國立臺灣大學醫學院職能治療學系暨研究所 碩士論文
Department of Occupational Therapy College of Medicine
National Taiwan University Master Thesis
自閉症障礙類群兒童重複行為的相關因子分析 The Correlates of Restricted and Repetitive Behaviors in
Children with Autism Spectrum Disorders
陳安如 An-Ju Chen
指導教授:曾美惠 博士 Advisor: Mei-Hui Tseng, Sc.D.
中華民國 102 年 6 月
June 2013
i
致謝
非常感謝曾老師的指導,才能夠順利完成論文。謝謝老師給予的建議以及投 入很多心力協助修改論文,讓內容得以更加完整和流暢。感謝論文審查口委楊宗 仁老師以及林巾凱老師的每個提醒和建議。感謝所有協助收案的相關單位,臺大 醫院、署立台北醫院、雙和醫院、歐緹斯特診所、德上診所,謝謝這些小兒職能 治療的臨床老師大力相助,讓本研究能從更多管道招募到研究個案。謝謝所有參 與本研究的家長、老師和兒童,正是因為有您們的參與,才能讓本研究得以完成。
謝謝研究室的學姊們,中佩學姊、宜靜學姊、千瑀學姊、瑋齊學姊,不管是 在協助收案、討論統計執行方法、或是日常生活各種的打氣和支持,都非常感謝 妳們。也謝謝在研究所時,彼此加油打氣的學長姊和同學們,每當覺得要走不下 去時,有你們的陪伴,才能繼續前進。
碩班這兩年,讓我學到的不只是做研究的方法,還有很多待人處事方面的磨 練,這些更為重要。最後,最需要感謝的是我的家人們。
安如 謹致 民國一○二年七月
ii
自閉症障礙類群兒童重複行為的相關因子分析
中文摘要
研究背景與目的
自閉症障礙類群(Autism Spectrum Disorder, ASD)包括自閉症 (Autism)、亞斯 伯 格 疾 患 (Asperger’s Disorder) 及 其 他 未 註 明 之 廣 泛 性 發 展 疾 患 (Pervasive Developmental Disorder Not Otherwise Specified, PDD-NOS)。根據精神疾病診斷準 則 手冊 -第四版內文 革新版 (American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, Fourth edition, Text Revision, DSM-IV-TR),
ASD 的三大診斷特徵分別為:社交能力缺損、溝通障礙和重複刻板的興趣。大約 有 90%-97%的自閉症障礙類群兒童有侷限與重複行為出現,侷限與重複行為是自 閉症障礙類群孩童的主要診斷之一,不僅影響孩童的學習、互動、更影響到各種 情境的參與。「國際健康功能與身心障礙分類 -兒童及青少年版」(International Classification of Functioning, Disability and Health for Children and Youth, ICF-CY) 包含健康狀況、身體功能與結構、活動、參與、情境因素(個人、環境),此參考架 構整合個人健康狀態在醫學與社會方面的觀點,說明疾病、功能、個人與環境間 互動的關係,不只是病理因素影響健康,且強調活動參與、情境因素的重要性。
過去有許多研究探討影響自閉症障礙類群兒童侷限與重複行為的因子,但是僅限 於 ICF-CY 其中的一、兩個領域。本研究目的,以 ICF-CY 為參考架構,探討學齡 前與國小低年級自閉症障礙類群兒童重複行為的相關因子,即依據文獻回顧結 果,自 ICF-CY 之身體功能與構造、活動及參與、環境及個人因素面向,各選出一 至二個過去研究中有顯著相關的相關因子作為獨立變項。研究假設為:這些選自 ICF-CY 各個面向的因子與自閉症障礙類群兒童的重複行為都有顯著相關。
研究方法
iii
共有八十六位自閉症障礙類群的兒童及其家長參與此研究,參與者轉介自發 展中心、職能治療診所、醫學中心的復健部、學校、自閉症家長協會及中華民國 自閉症基金會。本研究使用皮爾森(Pearson)相關和逐步多元線性迴歸分析,來探討 次領域重複行為以及整體重複行為的相關因子。依變項包含由家長填寫的「重複 行為量表」之重複行為總分,以及重複行為之五個次領域的分數:刻板行為、自 傷行為、強迫行為、儀式化與同一性行為及侷限興趣。獨立變項為依據文獻回顧 結果,以及 ICF-CY 架構,所選出可能之相關因子,包含年齡、自閉症嚴重程度、
感覺處理能力、表達性語言、接收性語言、適應行為、焦慮、親子關係及壓力。
結果
結果顯示,86 位個案平均月齡為 68.15 個月(標準差:15.60,範圍:37 到 105
個月),有 72 位男生 14 位女生,在重複行為量表的分數中顯示大部分(37.2-60.5%)
的填答分數集中在 0 分(從沒出現過此行為)到 1 分(出現過此行為,且是一個輕微 程度的問題)。皮爾森相關(Pearson correlation)顯示,整體重複行為量表分數,和嚴 重度(r =0.415, p <0.01)、表達性語言(r =-0.419, p <0.01)、接受性語言(r =-0.433, p
<0.01)、適應行為(r =-0.308, p <0.01)有顯著相關。逐步多元線性迴歸分析的結果顯 示,在整體的重複行為中,接收性語言和個案的年齡為顯著的相關因子,共解釋 20.9%的變異量。在刻板行為部分,接收性語言、年齡和適應行為是顯著的相關因 子,共解釋 42.2%的變異量。自傷行為與強迫行為,顯著的相關因子只有接收性語 言,對於兩個迴歸模型,分別解釋了 26.3%和 5.5%的變異量。儀式化與同一性行 為,及侷限興趣部分,則沒有顯著的相關因子。
結論
iv
此研究結果可以協助臨床工作者和照護者了解自閉症障礙類群兒童重複行為的相 關因子,即孩子的接收性語言、適應行為和年齡都是重複行為顯著的相關因子,
並且接受性語言是在不同重複行為次領域中最廣為出現的相關因子。即接收性語 言能力差、適應行為不好和年齡大重複行為越嚴重。本研究的結果能作為未來近 一步的實驗型研究,發展出有效的介入方式來降低自閉症障礙類群兒童的重複行 為。
關鍵字:自閉症障礙類群,侷限與重複行為,影響因子
v
Abstract
Background
With a prevalence of more than 90% in both autism and PDD-NOS groups,
restricted and repetitive behaviors (RRBs) affect their participation and adaptive function. International Classification of Functioning, Disability, and Health- Children
and Youth version (ICF-CY) describes functioning from a holistic perspective,
including health condition, body functions and structures, activity, participation, and
personal and environmental factors. The ICF-CY provides a framework to describe limitations of children’s functioning and emphasizes the impact of the environmental
factors on functioning from a developmental perspective. Thus, the purpose of the study
was to identify correlates of RRBs in preschool and early elementary school children
with autistic spectrum disorder from a holistic perspective by considering the variables
from all dimensions of the ICF-CY framework.
Method
Eighty six children with autistic spectrum disorders were recruited from
developmental centers, departments of rehabilitation at medical centers and hospitals,
elementary schools. Children with identifiable neurological conditions and patient who
vi
was illiteracy or couldn't read Chinese were excluded. Restricted and repetitive
behaviors were measured by Repetitive Behavior Scale-Revised (RBS-R). A range of
possible correlates were including severity, sensory processing, expressive language,
receptive language, adaptive behavior, age, anxiety, and parent-child relationship quality.
Descriptive analysis was conducted for basic information and the observed variables.
Pearson correlation investigated the relationships between five subtypes of RRBs and
potential correlates. Six separate multiple linear regression models identified the
correlates of each subtype of RRBs, including Stereotypy, Self-injurious Behavior,
Compulsions, Rituals and Sameness, Restricted Interests, and overall restricted and
repetitive behaviors.
