行政院國家科學委員會專題研究計畫 成果報告
探討果寡醣、異麥芽寡醣對慣性便秘安養中心居民之大腸 菌相、血液抗氧化狀態及大腸癌前危險指標之影響(第 3
年)
研究成果報告(完整版)
計 畫 類 別 : 個別型
計 畫 編 號 : NSC 96-2320-B-040-031-MY3
執 行 期 間 : 98 年 08 月 01 日至 99 年 07 月 31 日 執 行 單 位 : 中山醫學大學營養學系(所)
計 畫 主 持 人 : 陳曉鈴
計畫參與人員: 博士後研究:顏啟華
報 告 附 件 : 出席國際會議研究心得報告及發表論文
處 理 方 式 : 本計畫涉及專利或其他智慧財產權,2 年後可公開查詢
中 華 民 國 99 年 09 月 21 日
行政院國家科學委員會補助專題研究計畫
成果報告□期中進報告
探討果寡醣、異麥芽寡醣對慣性便秘安養中心居民之大腸菌相、
血液抗氧化狀態及大腸癌前危險指標之影響
計畫類別:個別型計畫 □整合型計畫 計畫編號:NSC 96-2320-B-040-031-MY3
執行期間: 96 年 08 月 01 日至 99 年 07 月 31 日 執行機構及系所:中山醫學大學
計畫主持人:陳曉鈴
計畫參與人員:顏啟華 郭怡文 曾韻樺 尤宣文 李孟智
成果報告類型(依經費核定清單規定繳交):□精簡報告 完整報告
本計畫除繳交成果報告外,另須繳交以下出國心得報告:
□赴國外出差或研習心得報告
□赴大陸地區出差或研習心得報告
出席國際學術會議心得報告 (已經上網繳交)
□國際合作研究計畫國外研究報告
處理方式:除列管計畫及下列情形者外,得立即公開查詢
涉及專利或其他智慧財產權,□一年□二年後可公開查詢
中 華 民 國 99 年 9 月 19 日
目錄
第一年成果 p. 2-13
第二年成果 p. 14-26
第三年成果 p. 27-32
成果報告自評表 p. 33
YEAR OF 2007
中文摘要
本研究探討果寡醣生技寡醣對安養中心低活動力老人腸道生理、菌相的調節作用,
以及血液過氧化狀態的影響。本研究於台中市安養中心進行,以固定飲食型態下分為安 慰劑期、補充期及恢復期。研究成果已被接受刊登(Nutrition)並且已先行於網路上刊登,
敬附論文於下。
關鍵詞: 果寡醣、老人、糞便細菌酵素、氧化壓力、短鏈脂肪酸、腸道功能 The Beneficial Effects of Fructo-oligosaccharides Supplementation on Fecal Bifidobacteria and Index of Peroxidation Status in Constipated Nursing-Home
Residents—A Placebo-controlled, Diet-controlled Trial 將刊登於 Nutrition 2010 (in press)
Abstract
Objective: This study assesses effects of fructo-oligosaccharides (FOS) supplementation on fecal bifidobacteria, lipid peroxidation index and indices of nutritional status, and whether effects of FOS sustained after its withdrawal, in constipated nursing-home residents. The associations of fecal bifidobacteria and blood measurements were also examined.
Methods: Six men and four women participated in a double-blind, diet-controlled study that consisted of a 4-wk placebo (3 mL fructose syrup) period, a 4-wk FOS (10 g/d) period and a 4-wk post period. Stools were collected during the last week of each period to determine the microflora and fecal weight. Fasting blood was collected at the end of each period and analyzed for thiobarbituric acid-reactive substances (TBARS) and biochemical indices.
Results: Fecal counts (Log counts/g dry feces) and daily fecal output of bifidobacteria significantly increased with FOS as compared to the placebo. The effect on bifidobacteria output lasted through the post period. Plasma TBARS concentration was reduced by 16%
and 21% in the FOS and the post period, respectively, as compared to that in the placebo period. The plasma cholesterol level was significantly reduced by approximately 7% in both the FOS and post period, respectively, as compared to that in the placebo period.
The increases in fecal bifidobacteria output during the FOS period (Log CFU/d) was associated with decreases in plasma TBARS and plasma cholesterol, respectively.
Conclusion: Supplementation of FOS increases the daily output of bifidobacteria, and decreases plasma TBARS and cholesterol concentrations in constipated nursing-home elderly residents and these effects remained at the end the post period.
