國立臺灣大學獸醫專業學院臨床動物醫學研究所 碩士論文
Graduate Institute of Veterinary Clinical Sciences School of Veterinary Medicine
National Taiwan University Master Thesis
比較敏伯斯登與伊馬替尼治療犬高風險皮膚肥大細胞瘤之 治療效果
Comparison of Treatment Effect for Vinblastine-based
Chemotherapy and Imatinib Alone in High-risk Canine Cutaneous Mast Cell Tumor
陳映華
Ying-Hua Chen
指導教授:李繼忠 博士
Advisor: Jih-Jong Lee, DVM, MS, Ph.D.
中華民國 109 年 7 月
中文摘要
肥大細胞瘤是犬隻最常見的皮膚腫瘤,在無法進行局部控制的情況下會使用 化學治療以及標靶治療等全身性治療。敏伯斯登為常用於肥大細胞瘤的第一線化 療藥物,除了單用之外也會搭配其他化療藥物使用,例如環磷醯胺。伊馬替尼是一
個酪氨酸激酶抑制劑,近期被發現可透過抑制失調的 KIT 蛋白進而抑制肥大細胞
瘤。然而個別病患應選擇化療還是標靶治療目前並沒有定論,因此本篇研究的目的 為比較在患有高轉移風險皮膚型肥大細胞瘤的犬隻使用以敏伯斯登為基礎的化療 和伊馬替尼的效果與毒性,並分析與無惡化存活期相關的預後因子。
本研究回溯性納入西元 2011 至 2019 年間,於國立臺灣大學生物資源暨農學
院附設動物醫院動物癌症治療中心以組織病理學或細胞學確診且無法切除之高轉 移風險皮膚型肥大細胞瘤,並使用以敏伯斯登為基礎的化療或伊馬替尼治療的犬 隻,分為敏伯斯登組(n = 21)以及伊馬替尼組(n = 20)進行比較。兩組的客觀反 應率沒有顯著差異(敏伯斯登組為 42.9%,伊馬替尼組為 35.0%,P = 0.606),然
而敏伯斯登組的臨床受益率(100.0%)顯著高於伊馬替尼組(80.0%,P = 0.048)。
兩組的中位無惡化存活期沒有顯著差異(敏伯斯登組為 83 天,伊馬替尼組為 51
天,P = 0.885)。敏伯斯登組的總體副作用發生率(71.4%)顯著高於伊馬替尼組
(35.0%,P = 0.019),而在個別比較時也有達到顯著差異的副作用種類為嗜中性球
低下(P = 0.048)以及精神不振(P = 0.021)。預後因子的部分,年紀小於 11 歲的 犬隻有顯著較長的中位無惡化存活期(P = 0.033),臨床分期第二期的犬隻也較第 四期的犬隻有顯著更長的中位無惡化存活期(P = 0.049)。
總結來說,使用以敏伯斯登為基礎的化療和伊馬替尼的治療效果相當,但敏伯 斯登組有較顯著的副作用。因此,在預期容易出現副作用並注重生活品質維持的病 患可以建議使用伊馬替尼。年齡與臨床分期為影響無惡化存活期的預後因子。
關鍵字:犬肥大細胞瘤、敏伯斯登、伊馬替尼
ABSTRACT
Mast cell tumor (MCT) is the most common canine cutaneous neoplasm. In cases that complete local control is impossible; often, systemic treatments are indicated, such as chemotherapy and tyrosine kinase inhibitor (TKI). Vinblastine (VBL) is a first-line chemotherapeutic agent often used alone or with other chemotherapeutic agents, such as cyclophosphamide (CTX). Imatinib is a TKI that has been recently shown to induce remission of MCT by inhibiting dysregulated KIT protein expression. The choice between chemotherapy and TKI for an individual patient remains equivocal. Therefore, the purpose of this study was to compare the efficacy and safety of VBL-based chemotherapy and imatinib in high-risk canine cutaneous MCT. The potential prognostic factors for the progression-free interval (PFI) were also investigated.
Dogs diagnosed with measurable high-risk cutaneous MCT by histopathology or cytology treated with VBL-based chemotherapy or imatinib alone at National Taiwan University Veterinary Hospital Animal Cancer Treatment Center from 2011 to 2019 were retrospectively enrolled and divided into VBL group (n = 21) or imatinib group (n = 20).
The objective response rate (ORR) was similar between the VBL group and the imatinib group (42.9% versus 35.0%, P = 0.606). However, the clinical benefit rate (CBR) was significantly higher for VBL group (100.0% versus 80.0%, P = 0.048). The median PFI was 83 days for the VBL group and 51 days for the imatinib group (P = 0.885). The incidence of side effects was significantly higher for VBL group (71.4% versus 35.0%, P
= 0.019), especially for neutropenia and lethargy (P = 0.048 and P = 0.021, respectively).
As for prognostic factors, median PFI was significantly longer for dogs younger than 11 years old, and also higher for dogs classified as stage 2 compared to stage 4 upon
multivariate analysis (P = 0.033 and P = 0.049, respectively).
In conclusion, the efficacy was similar between dogs treated with VBL-based chemotherapy and imatinib, but the toxicity was more prominent in the VBL group.
Therefore, imatinib may be advocated for patients that are expected to be more susceptible to adverse events and considering the quality of life. Age and clinical stage were prognostic factors for PFI in this study.
Keywords: canine mast cell tumor, vinblastine, imatinib
CONTENTS
中文摘要... i
ABSTRACT ... ii
CONTENTS ... iv
LIST OF FIGURES ... vi
LIST OF TABLES ... vii
LIST OF ABBREVIATIONS ... viii
Chapter 1 Literature review ... 1
1.1 Canine cutaneous mast cell tumor (cMCT) ... 1
1.2 Treatment of canine cMCT ... 2
1.3 VBL-based chemotherapy ... 3
1.4 TKIs ... 4
1.4.1 Dysregulation of tyrosine kinases in canine MCT ... 4
1.4.2 TKIs in veterinary medicine ... 4
1.4.3 Imatinib mesylate ... 5
1.4.4 Treatment decision between TKI and chemotherapy ... 6
1.5 Prognostic factors ... 6
Chapter 2 Introduction ... 8
Chapter 3 Materials and methods ... 9
3.1 Patient selection ... 9
3.2 Clinical stage ... 9
3.3 Tumor grade ... 10
3.4.1 VBL group ... 10
3.4.2 Imatinib group ... 11
3.5 Response ... 11
3.6 Toxicity ... 11
3.7 Statistical analysis ... 12
Chapter 4 Results ... 14
4.1 Demography ... 14
4.1.1 Patient characteristics ... 14
4.1.2 Tumor features and previous treatments ... 14
4.2 Treatment of VBL group ... 16
4.3 Treatment of imatinib group ... 16
4.4 Outcome ... 17
4.4.1 Response ... 17
4.4.2 PFI ... 17
4.5 Toxicity ... 18
4.6 Prognostic factors for PFI ... 19
Chapter 5 Discussion ... 20
5.1 Efficacy and toxicity ... 20
5.2 Prognostic factors ... 25
5.3 Limitations ... 27
Chapter 6 Conclusions ... 28
Figures... 29
Tables ... 36
REFERENCES ... 49
LIST OF FIGURES
Figure 1. The Kaplan-Meier curve for the progression-free interval (PFI) of the two groups. ... 29 Figure 2. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs achieved objective response in two groups. ... 30 Figure 3. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs achieved clinical benefit in two groups. ... 31 Figure 4. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs grouped by the age. ... 32 Figure 5. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs classified as stage 2 and stage 4. ... 33 Figure 6. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs classified as stage 3 and stage 4. ... 34 Figure 7. The Kaplan-Meier curve for the progression-free interval (PFI) for responders and non-responders. ... 35
LIST OF TABLES
Table 1. World Health Organization clinical staging system for mast cell tumors .... 36 Table 2. Comparison of characteristics of vinblastine and imatinib ... 37 Table 3. Veterinary cooperative oncology group – common terminology criteria for adverse events version 1.1 ... 38 Table 4. Comparison of patient characteristics between the two groups ... 39 Table 5. Comparison of tumor features and previous treatments between two groups ... 40 Table 6. Response to treatment in two groups ... 41 Table 7. Progression-free interval in two groups ... 42 Table 8. Episodes of toxicities classified according to the severity in two groups .... 43 Table 9. Incidence of toxicity in two groups ... 44 Table 10. Incidence of toxicity in two subgroups ... 45 Table 11. Univariate analysis of progression-free interval regarding patient characteristics ... 46 Table 12. Univariate analysis of progression-free interval regarding tumor features and previous treatments ... 47 Table 13. Multivariate analysis of possible prognostic factors for progression-free interval ... 48
LIST OF ABBREVIATIONS
Abbreviation Full description
ADL Activities of Daily Living
AgNOR Argyrophilic Nucleolar Organizer Regions
ALT Alanine Transaminase
CBR Clinical Benefit Rate
cMCT Cutaneous Mast Cell Tumor
CR Complete Remission
CTX Cyclophosphamide
FNA Fine-Needle Aspiration
GI Gastrointestinal
HPF High-Power Field
IV Intravenous
LN Lymph Node
LNN Lower Limit of Normal
MAS Masitinib
MCT Mast Cell Tumor
NR Not Reached
NTUVH National Taiwan University Veterinary Hospital OBD Optimal Biological Dose
ORR Objective Response Rate
PD Progressive Disease
PDGFR Platelet-Derived Growth Factor Receptor PFI Progression-Free Interval
PPN Partial Parenteral Nutrition
PR Partial Remission
RECIST Response Evaluation Criteria in Solid Tumors
RT Radiation Therapy
SC Subcutaneous
SD Stable Disease
TKI Tyrosine Kinase Inhibitor
TOC Toceranib
TPN Total Parenteral Nutrition
ULN Upper Limit of Normal
VBL Vinblastine
VCOG-CTCAE Veterinary Cooperative Oncology Group Common Terminology Criteria for Adverse Events
VCP Vinblastine-Cyclophosphamide-Prednisone/ Prednisolone VP Vinblastine-Prednisone/ Prednisolone
Chapter 1 Literature review
1.1 Canine cutaneous mast cell tumor (cMCT)
Canine cMCT is one of the most common cutaneous neoplasms in dogs, comprising 16% to 21% of all cutaneous tumors [1]. The incidence is higher in older dogs, with the mean age of 8 to 9 years; however, they have also been reported in younger dogs. There is no apparent sex predilection found. Although mixed-breed dogs have the highest incidence, several breeds are also predisposed, including Boxer, Boston terrier, English bulldog, Pug, Labrador, Golden retriever, and Schnauzer.