Results
A total of 86 children with autism spectrum disorder aged from 37 to 105 months
with 72 boys and 14 girls. The findings indicated that almost every subtype of RRBs
was centralized in lower score. Pearson correlations showed that overall RRBs were
significantly correlate with severity (r =0.415, p <0.01), expressive language (r =-0.419,
p <0.01), receptive language (r =-0.433, p <0.01), and adaptive behavior (r =-0.308, p
<0.01). The stepwise multiple linear regression model which explained 20.9% of the
variance revealed that receptive language and age of participants were significant
vii
correlates of overall RRBs. As for stereotypic behavior, the stepwise multiple linear
regression model showed that receptive language, age, and adaptive behavior were
significant correlates and accounted for 42.2% of the variance. Regarding self-injurious
behavior and compulsive behavior, the multiple stepwise linear regression model
revealed that receptive language was the only significant correlate explaining 26.3% and
5.5% of the variances respectively. As for ritualistic and sameness behavior and
restricted interests, no significant correlate was identified.
Conclusion
Knowledge of the correlates may help clinicians, parents, and school teachers
develop interventions targeted at the correlates in order to effectively reduce their RRBs.
Results of our study can serve as a basis for future experimental studies targeted at the
correlates to ameliorate restrictive and repetitive behaviors in children with ASD.
Keywords: Autism spectrum disorders, Restricted and repetitive behaviors, Correlates
viii
Table of Contents
Introduction ... 1
Literature review ... 5
Introduction to autism spectrum disorders ... 5
The diagnosis criteria of autism spectrum disorders ... 5
The prevalence of autism spectrum disorders ... 10
Restricted and repetitive behaviors ... 11
International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) as a conceptual framework ... 12
The correlates of restricted and repetitive behaviors in children with autism spectrum disorders ... 13
The relationships between restricted and repetitive behaviors and factors in the dimension of health condition factors ... 14
Severity ... 14
The relationships between restricted and repetitive behaviors and factors in the dimension of body function and structures ... 15
Sensory processing ... 15
The relationships between restricted and repetitive behaviors and activity and participation factors ... 15
Language ... 16
Adaptive behavior ... 16
The relationships between restricted and repetitive behaviors and personal factors ... 17
Age-related differences ... 17
Gender-related differences ... 18
Anxiety ... 18
The relationships between restricted and repetitive behaviors and environmental factors19 Parent-child relationship quality ... 19
ix
Limitations of previous studies ... 20
Conclusion ... 21
Research purposes ... 22
Hypotheses of the study ... 23
Methods ... 24
Participants ... 24
Measures ... 24
The Measure of Restricted and Repetitive Behaviors ... 24
The Measure Related to Health Condition ... 25
The Measure Related to Body Function and Structures ... 26
The Measures Related to Activity and Participation ... 27
The Measures Related to Personal and Environmental factors ... 29
Procedure ... 31
Statistical analysis ... 32
Results ... 34
Discussion ... 37
Conclusion ... 42
Acknowledgements ... 43
Reference ... 44
x
List of Tables
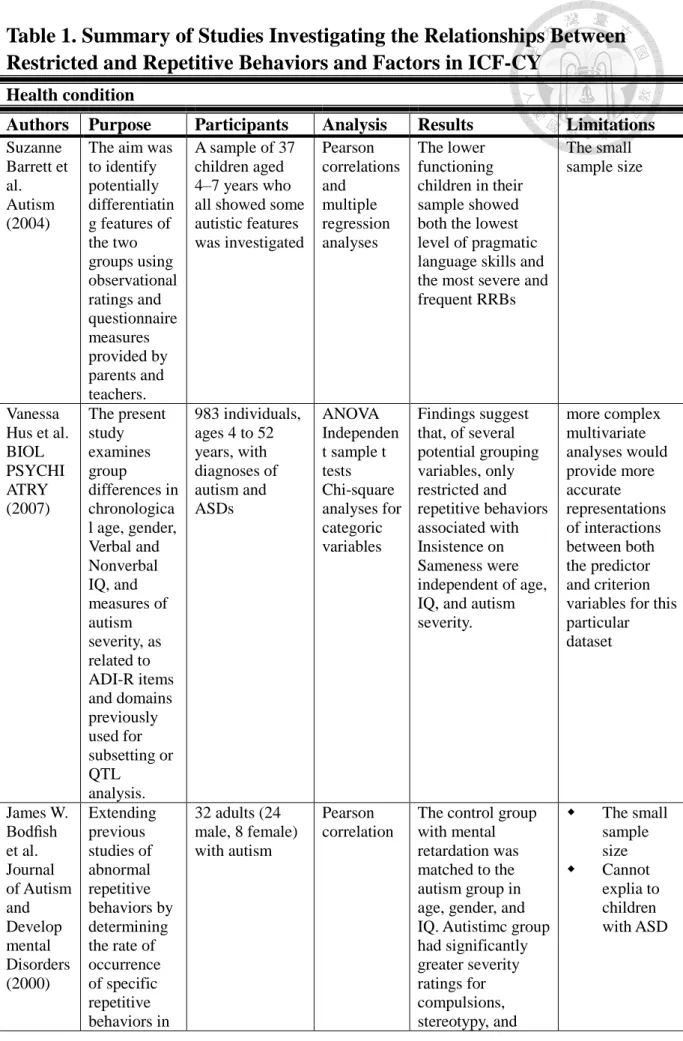
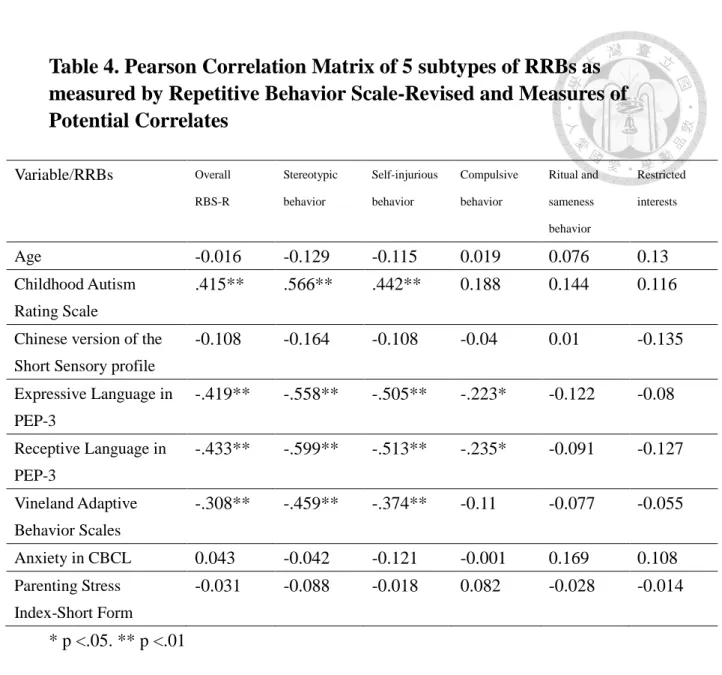
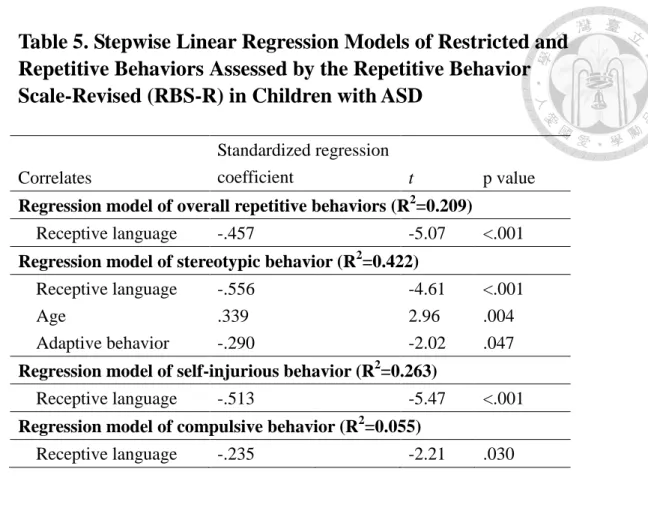
Table 1. Summary of Studies Investigating the Relationships Between Restricted and Repetitive Behaviors and Factors in ICF-CY ... 50 Table 2. Characteristics of Participants (N=86) ... 59 Table 3.The Descriptive Statistics on the Frequency of Occurrence for Each Item of Repetitive Behavior Scale-Revised ... 60 Table 4. Pearson Correlation Matrix of 5 subtypes of RRBs as measured by Repetitive Behavior Scale-Revised and Measures of Potential Correlates ... 63 Table 5. Stepwise Linear Regression Models of Restricted and Repetitive Behaviors Assessed by the Repetitive Behavior Scale-Revised (RBS-R) in Children with ASD ... 64
xi
List of Figures
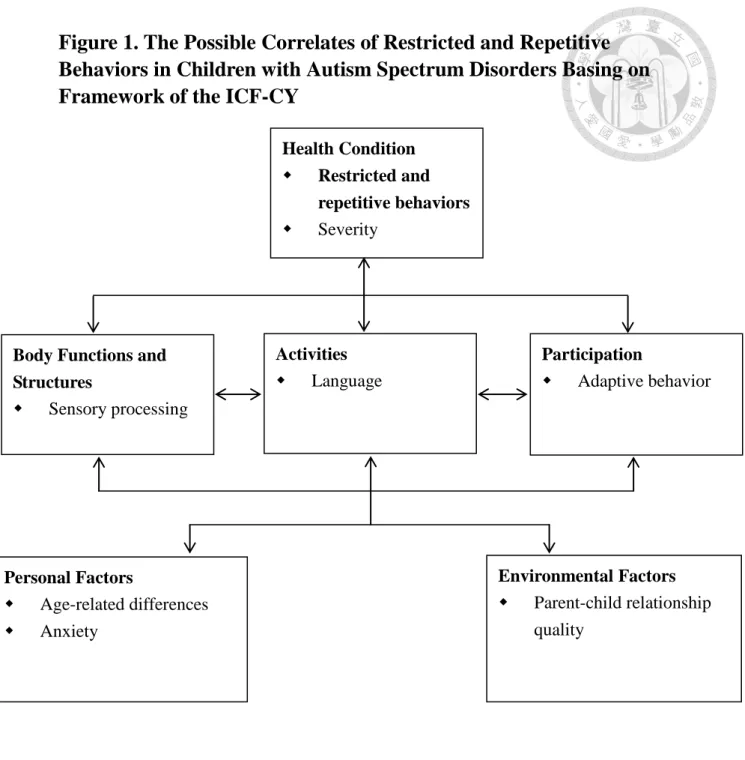
Figure 1. The Possible Correlates of Restricted and Repetitive Behaviors in Children with Autism Spectrum Disorders Basing on Framework of the ICF-CY ... 65 Figure 2. The Flow Chart of The Procedure... 66 Figure 3. The Correlates of Restricted and Repetitive Behaviors in Children with Autism Spectrum Disorders Basing on The Results of The Study ... 67
1
Introduction
Autistic spectrum disorders is a diagnosis group just like a spectrum ranging from
mild to severe, including autism, Asperger disorders, and PDD-NOS. According to
Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision
(DSM-IV-TR), individuals with autism spectrum disorder have qualitative impairment
in social interaction, qualitative impairments in communication, restricted, repetitive,
and stereotyped patterns of behavior, interests, and activities (American Psychiatric
Association, 2000). About 1 in 88 children have been identified with an autism
spectrum disorder (Centers for Disease Control, 2008; Prevention's Autism and
Developmental Disabilities Monitoring (ADDM) Network, 2012).
With a prevalence of more than 90% in both autism and PDD-NOS groups (Kim &
Lord, 2010), restricted and repetitive behaviors (RRBs) are classified by DSM-IV-TR
into four subtypes: (1) preoccupation with restricted interests; (2) nonfunctional routines
or rituals; (3) repetitive motor mannerisms; and (4) persistent preoccupation with parts
of objects. The two former subtypes are often defined as higher level repetitive
behaviors, and the other two as lower level repetitive behaviors (Turner, 1999).
Examples of RRBs may include flapping hands, flicking fingers in front of eyes, turning
