doi:10.6342/NTU201602214
國立臺灣大學公衛學院職業醫學與工業衛生研究所 碩士論文
Institute of Occupational Medicine and Industrial Hygiene College of Public Health
National Taiwan University Master Thesis
mTOR抑制劑用於降低腎臟移植患者 的癌症發生率與死亡率之研究
The study of mammalian target of rapamycin (mTOR) inhibitors lower the incidence of malignancy and mortality rate in post-renal transplantation patient
林鈺琳 Yu-Ling Lin
指導教授 ﹕陳保中博士
Advisor : Pau-Chung Chen, MD, Ph.D.
中華民國105年6月 June 2016
doi:10.6342/NTU201602214 i
中文摘要
研究背景
先前的研究指出 mammalian target of rapamycin inhibitors (mTOR 抑制劑)用在腎 臟移植的患者身上,有抑制腫瘤的功效;然而 mTOR 抑制劑對全癌症發生率影 響的程度,以至於對特定癌症發生率影響的程度,到死亡率的影響,目前仍是 存在爭議,也因為 mTOR 抑制劑當中的 sirolimus 是 2000 年起開始上市使用,
因此跟以往使用的免疫抑制劑間的交互作用仍未有定論。因此本篇研究藉由全 民健保資料庫去分析,在腎臟移植患者身上,使用 mTOR 抑制劑與否以及使用 的劑量多寡,對於全癌症、特定癌症及死亡率發生的影響程度。
研究方法
我們使用 2000 年到 2008 年間的全民健保資料庫中的重大傷病檔,選用其中末 期腎臟病透析患者(ICD-9: 585)以及腎臟移植術後(ICD-9: V420)兩個族群進行 世代研究。首先在配對年紀、性別、收入和地域性後,比較兩組癌症的發生率,
接著選用一種常見的 mTOR 抑制劑藥物 sirolimus 當代表,並將腎臟移植術後的 世代分成有使用過 sirolimus 和從未使用過 sirolimus 兩組,分析全癌症發生率、
特定癌症發生率以及死亡率的影響,另外加入干擾因子進行敏感試驗分析,和 分析不同 sirolimus 累積劑量對死亡率的影響。所有的統計分析是使用 SAS 9.4 進行。
研究結果
在腎臟移植的世代中發現,比起規則透析的世代有著較高癌症發生率,這個結
果和之前的一些研究相似,但是本研究的結果在統計分析下是沒有顯著意義
(HR 1.16 [95% CI 0.96–1.41],推論可能是因為 2000 年以後開始廣泛使用 mTOR
抑制劑的因素。再將腎臟移植的世代進一步分成有無使用 sirolimus 的兩個族
doi:10.6342/NTU201602214 ii
群,發現使用 sirolimus 能降低全癌症、泌尿上皮細胞癌以及肝細胞癌的發生率,
且皆有統計上顯著意義;只有大腸直腸癌的發生率呈現沒有統計顯著的上升。
最後在死亡率部分,sirolimus 可能會降低死亡率,而且在累積劑量的分層分析 中顯示,隨著累積劑量愈大,愈能降低死亡率,但這些降低死亡率的結果均未 達統計上顯著意義。
結論
mTOR 抑制劑使用在腎臟移植後,能降低特定癌症的發生率,並可能改善腎臟 移植患者的存活率,跟累積劑量可能也有相關性,但受限於本次世代研究的規 模,有些結果並未能達統計學上的意義,因此仍需日後相關的研究協助探討。
關鍵字 : mTOR 抑制劑、癌症發生率、死亡率、腎臟移植、透析
doi:10.6342/NTU201602214 iii
Abstract
Background
Previous clinical studies suggested that mammalian target of rapamycin inhibitors (mTORi) had antineoplastic effects in renal transplantation cohort. However, overall cancer incidence and mortality rate in mTORi-exposed subjects post renal
transplantation are equivocal.
Objective
We aimed to assess the association between the use of mTOR inhibitor and the risk of developing specific cancer types and mortality rate in renal transplantation cohort.
RESEARCH DESIGN AND METHODS
We conducted two nationwide, population based, cohort studies using the Taiwan National Health Insurance Research Database. In the first cohort, enrollees were defined as patients who received dialysis between 2000 and 2008. We separated this cohort into receiving renal transplantation group and dialysis group, which were matched by sex, age, income and area. Among the 9,394 eligible enrollees, we used Cox regression to assess the risk of cancer between two groups. The second cohort, subjects were defined as patients who received renal transplantation between 2000 and 2008. We separated the cohort into sirolimus-exposed subjects and
sirolimus-unexposed subjects. We compared the overall cancer incidence, specific
doi:10.6342/NTU201602214 iv
cancer types incidence and mortality rate between sirolimus-exposed subjects and sirolimus-unexposed subjects.
