4623 30.8
Rural area 176 35.2 5721 38.1
Age difference of parents
≦1 128 25.7 4089 27.3 <0.0001
>1-3 113 22.6 4475 29.9
>3-5 114 22.8 3405 22.7
>5 145 28.9 3031 20.2
Maternal education
Elementary or less 194 38.8 5688 37.9 0.1655
Junior high 141 28.2 3699 24.7
Senior high 126 25.2 4272 28.5
College or more 39 7.8 1341 8.9
Paternal education
Elementary or less 182 36.4 4342 28.9 0.0044
Junior high 114 22.8 3747 25.0
Senior high 130 26.0 4453 29.7
College or more 74 14.8 2458 16.4
Total 500 100.0 15000 100.0
a Based on χ2 test, Fisher’s exact test, or two-independent t test.
b Based on the information of birth registry.
Table 2. Odds ratio of adolescent completed suicide in relation to prior history of parental death
Odds Ratio (95% Confidence Interval)
Controls Cases Unadjusted Model 1 a Model 2 b
Death of parent(s)
No 14,036 432 1.00 1.00 1.00
Yes 964 68 2.29 (1.76-2.98) 2.29 (1.75-3.00) 2.20 (1.68-2.89)
Father died only 704 48 2.22 (1.63-3.01) 2.20 (1.61-3.01) 2.11 (1.54-2.89)
Mother died only 232 17 2.38 (1.44-3.93) 2.47 (1.49-4.09) 2.41 (1.45-4.01)
Both parents died 28 3 3.48 (1.05-11.50) 2.95 (0.88-9.95) 2.76 (0.82-9.36)
Paternal death c
No 14,268 449 1.00 1.00 1.00
Yes 732 51
Suicide cause 31 6 6.15 (2.55-14.82) 5.78 (2.23-
13.48)
5.38 (2.17-13.33)
Other causes 701 45 2.04 (1.49-2.80) 1.96 (1.42-2.71) 1.88 (1.35-2.60)
Maternal death d
No 14,740 480 1.00 1.00 1.00
Yes 260 20
Suicide cause 14 3 6.58 (1.89-22.98) 6.63 (1.82-
24.19)
6.59 (1.82-23.91)
Other causes 246 17 2.12 (1.29-3.50) 1.99 (1.20-3.31) 1.94 (1.16-3.24)
a Adjusted for study subject’s sex, parental ages at the time of delivery, place of birth, and receiver.
b Adjusted for the selected variables included in Model 1 and familial socioeconomic factors including urbanization of residence at birth, parental educational level, and age difference of parents.
c Additional adjustment for maternal death in both Model 1 and 2.
d
Table 3. Odds ratio of male adolescent completed suicide in relation to prior history of parental death Odds Ratio (95% Confidence Interval)
Unadjusted Model 1 a Model 2 b
Paternal death c
No (case/control=275/8,758) 1.00 1.00 1.00
Yes (case/control=32/452)
Suicide (case/control=5/18) 8.85 (3.26-24.00) 8.76 (3.18-24.14) 8.23 (2.96-22.90) Other causes (case/control=27/434) 1.98 (1.32-2.98) 1.88 (1.25-2.85) 1.76 (1.16-2.67)
Maternal death d 1.00 1.00 1.00
No (case/control=293/9,062) Yes (case/control=14/148)
Suicide (case/control=1/7) 4.42 (0.54-36.03) 3.42 (0.39-29.88) 3.50 (0.41-30.13) Other causes (case/control=13/141) 2.85 (1.60-5.09) 2.69 (1.49-4.88) 2.62 (1.44-4.76)
a Adjusted for study subject’s sex, parental ages at the time of delivery, place of birth, place of birth, and receiver.
b Adjusted for the selected variables included in Model 1 and familial socioeconomic factors including urbanization of residence at birth, parental educational level, and age difference of parents.
c Additional adjustment for maternal death in both Model 1 and 2.
d Additional adjustment for paternal death in both Model 1 and 2.
Table 4. Odds ratio of female adolescent completed suicide in relation to prior history of parental death Odds Ratio (95% Confidence Interval)
Unadjusted Model 1 a Model 2 b
Paternal death c
No (case/control=174/5,510) 1.00 1.00 1.00
Yes (case/control=19/280)
Suicide (case/control=1/13) 2.44 (0.32-18.73) 2.14 (0.27-17.10) 2.42 (0.30-19.57) Other causes (case/control=18/267) 2.14 (1.30-3.52) 2.07 (1.23-3.48) 2.07 (1.22-3.51) Maternal death d
No (case/control=187/5,678) 1.00 1.00 1.00
Yes (case/control=6/112)
Suicide (case/control=2/7) 8.68 (1.79-42.04) 11.01 (2.19-55.35) 9.71 (1.89-49.94) Other causes (case/control=4/105) 1.16 (0.42-3.17) 1.07 (0.38-2.97) 1.05 (0.38-2.93)
a Adjusted for study subject’s sex, parental ages at the time of delivery, place of birth, place of birth, and receiver.
b Adjusted for the selected variables included in Model 1 and familial socioeconomic factors including urbanization of residence at birth, parental educational level, and age difference of parents.
c Additional adjustment for maternal death in both Model 1 and 2.
d Additional adjustment for paternal death in both Model 1 and 2.