in circles for repetitive motor mannerisms, preoccupation with a part of objects, such as
2
flicking a rubber band or a paper, and routines and rituals representing insistence on
sameness. Children with ASD who manifest RRBs often have sensory processing
difficulties, poor language skills, lower adaptive behavior, and higher anxiety behaviors
(Gotham et al., 2013). These children with special needs would often cause tension
between parents and them (Baker, Seltzer, & Greenberg, 2011). RRBS also affect their
participation in daily life and adaptive function (Cuccaro et al., 2003; Leekam, Prior, &
Uljarevic, 2011).
International Classification of Functioning, Disability, and Health- Children and
Youth version (ICF-CY) is based on the International Classification of Functioning,
Disability, and Health (ICF) (WHO, 2001) which describes functioning from a holistic
perspective, i.e., health condition, body functions and structures, activity, participation,
and personal and environmental factors. The ICF-CY provides a framework to describe limitations of children’s functioning and the impact of contextual factors on functioning
in addition to health condition from a developmental perspective.
Despite the fact that many studies have investigated the correlates of RRBs in
individual with autism spectrum disorders (ASD), these studies only considered
variables from only one or two dimensions, for example, sensory processing
abnormalities (Boyd et al., 2010; Chen, Rodgers, & McConachie, 2009; Gabriels et al.,
2008; Joosten & Bundy, 2010) in the body function and structure domain, adaptive
3
response (Cuccaro et al., 2003) and language skill (Ray-Subramanian & Ellis Weismer,
2012) in the activity domain, or gender-related differences in the personal factor
domain and diagnosis difference (Kozlowski & Matson, 2012) in health condition
domain. Furthermore, the age range of participants in the majority of previous studies is
wide, for example, from 3 to 21(Cuccaro et al., 2007), or from 8 to 20 years old (South,
Ozonoff, & McMahon, 2005). Results of these studies may not be applicable to children
at a specific age range.
Based on the ICF-CY model, factors in each dimension may correlate with health
condition (Simeonsson et al., 2003). Our study addressed the following research
question: Do the possible correlates from each ICF domain significantly contribute to
RRBs in children with ASD?
We hypothesized that the significant variables from each ICF domain would
correlate with each subtype of RRBs, i.e., stereotypic behavior, self-injurious behavior,
compulsive behavior, rituals and sameness behaviors, and restricted interests,
respectively and the significant correlates of the five subtypes of RRBs would
encompass all dimensions of the ICF-CY model.
Thus, the purpose of the study was to identify correlates of RRBs in preschool and
early elementary school children with autistic spectrum disorder from a holistic
perspective by considering the variables from all dimensions of the ICF-CY framework.
4
The knowledge of the factors influencing RRBs will help clinicians to plan effective
intervention for children with autistic spectrum disorder.
5
Literature review
Introduction to autism spectrum disorders
Autism spectrum disorders (ASDs) are lifelong disabilities, ranging from mild to
severe, consisting of autism, Asperger syndrome, and pervasive developmental disorder
not otherwise specified (PDD-NOS). The core symptoms include impairment in social
function, communication, resistance to environmental change or change in daily
routines, and engagement in repetitive activities and stereotyped movements.
The diagnosis criteria of autism spectrum disorders
299.00 Autistic Disorder
The American Psychiatric Association's Diagnostic and Statistical Manual-IV, Text
Revision (DSM-IV-TR) provides standardized criteria to help diagnose autism spectrum
disorders.
A. A total of six (or more) items from (1), (2), and (3), with at least two from (1), and
one each from (2) and (3):
(1) Qualitative impairment in social interaction, as manifested by at least two of the
following:
6
(a) Marked impairment in the use of multiple nonverbal behaviors, such as
eye-to-eye gaze, facial expression, body postures, and gestures to regulate social
interaction
(b) Failure to develop peer relationships appropriate to developmental level
(c) A lack of spontaneous seeking to share enjoyment, interests, or achievements
with other people (e.g., by a lack of showing, bringing, or pointing out objects of
interest)
(d) Lack of social or emotional reciprocity
(2) Qualitative impairments in communication, as manifested by at least one of the
following:
(a) Delay in or total lack of, the development of spoken language (not accompanied
by an attempt to compensate through alternative modes of communication such as
gesture or mime)
(b) In individuals with adequate speech, marked impairment in the ability to
initiate or sustain a conversation with others
(c) Stereotyped and repetitive use of language or idiosyncratic language
(d) Lack of varied, spontaneous make-believe play or social imitative play
appropriate to developmental level
7
(3) Restricted, repetitive, and stereotyped patterns of behavior, interests, and activities
as manifested by at least one of the following:
(a) Encompassing preoccupation with one or more stereotyped and restricted
patterns of interest that is abnormal either in intensity or focus
(b) Apparently inflexible adherence to specific, nonfunctional routines or rituals
(c) Stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or
twisting or complex whole-body movements)
(d) Persistent precoccupation with parts of objects
B. Delays or abnormal functioning in at least one of the following areas, with onset
prior to age 3 years: (1) social interaction, (2) language as used in social communication,
or (3) symbolic or imaginative play.