Keywords: fructo-oligosaccharides, thiobarbituric acid-reactive substances (TBARS), constipation, elderly, cholesterol
Introduction
The elderly population has high incidences of impaired oral function and bowel function, and chronic diseases.[1,2] It has been reported that the elderly people with poor oral function tend to select fewer dietary fiber sources, fruits and vegetables, which aggravate their gastrointestinal conditions.[3] A soluble dietary fiber supplement that could be easily incorporated into their ordinary diet may improve the bowel function or age-related syndromes.
Fructo-oligosaccharides (FOS) has been commonly applied to functional food as it could modulate the bowel function. Two studies have indicated that daily administration of 10-15 g of FOS to healthy young adults significantly improves defecation frequency and feeling of incomplete defecation.[4,5] FOS is poorly digested in the human small intestine, but is fermented by the resident microflora in the human colon.[4] Its bifidogenic effects in healthy adults have been extensively demonstrated in well-controlled human trials.[4,6,7] Aging has been associated with decreased fecal bifidobacteria concentrations, which may partially cause dysfunction of the intestine, decreased immunity, and greater susceptibility to disease.[8]
Unfortunately, there is a lack of study that demonstrates the role for FOS in elderly subjects, especially in constipated, long-term care residents.
Free radical attack has been associated with neurodegenerative and cardiovascular diseases and cancer, all of which become more frequent with age.[9] Recent studies have found bifidogenic dietary fiber to have antioxidative effects [10-11]. An in vitro study demonstrates that fermentation of FOS by bifidobacteria exerts excellent eliminating effects on free radicals.[10] A clinical study also have suggested that consumption of prebiotics beneficially reduces blood oxidative status and elevates plasma antioxidant, such as
-tocopherol and uric acid, levels in men.[11] The possibility that FOS supplement may reduce the plasma pro-oxidative status in the elderly, as does a possible antioxidant mechanism for FOS, remains unexplored.
The main goal of this study was to assess effects of FOS supplementation on colonic microflora and lipid peroxidation status, and the association of these two measurements, in constipated nursing-home residents. A secondary objective was to determine if effects of FOS sustained after its withdrawal. The fecal characteristics, bowel functions, and selective plasma indices of nutritional status also were examined.
Materials and methods Subjects
We recruited volunteers from a local nursing home. The volunteers who were on medication for treating constipation or otherwise had spontaneous bowel movements less than three times per week or had straining with passage of bowel movement under no medication were defined as constipated. The criteria for recruitment were stable physiological condition, long-term residence (> 6-months), chronic constipation (> 6-months), ability to chew soft or blended diet, not bed-ridden, and no tobacco or antibiotic use. In addition, subjects agreed to comply with the cycled menus, and specimen (blood and fecal) collections.
All subjects were free of clinically wasting or terminal illness. Ten subjects (six males) aged 74.0 3.3 participated in the study. Seven subjects were treated for constipation with MgO, Dulcolax, Sennapur, or combination of either two. All medical regimens and fluid intake were kept constant throughout the study. The activity of daily life (ADL) was moderate as graded 73.8 3.3 point using Barthel index. [12] Most subjects were on regular and soft
diet; three were on blended diet.
Experimental design
This double-blind, placebo-controlled, diet-controlled study consisted of a 4-wk placebo (3 mL fructose syrup) period, a 4-wk FOS period, and a 4-wk post period. The study did not employ a crossover or randomized design because subjects could not tolerate long-term diet control. FOS was consumed as a drink and its dose was gradually increased from 5 g/d (first 7 d) to 10 g/d (d 8-28) to avoid potential intestinal distension. Neither sweetener was consumed during the post period. Spontaneous defecation and enema usage were recorded by the nurse. All stools voided during the last week of each period were individually collected in plastic bags to determine the fecal weight and microflora counts. Body weight was determined and fasting blood samples were collected on the last day of each period. The experimental protocol was approved by the ethics committee of Chung Shan Medical University Hospital; all volunteers provided written informed consent.
Diet and dietary intake assessment
Subjects consumed a 7-d cycled menu (Table 1) from one month before the study until the end of post period in order to exclude the possibility that dietary variation might confound the effects of FOS. The amount of food provided to individual subject in the experimental periods was based on the 3-d dietary assessment in the pre-experimental period. In order to assess the average intakes of energy, nutrients and dietary fiber, meals served to and left over by the subjects were weighed and recorded for three non-consecutive days during each period.
