For Peer Review
Single-Incision Laparoscopic versus Conventional Laparoscopic right hemicolectomy: A Comparison of Short-
term Surgical Results
Journal: Surgical Endoscopy Manuscript ID: SEND-10-0608 Manuscript Type: Original Article Date Submitted by the
Author: 22-May-2010
Complete List of Authors: Chen, William; China Medical University Hospital, Colorectal Surgery
Chang, Sheng-Chi; China Medical University Hospital, Colorectal Surgery
Wu, Christina; China Medical University Hospital, Colorectal Surgery Chiang, Hua-Che; China Medical University Hospital, Colorectal Surgery
Cheng, Long-Bin; China Medical University Hospital, Surgery Ke, Tao-Wei; China Medical University Hospital, Colorectal Surgery Please specify the country
from which you are submitting your manuscript.:
Taiwan, Province of China
Keyword: Colorectal < Cancer, Surgical < Technical, Bowel
For Peer Review
Single-Incision Laparoscopic versus Conventional Laparoscopic right hemicolectomy: A Comparison of Short-term Surgical Results
William Tzu-Liang Chen, Sheng Chi Chang, Hua Che Chiang, Christina Wu, Long-Bin Cheng, Tao Wei Ke,
Division of Colorectal Surgery, Department of Surgery Center of Minimally Invasive Surgery
China Medical University Hospital, China Medical University, Taichung, Taiwan
Corresponding author:
Tao-Wei Ke, MD
Address: No.2, Yu-Der Road, Taichung 404, Taiwan TEL:0966202253,+886-4-22052121-1638
Fax:+886-4-22029083 Original article
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Abstract
Background: Since the introduction of laparoscopic colectomy, improved short-term surgical results have been noted in other literature. Therefore, the current focus shifted to reducing the invasiveness of laparoscopic surgery, resulting in the invention of single incision laparoscopic surgery (SILS). Due to its comparable capabilities and feasibility, the
implementation of SILS has been rapidly growing in different fields. However, few studies discuss its true benefit compared to conventional laparoscopy. This study is the first to use SILS colectomy as an approach for malignant colon cancer. The aim of this cohort series is to compare the short-term surgical outcomes between SILS and conventional right
hemicolectomy.
Methods: This was a case control study comparing SILS right hemicolectomy patients
to traditional laparoscopic right hemicolectomy. The inclusion criteria were only ascending colon cecal lesions. Cases of obstruction or perforation required emergent operation or previous abdominal surgery were excluded. These patients were specifically matched in regard of patient’s age, gender, perioperative condition, surgical indication and tumor size.
No consideration or analysis of operative parameters and outcomes was made until this group was definitively selected as the best comparison cohort based on preoperative variables only.
Results: A total of 18 patients were included for SILS and the other 21 patients were completed by conventional laparoscopic right hemicolectomy. The SILS and traditional laparoscopic groups were similar in regard to age, gender, BMI, and perioperation outcomes.
Initial oncologic results were no different including equal length of distal cut margin,
numbers of harvested lymph nodes, and TMN stage. Three patients SILS colectomy group were converted (16.6%), and no conversion in the traditional laparoscopic colectomy group.
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Conclusion: Our preliminary experience with SILS right hemicolectomy demonstrated the safety of the procedure and its feasibility in malignant colon cancer. Although SILS right hemicolectomy may provide a subjective cosmetic advantage, there was no benefit in the short-term surgical outcomes. SILS is very situational, requires more effort from the surgeon, and may not offer more patient comfort. More experience with SILS and prospective trials would be needed to validate it as a more favorable alternative to conventional laparoscopic colectomy.
Key words: Single incision, Laparoscopy, right hemicolectomy, Short-term surgical results, Oncologic results, Scarless
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Introduction
The first laparoscopic colectomy was reported by Moises Jacobs et al[1] almost two decade ago. Laparoscopic colectomy has been an alternative method to open colectomy ever since.
Currently, several prospective randomized trials have shown its benefits in postoperation
outcomes, including improved pain management, faster return of bowel function, shortening of hospital stay, cosmesis, and most importantly, its equivalent effectiveness on long-term cancer outcome[2-5]. Despite its ameliorating effects, conventional laparoscopic colectomy still requires 3-6 abdominal incisions for completion of the procedure. Each incision carries potential morbidity risks from bleeding, hernia, or internal organ damage [6-7]. Current efforts have naturally shifted towards decreasing parietal trauma and visible scaring. As a result, single-port or single-incision laparoscopic surgery (SILS) has been introduced as an alternative to conventional laparoscopy.
The first SILS procedure was described in an appendectomy performed by Pelosi in 1992 [8]. This technique was quickly adapted and applied to other medical field such as gynecology, general surgery, and urology[9]. Despite its various applications, only a few SILS cases have been reported in the field of colorectal surgery. Reported benefits of SILS colectomy include better cosmesis, less postoperative pain, and faster postoperation recovery (leading to earlier discharge of the patient [10-11]. Thorough comparisons between the two approaches have yet to be made. Therefore, this study will analyze and compare the
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
short-term surgical results between SILS and conventional laparoscopic right hemicolectomy.
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Materials and Methods Patient selection
This prospective case-control study examined 39 patients with cancer of the right colon amenable to surgery. Indications for SILS right hemicolectomy include benign or malignant lesions of cecal and proximal ascending colon. Colonic obstruction, perforation, and history of abdominal surgery were contraindications for the procedure. SILS right hemicolectomy was approved by the Institutional Review Board (IRB) of China Medical Universtiy Hospital on November 11, 2009.