C. The disturbance is not better accounted for by Rett's disorder or childhood
disintegrative disorder.
299.80 Pervasive Developmental Disorder, Not Otherwise Specified (PDD-NOS)
This category should be used when there is a severe and pervasive impairment in the
8
development of reciprocal social interaction or verbal and nonverbal communication
skills, or when stereotyped behavior, interests, and activities are present, but the criteria
are not met for a specific pervasive developmental disorder, schizophrenia, schizotypal
personality disorder, or avoidant personality disorder. For example, this category
includes "atypical autism" -presentations that do not meet the criteria for autistic
disorder because of late age of onset, atypical symptomatology, or sub-threshold
symptomatology, or all of these.
299.80 Asperger's Disorder (or Asperger Syndrome)
An Asperger/HFA screening tool must meet all six areas defined by the DSM-IV
description of Asperger Syndrome (A-F below) to qualify for a positive rating from
First Signs:
A. Qualitative impairment in social interaction, as manifested by at least two of the
following:
(1) Marked impairment in the use of multiple nonverbal behaviors, such as
eye-to-eye gaze, facial expression, body postures, and gestures to regulate social
interaction
(2) Failure to develop peer relationships appropriate to developmental level
9
(3) A lack of spontaneous seeking to share enjoyment, interests, or achievements
with other people (e.g., by a lack of showing, bringing, or pointing out objects of
interest to other people)
(4) Lack of social or emotional reciprocity
B. Restricted, repetitive, and stereotyped patterns of behavior, interests, and activities,
as manifested by at least one of the following:
(1) Encompassing preoccupation with one or more stereotyped and restricted
patterns of interest that is abnormal either in intensity or focus
(2) Apparently inflexible adherence to specific, nonfunctional routines or rituals
(3) Stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or
twisting, or complex whole-body movements)
(4) Persistent preoccupation with parts of objects
C. The disturbance causes clinically significant impairment in social, occupational, or
other important areas of functioning.
D. There is no clinically significant general delay in language (e.g., single words used
by age 2 years, communicative phrases used by age 3 years).
10
E. There is no clinically significant delay in cognitive development or in the
development of age-appropriate self-help skills, adaptive behavior (other than in social
interaction), and curiosity about the environment in childhood.
F. Criteria are not met for another specific pervasive developmental disorder or
schizophrenia.
The prevalence of autism spectrum disorders
From 2004 to 2010, among the 7 cities and 18 counties in Taiwan, the prevalence
rates for ASDs in the age groups 3–5 years, 6–11 years, 12–14 years, and 15–17 years
were 9.1–16.4/10,000, 11.2–25.3/10,000, 6.9–19.6/10,000, and 4.5–14.3/10,000,
respectively. The prevalence rates of all age groups generally increased over the years (p
< 0.01 for all age groups). From 2004 to 2010, there were more boy cases than girl
cases in each year, and the boy-to-girl ratio ranged from 6.14:1 to 6.60:1 (mean =
6.43:1)(Lai, Tseng, Hou, & Guo, 2012).
Autism and Developmental Disabilities Monitoring (ADDM) Network (2012), a
division of Centers for Disease Control and Prevention (CDC) in the US, released data
on the prevalence of ASD, indicating that about one in 88 eight-year old children have
11
ASDs in multiple areas of the United States. Approximately 18.5 per 1,000 in boys and
3.9 per 1,000 in girls were identified as having ASDs. Comparison of 2008 findings
with earlier years indicated that an increase of 78% when the 2008 data were compared
with the data for 2002 (from 6.4 per 1,000 children aged 8 years in 2002 to 11.4 per
1,000 in 2008) (Baio, 2012). The reason for the increase in prevalence might be caused
by the differences in screening tools and diagnostic criteria (Sun & Allison, 2010).
Restricted and repetitive behaviors
Restricted and repetitive behaviors (RRBs), one of three core features of autism,
are classified by DSM-IV-TR into four subtypes: (1) preoccupation with restricted
interests; (2) nonfunctional routines or rituals; (3) repetitive motor mannerisms; and (4)
persistent preoccupation with parts of objects. Turner (1999) was the first one to classify RRBs into subcategories of “higher-level” and “lower-level” behaviors. The two former
subtypes are often defined as higher level repetitive behaviors, and the two others are
described together as lower level repetitive behaviors. As for higher-level behaviors,
routines and rituals represented insistence on sameness. With regard to lower-level
behaviors, they are more often manifested in younger and lower functioning children as
well as in children with intellectual disability or other brain-based impairments.(Leekam
et al., 2011) Examples of these higher-level RRBs may include preoccupation with a
12
part of objects, such as flicking a rubber band or a paper, routines and rituals
representing insistence on sameness. As for lower-level RRBs, behaviors such as body
rocking, hands flapping, fingers flicking in front of eyes, or turning in circles are
common in ASDs. Prevalence rates of at least one of RRBs ranged from 96–100% and
90–97% by age cohorts (2-6 years old) for autism and PDD-NOS groups, respectively
(Kim & Lord, 2010). There are overlaps between each type of RRBs and vary in
complexity. RRBs are influenced by the developmental level of cognitive and
communicative abilities and may interfere with learning in school (Leekam et al., 2011).
All these behaviors are not always present in the same individual and are often not
stable over their life time. In fact, in the same individual with ASD, they may change
not only in quantity but also quality and type (Militerni, Bravaccio, Falco, Fico, &
Palermo, 2002). Although children with various developmental disorders manifest
RRBs, RRBs are more frequently seen in children with ASD.
International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) as a conceptual framework
The World Health Organization’s International Classification of Functioning,
Disability, and Health (ICF) describes human functioning in terms of body functions
and structures (physiological functions and anatomical parts), activity (execution of a
13
task or action), participation (involvement in a life situation), and contextual factors
(including personal factors and environmental factors). In October of 2007, the
International Classification of Functioning, Disability, and Health for Children and
Youth (ICF-CY) was published by the WHO. International Classification of Functioning,
Disability and Health for Children and Youth (ICF-CY) is based upon the framework of
the ICF and includes developmental aspects for children and youth. The ICF-CY is
designed to record the characteristics of developing child and the influence of his or her
surrounding environments.
Studies have shown that not only body function and structure but also contextual factors influence child’s functioning and development. For instance, the relationship
between mother and child is a critical environmental factor, and will influence the child
throughout his or her whole life (Simeonsson et al., 2003).
The correlates of restricted and repetitive behaviors in children with autism spectrum disorders
Many studies have investigated the factors associated with restricted and repetitive
behaviors. The factors were various including every dimension in the ICF-CY, ranging
from health condition factors to contextual factors.
14
The relationships between restricted and repetitive behaviors and factors in the
dimension of health condition factors
Severity
Barrett et al. (2004) recruited 37 children with autism aged 4–7 years, and found
that the lower functioning children in their sample showed both the lowest level of
pragmatic language skills and the most severe and frequent RRBs. The limitation was
the small sample size (N=37)(Barrett, Prior, & Manjiviona, 2004). Hus et al. (2007)
collected 983 individuals, ages 4 to 52 years, with diagnoses of autism and ASDs. This
study described a complex set of relationships between repetitive sensory and motor
actions, verbal IQ, and verbal and nonverbal communication, with the lower functioning
group showing greater frequency of these low-level repetitive behaviors(Hus, Pickles,
Cook, Risi, & Lord, 2007). Bodfish et al. (2000) compared adults with mental
retardation with and without autism. The control group with mental retardation was
matched to the autism group in age, gender, and IQ. The autism group had significantly
greater severity ratings for compulsions, stereotypy, and self-injury. Repetitive behavior
severity was correlated to the severity of autism (Bodfish, Symons, Parker, & Lewis,
2000).