Fluid intake was calculated from the fluid intake record and the water content of food. The nutrient contents of all food ingested by the subjects were determined using local nutrient composition tables. [13]
Supplements of antioxidants, oligosaccharides- or lactic acid bacteria-containing foods, were not allowed during the study. The composition (%) of FOS (Institute of Microbial Resources, Taichung, Taiwan) was fructosylnystose, 0.65; nystose (-D-Fruf-(21)- - D-Fruf-(21)- -D-Fruf-(21)--D-Glup), 10.51; 1-kestose (-D-Fruf-(21)-- D-Fruf-(21)--D-Glup), 28.41; sucrose, 14.26; glucose, 20.34; fructose, 2.83 and moisture, 23.0. The composition of fructose syrup (Pay Inc., Taipei, Taiwan) was fructose, 55; glucose, 20; and moisture, 25. The FOS supplement and fructose therefore provided similar amount of carbohydrates to the volunteers. FOS and fructose were administered to subjects in water as an afternoon snack.
Fecal collection
Nine of ten subjects completed the 7-d fecal collection for all three periods. The one who did not complete fecal collection in the post period was not included for statistical analysis. All feces voided were collected in plastic bag, vacuumed and sealed, and then stored in ice buckets and immediately sent to our laboratory. Feces were then homogenized in a stomacher. All lyophilized feces excreted by an individual were weighed and pooled together as a fecal composite for further analysis of fecal microflora.
Quantitation of fecal bifidobacteria, clostridia and total bacteria
Fecal bacteria were assessed using fluorescence in situ hybridization method (FISH).[14]
The probes used were Bif164 [14] and Ib1 [15] specific for bifidobacteria and clostridia,
respectively, while the nucleic acid stain 4’, 6-diamidino-2-phenylindole (DAPI) was used for total bacterial counts.[14] Fecal microbial counts are expressed as log10 counts/g dry feces.
The daily microbial output was calculated by fecal count (count/g dry feces) daily dry fecal weight (g/d) and expressed as log10 counts/d.
Blood preparation, and measurements of plasma biochemical indices and thiobarbituric acid-reactive substances (TBARS)
Venous blood samples (4 mL) were collected on the last day after a 12-h fast into a 10 mL vacutainer tube containing heparin, and centrifuged at 1000 g to obtain the plasma for analysis. Blood was assured to be non-hemolytic. Plasma total cholesterol, triglyceride, urea nitrogen, creatinine, albumin, uric acid, AST and ALT levels were determined using an automatic analyzer (CX5 Synchron, Beckman, USA).
Aliquots of plasma were stored at -80 C for analysis of TBARS, according to the method described in Draper et al. with slight modifications.[16] Tenth mL of plasma or malonaldehyde dimethyl acetal (MDA) as the standard, and 30 L 0.091 mol/L of butylated hydroxytoluene, were mixed with 0.2 mL 0.02 mol /L of thiobarbituric acid. The mixture was boiled for 30 min in the dark. After cooling to ambient temperature, TBARS was extracted with 0.5 mL of n-butanol. The absorbance at 532 nm was measured. TBARS concentration was calculated in reference to MDA standards.
Statistics
All data were expressed as means ± SEM and analyzed with SPSS version 10.0 for Windows (SPSS, Inc., Chicago, IL). The fecal bacterial counts were log-transformed. All data were with normal distribution and treated as parametric data. Data were analyzed with repeated measure ANOVA followed by LSD analysis to compare the difference between two periods. The association between fecal bifidobacteria excretion and plasma measurement was determined using Pearson’s correlation. Effect was considered significant as P < 0.05.
Results
Subjects consumed the controlled defined diet all through the experiment; the dietary intake of nutrients and fluids are shown in Table 2. These subjects consumed similar amount of fluid, energy and nutrient among placebo, FOS and post period. The dietary fiber intake was approximately 1.55 g/mJ, 6.46 g/kcal.
Fecal wet weights are reported because use of enema may cause extra fluid excretion and overestimate the weight. Supplement of FOS increased fecal dry weight per week by 42% (P
= 0.024), but not dry weight per stool (P = 0.18), as compared with fecal weights during the placebo period (Table 3). The dry weight and dry weight per stool were not significantly greater in the post period as compared to the placebo period. Supplementation of FOS did not increase spontaneous defecation frequency, but significantly reduced the use of enema (P <
0.05) as compared to those in the placebo period. The decreased use of enema with FOS supplement did not sustain through the post period.