The clinical appearances of cMCT are variable, may present with tiny nodules that are a few millimeters in diameter, or masses that are several centimeters in diameter. The lesions are solitary in most of the cases, but multiple lesions are presented in 11% to 14%
cases, and they are most commonly found on the trunk, perineum, and limbs [1]. Release of mast cell granules, which contain histamine, heparin, and other vasoactive amines, may lead to erythema, edema, and ulceration of the surrounding tissue, and may even cause gastrointestinal (GI) ulceration, leading to clinical signs such as anorexia, vomiting, and diarrhea. The incidence of nodal and distant metastasis, including invasion of the spleen and liver, is reported to be 18% and 4.1%, respectively, for all cMCTs at initial diagnosis [2]. Although rarely seen, bone marrow infiltration can also occur in aggressive cMCTs.
In the majority of cases, cMCTs can be diagnosed based on fine-needle aspiration (FNA) cytology. Clinical staging of cMCT is based on World Health Organization (WHO) clinical staging system for MCTs [1] (Table 1), in which the number of lesions and the status of nodal or distant metastasis are taken into account, so the minimal diagnostic workup should include complete blood count, serum biochemistry, blood smear, three- view thoracic radiographs, abdominal ultrasound and FNA of the regional lymph nodes
(LNs).
The histologic grade of cMCTs was primarily based on the Patnaik 3-tier grading system [3], with grade I defined as low grade, grade II defined as an intermediate grade, and grade III defined as high grade; however, the Patnaik grade II cMCTs might present with some histologic variation among tumors, which resulted in unpredictable prognosis [4]. Kiupel 2-tier grading system was then developed to classified tumors into low-grade and high-grade to minimize the disagreement between pathologist with objective criteria, in which tumors were classified as high-grade if they possessed at least seven mitotic figures per 10 high-power field (HPF), at least three multinucleated cells per 10 HPF, at least three bizarre nuclei per 10 HPF or karyomegaly [5]. The 2-tier grading system was demonstrated to provide a more accurate prognosis than the 3-tier grading system [6].
1.2 Treatment of canine cMCT
As the biological behavior of canine cMCTs can vary significantly among cases, treatment decisions should take various factors into account, for example, clinical stage, tumor size, and tumor location.
Surgical excision should be attempted for local control of tumors in the area amenable for wide-margin excision, which includes up to a 3-cm lateral margin and one uninvolved fascial plane deep to the tumor. Adequate surgical resection may provide long-term control for low- and intermediate-grade cMCT [1], and re-excision of the dirty surgical margin or adjuvant radiation therapy (RT) may help achieve tumor-free margin in the case of incomplete excision.
In the cases of “high-risk” cMCTs, including dogs with Patnaik grade II MCTs with nodal or distant metastasis and dogs with Patnaik grade III or Kiupel high-grade MCTs,
local recurrence and distant metastasis will eventually develop following local control alone in most instances [1]. Hence, systemic treatments, including chemotherapy or TKI, are warranted for dogs with high-risk MCTs. Another indication for systemic treatments is treating measurable cMCTs that are not amenable for local control. Some studies have evaluated the efficacy of several chemotherapeutic agents for measurable cMCT, for example, VBL, CTX, and lomustine [7-10]. TKIs such as toceranib (TOC) and masitinib (MAS), have also been studied in such cases [11, 12].
1.3 VBL-based chemotherapy
VBL is an antimicrotubule agent commonly used in canine cMCTs, it interferes with the polymerization or depolymerization of the microtubules, resulting in the arrest of cell division. In one study, single-agent VBL resulted in a 12% to 27% objective response in 51 dogs with non-resectable grade II or grade III cMCTs [9]. In another study, 18 dogs with measurable grade II or grade III cMCTs were treated with the combination therapy of VBL and prednisone (VP protocol). VBL was given as a rapid intravenous (IV) bolus at 2 mg/m2 every 1-2 weeks; prednisone was administered orally at an initial dose of 2 mg/kg daily, then tapered and discontinued over 12-26 weeks. This protocol resulted in a 47% objective response and a median response duration of 154 days. Adverse events were noted in 20% of patients and considered mild and self-limited in most cases [7] (Table 2).
CTX is an alkylating anticancer agent that functions by interfering with DNA replication as well as RNA transcription and replication. A study evaluated the combination of vinblastine-cyclophosphamide-prednisone (VCP protocol) for the treatment of canine high-grade MCTs. VBL was administered as a rapid IV bolus at 2-2.2 mg/m2 every three weeks (on day 1 of the 21-day protocol); CTX was administered at
200-250 mg/m2 every three weeks either orally (over day 8-11 of the 21-day protocol) or as a rapid IV bolus (on day 8 of the 21-day protocol); prednisone was administered orally at an initial dose of 1 mg/kg daily, then tapered and discontinued over 24-32 weeks.
Eleven dogs were treated in the presence of gross lesions, resulting in a 64% objective response and a median progression-free survival time of 74 days. Only minimal toxicity was seen in all treated dogs [8].
1.4 TKIs
1.4.1 Dysregulation of tyrosine kinases in canine MCT
Tyrosine kinases are cellular proteins that take part in normal cell signal transduction.
Binding of external signals generate from growth factors or other stimuli initiates the phosphorylation of tyrosine kinases, leading to the generation of intracellular signaling that regulates cell growth, differentiation, and motility. Dysregulation of tyrosine kinases results in persistent autophosphorylation in the absence of external signals and eventually leads to uncontrolled cell proliferation and survival [12].
The mutation of tyrosine kinase KIT, which is encoded by the c-kit gene, has been identified in about 8.3% to 17% of canine cMCTs, with a higher incidence of up to 35%
reported in higher grade cMCTs [13-17]. The presence of c-kit mutations is associated with worse prognosis, including increased risk of local and systemic recurrence, shorter median progression-free survival, shorter median overall survival, and increased risk of MCT-related death [1, 13, 14].
1.4.2 TKIs in veterinary medicine
TKIs work by blocking the ATP-binding site of tyrosine kinases, inhibiting the
orally bioavailable TKIs, TOC, and MAS were approved for treating canine MCTs, and limited studies have also been performed with the human TKI, imatinib mesylate (Gleevec, Novartis) [1, 12].
1.4.3 Imatinib mesylate
Imatinib mesylate is a TKI used initially in the human patient against the BCR-ABL fusion protein in chronic myeloid leukemia. It has also been demonstrated to have antitumor activity against other tumors by targeting several mutated kinases, for example, KIT, platelet-derived growth factor receptor (PDGFR), ABL1, and ABL2 [12, 18].