15
The relationships between restricted and repetitive behaviors and factors in the
dimension of body function and structures
Sensory processing
Abundant research indicated abnormal sensory processing in the ASDs population.
Significant correlations were found between sensory abnormalities and RRBs(Boyd et
al., 2010; Boyd, McBee, Holtzclaw, Baranek, & Bodfish, 2009; Chen et al., 2009;
Gabriels et al., 2008; Joosten & Bundy, 2010). Gabriels et al. (2008) indicated children
with ASD with higher frequency of RRBs would have a higher rate of abnormal sensory
processing as measured by the Sensory Profile. Chen et al. (2009) found that significant
relationships were noted between the frequency and intensity of RRBs and both tactile
sensitivity and visual/ auditory sensitivity. Boyd et al. (2010) reported that a high level
of hyperresponsive behaviors predicted a high level of repetitive behaviors. These
findings provide evidence for the correlations between sensory processing difficulties
and RRBs in children with ASD.
The relationships between restricted and repetitive behaviors and activity and
participation factors
16
Language
Ray-Subramanian et al. (2012) examined whether language skills and nonverbal
cognitive skills were associated with clinician-observed RRBs in a sample of 115 children with ASD at ages 2 and 3. By age 3, RRBs were significantly negatively
correlated with receptive and expressive language, as well as nonverbal cognitive skills.
Increases in receptive and expressive language from age 2 to 3 significantly predicted
decreases in RRBs (Ray-Subramanian & Ellis Weismer, 2012).
Adaptive behavior
Cuccaro et al. (2003) found a negative correlation between level of adaptive
behavior and repetitive sensory motor actions when examining the factor structure of
the Autism Diagnostic Interview-Revised (ADI-R) and the relationship between
identified factors and developmental level. Two factors were identified: Factor
1—repetitive sensory motor actions and Factor 2—resistance to change. Joosten et al.
(2010) used the Vineland Adaptive scale and Motivation Assessment Scale (MAS;
Durand & Crimmins, 1988) which is assessing the motivation for stereotypical
behaviors to investigate the difference in children with intellectual disability (ID) and
ASD. The results showed that children with ASD scoring lower in adaptive behavior
would have more tendencies to reveal the stereotypical behaviors (Joosten & Bundy,
17
2010).
The relationships between restricted and repetitive behaviors and personal factors
Age-related differences
Esbensen et al. (2009) investigated age related differences in RRBs in 712 2- to
62-year-old individuals with ASD. The results indicated that older individuals tended to
exhibit fewer RRBs than younger individuals. Those individuals with ASD comorbid
with diagnosis of intellectual disability would have decreased RRBs with age. Scores of
all subscales of the RBS-R, such as restricted interests, stereotyped, ritualistic
compulsive, and self-injurious reduced with age (Esbensen, Seltzer, Lam, & Bodfish,
2009). Richler et al. (2010) indicated that repetitive sensory and motor behaviors
remained high across the age range of 2 to 9 and only decreased in children with higher
nonverbal IQ at age 9. In contrast, insistence on sameness behaviors started with lower
severity at age 2 years and high insistence on sameness scores were associated with
older ages and with milder social and communication impairments (Richler, Huerta,
Bishop, & Lord, 2010). Militerni et al. (2002), in a study with 2- to 4- and 7- to
11-year-old children with ASD, found that younger children displayed more motor and
sensory repetitive behaviors and older children had more complex behaviors, such as
18
repetitive complex sequences and repetitive language (Militerni et al., 2002). Both
Richler et al. (2010) and Militerni et al. (2002) indicated that insistence on sameness
behaviors or more complicated repetitive behaviors were related to older children.
Richler et al. (2010) indicated that repetitive sensory and motor behaviors remain high
from the age of 2 to 9. However, the result of Militerni et al.’s (2002) study showed that
motor and sensory repetitive behaviors gradually decreased with age. The discrepancy
may be due to different measures used. Richler et al. (2010) used Autism Diagnostic
Interview–Revised revealed two RRB factors, i.e. repetitive sensorimotor (RSM) behavior and insistence on sameness (IS) behavior. As for Militerni et al.’s (2002) study,
presence of a repetitive behavior was screened for through parental interview by means
of a semi-structured, non-standardized questionnaire.
Gender-related differences
Kozlowski et al. (2012) investigated both group and gender differences in the rates
of stereotypic behaviors in 322 infants and toddlers who were classified into the autism,
PDDNOS, and typically developing groups. Results showed no significant gender
differences in the rates of stereotypic behaviors (Kozlowski & Matson, 2012).
Anxiety
19
RRBs were triggered by intrinsic and extrinsic motivators in children with ASD.
Joosten et al. (2009) showed that anxiety was likely to be an intrinsic motivator whereas
escape and gaining a tangible object were the two most common extrinsic motivators
(Joosten, Bundy, & Einfeld, 2009). Gotham et al. (2013) explored the association
between anxiety and ASD symptoms; particularly the degree to which the relationship
was explained by insistence on sameness (IS) behaviors. Child Behavior Checklist
Anxiety Problems T-scores was used to measure anxiety. The results indicated that
higher anxiety was associated with higher overall RBS-R and sameness subscale scores
(Gotham et al., 2013).
The relationships between restricted and repetitive behaviors and environmental factors
Parent-child relationship quality
Positive family atmosphere may have positive effects on the child such as
ameliorating the autism symptoms and mitigating behavior problems. Smith et al. (2008)
recruited 149 families of adolescents and adults with ASD, and recorded their mother
and child relationship quality. The results indicated that high levels of relationship
quality was related to subsequent reductions in repetitive behaviors and behavior
problems (Smith, Greenberg, Seltzer, & Hong, 2008). Baker et al. (2011) also showed
20
the same result. Participants were 149 families of children diagnosed with autism who
were between the ages of 10 and 22 years during the 3-year period examined. Mothers
reported on family adaptability, the mother–child relationship, their own depressive
symptoms, and the behavior problems of their children. The rating included of hurtful to
self, unusual or repetitive, withdrawn or inattentive, socially offensive, uncooperative,
hurtful to others, destructive to property, and/or disruptive. Testing of the path model
indicated high occurrence of behavior problems and maternal depression over time
(Baker et al., 2011).
Limitations of previous studies
The ICF-CY conceptual framework provides a new paradigm of human
functioning and disability, and it can be used to guide holistic and interdisciplinary
approaches to assessment and intervention (Simeonsson et al., 2003). Although there are
many studies investigating the correlates of RRBs in individual with ASD, some studies
only considered the domain of body functions and structures (Boyd et al., 2010; Chen et
al., 2009; Gabriels et al., 2008) and some studies only investigated contextual
factors(Baker et al., 2011; Kozlowski & Matson, 2012). There was no study examining
the potential correlates of RRBs considering variables from all domains of the ICF-CY,
i.e., body function and structures, activity and participation factors, and environmental
21
factors, simultaneously. Furthermore, many previous studies recruited subjects with
ASD across a large age range. For example, South et al. (2005) recruited individuals
with ASD aged 8 to 20 years (South et al., 2005). Cuccaro et al. (2007) collected data
from individuals with ASDs aged 3 to 21. It would be difficult to apply the results to
children at a specific age (Cuccaro et al., 2007).
Conclusion
Previous studies manifested that restricted and repetitive behaviors negatively
related to language and adaptive behavior. Furthermore, RRBs are positively correlated
with severity, sensory processing abnormalities and anxiety of individuals with autism
spectrum disorder. The relationships between RRBs and age are still inconsistent.
In the domain of activity, receptive and expressive language skills were negatively
correlated with RRBs in children with ASD. Ray-Subramanian et al.’s (2012) study
recruited toddler only in 2 to 3 years old such that it was difficult to apply the results to
children in preschool or early school age for the later would have more challenge in
using language to interact with peers.