RESULTS
An increased risk of cancer was observed in patient post renal transplantation
compared with those who in dialysis, although it was not significant (HR 1.16 [95%
CI 0.96–1.41]. A decreased risk of cancer was observed in sirolimus-exposed subjects rather than sirolimus-unexposed subjects in renal transplantation subjects (crude HR 0.21 [95% CI 0.13–0.34]; adjusted HR 0.25 [95% CI 0.15–0.41]).
Sirolimus-exposed subjects may decrease the incidence of urothelial cancer and hepatoma. Colorectal cancer showed an insignificant increased incidence in sirolimus-exposed subjects compared to sirolimus-unexposed subjects. We found lower mortality incidence in sirolimus-exposed subjects compared to
sirolimus-unexposed subjects, although this difference was not significant. As sirolimus dosage increased, mortality incidence trended down.
CONCLUSIONS
The use of mTOR inhibitor may be associated with a decreased risk of cancer and
mortality rate in patients post renal transplantation. Further studies are warranted to
confirm our findings.
doi:10.6342/NTU201602214 v
Key words: mTOR inhibitor, cancer incidence, mortality rate, renal transplantation,
dialysis
doi:10.6342/NTU201602214
目 錄
中文摘要……… i
英文摘要………iii
Chapter 1. Introduction………1
1.1 Background………1
1.2 Purpose………1
Chapter 2. Research design and methods………2
2.1 Study population………3
2.2 Exposure and outcome definitions………4
2.3 Statistical analyses………4
Chapter 3. Results……… 6
Chapter 4. Discussion………8
Chapter 5. Conclusions………13
References……… 14
doi:10.6342/NTU201602214
表目錄
Table 1. Characteristics in dialysis subjects and transplantation subjects…………17 Table 2. Overall cancer between dialysis subjects and transplantation subjects……18 Table 3. Characteristics in sirolimus-exposed subjects and sirolimus-unexposed
subjects………..19 Table 4. Specific cancer types incidence associated with sirolimus exposure……20 Table 5. Sensitivity test for adjusted HRs of cancer in potentially confounding drugs
……… 21
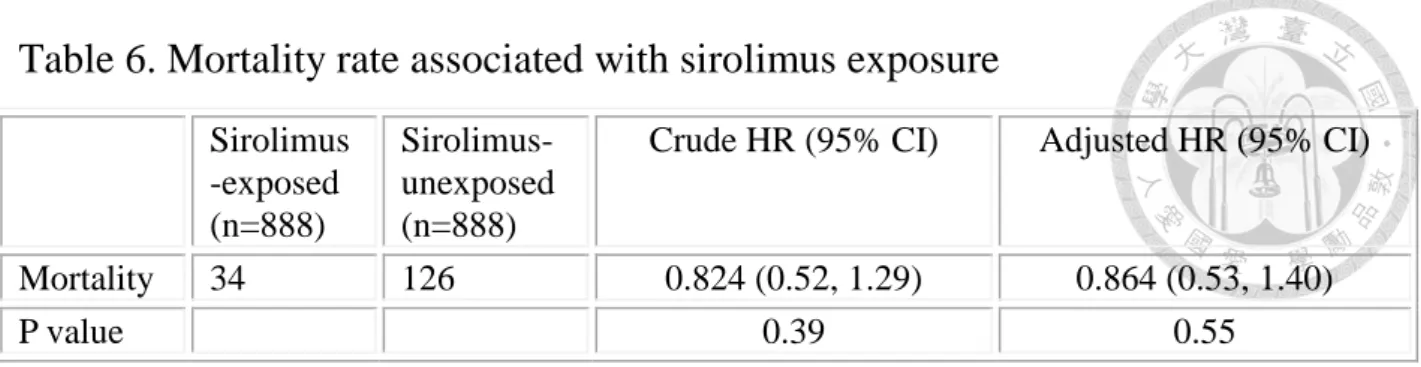
Table 6. Mortality rate associated with sirolimus exposure………22
Table 7. Mortality incidence associated with sirolimus cDDD………23
doi:10.6342/NTU201602214
圖目錄
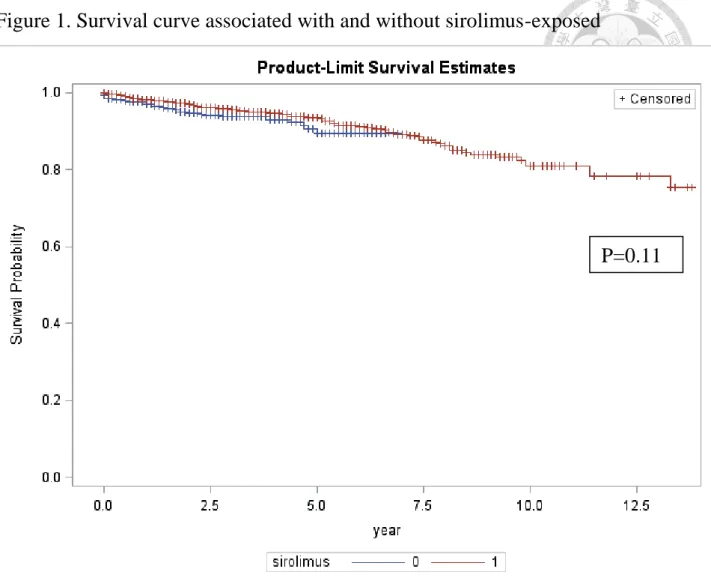
Figure 1. Survival curve associated with and without sirolimus-exposed………...24
doi:10.6342/NTU201602214
- 1 -
Chapter 1. Introduction
1.1 Background
Patient who receives dialysis for end stage kidney disease has higher cancer risk than the general population, especially urothelial carcinoma. Previous study revealed that the standardized incidence ratio for the dialysis period was significantly higher than that for the before renal replacement therapy period (1).After transplantation, the risk was markedly higher than in both preceding periods. It meant kidney transplant recipients have higher cancer risk than dialysis, even though end-stage kidney disease patients (1). It’s mainly due to immunosuppressive agent for preventing graft rejection. For example, one kind of calcineurin inhibitors, cyclosporin, lead to the loss of tumor immunosurveillance which was supported by an increased incidence of human