Imatinib has been used off-label for dogs and cats, similarly to most chemotherapeutic drugs in veterinary medicine [18]. Although no study has been performed to evaluate the pharmacokinetics of imatinib yet, some clinical studies have already shown the efficacy of imatinib against canine MCTs since 2008. In a study that enrolled 21 dogs with measurable cMCTs treated with imatinib (10 mg/kg daily), objective response was achieved in 10 dogs within 14 days of treatment initiation with response duration up to 63 days [19]. In another study, two dogs with aggressive MCTs presented with bone marrow involvement all achieved complete remission soon after treated with imatinib (4.4 mg/kg daily) [20]. In a review study, a total of 38 cases of MCTs treated with imatinib (10-12.7 mg/kg daily) have been reported in veterinary literature; of these, 16 cases had a detectable mutation in c-kit exon 8, 9 or 11, and all of them achieved complete or partial remission; of the 22 cases without a detectable mutation, objective response was only achieved in 5 cases [18]. Imatinib appears to be well-tolerated at an approximate dose of 10 mg/kg daily or less. Adverse events were only reported in a small number of dogs in previous studies, including neutropenia, vomiting, and elevation of serum liver enzymes, which were usually mild and improved following dose reduction or
temporary withdrawal of imatinib [18] (Table 2).
1.4.4 Treatment decision between TKI and chemotherapy
The decision-making between TKI or chemotherapy for an individual patient with canine cMCT has been of interest in recent studies, especially for the c-kit mutation status.
In the registration trial and a preliminary study for TOC, the ORRs were significantly higher for tumors with c-kit mutation than those without; however, the long-term outcome was not reported [12, 21]. A similar finding was also reported in the registration trial for MAS and a study with a small number of patients treated with imatinib [19, 22]. However, in a recent study, there was no significant difference in ORR and overall survival time between patients with or without c-kit mutation treated with MAS, and the initial response to MAS was the most reliable prognostic factor for survival time [23]. In a prospective, randomized trial enrolling 88 dogs with grade II or grade III macroscopic cMCTs, the use of either KIT pattern or c-kit mutation status alone was not sufficient to make treatment decisions between TOC and VBL as the clinical outcomes were similar between two groups [24]. These results suggest that possession of c-kit mutation may indicate a better response rate to TKIs, but not the long-term outcome, and its utility for selection of MCT treatments remains equivocal [25, 26].
1.5 Prognostic factors
Various prognostic indicators have been identified for canine MCTs, and no single factor is entirely predictive of the biological behavior and clinical outcome. Histologic grade is the most reliable prognostic factor, dogs with well-differentiated MCTs usually experience long-term survival after adequate local control [27-30]; however, local
recurrence or metastasis eventually develop in 55% to 96% of dogs with undifferentiated MCTs, and most dogs die within one year despite managed with aggressive local treatment and adjuvant systemic treatment [1, 31, 32]. Several markers of proliferation are associated with more aggressive behavior, for example, Ki-67 and argyrophilic nucleolar organizer regions (AgNOR) [1].
Clinical-stage is also an important indicator. Stage 0 and stage 1, which represent local disease without nodal or distant metastasis, are associated with a better prognosis compared to the later stage. However, the prognostic significance of stage 3 remains controversial, some studies found an inferior outcome in dogs with stage 3 MCTs [33, 34], but other studies did not [7, 27, 32, 35, 36], and it is still unclear if multiple tumors represent a form of metastasis or multiple unrelated MCTs.
Other prognostic factors have also been reported. Certain breeds tend to develop MCTs with more benign behavior, for example, Boxer, Pug, Boston terrier, and Bulldog [37]. MCTs at prepuce, scrotum, and mucous membrane sites are associated with more aggressive behavior compared to that at other locations [27, 35, 38]. Local recurrence after surgical excision usually indicates a worse prognosis [7, 23, 39]. The presence of clinical signs, such as anorexia, vomiting, or diarrhea, may also relate to worse prognosis [27].
Chapter 2 Introduction
MCT is one of the most common cutaneous neoplasms in dogs, and the clinical appearance and biological behavior can vary significantly among cases [1]. Wide-margin excision is the mainstay of treatment. However, some tumors are non-resectable due to the size and the location, so systemic treatments, including chemotherapy and TKI, are indicated in those cases, especially for the tumors with aggressive behavior.
VBL is an antimicrotubule agent often used in the first-line chemotherapy in canine MCT, with or without the combination of other cytotoxic agents, such as CTX. VBL- based chemotherapies are reported to elicit an objective response in about 40% to 60% of cases with well-tolerated toxicities, mainly neutropenia and GI signs [7, 8, 24]. Imatinib is a TKI that has been recently shown to result in remission of canine MCT by inhibiting dysregulated KIT protein. The efficacy and safety are only reported in a few retrospective case studies, with a response rate range from 45% to 55% and mild toxicities in a small number of cases [18-20].
The choice between chemotherapy and TKI for an individual patient remains equivocal, and there has been no study comparing the use of VBL-based chemotherapy and imatinib. Therefore, the purpose of this study was to compare the efficacy and safety of VBL-based chemotherapy and imatinib in non-resectable high-risk canine cMCTs.
Besides, the potential prognostic factors for median PFI were also investigated.
Chapter 3 Materials and methods
3.1 Patient selection
The medical records from client-owned dogs with high-risk cMCTs treated with VBL-based chemotherapy (including VCP and VP protocol) or imatinib at National Taiwan University Veterinary Hospital (NTUVH) Animal Cancer Treatment Center from 2011 to 2019 were retrospectively reviewed. The patients were grouped into the VBL group or the imatinib group. High-risk MCT was defined as histopathologically diagnosed Patnaik grade III or Kiupel high-grade MCT [3, 5], or histopathologically diagnosed Patnaik grade II or cytologically diagnosed MCT with the presence of cytologically confirmed nodal or visceral metastatic disease. Other criteria for inclusion in the study included measurable gross lesion and available medical records. Patients treated with concurrent antineoplastic treatment other than steroids, including chemotherapy, target therapy, and RT, were excluded. Prior chemotherapy or target therapy was allowed if more than three weeks had elapsed since the last treatment or progressive disease observed.
The following data were recorded for each patient: the institution of treatment, age at the time of diagnosis, breed, sex, body weight, tumor location, the sum of the longest diameter of target lesions, previous treatment, clinical stage and substage, and histological grade. Treatment information was also collected, including the number of doses, dose interval, dosage, response, and adverse events.
3.2 Clinical stage
All patients underwent clinical staging according to the WHO clinical staging system for MCTs [1] (Table 1). The results of physical examination, complete blood count,
serum biochemistry panel, blood smear, thoracic radiography, abdominal ultrasound, fine-needle aspiration of the regional lymph node, and/or fine-needle aspiration of the spleen were included. Cases with honeycomb appearance of the spleen would also be classified as stage 4 even without cytological confirmation.
3.3 Tumor grade
Tumors were classified as Grade I, Grade II, or Grade III according to the Patnaik grading system, or classified as low-grade or high-grade according to the Kiupel grading system [5] by the pathologist in School of Veterinary Medicine, National Taiwan University.
3.4 Treatments
3.4.1 VBL group
The patients in the VBL group received either VCP protocol or VP protocol, and the regimens depended on clinicians’ preference. In VCP protocol, VBL (Vinblastine Injection, Hospira) was administered as a rapid IV bolus at 2 mg/m2 to 3 mg/m2 every three weeks (on day 1 of the 21-day protocol). CTX (Endoxan, Baxter) was administered at 200 mg/m2 to 250 mg/m2 every three weeks orally (over day 8 to day 9 of the 21-day protocol). In VP protocol, VBL was administered as a rapid IV bolus at 2 mg/m2 to 3 mg/m2 every one to two weeks. Prednisolone was administered orally at a dosage range of 1 mg/kg/day to 2 mg/kg/day, then tapered over several weeks on a clinician-dependent basis.
3.4.2 Imatinib group
Imatinib (Gleevec, Novartis) was administered orally at a target dosage of 10 mg/kg once daily. Prednisolone was administered orally at a dosage range from 1 mg/kg/day to 2 mg/kg/day, then tapered over several weeks on a clinician-dependent basis.
3.5 Response
Antitumor responses were evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST) criteria [40]. Target lesions were measured with calipers at each recheck, and the sum of the longest diameters of each target lesion would be recorded in the case of multiple tumors. Responses were calculated by the formula listed below:
tumor response = [(post-treatment measurement – pre-treatment measurement) / pre- treatment measurement] x 100%, then categorized as complete remission (CR; the disappearance of all target lesions and all lymph nodes <10 mm short axis), partial remission (PR; >30% but <100% decrease in the sum of diameters of target lesions), progressive disease (PD; at least a 20% increase in the sum of diameters of target lesions or appearance of a new lesion), stable disease (SD; neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD).