In the domain of participation, previous studies showed that adaptive behavior was
significantly, negatively related to RRBs in children with ASD (Cuccaro et al., 2003;
Joosten & Bundy, 2010). However, these studies recruited children with a large age
22
band, from 3 to 21 years old, and did not consider comorbid situation in participants
(Cuccaro et al., 2003).
Regarding the personal factor, the relationship between age and RRBs in
children with ASD was still not consistent (Esbensen et al., 2009; Militerni et al., 2002;
Richler et al., 2010). Furthermore, RRBs were correlated with severity and anxiety in
children with ASD (Goldman et al., 2009; Joosten & Bundy, 2010). The interaction
quality between mother and children were negatively correlated with RRBs. Children
with ASD had better interaction with their mother would have lower RRBs (Baker et al.,
2011; Smith et al., 2008).
Few studies considered the factors in the environmental domains when examining
the correlates of RRBs in children ASD (Cuccaro et al., 2003; Richler et al., 2010;
Smith et al., 2008). These studies only considered variables in environmental factor and
body function and structures.
Despite the fact that many studies have investigated the correlates of RRBs in
individual with ASD, these studies only considered variables from only one or two
dimensions of the ICF-CY.
Research purpose
The purpose of the study was to identify the correlates of restricted and repetitive
23
behaviors in preschool and early elementary school children with autism spectrum
disorder adopting the ICF-CY as a conceptual framework. The factors in all dimensions
of the ICF-CY were taken into account as potential correlates.
Hypotheses of the study
1. Autistic severity, sensory processing, expressive language, receptive language,
adaptive behavior, age, anxiety and patient-child relationship quality would
significantly correlate with overall RRBs as measured by Repetitive Behavior
Scale-Revised (RBS-R)
2. Autistic severity, sensory processing, expressive language, receptive language,
adaptive behavior, age, anxiety and patient-child relationship quality would
significantly correlate with five subtypes of RRBs, i.e., stereotypic behavior,
self-injurious behavior, compulsive behavior, rituals and sameness behaviors, and
restricted interests as measured by Repetitive Behavior Scale-Revised (RBS-R),
respectively.
3. The significant correlates of the five subtypes of RRBs (stereotypic behavior,
self-injurious behavior, compulsive behavior, rituals and sameness behaviors, and
restricted interests) would encompass all dimensions of the ICF-CY model.
24
Methods
Participants
Eighty-six children with autistic spectrum disorders were recruited from
developmental centers, departments of rehabilitation at medical centers and hospitals,
elementary schools, and Autism Parents Association(自閉症家長協會) in northern
Taiwan as well as Autism Foundation of the Republic of China(中華民國自閉症基金 會). Children were included if (1) they were diagnosed as autism spectrum disorder by
psychiatrists; (2) they were preschoolers or early elementary school children; (3) their
primary caregivers gave informed consents. Children with identifiable neurological
conditions and parents who were illiterate or couldn't read Chinese were excluded.
Measures
The following measures were classified by the ICF-CY dimensions (Figure 1).
The Measure of Restricted and Repetitive Behaviors
Repetitive Behavior Scale-Revised (RBS-R):
The RBS-R is a questionnaire that assesses 43 discrete types of repetitive
behaviors across 6 subscales (Stereotypy, Self-injurious Behavior, Compulsions,
25
Rituals, Sameness, and Restricted Interests). Scores for each item on the measure
range in 0 (behavior does not occur), 1 (behavior occurs and is a mild problem), 2
(behavior occurs and is a moderate problem), and 3 (behavior occurs and is a
severe problem). Lam et al. (2007) conducted a factor analysis (based on N = 320
caregivers of individuals with autism) resulting in a five-factor solution that was
clinically meaningful and statistically sound. Factor loadings ranged from 0.51 -
0.66, accounting for 47.5% of the variance; internal consistency of the scales
ranged from 0.78 - 0.91 and inter-rater reliability ranged from 0.57 - 0.73. The five-factor solution was deemed as most appropriate because they were easily
interpretable with good internal consistency, high item-total correlations, and reasonable fit as indicated by the RMSEA statistic. (Lam & Aman, 2007). In this
study we used the total score of the RBS-R, and the score of each subtypes based
on Lam et al.’s (2007) factor analysis as the dependent variable.
The Measure Related to Health Condition
Childhood Autism Rating Scale (CARS):
The CARS (Schopler, Reichler, DeVellis, & Daly, 1980) is a 15-item behavior
observational rating scale. The questionnaire is used for individuals 24 months of
age and above. In our study we adopted the method of observing children and
26
interviewing with parents who are familiar with children. The CARS can help
clinicians to identify the severity of autism, total scores from normal (non-autistic)
to severely abnormal (severely autistic). The total CARS score for each child has a
possible range of from 15 to 60. A higher score (a score > 29.5) indicates more
severely autistic. The items in CARS contain social, language, and cognitive skills,
with each item having a continuum rating. It has short administration time (10-15
min) and value in screening to quickly identify children with autism. The reliability
is good with internal consistency of 0.94 and inter-rater reliability of 0.71(Schopler
et al., 1980).
The Measure Related to Body Function and Structures
Chinese version of the Short Sensory profile (SSP-C):
The SSP-C is a 35-item caregiver questionnaire which evaluates children’s
sensory processing and their response to sensory events in everyday life. The
questionnaire is used for children from 3 to 10 years of age. Caregivers give their
answers through a 5-point Likert scale (nearly never = 5, seldom = 4, occasionally
= 3, frequently = 2, almost always = 1). A higher score indicates better sensory
processing abilities (Tseng & Chen, 2008). Psychometric properties are detailed on
the user manual. The internal consistency of the SSP total and sections ranged from
27
0.70 to 0.90. All the section and factor scores of the SP-C demonstrated significant
differences between children with and without ASD (Tseng & Chen, 2008). The
Chinese version SP demonstrated acceptable to good internal consistency (Cronbach’s α=.62 -.90), good test-retest reliability for total scores (ICC=.79), and
poor to good test-retest reliability for each section scores and each factor scores
(ICC=.44 - .90). In this study we used the total score of the SSP as a possible
correlate of the participation with ASD because it is the most sensitive indicator of
sensory dysfunction (Tomchek & Dunn, 2007).
The Measures Related to Activity and Participation
Psychoeducational Profile-3(PEP-3):
The PEP-3 is a norm-referenced scale measuring development and
maladaptive behavior in children with ASD between the developmental ages of 2
to 7.5 years(Schopler, Lansing, Reichler, & Marcus, 2004). The Performance
section is made up of 10 subtests: 6 that measure developmental abilities and 4 that
measure maladaptive behaviors. These subtests are combined to form 3
Composites: Communication, Motor and Maladaptive Behaviors. The Motor
Composite includes Fine Motor, Gross Motor, and Visual-Motor Imitation. The
Maladaptive Behavior composite contains Affective Expression, Social Reciprocity,
28
Characteristic Motor Behaviors, and Characteristic Verbal Behaviors. The
Cognitive Verbal/Preverbal, Expressive Language and Receptive Language
subtests, which belong to the Communication Composite were used to measure
cognitive and language ability. The Expressive Language subtest (25 items)
measures naming ability, production of phrases, reading and counting ability, color
and letter naming, the ability to produce nouns, pronouns and age appropriate
syntax, the ability to express relations such as big and little, as well as some
pragmatic information such as the ability to state name and gender when asked and
the ability to use words and gestures to request help. The Receptive Language subtest (19 items) measures a child’s ability to understand communication through
activities such as pointing to body parts upon command, identifying shapes, letters,
and objects and demonstrating the ability to follow directions and respond to
gestures, understand action words and respond to wh- questions(Fulton &
D'Entremont, 2013). Test items on the Performance Scale are scored as Passing (2
points), Emerging (1 point) and Failing (0 points) depending on specific scoring
criteria prescribed in the administration guidelines. We used the raw score of
subtests of Expressive Language and Receptive Language in our study.