Prior to surgery, all patients undergoing SILS colectomy were informed that the procedure was minimally invasive and would be attempted via a single umbilical incision.
Patients were also informed of the possible additional incisions or trocar ports needed to complete the procedure, as well as the chance of conversion to a conventional laparoscopic or open colectomy. Advantages and disadvantages were reviewed to ensure that patients were fully educated about the procedure.
Patients who underwent traditional right hemicolectomies from August 2006 to
November 2007 were selected to serve as the control group for this study (n=21). The SILS right hemicolectomy group was formed by selected patients undergoing the procedure, all of which were completed by February 2010 (n=18). Patients were specifically matched with respect to patient’s age, gender, surgical indication, intraoperative and postoperative
morbidity and mortality (within 30 days from surgery), operative time, estimated blood loss,
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
length of incision, conversion rate and length of postoperative narcotic used, return of bowel function, length of hospital stay, and initial oncologic features including, size of the tumor, distal free margin, number of lymph node harvest, and pathologic TMN stage. No
consideration or analysis of operative parameters and outcomes was made until this group was definitively selected as the best comparison cohort based on preoperative variables only.
Surgical technique
The operative techniques for conventional laparoscopy and SILS right hemicolectomy were performed in a medial-to-lateral fashion and extracorporeal stapled functional
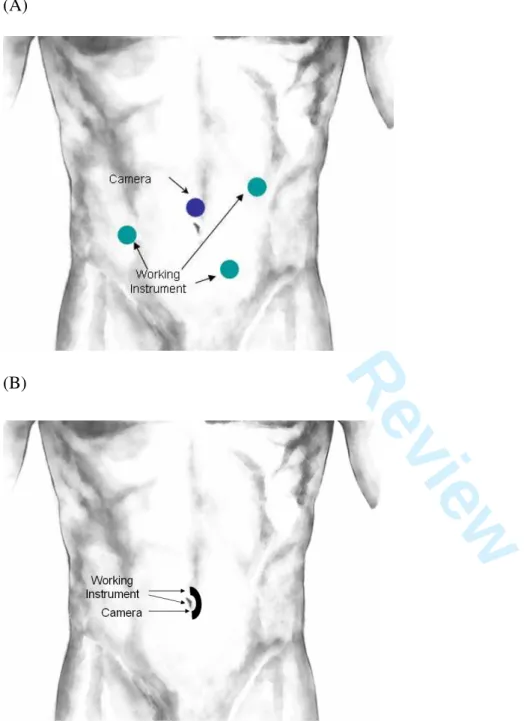
end-to-end ileocolic anastomosis, despite being conducted through different port placement methods. For conventional laparoscopy, we utilized four ports. After the first supraumbilical 12 mm trocar was inserted as a camera port, the other three 5 mm trocars were placed
respectively in the right lower abdominal quadrant, the lower abdominal midline 4 cm above the pubic synthesis, and the left lower quadrant, all under laparoscopic guidance (Figure 1A).
For the SILS right hemicolectomy, a 3 cm periumbilical incision was made and deepened to the level of fascia (Figure 1B). Pneumoperitoneum was induced by use of a Veress needle and maintained at 12 mmHg with carbon dioxide. A 5 mm trocar was introduced at the middle of wound to initially explore the abdominal cavity with a rigid 5 mm 30° angled laparoscope. Subsequently, another two 5 mm trocars were placed through the same
periumbilical access at the bilateral pole of the same wound. Distance between trocars were kept as far as possible and the adjacent three trocars should were kept at different heights to reduce crowding (Figure 2A).
Traditional laparoscopic instruments were used for SILS and conventional laparoscopic colectomy. The only difference was the use of a 5 mm 30° angled laparoscopy instead of a 10
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
mm 30° angled laparoscopy. In order to perform the procedure with a medial-to-lateral approach, the ileocolic pedicle was exposed with retraction of the ileocolic junction by rigid grasper. Then, 5 mm laparoscopic monopolar scissors were used for mesocolic dissection and isolating the ileocolic vessels. The Ligasure device was used for vascular control. The entire ascending colon and terminal ileum were freed after complete mobilization of the right colon from the retroperitoneum, parietal peritoneal reflection, omentum and right-angle ligament by alternatively using laparoscopic monopolar scissor and the Ligasure device. During SILS colectomy, the three trocars in the camera and operator ports were alternated in order to achieve the best angle of vision and appropriate triangulation of the target area.
After mobilizing the entire right side colon, a small abdominal incision was made to extract the specimen. For conventional laparoscopy, the trocar wound was extended to a length comparable to the tumor size. For SILS colectomy, the three trocars were removed and the fascia layer opened via the same periumbilical wound. The wound retractor was set up through the small umbilical incision, maximizing exposure to allow easy specimen removal (Figure 2B). After extracorporeal ileocolic anastomosis, a surgical glove attached with three trocars was then fixed to the outer ring of the wound retractor (Figure 2C). This procedure enables re-establishment of the pneumoperitoneum, so that bleeders and bowel axis can be checked. Finally, the wound was closed by layers and the length of wound was measured (Figure 2D).
In this study, conversions were defined as any unplanned laparotomy at any time during the surgery or any procedure done through an unplanned incision. Also an addition trocar insertion or any procedure done through a hand port would be considered as a conversion as well. The indication and timing of conversion were all dependent on the surgeon’s judgment and experience.