papillomavirus observed in transplant recipients with skin cancers as compared with skin cancers in patients not on immunosuppressive therapy (2). Similar situation of tumorigenesis was found in patients who was on tacrolimus therapy for immunosuppression (3). On the contrary, mammalian target of rapamycin (mTOR) inhibitor, a kind of immunosuppressive agent has anti-carcinogenic effect through several mechanisms (4). For instance, everolimus, an mTOR inhibitor, is currently approved for the treatment of hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative breast cancer through inhibition of the phosphoinositide 3 kinase (PI3K)/Akt/mammalian target of rapamycin (mTOR) pathway (5). mTOR inhibitor was used extensively from 2000, and it supplied another choice after renal transplantation and changed the balance of immunosuppressant using.
1.2 Purpose
Our study mainly discussed about the relationship between mTOR inhibitor and cancer incidence, and incidence of specific cancer types. Whether mTOR inhibitor could decrease the carcinogenic
doi:10.6342/NTU201602214
- 2 -
effect of CNI or not. Because the main outcome of mTOR inhibitor used after renal transplantation was cancer incidence out of survival rate in the great majority previous studies, we discussed the mortality rate as the secondary outcome in our study.
doi:10.6342/NTU201602214
- 3 -
Chapter 2. Research design and methods
2.1 Study population
We obtained the population for this study from the National Health Insurance Research Database (NHIRD) in Taiwan between 1 January 2000 and 31 December 2008. The National Health Insurance (NHI) program started in Taiwan in March 1995 . By the end of 2008, more than 99% of the entire Taiwanese population was enrolled in this program (6, 7). According to the Regulations Governing the Review of the Medical Services, the Bureau of National Health Insurance (BNHI) supplied for a review system that medical experts can inspect reimbursement claims filed by contracted medical institutions and screen the type, volume, quality, and appropriateness of medical services provided under the NHI program. The claims review system can identify the quality of NHI fee schedule, drug list, clinical guidelines, and patient situations. In accordance with the NHI Act, false diagnoses or inappropriate medical services will yield a severe penalty (7,8). The National Health Research Institute (NHRI) maintains and shields the privacy of all datum and claims data from the BNHI reimbursement data files. From the system, the NHIRD, NHRI has established a comprehensive computerized database (9). Specific data subsets in the NHIRD also applied for research purposes after ethical approval is obtained. In Taiwan, diagnoses of cancer must be confirmed by tissue pathology and are usually accurate. Catastrophic Illness Registry enrolled insured patients with eligible cancer who apply for a catastrophic illness certificate. The diagnosis of illness by physicians and a formal review by the BNHI provide the issuance of the certificate. Every enrollee of NHI was given a unique personal identification number in NHIRD. Researcher was able to link electronic data by identification number between different databases (9). With approval from the Ethics Review Board at the National Taiwan University College of Public Health, we conducted a
retrospective, nationwide, population-based, dialysis cohort study and renal transplantation cohort study among all enrollees in the NHI between 1 January 2000 and 31 December 2008. We excluded
doi:10.6342/NTU201602214
- 4 -
the subject whose age was younger than twenty years old, the diagnosis of cancer was less than one year after sirolimus using and mortality of subject was less than one year after sirolimus using.