Vineland Adaptive Behavior Scales (VABS):
29
Vineland Adaptive Behavior Scales are designed to assess adaptive behavior defined as ‘the individual’s performance in daily life activities necessary for
personal and social independence’. This scale contains four different domains of
adaptive behavior, i.e., Communication, Daily Living Skills, Socialization, and
Motor Skills. The VABS was administered through a semi-structured interview
with parents or caregivers (Sparrow et al., 1984). The VABS is a norm-referenced
test measuring adaptive behavior in domains of communication (receptive,
expressive, and written), daily living skills (personal, domestic, and community),
socialization (interpersonal relations, play and leisure time, and coping skills), and
motor skills (gross motor, fine motor). Each item is measured from 0 to 2 .The
Vineland Adaptive Behavior Scales was translated in Chinese by Wu et al. in 2004
and can be applied to caregivers who have children in three to twelve years old. We
used the total score in our study.
The Measures Related to Personal and Environmental factors
Child Behavior Checklist Chinese version (CBCL-C):
The CBCL is one of the most commonly used parent-report questionnaire that
assesses emotional and behavioral problems in children of 4-18 year-olds
(Achenbach, 1991). The CBCL was translated to the Chinese version (CBCL-C) by
30
Huang, Chung, & Wang (1994). The CBCL-C includes 113 items to assess eight
narrow-band syndromes (Withdrawn, Somatic complaints, Anxious/Depressed,
Social problems, Thought problems, Attention problems, Delinquent behavior, and
Aggressive behavior) and two broad-band syndromes (internalizing and
externalizing behavior problems). The internalizing problems include Withdrawn,
Somatic complaints, and Anxiety/Depression. The externalizing problems include
Delinquent behavior and Aggressive behavior (Huang, et al., 1994). The test-retest
reliability is 0.51-0.74, and the internal consistency is 0.81-0.92 (Huang, et al.,
1994). The CBCL/1 1 /2 –5 also assesses emotional and behavioral problems for
toddlers and preschoolers ranging from 18 months to 5 years old. The internalizing
problems (36 items), consists of four syndrome subscales (Emotionally Reactive,
Anxious/Depressed, Somatic Complaints, and Withdrawn). The externalizing
problems (24 items), consists of two syndrome subscales (Attention Problems and
Aggressive Behavior). In our study, we used the Anxiety/Depression T score to
represent the degree of anxiety.
Parenting Stress Index-Short Form (PSI-SF):
The PSI-SF (Abidin, 1983; Loyd & Abidin, 1985) was designed to measure
the interactions between the parent and the child and assess stress in the
31
parent-child relationship. It is a 36-item questionnaire that contains three subscales,
including parental distress, parent-child dysfunctional interaction, and difficult
child. It is a common screening tool used to assess stress experienced by parents of
a child with a disability. It identifies dysfunctional parenting and predicts the
potential for parental behavior problems and child adjustment difficulties within
the family system. While its primary focus is on the preschool child, the PSI can be
used with parents whose children are 12 years of age or younger. Each item were
rated from 1(strongly disagree) to 5(strongly agree). Thus, the total score ranges
from 36 to 180. The PSI-SF shows good reliability and validity (Reitman, Currier,
& Stickle, 2002).
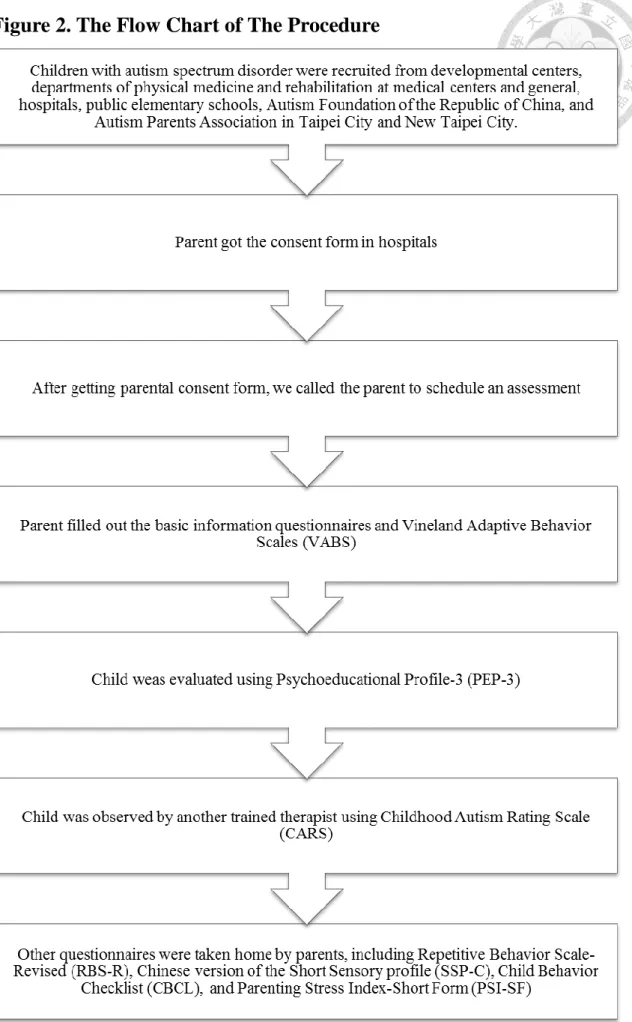
Procedure
This study was approved by the Institute Review Board of National Taiwan
University Hospital. Children with autism spectrum disorder were recruited from
developmental centers, departments of physical medicine and rehabilitation at medical
centers and general hospitals, public elementary schools, Autism Foundation of the
Republic of China, and Autism Parents Association in Taipei City and New Taipei City.
Consent forms and a letter which explained the purpose of study were given to parents
with children with ASD. After getting parental consent form, we called the parent to
32
schedule an assessment at School of Occupational Therapy, National Taiwan University.
At the beginning of the assessment, parent filled out the basic information
questionnaires and the Vineland Adaptive Behavior Scales (VABS). Researchers gave a
package of questionnaires to parents, including Repetitive Behavior Scale-Revised
(RBS-R), Chinese version of the Short Sensory profile (SSP-C), Child Behavior
Checklist (CBCL), and Parenting Stress Index-Short Form (PSI-SF). While parents
were filling out the basic information questionnaire and the VABS, the child was
evaluated by trained therapists using Psychoeducational Profile-3(PEP-3). The child
was also observed by another trained therapist using Childhood Autism Rating Scale
(CARS). Other questionnaires were taken home by parents. Parents would return the
completed questionnaires within one month (Figure 2).
Statistical analysis
Statistical analyses were performed using SPSS 17.0 software (Norusis, 2008;
Statistics, 2008). Two-sided p≦0.05 was considered statistically significant. Descriptive
analysis was conducted for basic information and the observed variables. We also used
Pearson correlation to investigate the relationships between five subtypes of RRBs and
potential correlates. We fitted six separate multiple linear regression models to identify
the correlates of each subtype of RRBs, including Stereotypy, Self-injurious Behavior,
33
Compulsions, Rituals and Sameness, Restricted Interests, and overall restricted and
repetitive behaviors. The independent variables included expressive language and
receptive language as measured by the PEP-3, severity as measured by the CARS,
sensory processing as measured by the SSP-C, anxiety as measured by the CBCL,
adaptive behavior as measured by the VABS, and demographic data of children.
34
Results
Descriptive statistics of demographic was shown in Table 2. A total of 86 children
with autism spectrum disorder aged from 37 to 105 months (mean: 68.15 months; SD:
15.60 months) with 72 boys and 14 girls. The majority of participants (73.3%) were
children with autism. The frequency of occurrence for each subtype of RRBs was
shown in Table 3. The findings indicated that almost every subtype of RRBs was
centralized in lower scores, except the restricted interests. Namely, the items described
RRBs rarely occur in our participants. For instance, the scores of most items
(37.2-60.5%) of Stereotypic Behavior were 0 , indicating that the behavior does not
occur, and the scores of a much higher percentage of items of Self-injurious Behavior
were 0 (41.9-84.9%). The score of overall restricted and repetitive behaviors was 0-129
in this questionnaire. However, our study showed that the score of overall RRBs was
just ranging from 2 to 63.