Postoperatively, patients were offered a liquid diet soon after surgery, but no dietary
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
restrictions thereafter. Oral or intravenous narcotics were given as needed postoperatively pain control. Discharge criteria included tolerance of general meals without nausea or vomiting, absence of abdominal distention, and passage of flatus.
Statistics
Data were analyzed by using the χ² test for categorical values and the Mann-Whitney U test for continuous variables. Difference with a p-value of p < 0.05 was considered to be statistically significant.
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Results
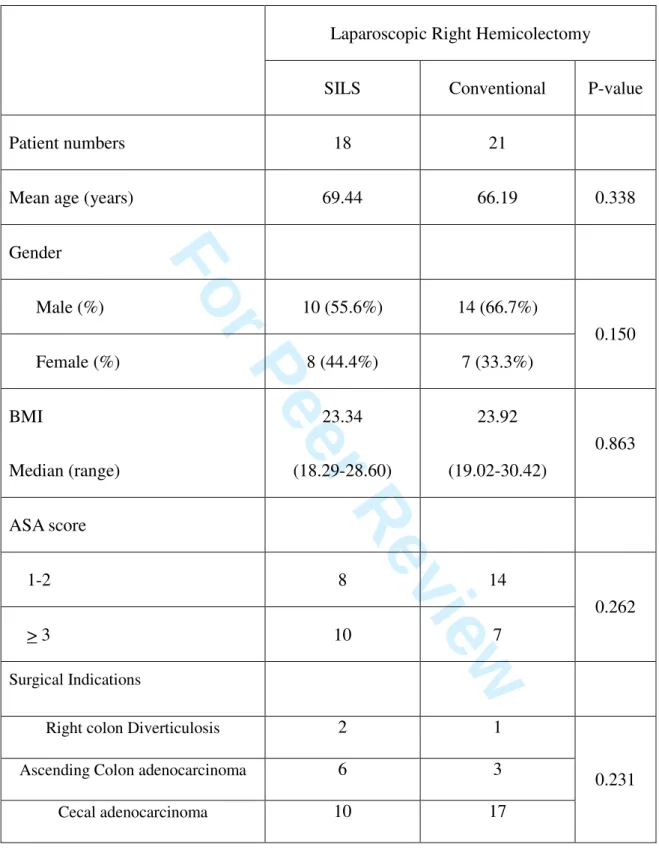
Of the 39 patients enrolled in the study, there were 15 females and 24 males which were distributed into two groups, SILS and conventional laparoscopic. As previously mentioned, all patients were matched as closely as possible in selection criteria. Data of the two patient groups can be seen in Table 1.
There was no operative mortality in either SILS or traditional right hemicolectomy groups.
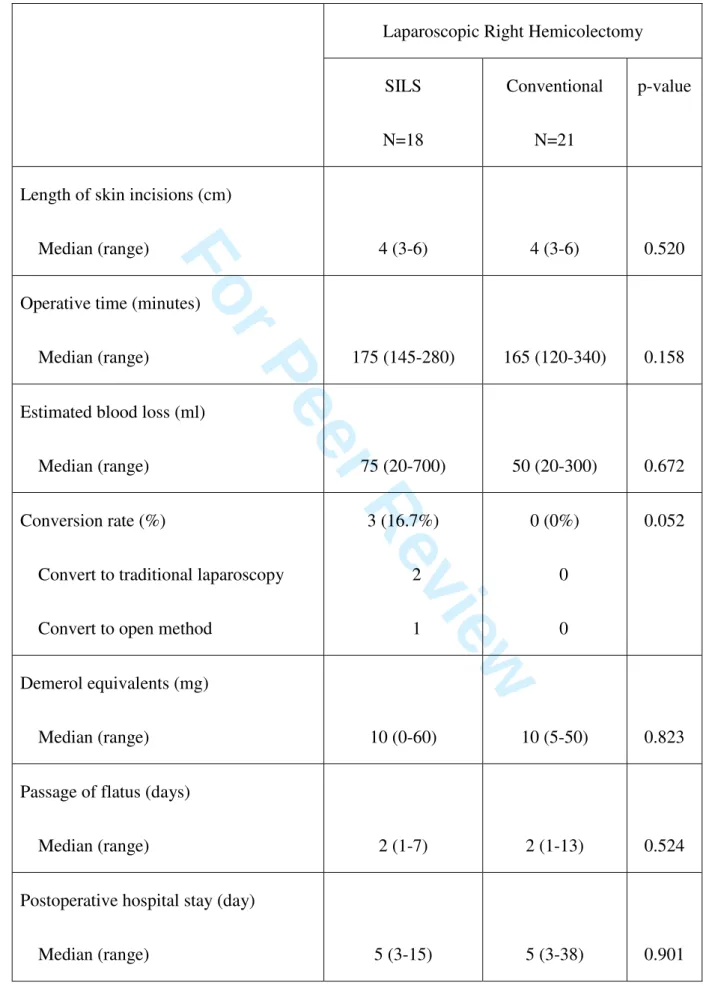
Operative time required was slightly longer in the SILS group compared to the traditional group 175 (145-280) minutes vs. 165 (120-340) minutes, but the differences are not
statistically significant. There was also no significant difference in median estimated blood loss between the two groups 75 (20-700) mL vs. 50 (20-300) mL. In the SILS group, there was one conversion to open surgery due to ielocolic artery bleeding, and two cases converted to traditional laparoscopic right hemicolectomy due to visceral obesity and thus unclear anatomy. There were no conversions in the tradition laparoscopy group. Analysis of
postoperative outcomes revealed no significant differences between the two groups (Table 2).