2.2 Exposure and outcome definitions
The primary exposure of interest was the cancer incidence between dialysis subjects and renal transplantation subjects. Renal transplantation subjects were defined according to codes (V420) from the International Classification of Diseases (ICD-9). On the other hand, the subjects of dialysis which were matched by sex, urban, income, age (i.e., with the same birth calendar year), were defined base on codes (585) from ICD-9. The secondary outcome of interest was sirolimus user as compared to user of nonsirolimus-containing immunosuppressive agents in renal transplantation subjects. Incidence estimates and measures of association were calculated for cancers that occurred 12 months after the use of sirolimus or nonsirolimus-containing immunosuppressive agents.
Furthermore, the outcome of interest which was diagnosis of specific cancer types, such as
urothelial carcinoma, hepatoma and so on, due to high cancer incidence of urothelial carcinoma and hepatoma post renal transplantation in Taiwan according to previous study was analyzed in renal transplantation subjects. Finally, in renal transplantation subjected, mortality rate between sirolimus exposed user and sirolimus unexposed user was analyzed.
2.3 Statistical analyses
We used Cox regression to assess the risk of cancer incidence between dialysis subjects and renal transplantation subjects. The hazard ratios (HRs) and 95% CIs for cancer incidence were calculated and estimated as unadjusted and adjusted for covariates (including sex, age, urbanization, income, diabetes, hypertension, cardiovascular event, coronary artery disease, cardiomyopathy, heart failure,
doi:10.6342/NTU201602214
- 5 -
arrhythmia, dyslipidemia, anemia, brain infarction and brain hemorrhage). We assessed the dose- or duration-response effects according to the category of exposure and test by significant assessment of the b coefficients (i.e., P value) of exposure, which was regarded as a continuous variable.
Sensitivity analyses based on the therapy of sirolimus were conducted to assess whether the effect of sirolimus would be altered by adding potentially confounding drugs, including steroid and other immunosuppressive agents. All analyses were conducted using the SAS version 9.4 software package (SAS Institute, Cary, NC).
doi:10.6342/NTU201602214
- 6 -
Chapter 3. Results
We identified 4,697 dialysis subjects and 4,697 renal transplantation subjects by matching with sex and age between 1 January 2000 and 31 December 2008. Table 1 summarized the demographic and clinical characteristics of the study population. The median age was 48.3 years at dialysis group and 45.3 years at renal transplantation group. Regarding the potential confounders, the dialysis subjects were more likely to have diabetes, coronary artery disease, CV event, stroke, intracranial
hemorrhage and congestive heart failure than renal transplantation subjects. Table 2 showed an increased risk of cancer in renal transplantation subjects compared with dialysis subjects, although this difference was insignificant (HR 1.16 [95% CI 0.96–1.41]).
We summarized the demographic and clinical characteristics of sirolimus-exposed subjects and sirolimus-unexposed subjects in renal transplantation subjects (Table 3). In these subjects, we noted significant lower incidence of all cancer in sirolimus-exposed subjects than non-sirolimus-exposed subjects (crude HR 0.21 [95% CI 0.13–0.34]; adjusted HR 0.25 [95% CI 0.15–0.41]). Similar results were observed in urothelial cancer subjects (crude HR 0.25 [95% CI 0.13–0.48]; adjusted HR 0.33 [95% CI 0.16–0.65]) and HCC subjects (crude HR 0.15 [95% CI 0.03–0.70]; adjusted HR 0.19 [95% CI 0.04–0.88]). Except colorectal cancer showed an insignificant increased incidence in sirolimus-exposed subjects compared with non-sirolimus-exposed subjects (crude HR 1.87 [95% CI 0.16–21.1), the other cancers revealed insignificant decreased incidence in sirolimus-exposed subjects compared with non-sirolimus-exposed subjects, such as breast cancer (crude HR 0.23 [95%
CI 0.02–2.13]; adjusted HR 0.48 [95% CI 0.04–05.18) and lymphoma (crude HR 0.95 [95% CI 0.06–15.4]; adjusted HR 0.84 [95% CI 0.03–23.3]) (Table 4). In sensitivity tests, the significance of the decreased risks of all cancer in sirolimus-exposed subject was not altered by adding potentially confounding immunosuppressive agents (Table 5).
doi:10.6342/NTU201602214
- 7 -
In renal transplantation subjects, we found lower mortality incidence in sirolimus-exposed subjects compared to sirolimus-unexposed subjects, although this difference was not significant (crude HR:
0.82, [95% CI 0.52–1.29]; adjusted HR 0.86 [95% CI 0.53–1.40]) (Table 6). Similar result was noted in survival curve between sirolimus-exposed subjects and sirolimus-unexposed subjects (p=0.11) (Figure 1). The dose- or duration-response relationships between the use of sirolimus and a decreased mortality were observed based on the cumulative dose of the sirolimus (Table 7). As sirolimus dosage increased, the mortality rate decreased gradually, although this difference was not significant.