3.6 Toxicity
Adverse events were evaluated based on the results of the blood exam and patient history at each recheck. They were attributed to the study treatment if they occurred or increased in severity during or after exposure to the drug while no evidence of disease progression, showing dose-response patterns in the individual patient, and resolved with drug interruption [41]. Treatment-related adverse events were then graded from 1 to 5
based on the Veterinary Cooperative Oncology Group Common Terminology Criteria for Adverse Events (VCOG-CTCAE) [42] (Table 3).
3.7 Statistical analysis
To compare the demographic distribution and the tumor features between groups, we have conducted the following tests. Pearson’s chi-square test was used in categorical data including breed, sex, stage, substage, had received previous steroid treatment or not, previous systemic treatment, local recurrence or not, and tumor location. If the expected value of a given cell in the comparison was less than five, Fisher’s exact test was substituted for Pearson’s chi-square test. The Mann-Whitney U test compared continuous data including body weight, age, the sum of the longest diameter of target lesions, and median dosage of prednisolone.
ORR, CBR and PFI were defined as below: The ORR was defined as the percentage of patients that had experienced CR or PR The CBR was defined as the percentage of patients that had experienced CR, PR, or SD [40]. PFI was calculated from the date of treatment initiation to the date of PD.
To compare ORR and CBR between groups, Pearson’s chi-square test was used, but Fisher’s exact test was used instead if the expected value of a given cell in the comparison was less than five. Median PFI was calculated by the Kaplan-Meier method. Cases were censored if they had not developed PD at the time of data analysis or treatment withdrawn due to reasons unrelated to disease progression. The difference of median PFI between groups was assessed with the log-rank test.
The incidence of adverse events between groups was analyzed by Pearson’s chi- square test or by Fisher’s exact test if the expected value of a given cell in the comparison
was less than five.
Univariate analysis to assess potential prognostic factors in PFI was performed by the Kaplan-Meier method with the log-rank test. Factors included age, breed, sex, body weight, the sum of the longest diameter of the target lesions, local recurrence or not, tumor location, the median dosage of prednisolone, stage, substage, had received previous steroid treatment or not, previous systemic treatment, and objective response to the treatment. Factors found to be significant (P < 0.05) in univariate analysis were then included in multivariate analysis using the Cox proportional hazards model.
Statistical significance was established as P < 0.05. All statistical analyses were performed with SPSS v. 25 software.
Chapter 4 Results
4.1 Demography
4.1.1 Patient characteristics
A total of 41 dogs fulfilled the inclusion criteria. Twenty-one dogs received VBL- based chemotherapy, including eleven dogs treated with VCP protocol and ten dogs treated with VP protocol, and 20 dogs received imatinib target therapy. There were 24 (58.5%) pure breeds and 17 (41.5%) mixed breeds. The median age was eleven years (range 6-15 years) in the VBL group and ten years (range 4-17 years) in the imatinib group. Twenty-one (51.2%) dogs were female (1 intact, 20 spayed), and twenty (48.8%) dogs were male (11 intact, 9 castrated). Median body weight was significantly higher in VBL group (17.6 kg, range 4.9-36.8 kg) compared to imatinib group (10.9 kg, range 2.6- 34.5 kg; P = 0.003). No significant differences observed in the breed, age, and, sex (Table 4).
4.1.2 Tumor features and previous treatments
In VBL group, one dog (4.8%) was stage 1, 4 dogs (19.0%) were stage 2, 7 dogs (33.3%) were stage 3, and 9 dogs (42.9%) were stage 4; however, abdominal ultrasound was not performed for staging in 3 dogs (1 classified as stage 2, 2 classified as stage 3).
In imatinib group, 6 dogs (30.0%) were stage 2, 8 dogs (40.0%) were stage 3, and 6 dogs (30.0%) were stage 4; abdominal ultrasound was not performed in 5 dogs (1 classified as stage 2, 4 classified as stage 3). In the VBL group, ten dogs (47.6%) were substage a, and 11 dogs (52.4%) were substage b. In imatinib group, 11 dogs (55.0%) were substage a, and 9 dogs (45.0%) were substage b. The median sum of the diameter of target lesions
the imatinib group. In the VBL group, tumors were located on the trunk in six dogs (28.6%), on limbs in three dogs (14.3%), and ten dogs (47.6%) had multiple cutaneous tumors, two dogs (9.5%) had only metastasized lymph nodes as gross lesions. In imatinib group, tumors were located on the trunk in five dogs (25.0%), on limbs in two dogs (10.0%), on the head in two dogs (10.0%), and nine dogs (45.0%) had multiple cutaneous tumors, two dogs (10.0%) had only metastasized lymph nodes as gross lesions. The tumors were local recurrent in eleven dogs (52.4%) in the VBL group and ten dogs (50.0%) in the imatinib group. No significant difference observed in the clinical stage, substage, sum of the diameter of target lesions, tumor location, and local recurrent tumor between the VBL group and the imatinib group (Table 5). However, in VBL group, there were more dogs classified as substage a in dogs receiving VCP protocol (n = 8; 72.7%) than in dogs receiving VP protocol (n = 2; 20.0%; P = 0.030).
Seven dogs (33.3%) in the VBL group were diagnosed with cMCTs by histopathology, including 2 Patnaik grade II, 1 Patnaik grade II-III, 1 Patnaik grade III, and 3 Kiupel high-grade cMCTs. Ten dogs (50.0%) dogs in the imatinib group were diagnosed with cMCT by histopathology, including 1 Patnaik grade I-II, 2 Patnaik grade II-III, 2 Patnaik grade III, and 5 Kiupel high-grade cMCTs. All dogs with Patnaik grade I-II or Patnaik grade II cMCTs were presented with LN metastasis or distant metastasis.
Four dogs (19.0%) had received other systemic treatments previously in VBL group, including imatinib (n = 1), palladia (n = 2), and CTX (n = 1). Nine dogs (45.0%) had received other systemic treatments previously in imatinib group, including VBL (n = 4), CTX (n = 4), chlorambucil (n = 2), palladia (n = 5). Ten dogs (47.6%) had received steroids previously in the VBL group, and 13 dogs (65.0%) had received steroids previously in the imatinib group. No significant difference observed in the distribution of dogs that had received previous systemic treatment or steroids between two groups (Table
5). Ancillary medications were concurrently given for prevention or alleviation of paraneoplastic syndromes in all cases based on the clinicians’ judgment, including diphenhydramine, famotidine, and sucralfate.
4.2 Treatment of VBL group
A total of 21 dogs received a median of 3 VBL doses (range 1-8 doses), with median dosage at 2.25 mg/m2 (range 2-2.55 mg/m2) and a median dose interval of 2 weeks (range 1-6 weeks). For dogs receiving VCP protocol, the median dosage of VBL was 2.25 mg/m2 (range 2-2.5 mg/m2), with median dose interval of 3 weeks (range 1-6 weeks); the median dosage of CTX was 250 mg/m2 (range 200-250 mg/m2), with median dose interval of 3 weeks (range 1-6 weeks). For dogs receiving VP protocol, the median dosage of VBL was 2.39 mg/m2 (range 2-2.55 mg/m2), with a median dose interval of 2 weeks (range 1- 4 weeks). Six dogs experienced dose escalation of VBL (3 in VCP subgroup, 3 in VP subgroup), and two dogs experienced dose reduction of VBL due to unfavorable adverse effects (all in VCP subgroup). All dogs received concurrent prednisolone, and the median dosage of prednisolone was 0.85 mg/kg/day (range 0.25-2.25 mg/kg/day). For dogs receiving VCP protocol, the median dosage of prednisolone was 0.85 mg/kg/day (range 0.25-2 mg/kg/day); for dogs receiving VP protocol, the median dosage of prednisolone was 0.55 mg/kg/day (range 0.25-2.25 mg/kg/day). There was no significant difference in the dosage of prednisolone (P = 0.695) between dogs treated with VCP or VP protocol.
4.3 Treatment of imatinib group
The median dosage of imatinib was 9.3 mg/kg/day (range 2.3-12.7 mg/kg/day). Two
for dose reduction was CR in 2 dogs and SD in 1 dog. Eighteen dogs received concurrent prednisolone, with the median dosage at 0.5 mg/kg/day (range 0.15-2 mg/kg/day).