We used Pearson correlations to indicate the relationships between RRBs,
including Stereotypy, Self-injurious Behavior, Compulsions, Rituals and Sameness, and
Restricted Interests respectively and potential variables (Table 4). The findings showed
that overall RRBs were significantly correlated with severity (r=0.415, p<0.01),
expressive language (r =-0.419, p <0.01), receptive language (r =-0.433, p <0.01), and
35
adaptive behavior (r =-0.308, p <0.01). As for the subtypes of RRBs, stereotypic
behavior and self-injurious behavior had the same significant correlates, i.e. severity,
expressive language, receptive language, and adaptive behavior. Compulsive behavior
was significantly correlated with expressive language and receptive language. However,
no significant independent variables correlated with ritual and sameness behavior and
restricted interests respectively.
Stepwise multiple linear regression analysis was conducted to investigate the
correlates of overall RRBs, stereotypic behavior, self-injurious behavior, compulsive
behavior, rituals and sameness behaviors, and restricted interests. The stepwise multiple
linear regression model for RRBs, as measured by the repetitive behavior scale-revised
(RBS-R)(Bodfish et al., 2000), revealed that receptive language and age of participants
were significant correlates of overall RRBs. The model explained 20.9% of the variance.
The score of overall RRBs was higher when the receptive language was poorer and the
age of participants with ASD was older. It indicated that children with delayed receptive
language skill had a high severity level of RRBs.
As for stereotypic behavior, the stepwise multiple linear regression model showed
that receptive language, age, and adaptive behavior were significant correlates and
accounted for 42.2% of the variance. The score of stereotypic behavior subscale was
higher when the score of receptive language was lower, participants were older, and the
36
score of adaptive behavior was lower. That is, children with poorer receptive language
and worse adaptive behavior had higher stereotypic behavior. Furthermore, stereotypic
behavior increased when children with ASD were getting older.
Regarding self-injurious behavior, the multiple stepwise linear regression model
revealed that receptive language was the only significant correlate explaining 26.3 % of
the variance. The score of self-injurious behavior subscale was higher when the score of
receptive language was lower. It indicated that children who have poorer receptive
language had a higher level of severity of self-injurious behavior.
As regards compulsive behavior, the multiple stepwise linear regression model
indicated that receptive language was the only significant correlate and could explain
5.5% of the variance. The score of compulsive behavior subscale was higher when the
score of receptive language was lower. That is, children who have poorer receptive
language skill had a higher level of severity of compulsive behavior.
As for ritualistic and sameness behavior and restricted interests, no significant
correlate was identified.
37
Discussion
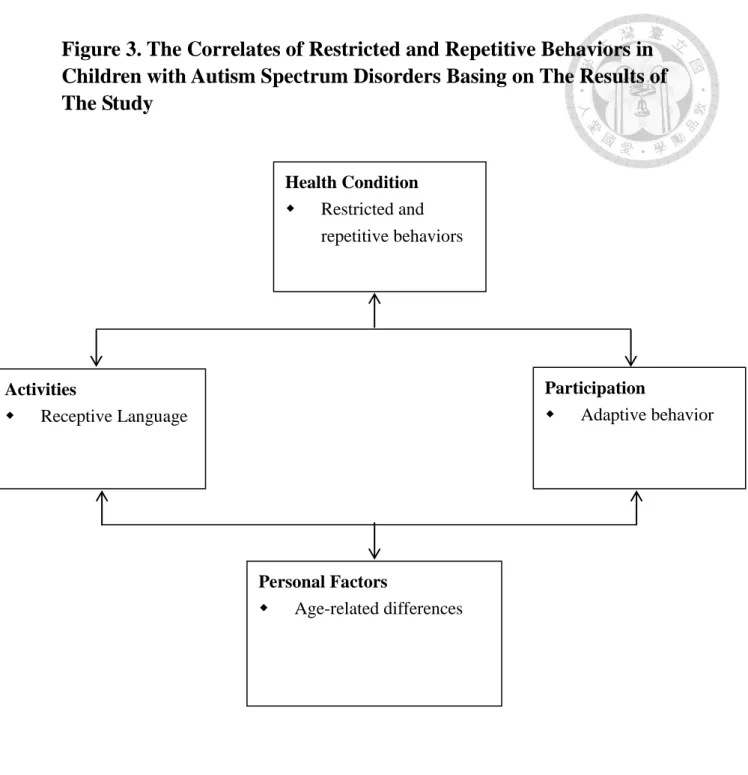
This study considered variables from the entire scope of the ICF-CY when
investigating the correlates of RRBs in children with ASD. Our hypothesis was that
severity, sensory processing, expressive language, receptive language, adaptive behavior,
age, anxiety and patient-child relationship quality would significantly correlate with
overall RRBs. Results of this study partially support our hypotheses, i.e., only receptive
language, adaptive behavior, and child’s age being the significant correlates of RRBs
(Table 5 and Figure 3). Furthermore, our finding was consistent with previous studies
(Cuccaro et al., 2003; Delinicolas & Young, 2007; Kozlowski & Matson, 2012;
Ray-Subramanian & Ellis Weismer, 2012). For instance, Cuccaro et al. (2003) and
Joosten et al. (2010) indicated that children with ASD scoring lower in adaptive
behavior would be more likely to manifest repetitive sensory motor actions and
stereotypical behaviors (Cuccaro et al., 2003; Joosten & Bundy, 2010).The correlates of
each subtype of RRBs are somewhat similar. First, delayed receptive language skill is
the correlate for all the subtypes of repetitive behavior except for ritualistic and
sameness behavior and restricted interests. Second, adaptive behavior and age were the
significant correlates of stereotypic behavior.
Receptive language skill is in the area of activity in the ICF-CY. Results of our
38
study lend partially support to previous study (Ray-Subramanian & Ellis Weismer,
2012). Ray-Subramanian et al. (2012) indicated receptive language skills were
negatively associated with RRBs at ages 2 and 3. In our study, receptive language skill
was the correlates of three subtypes of RRBs, i.e., stereotypic, self-injurious and
compulsive behaviors. Among them, receptive language skill was the only correlate of
two types of RRBs, i.e., self-injurious and compulsive behaviors. The findings from our
study suggest that the poorer the receptive language skill the severer the stereotypic behavior, self-injurious, and compulsive behaviors. The explanation may be that due to difficulty understanding others ’commands, children with ASD decreased their anxiety
by RRBs (Joosten et al., 2009; Leekam et al., 2011). Another explanation may be that
children with ASD indulged in the stereotypic behavior and compulsive behaviors to
decrease boringness (Leekam et al., 2011; Zentall & Zentall, 1983) .
The finding that adaptive behavior is the correlate of stereotypic behavior is
consistent with Cuccaro et al.’s study that children with ASD had poorer adaptive
behavior would have higher repetitive sensory motor actions(Cuccaro et al., 2003). The
reason may be that children with poor adaptive behavior may use repetitive sensory
motor actions or stereotypic behaviors as a coping strategy such as body rocking to
reduce anxiety (Leekam et al., 2011).
Our study showed that stereotypic behavior increased with age, a finding
39
inconsistent with Esbensen et al.’s (2009) study which showed older participants
tended to exhibit fewer RRBs than younger participants. The discrepancy may probably
be due to differences in age range of participants. The age range of the participants in our study is from 3 to 9 but that of Esbensen et al.’s (2009) study is from 2 to 62. In
consistent with Militerni et al.’s (2002) and Richler et al.’s study (2010), our study
found that overall RRBs and stereotypic behavior increased with age. Militerni et al.’s (2002) study recruited individuals from age 2 to 4 and 7 to 11, and Richler et al.’s (2010)
study collected participants with the age range of 2 to 9. Our study also showed that
stereotypic behavior increased with age. Perhaps the RRBs gradually decrease in their
life span, but its prevalence remains high in preschool children and school children. The
stereotypic behavior may be a coping strategy for children with ASD to enable them to
either regulate high levels of arousal or to reduce anxiety (Leekam et al., 2011). Another
reason might be that the participants with older age in our study were more severe than
younger children.
It is interesting to note that no predictors entered into the models of restricted
interests, and ritual and sameness behavior respectively and both subtypes are
higher-level RRBs. A close examination of the data revealed that no variable was
significantly correlated with restricted interests, and ritual and sameness behavior in
Pearson correlation matrix. The correlates identified in previous studies such as adaptive