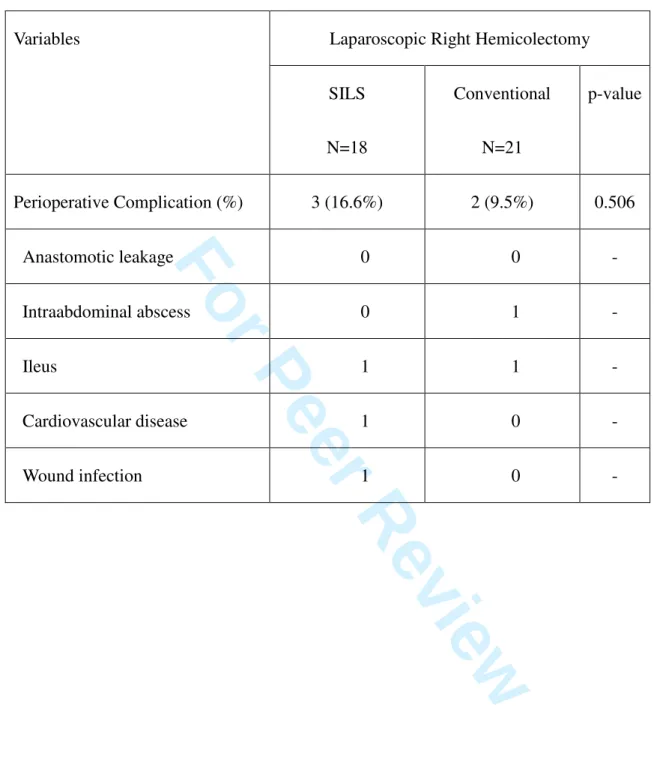
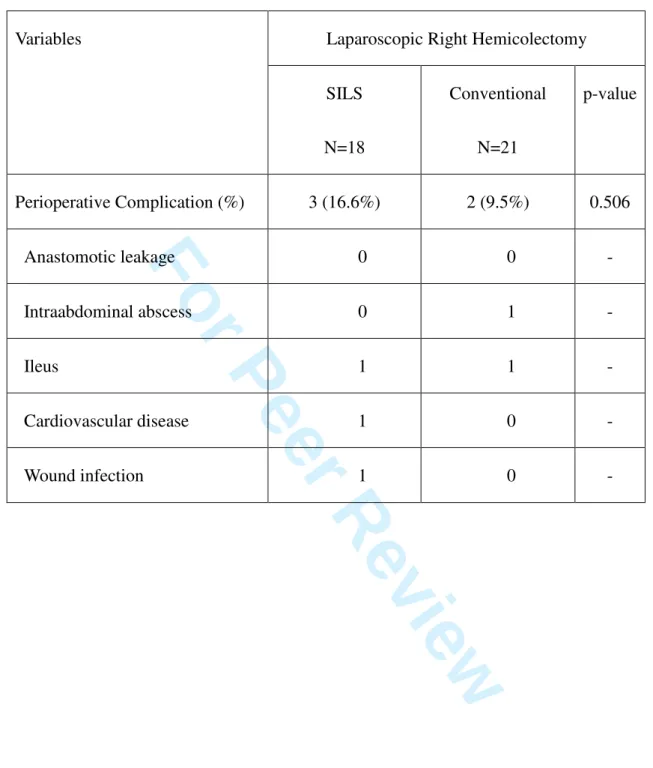
In regards to postoperative recovery, there were no differences observed in the usage of narcotics, time till flatus passage, and postoperative hospital stay. Three postoperative complications occurred in the SILS group and four in the conventional laparoscopic group;
overall complication rates were nearly equivalent in both groups 3 (16.6%) vs. 2 (9.5%), p = 0.506). In the SILS group, a total of three patient developed complications: one patient had a prolonged postoperative ileus, one developed postoperative arrhythmia, and one patient developed a postoperation wound infection. All three patients were successfully managed conservatively, and safely discharged from the hospital. In the traditional laparoscopic group, one patient developed intraabdominal abscess resulting of wound infection. This patient underwent with total parental nutrition, antibiotic therapy, and computer tomographic-guided abscess drainage. The patient was discharged 38 days after surgery. One other patient in the
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
conventional laparoscopic group developed postoperative ileus. Complete postoperative complications are listed in Table 3.