doi:10.6342/NTU201602214
- 8 -
Chapter 4. Discussion
In this cohort of 1776 renal transplants, sirolimus user was associated with a decreased cancer incidence. Cancer incidence appeared lower for a number of specific cancer types, though these associations were not absolute statistically significant except hepatoma and urothelial cancer. Even though we adjusted confounding factors, the trend of lowering incidence of hepatoma and urothelial cancer still existed. The reduced cancer incidence in our study might both result from the
antineoplastic effect of sirolimus and the result of reducing CNIs. Furthermore, not only the benefit of decreased cancer incidence, but the trend of decreased mortality incidence in sirolimus user in our study. We also observed the dose-response effect between sirolimus dosage and survival rate which was never mentioned in previous studies.
Renal transplantation was associated with a marked increase in cancer risk at a wide variety of sites, and this phenomenon was mainly due to immunosuppressive agent (10). Nevertheless, an increased cancer incidence turned into insignificant with the use of mTOR inhibitors in a recent decade according to our results (Table 2). We supposed the possible reason may be due to mTOR inhibitors which had antineoplastic effect was used extensively from 2000. Our results of this large
population-based study indicated that the use of sirolimus may be associated with decreased risks of cancer and mortality in patients post renal transplantation. The majority of the published preclinical studies have suggested that mTOR inhibitors have antineoplastic effects (11). The possible
mechanism by which mTOR inhibitors cause cell differentiation and induce cancer cell apoptosis has been demonstrated in prior studies (12,13). Besides, in vivo study, it showed that VEGF, CXCR3 and CXCR3-binding ligands (CXCL10 and CXCL11) are overexpressed in
post-transplantation renal cancer tissues following CNI (CsA) treatment and mTOR inhibitors could inhibite CNI-induced over-expression of the angiogenic cytokine VEGF, and the chemokine
doi:10.6342/NTU201602214
- 9 -
receptor CXCR3 and its ligands in post-transplantation tumor tissues (13). Our results are consistent with prior in vitro studies and provide clinical evidence for a decreased risk of cancer that is
associated with the use of mTOR inhibitors in patients post renal transplantation.
Previous studies have been conducted to investigate the association between the use of mTOR inhibitors and the risk of developing cancer, but only few clinical studies focused on the relationship between mTOR inhibitors and specific cancer types (11). Yanik et al. (14) conducted a retrospective analysis in a population from SRTR in the U.S. to assess the influence of sirolimus on the risk of specific cancer types. A reduction of risk for specific cancer types in patients treated with sirolimus was observed except prostate cancer (unadjusted HR 1.70 [95% CI 1.05–2.74], adjusted HR 1.86 [95% CI 1.15–3.02]). However, the reduction of risk for each cancer type did not attain statistical significance. Most previous studies mentioned about nonmelanoma skin cancers, because these are a common malignant complication following a kidney transplant in western countries, not in Asia countries (15). But we observed different significance of specific cancer types compared to the results of SRTR. Our results revealed the reduction of risks of urothelial cancer and hepatoma were significant, and these results had been proved in previous studies (16) (17). Incidence of colorectal cancer incidence increased insignificantly. Similar result was mentioned in previous study in 2005, which showed one de novo colorectal cancer in eleven patients with solid tumors in the
sirolimus/everolimus alone group (18). However, in vitro study showed that mTOR is commonly activated in colon cancer. mTOR complex 1 (mTORC1) is a major downstream target of the
PI3K/ATK pathway and activates protein synthesis by phosphorylating key regulators of messenger RNA translation and ribosome synthesis. Rapamycin analogs are non-ATP-competitive mTORC1 inhibitors, and suppress proliferation and tumor angiogenesis and invasion (19). It needed further study to identify the difference between in vivo and in vitro.
doi:10.6342/NTU201602214
- 10 -
Calcineurin inhibitors were widely recommended for the primary prevention of graft rejection in patients post renal transplantation, and it has been proved to increase cancer incidence (20). The regimen consisting of cyclosporine, azathioprine with prednisolone could be distinguished by the highest risk of malignancy occurrence (5.2%) (20). Therefore, increased cancer incidence post renal transplantation is considered as calcineurin inhibitors neoplastic effect. Comparison sirolimus users alone with other immunosuppressive agent users was difficult to practice in our study, because the sample size was too small and there were only 21 subjects in sirolimus alone group. According to our analysis, sirolimus supplied anti-neoplastic effect to renal transplantation subjects whether calcineurin inhibitors exposure or not. In addition, sirolimus might neutralize neoplastic effect of calcineurin inhibitors. As concern about steroid, azathioprine and mycophenolate might be major confounders in our study, we conducted an additional sensitivity analysis to investigate the effect of concomitant use of sirolimus and steroid, azathioprine or mycophenolate. In our additional
sensitivity analysis, the use of sirolimus showed a significant decrease in the risk of cancer within the groups that concomitantly used steroid, azathioprine or mycophenolate (p=0.01).