Fecal counts (Log counts/g dry feces) of bifidobacteria significantly increased (P =
0.002); clostridia significantly decreased (P = 0.02); total bacteria counts did not significantly change in the FOS period as compared with the placebo period d (Table 4).
FOS supplement also effectively increased the daily fecal outputs of bifidobacteria (P = 0.004) and total bacteria (P = 0.03). The increased bifidobacteria output with FOS supplementation lasted through the post period (P = 0.01). Bifidobacteria contributed to 11.9 ± 3.8% of total fecal bacteria in the placebo, which was not significantly different from that in the FOS (12.5 ± 4.5%) or post (12.8 ± 5.3%) period, respectively.
The plasma TBARS concentration in the placebo period was 12.5 0.6 μmol/L, which was significantly reduced to 10.9 0.5 (P = 0.09) in the FOS period, and 10.3 0.4 (P
= 0.02) in the post period. Plasma concentrations of cholesterol, triglyceride, urea nitrogen, creatinine, albumin, and uric acid during different periods are shown in Table 5. The plasma cholesterol level was significantly reduced by approximately 7% in the FOS period (P
= 0.043) and post period (P = 0.039), respectively, as compared to that in the placebo period. Plasma urea nitrogen level was significantly reduced by ~15% in the FOS period (P
= 0.049) as compared to that in the placebo period. Plasma concentrations of triglyceride, creatinine, albumin, uric acid and activities of AST and ALT remained unchanged during the study.
The increase in fecal bifidobacteria output during the FOS period (Log10 CFU/d) was significantly associated with decrease in plasma TBARS (P = 0.02) or cholesterol concentrations (P = 0.04) (Fig. 1), but not correlated with the decrease in plasma urea nitrogen concentration ( = 0.41, P = 0.31).
The body weight (kg) was 51.4 4.0, 52.8 4.0 and 54.0 4.0, with body mass index (kg/m2) 20.8 1.3, 21.4 1.2 and 21.9 1.2, in the placebo, FOS and placebo period, respectively. The body weights exerted time effect (P = 0.022), and the weights in the post period was significantly greater that in the placebo period.
Discussion
Our study, in agreement with a previous observation from a small group of constipated elderly men, observed that FOS supplementation significantly increased dry fecal mass (~
0.41 g increase /g FOS ingested).[17] The bulky effect partially diminished at the end of post period, which suggested the metabolism of FOS was associated with its bulky effect. A previous study indicated that the bulky effect of fermentable fiber mainly was due to increased bacterial mass [18]. An increased bacterial population (CFU/g dry feces) has been observed in this study, which may partially mediates the bulky effect of FOS.
Although the defecation frequency did not increase with FOS, the decreased enema usage and slight change in fecal dry weight per stool suggest the passage of stool was more feasible and complete with FOS supplementation in our subjects. Since reduced swallowing and chewing ability limit the amount of fiber consumed by the Taiwanese elderly [1], supplementation of soluble oligosaccharides could be an important regimen to improve their bowel functions. The increased fecal dry mass and decreased enema usage did not sustain to
the post period, which suggest continuous supplementation is required to maintain significant improvement of bowel function in the chronically constipated older persons.
The bifidogenic effect of FOS in healthy adults has been extensively demonstrated in well-controlled human trials [6,7,19,20], but is rarely demonstrated in the elderly humans.
These previous studies concluded that around 10 g of FOS per day effectively stimulated the proliferation of colonic bifidobacteria. Similar to previous studies, our study confirms that this dose (10 g, 4 wk) of FOS significantly increases fecal concentration and daily excretion of bifidobacteria in the constipated elderly. This bifidogenic effect did not fully sustain at the end of post period (28 d), which also was similar to a previous study that bifidogenic effect of FOS and partially-hydrolyzed guar gum mixture diminished at 14 day after its withdrawal [21]. However, we observed an increased daily output of fecal bifidobacteria in the post period as compared to that in the placebo period, which was likely to be due to slight, but not statistically significant, increases in both the fecal mass and fecal bifidobacteria concentration.