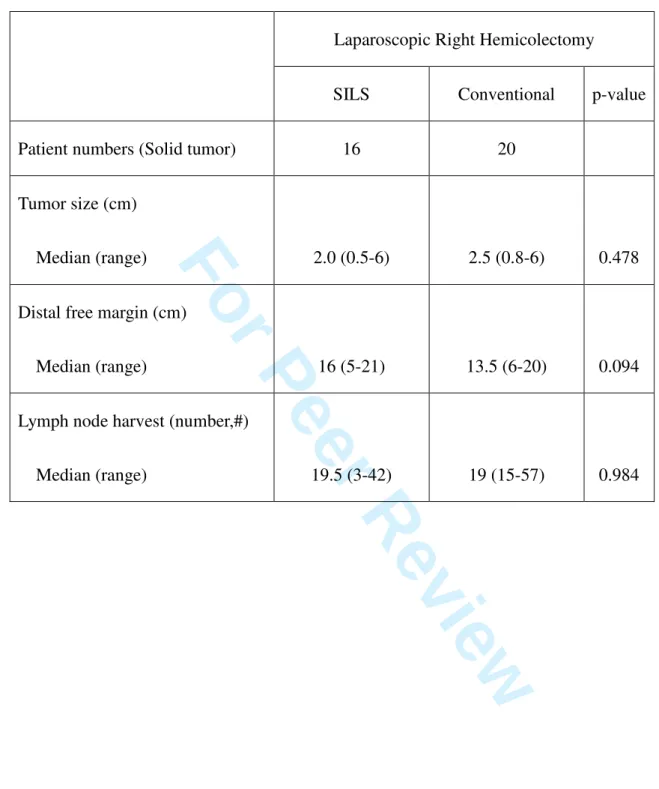
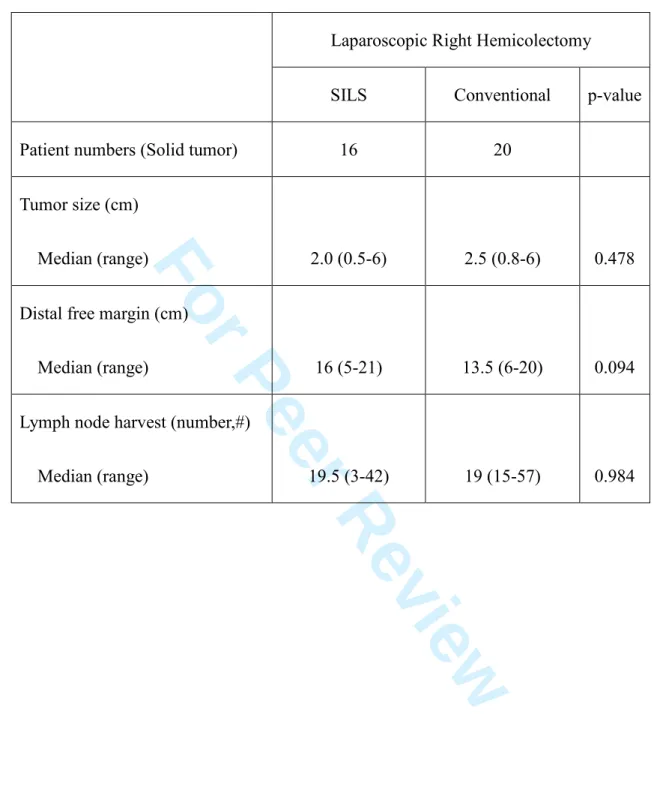
There were 16 cecal and proximal ascending colon cancers resected in the SILS group, matched with 20 cases that were previously done by traditional laparoscopic right
hemicolectomy. The initial oncological results also showed no difference in terms of tumor size, length of distal tumor-free margin, lymph nodes harvest, and TMN staging (Table.4).
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Discussion
Since the introduction of laparoscopy in the early 1990s, the minimal invasive technique has ushered in a new era of surgical treatment for diseases. A mere number of incisions are made for the port sites, yet each wound contributes to postoperative pain and potential risks of hemorrhage, hernia, or intraperitoneal organ injury. Reducing the invasiveness of
laparoscopic surgery would theoretically lower the rates of complications. Single-incision laparoscopy offers the wanted reductions in abdominal incisions and scarring while
maintaining low rates of morbidity. This is a homogenous study demonstrates the feasibility and comparable outcomes for right hemicolectomy, but it is imperative that we evaluate two questions: does SILS offer any benefits, aside from improved cosmesis, compared to
standard surgical techniques of laparoscopic right hemicolectomy? Could SILS replace the status of traditional laparoscopic surgery?
Our data revealed that all perioperative outcomes and short-term measures of
convalescence were equivalent between SILS and conventional laparoscopic colectomy. In this study SILS group did not have a reduction of postoperative pain and or shorten the time for bowel recovery as compare to traditional group. All the variants listed above were similar between the two methods and no obvious advantages from SILS colectomy were seen.
In the present study, SILS colectomy did not reduce the postoperative pain based on the number of narcotics used. This result was also demonstrated on the study of SILS
cholecystectomies by Merchant et al [12] and Stozenburg et al [13] on SILS nephrectomy.
Another limitation of SILS laparoscopic colectomy is that it requires a handpicked selection of patients. Visceral obesity was the primary cause of conversion in this study for SILS cases. Poor visualization of anatomic plane and require better surgical techniques.
Since BMI values may not serve as an accurate predictor of visceral obesity, abdominal CT
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
scans are suggested for future efforts in properly selecting patients for SILS colectomy and reducing the number of conversions [14].
The inherent technicality of SILS right hemicolectomy also proves to be an obstacle for expanding the usage of the procedure. Standard laparoscopic surgery may be done through multiple ports, allowing variation of scope placement and angling when met with
obstructions. In single-port surgery, no additional ports exist for placement of the scope and maneuvering is greatly restricted by nearby instruments. Therefore, SILS requires an
experienced surgeon to overcome the difficulties of triangulation, pneumoperitoneum leaks, and instrument crowding. Recent innovation of articulating instruments and devices had reduced the impact of spatial issues, but the main determinant of the SILS learning curve is adapting to the counterintuitive maneuvering that is required by the surgeon.