A potential bias that may result from confounding indications is the association between end-stage kidney disease and cancer risk. End-stage kidney disease and cancer have many mutual risk factors, and end-stage kidney disease is suggested to be associated with an increased risk of certain cancers.
A recent study also indicated that the longer dialysis duration was related to the risk of cancer and certain other cancer-related causes of death (21). The potential causality or association between end-stage kidney disease and cancer has not been clearly established, and it remains unclear whether the association between these two diseases is direct or indirect, and whether the cancer risk would be influenced by the dialysis induced anuria. There are limitations of our database in that the
doi:10.6342/NTU201602214
- 11 -
NHIRD did not include detailed results from laboratory tests; thus, we were unable to provide exact measurements of uremic toxin level or urine amount status.
Except cancer incidence, we also focused on mortality rate between sirolimus-exposed subjects and sirolimus-unexposed subjects. We searched the PubMed database for articles published up to April 2016 and identified four original clinical studies focusing on the assessment of survival rate in patients exposed to sirolimus. Most results of previous clinical studies appeared to be neutral in regard to survival rate. After renal transplantation, few studies showed good survival rate in sirolimus-unexposed subjects (22). On the contrary, some studies supported that an increased survival rate came with an increased dosage of sirolimus (23). In our study, sirolimus-exposed subjects had insignificant lower mortality rate compared to sirolimus-unexposed subjects (p=0.39).
The survival curve of sirolimus-exposed subjects seemed to be better than the curve of
sirolimus-unexposed subjects (p=0.11). Base on the result, we analyzed the relationship between sirolimus cumulative defined daily dose and mortality rate further. It seemed to be a trend that as the sirolimus cddd increased, the mortality rate decreased, although the result was insignificant. This finding had never been mentioned in previous clinical studies. It was a future work that whether there was a threshold of effective sirolimus cddd in survival rate prolongation or not, but the dose-response effect between sirolimus and survival rate gave us a guild to follow it.
We also had incomplete data on several variables known to be associated with cancer, such as unhealthy life habit, obesity, a family history of cancer, recurrent or de novo cancer, smoking or alcohol consumption. Furthermore, a detection bias could occur in our study in those patients receiving renal transplantation might have access to a better economic status and an increased opportunity to receive cancer screening, which would result in higher cancer detection rates and
doi:10.6342/NTU201602214
- 12 -
would also decrease subsequent cancer rates. Some confounders about mortality, such as accident, could not be corrected in our database, which might relate to detection bias.
doi:10.6342/NTU201602214
- 13 -
Chapter 5. Conclusions
This study provided clinical evidence that mTOR inhibitors had an antineoplastic effect on cancer among patients post renal transplantation. An increased survival rate in mTOR inhibitor users may make a benefit out of cancer incidence. Even though mTOR inhibitors have these advantages, they are unable to replace with calcineurin inhibitors completely nowadays. The complexity of the links between renal transplantation, cancer, and mTOR inhibitors warrants clarification through further studies.
doi:10.6342/NTU201602214
- 14 -
References
1. CM Vajdic, SP McDonald, MR McCredie, et al. Cancer incidence before and after kidney transplantation. JAMA 2006; 296: 2823–2831.
2. Harwood CA, Surentheran T, McGregor JM, et al. Human papillomavirus infection and
non-melanoma skin cancer in immunosuppressed and immunocompetent individuals. J Med Virol 2000;61:289–297.
3. Kauffman HM, Cherikh WS, McBride MA, Cheng Y, Hanto DW. Post-transplant de novo malignancies in renal transplant recipients: the past and present. Transpl Int 2006;19:607–20.
4. Douros J, Suffness M. New antitumor substances of natural origin. Cancer Treat Rev 1981; 8:
63–87.