The median dosage of prednisolone was not statistically different between the VBL group and the imatinib group (P = 0.212).
4.4 Outcome
4.4.1 Response
In the VBL group, one dog achieved CR, eight dogs achieved PR, and 12 dogs achieved SD. The ORR in the VBL group was 42.9%, and the CBR was 100.0%. The ORR in VCP subgroup was 54.5% (1 CR and 5 PR), and was 30.0% (3 PR) in VP group (P = 0.387). The median time to response was 14 days (range 7-49 days) for responders.
In the imatinib group, three dogs achieved CR, four dogs achieved PR, and nine dogs achieved SD. The ORR in the imatinib group was 35.0%, and the CBR was 80.0%. The median time to response was 17 days (range 7-35 days) for responders.
There was no statistical difference in ORR between 2 groups (P = 0.606); however, the CBR was significantly higher in the VBL group than in the imatinib group (P = 0.048) (Table 6).
4.4.2 PFI
The median PFI was 83 days (range 7-239 days) in VBL group, with a median PFI of 121 days (range 7-239 days) in VCP subgroup and 55 days (range 14-83 days) in VP subgroup (P = 0.290). Eleven dogs were censored during follow-up, and the reason for drug withdrawal included the clients’ request (n = 4), unrelated death (n = 2), unfavorable side effects (n = 2), remaining CR (n = 1), remaining SD (n = 1), and undergoing surgical
excision (n = 1).
The median PFI was 51 days (range 7-415 days) in the imatinib group. Nine dogs were censored during follow-up, and the reason for drug withdrawal included the clients’
request (n = 4), unrelated death (n = 1), remaining CR (n =1), remaining SD (n = 1), receiving RT (n = 1), and lost to follow-up (n = 1).
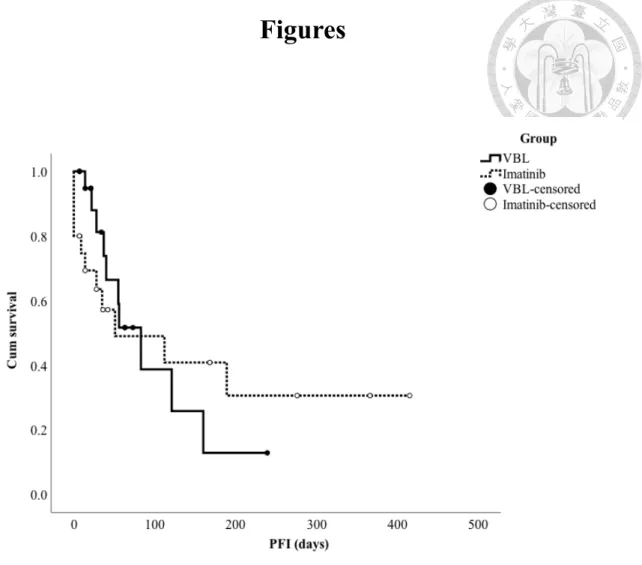
The median PFI between 2 groups was not significantly different (P = 0.885), and was neither statistically different for dogs that achieved objective response or clinical benefit (P = 0.080 and P = 0.387, respectively) (Table 7) (Figure 1-3).
4.5 Toxicity
Adverse effects were noticed in 15 (71.4%) dogs in the VBL group and 7 (35.0%) dogs in the imatinib group (P = 0.019) (Table 9) and were considered mild in most instances (Table 8).
In VBL group, neutropenia was noticed for five episodes (all were grade 1) in 5 (23.8%) dogs, lethargy was noticed for eight episodes (grade 1) in six (28.6%) dogs, anorexia was noticed for five episodes (2 grade 1, 3 grade 2) in five (23.8%) dogs, GI signs were noticed for eleven episodes (grade 1) in six (28.6%) dogs, and elevation of alanine transaminase (ALT) was noticed for twelve episodes (6 grade 1, 5 grade 2, 1 grade 3) in nine (42.9%) of dogs. There was no significant difference in the incidence of adverse effects between VCP and VP subgroups (Table 10).
In imatinib group, neutropenia and lethargy were not reported in any dog, anorexia was noticed for three episodes (grade 1) in two (10.0%) dogs, GI signs were noticed for two episodes (grade 1) in two (10.0%) dogs, and elevation of ALT was noticed for six episodes (2 grade 1, 4 grade 2) in four (20.0%) dogs (Table 9).
The incidence of neutropenia and lethargy was significantly higher for dogs in the VBL group than the imatinib group (P = 0.048 and P = 0.021, respectively) (Table 9).
4.6 Prognostic factors for PFI
Prognostic factors that were subjected to the univariate analysis included age (< or
≥ median age), breed, sex, body weight (< or ≥ median body weight), the sum of the diameter of the target lesions (< or ≥ median sum), local recurrence or not, tumor location, the median dosage of prednisolone (< or ≥ median dosage of prednisolone), stage, substage, had received previous steroid treatment or not, previous systemic treatment, and objective response to the treatment.
Variables that had a significant influence on PFI identified on the univariate analysis included age, stage, and objective response (Table 11 and Table 12). Median PFI was significantly shorter for dogs older than 11 years old (51 days versus 189 days, P = 0.048) (Figure 4). Dogs classified as stage 4 had significantly shorter median PFI (35 days) compared to dogs classified as stage 2 (not reached, P = 0.005) and stage 3 (189 days, P
= 0.017) (Figure 5 and Figure 6). The median PFI for non-responders was also significantly shorter (40 days versus 160 days, P = 0.025) (Figure 7).
Upon multivariate analysis, age ≥ 11 years-old remained to be a negative prognostic factor for PFI (P = 0.033), with a hazard ratio of 3.710 (95% CI, 1.110-12.408). Dogs classified as stage 2 had significantly longer PFI compared to stage 4 (HR, 0.223; 95%
CI, 0.050-0.996; P = 0.049). There was no significant difference between the PFI of responders and non-responders (P = 0.231) (Table 13).
Chapter 5 Discussion
5.1 Efficacy and toxicity
Systemic treatments, including chemotherapy and TKI, are options for dogs with non-resectable cMCTs when RT is not accessible, especially for those with tumors showing high metastatic-risk. For chemotherapy, VBL is commonly used as the first-line agent alone or combined with other chemotherapeutic agents, such as CTX [8]. For TKI, imatinib has not been thoroughly investigated as TOC or MAS, and its clinical application is only reported in some retrospective case studies with a small population [18-20, 43- 45]. Our study retrospectively compared the efficacy and safety of VBL-based chemotherapy and imatinib in dogs with macroscopic high-risk cMCTs, which has not been reported at the time this study was ended.
The population of dogs in our study was similar to those of previous studies.
However, the retrospective nature of our study indeed resulted in some bias. Firstly, when comparing patient characteristics, body weight was significantly higher in the VBL group, and it was most likely a bias caused by the fact that the cost of imatinib was much higher than chemotherapeutic agents, making it unaffordable for some clients, especially for those with large-breed dogs. Despite that, in statistical analysis, the distribution of body weight seemed not to influence the clinical outcome. Secondly, there were more dogs classified as substage b in the VP subgroup compared to the VCP subgroup (80.0% versus 27.3%, P = 0.03), and it was caused by the different preferences between clinicians choosing the treatment regimen. The presence of systemic illness might cause the patients to be more susceptible to the treatment toxicity; however, the incidence of side effects was not significantly different between the two subgroups.
versus 35.0%, P = 0.606), but the CBR was significantly higher in VBL group (100.0%
versus 80.0%, P = 0.048). The difference in mechanism of action could explain it.
Imatinib inhibited the tumor growth by targeting mutated KIT proteins, so tumors that did not show clinical benefit was assumed to possess wild-type c-kit gene. For VBL, it acted by interfering with the mitosis of highly proliferative tumor cells, so at least SD could be expected initially in most cases.
There was no significant difference in PFI between two groups (83 days for the VBL group and 51 days for the imatinib group, P = 0.885). When comparing dogs that achieved an objective response, the PFI was longer for those in the imatinib group. Still, statistical significance was not reached (not reached versus 55 days for the VBL group, P = 0.080), and it might be due to the small case number of responders. However, the retrospective nature of our study could also result in bias that influences PFI. As there was no standard schedule for regular follow-up, disease progression would be recorded earlier for patients with shorter recheck interval and recorded latter for patients with longer recheck interval, resulted in longer PFI in the latter cases. A further prospective study with a larger population is required to confirm our findings.
One retrospective study reported an ORR of 63.6% for dogs with macroscopic, Patnaik grade II to III cMCTs treated with VCP protocol, which was higher than that of the VCP subgroup in our study (54.5%). The median PFI was 74 days in that study [8].