The learning curve of the technique may be improved by existing familiarity to general laparoscopy. Despite these improvements, compromising overall safety for minor cosmetic improvements still remains the biggest concern. The benefits reaped by SILS colectomy patients do not outweigh the procedural difficulties faced by the surgeon. Not only is the operative field greatly reduced, but also sustaining cumbersome positioning during the operation may lead to long-term physical discomfort for the surgeon.
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Conclusion
Our initial experience with SILS demonstrated its feasibility for right hemicolectomy. We also found that SILS was efficacious in patients with malignant cecal and ascending colon cancer, providing similar oncologic resection results as conventional laparoscopy. However, aside from the smaller length of incision, we noted no significant differences in perioperative outcomes or short-term measures of convalescence. The drawbacks of SILS include its usage being very situational, need for careful patient selection, and dependence on the surgeon’s ability to adapt to its unique scope setup.
In the end, SILS offers a subjective cosmetic advantage but its trade-offs make it a questionable alternative to conventional laparoscopy. Increasing case volume and prospective comparison between SILS and conventional laparoscopic colectomy may validate its true value and clearly define its ability to improve surgical outcomes. As for now, success and ease of the procedure are essential for patient comfort as well as avoiding complications.
These factors remain as the primary concern for surgeons, thus multiport laparoscopic colectomy is still the preferable option from our point of view.
Disclosure:
Dr. William Tzu-Liang Chen, Dr. Tao-Wei Ke, Dr. Sheng-Chi Chang, Dr. Hua-Che Chiang, Dr. Christina Wu, and Dr. Long-Bin Jeng, MD have no conflicts of interest or financial ties to disclose
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Reference
1. Jacobs M, Verdeja JC, Goldstein HS (1991) Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc 1:144-150
2. Milsom JW, Bohm B, Hammerhofer KA, Fazio V, Steiger E, Elson P (1998) A
prospective, randomized trial comparing laparoscopic versus conventional techniques in colorectal cancer surgery: a preliminary report. J Am Coll Surg 187:46-54;
discussion 54-45
3. Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM, Visa J (2002) Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 359:2224-2229
4. (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 350:2050-2059
5. Leung KL, Kwok SP, Lam SC, Lee JF, Yiu RY, Ng SS, Lai PB, Lau WY (2004) Laparoscopic resection of rectosigmoid carcinoma: prospective randomised trial.
Lancet 363:1187-1192
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
6. Lowry PS, Moon TD, D’Alessandro A, Nakada SY (2003) Symptomatic port-site hernia associated with a non-bladed trocar after laparoscopic live-donor nephrectomy.
J Endourol 17:493–494
7. Marcovici I (2001) Significant abdominal wall hematoma from an umbilical port insertion. JSLS 5:293–295
8. Pelosi MA, Pelosi MA, 3rd (1992) Laparoscopic appendectomy using a single umbilical puncture (minilaparoscopy). J Reprod Med 37:588-594
9. Canes D, Desai MM, Aron M, Haber GP, Goel RK, Stein RJ, Kaouk JH, Gill IS (2008) Transumbilical single-port surgery: evolution and current status. Eur Urol
54:1020-1029
10. Merchant AM, Lin E (2009) Single-incision laparoscopic right hemicolectomy for a colon mass. Dis Colon Rectum 52:1021-1024
11. Bucher P, Pugin F, Morel P (2009) Single-port access laparoscopic radical left colectomy in humans. Dis Colon Rectum 52:1797-1801
12. Merchant AM, Cook MW, White BC, Davis SS, Sweeney JF, Lin E (2009)
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Transumbilical Gelport access technique for performing single incision laparoscopic surgery (SILS). J Gastrointest Surg 13:159-162
13. Stolzenburg JU, Kallidonis P, Hellawell G, Do M, Haefner T, Dietel A, Liatsikos EN (2009) Technique of laparoscopic-endoscopic single-site surgery radical nephrectomy.