5. Lee JJ, Loh K, Yap YS. PI3K/Akt/mTOR inhibitors in breast cancer. Cancer Biol Med. 2015 Dec;12(4):342-54.
6. Chiang TL. Taiwan’s 1995 health care reform. Health Policy 1997;39:225–239
7. Bureau of National Health Insurance. Available from http://www.nhi.gov.tw/
Resource/webdata/Attach_13767_1_National% 20Health%20Insurance%20in%
20Taiwan%202010.pdf. Accessed 20 October 2011
8. Lu JF, Hsiao WC. Does universal health insurance make health care unaffordable? Lessons from Taiwan. Health Aff (Millwood) 2003;22:77–88
9. InstitutesNHR.NationalHealth Insurance Research Database. Available from http://
w3.nhri.org.tw/nhird/en/index.htm. Accessed 20 October 2011
10. Vajdic CM, McDonald SP, McCredie MR, et al. Cancer incidence before and after kidney transplantation. JAMA. 2006 Dec 20; 296(23): 2823-31.
doi:10.6342/NTU201602214
- 15 -
11. Yanik EL, Siddiqui K, Engels EA. Sirolimus effects on cancer incidence after kidney transplantation: a meta-analysis. Cancer Med. 2015 Sep;4(9):1448-59.
12. Manuelli M, De Luca L, Iaria G, et al. Conversion to rapamycin immunosuppression for malignancy after kidney transplantation. Transplant Proc. 2010 May; 42(4): 1314-6.
13. Basu A, Liu T, Banerjee P, et al. Effectiveness of a combination therapy using calcineurin inhibitor and mTOR inhibitor in preventing allograft rejection and post-transplantation renal cancer progression. Cancer Lett. 2012 Aug 28; 321(2): 179-86.
14. Yanik EL, Gustafson SK, Kasiske BL, et al. Sirolimus use and cancer incidence among US kidney transplant recipients. Am J Transplant. 2015 Jan;15(1):129-36.
15. Gu Y-H, Du J-X, Ma M-L. Sirolimus and, non-melanoma skin cancer prevention after kidney transplantation: A meta-analysis. Asian Pac J Cancer Prev 2012; 13: 4335–39.
16. Pinto-Leite R, Arantes-Rodrigues R, Palmeira C, et al. Everolimus combined with cisplatin has a potential role in treatment of urothelial bladder cancer. Biomed Pharmacother. 2013
Mar;67(2):116-21.
17. Ashworth RE, Wu J. Mammalian target of rapamycin inhibition in hepatocellular carcinoma.
World J Hepatol. 2014 Nov 27;6(11):776-82.
18. Kauffman HM, Cherikh WS, Cheng Y, Hanto DW, Kahan BD. Maintenance
immunosuppression with target-of-rapamycin inhibitors is associated with a reduced incidence of de novo malignancies. Transplantation. 2005 Oct 15;80(7):883-9.
19. He K, Zheng X, Li M, Zhang L, Yu J. mTOR inhibitors induce apoptosis in colon cancer cells via CHOP-dependent DR5 induction on 4E-BP1 dephosphorylation. Oncogene. 2016 Jan 14;35(2):148-57.
doi:10.6342/NTU201602214
- 16 -
20. Watorek E, Boratynska M, Smolska D, et al. Malignancy after renal transplantation in the new era of immunosuppression. Ann Transplant. 2011 Apr-Jun; 16(2):14-8.
21.Ikezawa E, Kondo T, Hashimoto Y, et al. Clinical symptoms predict poor overall survival in chronic-dialysis patients with renal cell carcinoma associated with end-stage renal disease. Jpn J Clin Oncol. 2014 Nov;44 (11):1096-100.
22. Tellis V, Schechner R, Mallis M, et al. No-load sirolimus with tacrolimus and steroids is safe and effective in renal transplantation. Transplant Proc 2005; 37:906-8.
23. Lo A, Egidi MF, Gaber LW, et al. Observations regarding the use of sirolimus and tacrolimus in high-risk cadaveric renal transplantation. Clin Transplant 2004; 18: 53-61.