Two studies using VP protocol for dogs with similar disease status reported ORR of 43%
and 47%, which was also higher than that of the VP subgroup in our study (30.0%). The median PFI was 78 and 154 days [7, 24]. The distribution of histologic grade might be a reason for the difference in clinical outcome between previous studies and our study;
however, it could not be confirmed as the histologic grade was only reported in 7 cases in VBL group in our study.
In previous studies, the overall ORR for dogs with similar disease status treated with imatinib was 47.6% to 55.3%, with ORR up to 100.0% for tumors possessing mutated c- kit and 22.7% to 31.3% for tumors possessing wild-type c-kit; however, the median PFI
was not reported [18, 19]. In the present study, ORR seemed to be lower (35.0%).
However, the distribution of the mutation status of the c-kit gene in our population was not evaluated, so it remained unknown if it was the factor influencing our outcome or not.
Besides, imatinib was administered after the failure of chemotherapy and steroid treatment in about half of the cases. It is reported that steroids and some chemotherapeutic agents, such as VBL and chlorambucil, are P-glycoprotein inducers [46], and imatinib is a substrate to P-glycoprotein [47, 48]. Hence, the overproduction of P-glycoprotein caused by previous treatments might have resulted in resistance to imatinib, causing an inferior outcome. This phenomenon has been reported in MAS, which is also a substrate to P-glycoprotein [22].
Corticosteroids are widely used in cases of canine MCT due to their effect of decreasing the growth and reproductive rates of tumor cells [49], reducing the local inflammation caused by the tumor, and also improving the patients’ activity and appetite.
An early study reported an ORR of 20% for cutaneous and subcutaneous canine MCTs treated with oral prednisone [49]. However, the administration of corticosteroids is thought to be mildly beneficial and lack durable efficacy in other later studies, especially in the cases of high-grade MCTs [8, 50]. Most of the patients in our study were given prednisolone concurrently, but all of them had experienced PD when taking prednisolone before starting VBL or imatinib treatment, so the remission of the tumor was less likely to be caused by prednisolone. In contrast, imatinib and VBL are both substrates to P- glycoprotein [48], so the ORR and PFI in both groups might be affected negatively by the
prednisolone.
There was a significant difference in overall toxicity between the two groups. The proportion of dogs experienced side effects during treatment was twice higher in VBL group than in imatinib group (71.4% versus 35.0%, P = 0.019), and it could be a reason to advocate for the use of imatinib in patients expected to be more susceptible to adverse events and considering about quality of life. It was predictable that significantly more dogs were affected by neutropenia in the VBL group (23.8% versus 0.0%, P = 0.048) as bone marrow suppression was the dose-limiting toxicity of VBL, and was rarely reported for imatinib [18]. Lethargy was only reported in the VBL group (28.6% versus 0.0%, P = 0.021); however, as the interpretation of lethargy could be subjective, the inter-observer bias could exist. It should be noticed that although the effort was made to verify the side effects attributed to the treatment, the paraneoplastic syndromes caused by MCT, which also elicit lethargy, anorexia, and GI signs, still could not be excluded entirely.
Furthermore, the influence of concurrent prednisolone administration on the elevation of ALT in both groups could neither be excluded. Overall, both treatments were well tolerated as the toxicities were mild and self-limiting; in most instances, only two dogs required dose reduction due to side effects in the VBL group in our study.
The toxicity of VBL-based chemotherapy was reported in about 10% to 20% patients in two retrospective studies [7, 8]. Only the abnormality of complete blood count was evaluated, the result of serum biochemistry was not reported. Besides, the substage and tumor burden was not reported in both studies, which might also affect the susceptibility to adverse events. In a recent prospective clinical trial, the incidence of side effects was 89% [24], which was higher than that in our study. However, the starting dose of VBL was 2.5 mg/m2 for all patients in that study and was 2 mg/m2 for most patients in our study.
Side effects, including neutropenia, GI signs, and elevation of serum liver enzyme, are rarely reported in the clinical studies of imatinib with or without concurrent administration of steroids [18-20, 45]. In contrast, side effects were detected in 35% of patients in the present study. It could be explained by the fact that 45% of our patients were classified as substage b, causing them to be more susceptible to the toxicity elicited by the treatment.
VCP and VP protocols are commonly used in canine MCT, but there has been no research comparing the efficacy and toxicity of both protocols. In our study, the tendency to a better outcome and a higher incidence of side effects in the VCP subgroup were observed, but the differences were not significant. Although the median dose interval of VBL was longer in the VCP subgroup (3 weeks) than in the VP subgroup (2 weeks) when the administration of CTX was taken into account, the median dose interval of chemotherapeutic agents would be 1.5 weeks in VCP subgroup. The relative dose intensity of the combination would be 1.3 versus 1 for a single agent. As there were only 11 and 10 cases in each subgroup, a prospective study with a larger population is warranted to confirm this finding.
It is worth noting that TKI is classified as a cytostatic agent rather than a cytotoxic agent, which most often inhibit tumor growth and prevent metastasis, but not necessarily expected to shrink tumors. If WHO or RECIST criteria were used, such clinical benefit would be ignored. Consequently, the best way for response evaluation and the expected treatment endpoint for TKI may be different from those applied for chemotherapy, so other criteria should be incorporated, such as the saturation and modulation of the target or the alteration of the target-mediated pathway. Moreover, target therapies usually have maximal target inhibition at non-toxic doses, which is known as the optimal biological
imatinib has not been identified currently, and it is possibly lower than the dosage commonly used, which is 10 mg/kg/day. Durable CR was observed when imatinib was used at a dosage of 4.4 mg/kg/day for two dogs with measurable MCT and bone marrow involvement in a case study [20]. Hence, further research is required for the practical response evaluation of TKI, and also for finding out the OBD of imatinib.
5.2 Prognostic factors
The clinical appearance and biological behavior of canine cMCT are variable, and many factors are affecting the clinical outcome. Several negative prognostic factors have been reported in canine cMCTs, for example, histologic grade, clinical stage, local recurrence, and systemic signs [1]. However, in our study, the age and clinical stage at diagnosis were the only two factors that significantly influence the time to progression.
Dogs older than 11 years-old had significantly shorter median PFI than those younger than 11 years old (189 days versus 51 days; HR, 3.710; 95% CI, 1.110-12.408;
P = 0.048 and P = 0.033 for univariate and multivariate analysis, respectively). A similar
finding was only reported in a study of canine MCT treated with RT [52] and was thought to be associated with aging changes.
Dogs classified as stage 2 had significantly longer median PFI compared to stage 4 (not reached versus 35 days; HR, 0.223; 95% CI, 0.050-0.996; P = 0.005 and P = 0.049 for univariate analysis and multivariate analysis, respectively). This result was expectable as stage 4 might indicate a larger tumor burden or more aggressive tumor behavior compared to stage 2, and was also reported by other studies [1, 39]. A significant difference in PFI was not observed when comparing stage 1 to stage 4 in both univariate analysis and multivariate analysis, and it was likely due to the small number of patients
classified as stage 1. The median PFI between dogs classified as stage 3 and stage 4 was only significantly different in univariate analysis (189 days versus 35 days, P = 0.017), but not in multivariate analysis (P = 0.187). However, it should be noticed that abdominal ultrasound was not performed in 6 dogs classified as stage 3, so their clinical-stage might be underestimated.
In a retrospective study of canine MCT treated with MAS, the initial response to treatment was the only reliable prognostic factor [23]. Although the median PFI was longer for responders compared to non-responders in univariate analysis (160 days versus 40 days, P = 0.025) in the present study, the difference was not significant upon multivariate analysis (P = 0.231). The possible explanation was the small population of our study; hence, a prospective study with a larger population would be warranted to verify this finding.
Substage b and more significant target lesion, which were reported to be negative prognostic factors in previous studies, seemed to be associated with shorter median PFI in our study; however, a significant difference was not reached upon univariate analysis (P = 0.696 and P = 0.327, respectively). Local recurrence was also reported to be a negative prognostic factor; however, it was also not associated with the median PFI in our study. It might be due to the small population of our study or the selection bias that only patients with high metastatic-risk MCT were enrolled.
It was interesting that dogs received a higher median dosage of prednisolone during treatment had a trend toward shorter PFI, although the difference was not significant upon univariate analysis (P = 0.059). As mentioned, both VBL and imatinib were substrates to P-glycoprotein [48], so one possible explanation was that the administration of prednisolone might cause overproduction of P-glycoprotein, resulting in an inferior
sometimes concurrently prescribed for patients with more aggressive MCT that did not respond well to the chemotherapy or TKI treatment alone. Therefore, a prospective clinical trial would be required to figure out the influence of the administration of prednisolone during the treatment of canine cMCT.