Eur Urol 56:644-650
14. Tsujinaka S, Konishi F, Kawamura YJ, Saito M, Tajima N, Tanaka O, Lefor AT (2008) Visceral obesity predicts surgical outcomes after laparoscopic colectomy for sigmoid colon cancer. Dis Colon Rectum 51:1757-1765; discussion 1765-1757
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
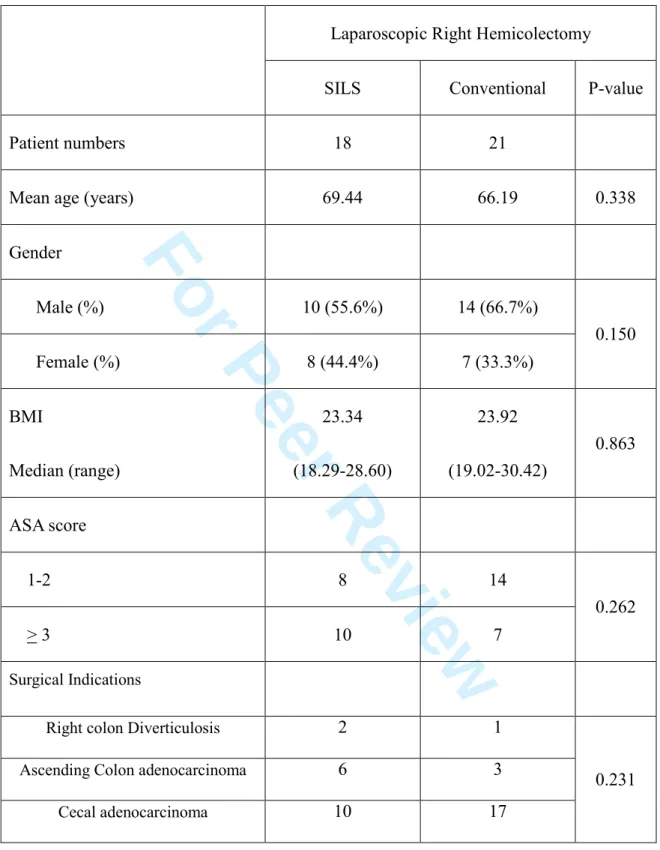
Table 1. Patient’s demographics
Laparoscopic Right Hemicolectomy
SILS Conventional P-value
Patient numbers 18 21
Mean age (years) 69.44 66.19 0.338
Gender
Male (%) 10 (55.6%) 14 (66.7%)
Female (%) 8 (44.4%) 7 (33.3%)
0.150
BMI
Median (range)
23.34 (18.29-28.60)
23.92 (19.02-30.42)
0.863
ASA score
1-2 8 14
> 3 10 7
0.262
Surgical Indications
Right colon Diverticulosis 2 1
Ascending Colon adenocarcinoma 6 3
Cecal adenocarcinoma 10 17
0.231
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
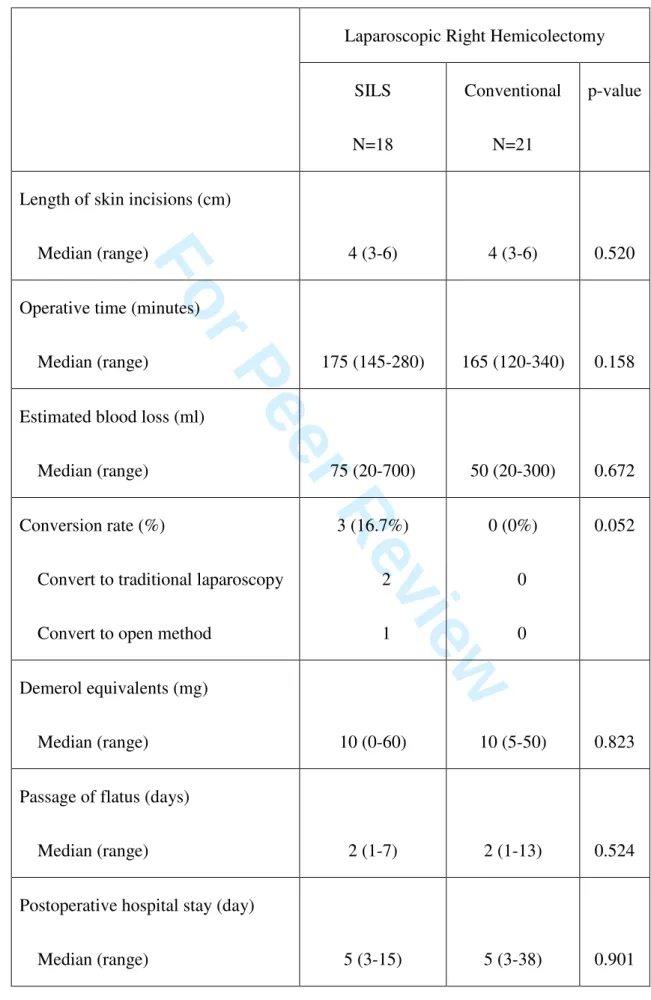
Table 2 Perioperative outcomes
Laparoscopic Right Hemicolectomy SILS
N=18
Conventional N=21
p-value
Length of skin incisions (cm)
Median (range) 4 (3-6) 4 (3-6) 0.520
Operative time (minutes)
Median (range) 175 (145-280) 165 (120-340) 0.158
Estimated blood loss (ml)
Median (range) 75 (20-700) 50 (20-300) 0.672
Conversion rate (%)
Convert to traditional laparoscopy Convert to open method
3 (16.7%) 2 1
0 (0%) 0 0
0.052
Demerol equivalents (mg)
Median (range) 10 (0-60) 10 (5-50) 0.823
Passage of flatus (days)
Median (range) 2 (1-7) 2 (1-13) 0.524
Postoperative hospital stay (day)
Median (range) 5 (3-15) 5 (3-38) 0.901
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Table 3 Surgical complications
Laparoscopic Right Hemicolectomy Variables
SILS N=18
Conventional N=21
p-value
Perioperative Complication (%) 3 (16.6%) 2 (9.5%) 0.506
Anastomotic leakage 0 0 -
Intraabdominal abscess 0 1 -
Ileus 1 1 -
Cardiovascular disease 1 0 -
Wound infection 1 0 -
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Table 4 oncologic outcomes
Laparoscopic Right Hemicolectomy
SILS Conventional p-value
Patient numbers (Solid tumor) 16 20
Tumor size (cm)
Median (range) 2.0 (0.5-6) 2.5 (0.8-6) 0.478
Distal free margin (cm)
Median (range) 16 (5-21) 13.5 (6-20) 0.094
Lymph node harvest (number,#)
Median (range) 19.5 (3-42) 19 (15-57) 0.984
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Figure 1-(A) Schematic of conventional laparoscopy port placement for right hemicolectomy;
(B) Schematic of port placement for single-incision laparoscopic surgery (SILS) for right hemicolectomy
(A)
(B)
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
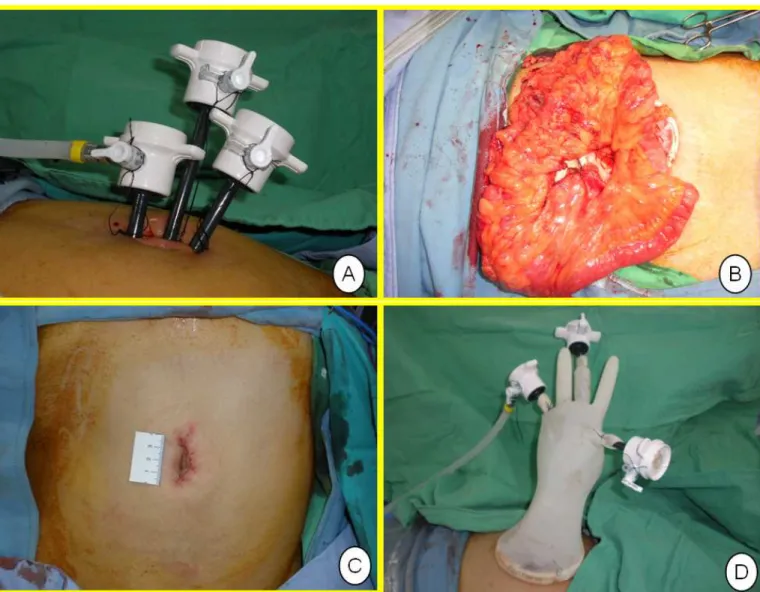
Figure 2-(A) SILS port placement for right hemicolectomy, and the adjacent three trocars stand on different height. (B) Specimen extraction from umbilical incision. (C) The surgical glove attached with three trocars was then fixed to the outer ring of the wound retractor. (D) Wound at the umbilicus at the end of the operation.
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Table 1. Patient’s demographics
Laparoscopic Right Hemicolectomy
SILS Conventional P-value
Patient numbers 18 21
Mean age (years) 69.44 66.19 0.338