doi:10.6342/NTU201602214
- 17 -
Table 1. Characteristics in dialysis subjects and transplantation subjects
Dialysis Transplantation
N 4697 4697
Sex
female 2212 (47.1) 2212 (47.1)
male 2485 (52.9) 2485 (52.9)
Age, years
≦ 40 1600 (34.1) 1600 (34.1)
41-50 957 (20.4) 1492 (31.7)
51-60 1298 (27.6) 1178 (25.1)
61-70 751 (16.0) 385 (8.2)
> 70 91 (1.9) 42 (0.9)
Mean (SD) 47.3 ± 12.6 44.8 ± 11.2
Median (IQR) 48.3 45.3
Dialysis duration Covariates
Hypertension 3457 (73.6) 3592 (76.5)
Hyperlipidemia 1831 (39.0) 1817 (38.6)
Diabetes 2101 (44.7) 1328 (28.3)
CAD 1694 (36.1) 978 (20.8)
CV event 1730 (36.8) 1001 (21.3)
Cardiomyopathy 172 (3.7) 97 (2.07)
Stroke 701 (14.9) 302 (6.4)
ICH 949 (20.2) 436 (9.3)
Anemia 2689 (57.3) 2642 (56.3)
Arrhythmia 708 (15.1) 537 (11.4)
CHF 1308 (27.9) 618 (13.2)
doi:10.6342/NTU201602214
- 18 -
Table 2. All cancer between dialysis subjects and transplantation subjects
Dialysis (n=4697) Transplantation (n=4697) HR (95% CI) P-value
All cancer 143 241 1.16 (0.96, 1.41) 0.11
doi:10.6342/NTU201602214
- 19 -
Table 3. Characteristics in sirolimus-exposed subjects and sirolimus-unexposed subjects
Sirolimus-exposed Sirolimus-unexposed
N 888 888
Sex
female 446 (50.2) 446 (50.2)
male 452 (49.8) 452 (49.8)
Age, years
≦ 40 366 (41.2) 366 (41.2)
41-50 281 (31.6) 253 (28.5)
51-60 185 (20.8) 216 (24.3)
61-70 53 (6.0) 47 (5.3)
> 70 3 (0.4) 6 (0.7)
Mean (SD) 43.4 ± 11.0 43.9 ± 11.0
Median (IQR) 43.9 44.8
Dialysis duration Covariates
Hypertension 733 (82.6) 659 (74.1)
Hyperlipidemia 371 (42.2) 365 (41.1)
Diabetes 276 (31.1) 245 (27.6)
CAD 207 (23.3) 187 (21.1)
CV event 211 (23.8) 192 (21.6)
Cardiomyopathy 24 (2.7) 25 (2.9)
Stroke 56 (6.3) 64 (7.2)
ICH 84 (9.5) 86 (9.7)
Anemia 583 (65.7) 485 (54.6)
Arrhythmia 90 (10.1) 89 (10.0)
CHF 144 (16.2) 107 (12.0)
doi:10.6342/NTU201602214
- 20 -
Table 4. Specific cancer types incidence associated with sirolimus exposure
Cancer Sirolimus -exposed (n=888)
Sirolimus- unexposed
(n=888)
Crude HR (95% CI) Adjusted HR (95% CI)
All cancer 21 120 0.21 (0.13, 0.34) 0.25 (0.15, 0.41)
Urothelial cancer
11 48 0.25 (0.13, 0.48) 0.33 (0.16, 0.65)
HCC 2 25 0.15 (0.03, 0.70) 0.19 (0.04, 0.88)
Colorectal cancer
2 3 1.87 (0.16, 21.12) 0.94 (0.05, 17.09)
Lung cancer 1 1 0.94 (0.05, 15.21) -
Prostate cancer
0 4 - -
Breast cancer
1 5 0.23 (0.02, 2.13) 0.48 (0.04, 5.18)
Lymphoma 1 1 0.95 (0.06, 15.41) 0.84 (0.03, 23.30)
Sirolimus-exposed subjects and unexposed subjects were under 1:1 match by sex,
age, income and urbanization. Adjusted for sex, age, income, urbanization, diabetes,
hypertension, cardiovascular event, coronary artery disease, cardiomyopathy, heart
failure, arrhythmia, dyslipidemia, anemia, brain infarction and brain hemorrhage.
doi:10.6342/NTU201602214
- 21 -
Table 5. Sensitivity test for adjusted HRs of cancer in potentially confounding drugs
Confounding drug HR (95% CI) P value
Main model 0.163 (0.040, 0.658) 0.01
Main model + steroid 0.134 (0.028, 0.648) 0.01 Main model + Mycophenolate 0.163 (0.040, 0.658) 0.01 Main model + Azathioprine 0.163 (0.040, 0.658) 0.01
Main model, adjusted for sex, age, income, urbanization, diabetes, hypertension,
cardiovascular event, coronary artery disease, cardiomyopathy, heart failure,
arrhythmia, dyslipidemia, anemia, brain infarction and brain hemorrhage.
doi:10.6342/NTU201602214
- 22 -
Table 6. Mortality rate associated with sirolimus exposure
Sirolimus -exposed (n=888)
Sirolimus- unexposed (n=888)
Crude HR (95% CI) Adjusted HR (95% CI)
Mortality 34 126 0.824 (0.52, 1.29) 0.864 (0.53, 1.40)
P value 0.39 0.55
Adjusted for sex, age, income and urbanization
doi:10.6342/NTU201602214
- 23 -
Table 7. Mortality incidence associated with sirolimus cDDD
Crude OR (95% CI) Adjusted 0R (95% CI)
<24 1.00 (reference) 1.00 (reference)
24-52 0.85 (0.34, 2.13) 0.84 (0.29, 2.37)
>52 0.69 (0.31, 1.51) 0.85 (0.35, 2.01)
Adjusted for sex, age, income and urbanization
doi:10.6342/NTU201602214
- 24 -