Among the prognostic factors mentioned in previous studies, the histologic grade is the most predictive factor [1]. However, in our study, complete histological information was not available in more than half of the patients as most of their tumors were not amenable for surgery, thus, the influence of histologic grade was unable to investigate.
5.3 Limitations
There were several limitations to this study. Only dogs with non-resectable high- grade MCTs or cytologically diagnosed MCTs with metastasis were enrolled. However, it might lead to selection error, as the early stage high-grade MCTs without metastasis might be excluded, and the late-stage low-grade MCTs with metastasis might be included if they were diagnosed by cytology. Due to the retrospective nature, some data regarding the disease status were incomplete, for example, FNA of visceral organs was not performed in our patients for staging, and histopathological diagnosis of the target lesions and regional LNs was not available for all patients. Besides, both c-kit mutation status and KIT localization were not evaluated. The treatment choices were based on clinicians’
preference, and the cost of imatinib in some patients might prohibit its use. As there was no standard schedule for recheck during treatment, the incidence of toxicity and PFI might be affected by the frequency of assessment.
Chapter 6 Conclusions
In conclusion, when comparing the efficacy in treating measurable high-risk canine cutaneous MCT, only CBR was significantly higher for dogs treated with VBL-based chemotherapy than with imatinib, a significant difference was not observed in ORR and median PFI. The incidence of toxicity was significantly higher for dogs treated with VBL- based chemotherapy, especially for neutropenia and lethargy. Hence, imatinib could be advocated when adverse events are of great concern to the patient. Younger age and stage 2 compared to stage 4 were associated with a longer PFI in the study.
Figures
The median PFI for the VBL group (solid line, n = 21) and the imatinib group (dashed line, n = 20) was 83 days and 51 days, respectively. There was no significant difference in PFI between 2 groups (P = 0.885).
Figure 1. The Kaplan-Meier curve for the progression-free interval (PFI) of the two groups.
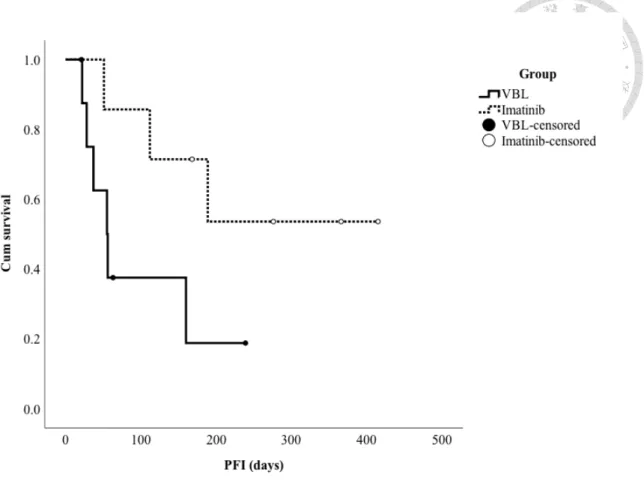
Figure 2. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs achieved an objective response in two groups.
For dogs achieved an objective response, the median PFI for the VBL group (solid line, n = 9) and the imatinib group (dashed line, n = 7) was 55 days and not reached, respectively. The difference was not significant (P = 0.080).
Figure 3. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs achieved clinical benefit in two groups.
For dogs achieved clinical benefit, the median PFI for the VBL group (solid line, n = 21) and the imatinib group (dashed line, n = 16) was 83 days and 189 days, respectively. The difference was not significant (P = 0.387).
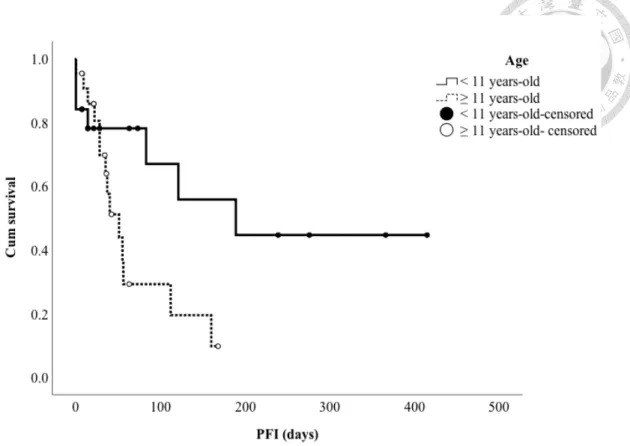
Figure 4. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs grouped by the age.
The median PFI was 189 days for dogs younger than 11 years-old (solid line, n = 19) and 51 days for dogs older than 11 years-old (dashed line, n = 22) (P = 0.048).
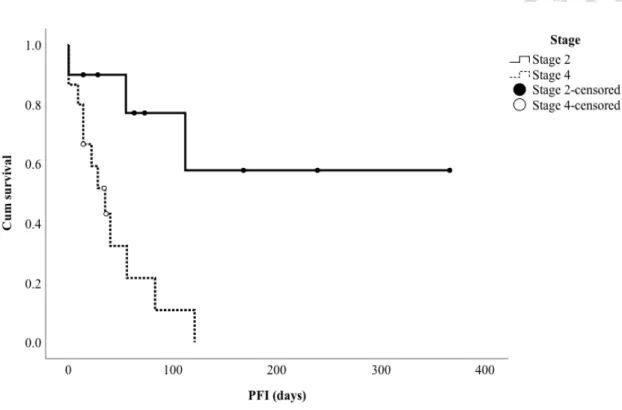
Figure 5. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs classified as stage 2 and stage 4.
The median PFI was not reached for dogs classified as stage 2 (solid line, n = 10) and 35 days for dogs classified as stage 4 (dashed line, n = 15) (P = 0.005).
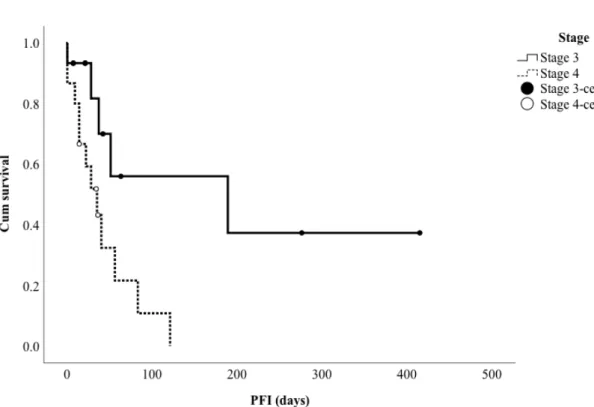
Figure 6. The Kaplan-Meier curve for the progression-free interval (PFI) for dogs classified as stage 3 and stage 4.
The median PFI was 189 days for dogs classified as stage 3 (solid line, n = 15) and 35 days for dogs classified as stage 4 (dashed line, n = 15) (P = 0.015).
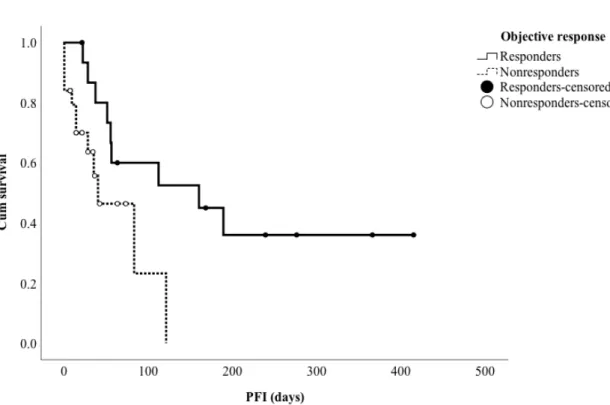
Figure 7. The Kaplan-Meier curve for the progression-free interval (PFI) for responders and non-responders.
The median PFI was 160 days for responders (solid line, n = 16) and 40 days for non- responders (dashed line, n = 25) (P = 0.025).
Tables
Table 1. World Health Organization clinical staging system for mast cell tumors Stage Description
0 One tumor incompletely excised from the dermis, identified histologically, without regional LN involvement
1 One tumor confined to the dermis without regional LN involvement 2 One tumor confined to the dermis, with regional LN involvement 3 Multiple dermal tumors; large, infiltrating tumors with or without
regional LN involvement
4 Any tumor with distant metastasis, including blood or bone marrow involvement
Substage
a Without systemic signs b With systemic signs
Note. Adapted from London et al., 2013. LN, lymph node.