Gender
Male (%) 10 (55.6%) 14 (66.7%)
Female (%) 8 (44.4%) 7 (33.3%)
0.150
BMI
Median (range)
23.34 (18.29-28.60)
23.92 (19.02-30.42)
0.863
ASA score
1-2 8 14
> 3 10 7
0.262
Surgical Indications
Right colon Diverticulosis 2 1
Ascending Colon adenocarcinoma 6 3
Cecal adenocarcinoma 10 17
0.231
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Table 2 Perioperative outcomes
Laparoscopic Right Hemicolectomy SILS
N=18
Conventional N=21
p-value
Length of skin incisions (cm)
Median (range) 4 (3-6) 4 (3-6) 0.520
Operative time (minutes)
Median (range) 175 (145-280) 165 (120-340) 0.158
Estimated blood loss (ml)
Median (range) 75 (20-700) 50 (20-300) 0.672
Conversion rate (%)
Convert to traditional laparoscopy Convert to open method
3 (16.7%) 2 1
0 (0%) 0 0
0.052
Demerol equivalents (mg)
Median (range) 10 (0-60) 10 (5-50) 0.823
Passage of flatus (days)
Median (range) 2 (1-7) 2 (1-13) 0.524
Postoperative hospital stay (day)
Median (range) 5 (3-15) 5 (3-38) 0.901
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Table 3 Surgical complications
Laparoscopic Right Hemicolectomy Variables
SILS N=18
Conventional N=21
p-value
Perioperative Complication (%) 3 (16.6%) 2 (9.5%) 0.506
Anastomotic leakage 0 0 -
Intraabdominal abscess 0 1 -
Ileus 1 1 -
Cardiovascular disease 1 0 -
Wound infection 1 0 -
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Table 4 oncologic outcomes
Laparoscopic Right Hemicolectomy SILS Conventional p-value
Patient numbers (Solid tumor) 16 20
Tumor size (cm)
Median (range) 2.0 (0.5-6) 2.5 (0.8-6) 0.478
Distal free margin (cm)
Median (range) 16 (5-21) 13.5 (6-20) 0.094
Lymph node harvest (number,#)
Median (range) 19.5 (3-42) 19 (15-57) 0.984
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Figure 1A Schematic of conventional laparoscopy port placement for right hemicolectomy 254x204mm (72 x 72 DPI)
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Figure 1B Schematic of port placement for single-incision laparoscopic surgery (SILS) for right hemicolectomy
350x270mm (72 x 72 DPI)
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Figure 2 (A) SILS port placement for right hemicolectomy, and the adjacent three trocars stand on different height. (B) Specimen extraction from umbilical incision. (C) The surgical glove attached
with three trocars was then fixed to the outer ring of the wound retractor. (D) Wound at the umbilicus at the end of the operation
486x373mm (72 x 72 DPI)
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
Schematic of port placement for single-incision laparoscopic surgery (SILS) for right hemicolectomy 350x270mm (72 x 72 DPI)
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60
For Peer Review
(A) SILS port placement for right hemicolectomy, and the adjacent three trocars stand on different height. (B) Specimen extraction from umbilical incision. (C) The surgical glove attached with three trocars was then fixed to the outer ring of the wound retractor. (D) Wound at the umbilicus at the
end of the operation 486x373mm (72 x 72 DPI)
3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60