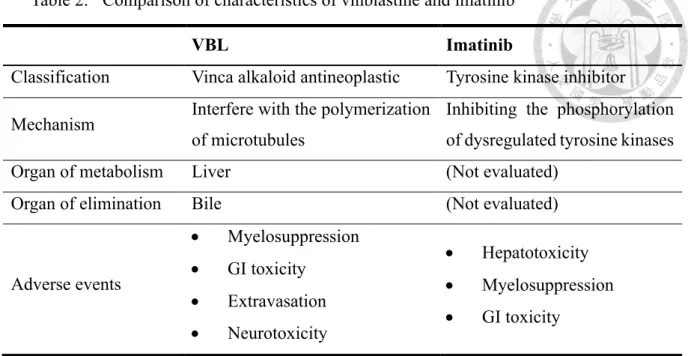
Table 2. Comparison of characteristics of vinblastine and imatinib
Note. VBL, vinblastine; GI, gastrointestinal.
VBL Imatinib
Classification Vinca alkaloid antineoplastic Tyrosine kinase inhibitor Mechanism Interfere with the polymerization
of microtubules
Inhibiting the phosphorylation of dysregulated tyrosine kinases
Organ of metabolism Liver (Not evaluated)
Organ of elimination Bile (Not evaluated)
Adverse events
• Myelosuppression
• GI toxicity
• Extravasation
• Neurotoxicity
• Hepatotoxicity
• Myelosuppression
• GI toxicity
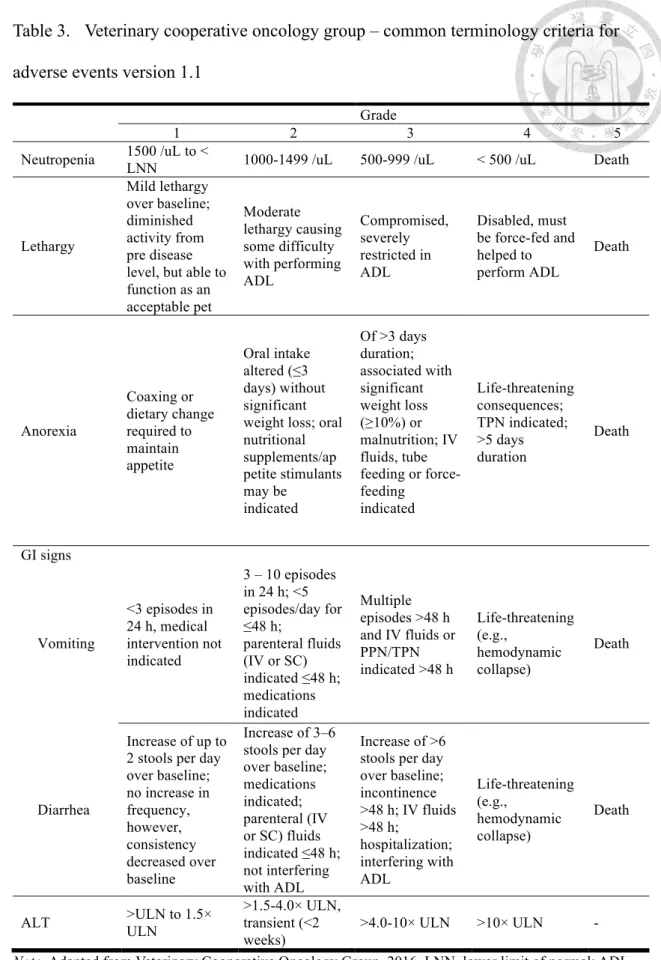
Table 3. Veterinary cooperative oncology group – common terminology criteria for adverse events version 1.1
Grade
1 2 3 4 5
Neutropenia 1500 /uL to <
LNN 1000-1499 /uL 500-999 /uL < 500 /uL Death
Lethargy
Mild lethargy over baseline;
diminished activity from pre disease level, but able to function as an acceptable pet
Moderate lethargy causing some difficulty with performing ADL
Compromised, severely restricted in ADL
Disabled, must be force-fed and helped to perform ADL
Death
Anorexia
Coaxing or dietary change required to maintain appetite
Oral intake altered (≤3 days) without significant weight loss; oral nutritional supplements/ap petite stimulants may be
indicated
Of >3 days duration;
associated with significant weight loss (≥10%) or malnutrition; IV fluids, tube feeding or force- feeding
indicated
Life-threatening consequences;
TPN indicated;
>5 days duration
Death
GI signs
Vomiting
<3 episodes in 24 h, medical intervention not indicated
3 – 10 episodes in 24 h; <5 episodes/day for
≤48 h;
parenteral fluids (IV or SC) indicated ≤48 h;
medications indicated
Multiple episodes >48 h and IV fluids or PPN/TPN indicated >48 h
Life-threatening (e.g.,
hemodynamic collapse)
Death
Diarrhea
Increase of up to 2 stools per day over baseline;
no increase in frequency, however, consistency decreased over baseline
Increase of 3–6 stools per day over baseline;
medications indicated;
parenteral (IV or SC) fluids indicated ≤48 h;
not interfering with ADL
Increase of >6 stools per day over baseline;
incontinence
>48 h; IV fluids
>48 h;
hospitalization;
interfering with ADL
Life-threatening (e.g.,
hemodynamic collapse)
Death
ALT >ULN to 1.5×
ULN
>1.5-4.0× ULN, transient (<2 weeks)
>4.0-10× ULN >10× ULN -
Note. Adapted from Veterinary Cooperative Oncology Group, 2016. LNN, lower limit of normal; ADL, activities of daily living (eating, sleeping, defecating and urinating); GI, gastrointestinal; IV, intravenous;
SC, subcutaneous; ALT, alanine transaminase; TPN, total parenteral nutrition; PPN, partial parenteral
Table 4. Comparison of patient characteristics between the two groups
Note. VBL, vinblastine.
VBL group (n = 21)
Imatinib group (n = 20)
P-value
Age (years) 0.609
Median (range) 11 (6-15) 10 (4-17)
Bodyweight (kg) 0.003
Median (range) 17.6 (4.9-36.8) 10.9 (2.6-34.5)
Breed 0.146
Pure breed 10 (47.6%) 14 (70.0%)
Mixed breed 11 (52.4%) 6 (30.0%)
Sex 0.437
Female 12 (57.1%) 9 (45.0%)
Male 9 (42.9%) 11 (55.0%)
Table 5. Comparison of tumor features and previous treatments between two groups VBL group
(n = 21)
Imatinib group (n = 20)
P-value
Stage 0.694
1 1 (4.8%) 0 (0.0%)
2 a 4 (19.0%) 6 (30.0%)
3 b 7 (33.3%) 8 (40.0%)
4 9 (42.9%) 6 (30.0%)
Substage 0.636
a 10 (47.6%) 11 (55.0%)
b 11 (52.4%) 9 (45.0%)
The diameter of target lesions (cm)
0.540 6.7 (1.0-24.8) 6.3 (1.0-24.5)
Location 0.810
Trunk 6 (28.6%) 5 (25.0%)
Limb 3 (14.3%) 2 (10.0%)
Head 0 (0.0%) 2 (10.0%)
Multiple cutaneous 10 (47.6%) 9 (45.0%)
LN only 2 (9.5%) 2 (10.0%)
Local recurrence 0.879
Yes 11 (52.4%) 10 (50.0%)
No 10 (47.6%) 10 (50.0%)
Previous systemic treatment 0.074
Yes 4 (19.0%) 9 (45.0%)
No 17 (81.0%) 11 (55.0%)
Previous steroid treatment 0.262
Yes 10 (47.6%) 13 (65.0%)
No 11 (52.4%) 7 (35.0%)
Note. VBL, vinblastine.
a. Abdominal ultrasound was not performed in 1 dog in VBL group and one dog in imatinib group b. Abdominal ultrasound was not performed in 2 dogs in VBL group and four dogs in imatinib group
Table 6. Response to treatment in two groups
Note. Responses were defined according to “Response Evaluation Criteria in Solid Tumors” by Eisenhauer et al., 2009. VBL, vinblastine.
a. The clinical benefit included complete remission, partial remission and stable disease.
VBL group (n = 21)
Imatinib group (n = 20)
P-value
Objective response rate 0.606
Complete remission 1 (4.8%) 3 (15.0%)
Partial remission 8 (38.1%) 4 (20.0%)
Stable disease 12 (57.1%) 9 (45.0%)
Progressive disease 0 (0.0%) 4 (20.0%)
Clinical benefit rate 0.048
Clinical benefit a 21 (100.0%) 16 (80.0%)
Progressive disease 0 (0.0%) 4 (20.0%)