The antioxidative properties of prebiotics in rats [22] and humans [11] have been previously reported. We further demonstrated that FOS supplementation reduced plasma lipid peroxidative level in the elderly. In addition, our study demonstrated that the antioxidative effect of FOS supplementation was closely associated with its bifidogenic effect. This result is supported by previous in vitro studies that the intact cells [23,24], cell-free intracellular extract [23] or cell walls of lactic acid bacteria [25], and the fermentation of FOS by lactic acid bacteria [10] exert antioxidative effects. Although the mechanism is unclear, a recent study indicates that fermentation of FOS by lactic acid bacteria increases the radical scavenging ability and reduces the lipid peroxide.[10] Therefore, colonic bifidobacteria are likely to be a vital component involved in the antioxidative effects of FOS in humans.
Although dietary supplementation of inulin (10%) has been reported to decrease total serum cholesterol level in normolipidemic rats [26] and reduce hepatic cholesterol level and atherosclerotic lesion area in aortic sinus in apolipoprotein E-deficient mice [27], the mechanism by which FOS exerted hypocholesterolemic effect remains to be investigated.
The enhanced fecal bile acid output with FOS supplementation in mice [28] and inhibition of hepatic cholesterogenesis by propionate that is generated from fermentation [29] could partially mediate the hypocholesterol effects of FOS. However, other mechanism was involved in this effect since the hypocholesterolemic effect remained after FOS was withdrawn. An in vitro study have suggested that lactic acid bacteria assimilate cholesterol from the culture medium.[30] Therefore, it is hypothesized that FOS may increase fecal cholesterol excretion by stimulating bifidobacteria growth, which in turn reduces the blood cholesterol level. Our study found a close association between the FOS-induced increase in fecal bifidobacteria excretion and the FOS-induced decrease in plasma cholesterol level, which support that bifidobacteria may mediate the hypocholesterolemic effect of FOS in the elderly subjects.
The role of FOS on nitrogen metabolism has been extensively studied in normal rats and in renal-failure animal models.[31-33] These studies conclude that FOS reduces blood urea concentration and this effect is in a dose-dependent pattern.[32] Our study extended this
finding that FOS reduced BUN in nursing-home residents whose renal function was normal.
Although the increased daily excretion of bifidobacteria was not closely associated with the decreased BUN, FOS is likely to enhance the blood urea utilization by colonic microflora which therefore enhances the fecal disposal of nitrogen waste.[34]
Conclusion
Results from this study conclude that addition of 10 g of FOS per day to a low fiber diet can stimulate the dry fecal mass, proliferation and fecal excretion of bifidobacteria, and exert beneficial effects on blood antioxidative status, lipid, and urea status in constipated nursing-home residents. The beneficial effect of FOS on daily excretion of fecal bifidobacteria, and plasma TBARS and cholesterol levels sustain for 28 d after its withdrawal.
bifidogenic function of FOS may mediate its antioxidative effects.
Acknowledgements
This work was supported in part by grant NSC-96-2320-B-040-031-MY3, National Science Council, Taiwan, ROC. Supply of fructo-oligosaccharide by the Institute for Microbial Resources (Taichung, Taiwan) is appreciated. No conflict of interest applied in this work.
References
[1] Chen HL, Huang YC. Fiber intake and food selection of the elderly in Taiwan. Nutr 2003;
19: 332-6.
[2] Read NW, Celik A F, Katsinelos P. Constipation and incontinence in the elderly. J Clin Gastroenterol 1995; 20: 61-70.
[3] Hildebrandt G, Dominguez BL, Schork MA, Loesche WJ. Functional units, chewing, swallowing, and food avoidance among the elderly. J Prosthe Dent 1997; 77: 588-95.
[4] Gibson GR, Beatty ER, Wang X, Cummings JH. Selective stimulation of bifidobacteria in the human colon by oligofructose and inulin. Gastroenterology 1995; 108: 975-82.
[5] Liu S, Ling Y, Tasi C. Biotechnically synthesized oligosaccharides and polydextrose reduce constipation and putrefactive metabolites in the human. J Chinese Nutr Soc (Taiwan) 1994; 19: 221-32.
[6] Bouhnik Y, Vahedi K, Achour L, Attar A, Salfati J, Pochart P, et al. Short-chain fructo-oligosaccharide administration dose-dependently increases fecal bifidobacteria in healthy humans. J Nutr 1999; 129: 113-6.
[7] Buddington RK, Williams CH, Chen SC, Witherly SA. Dietary supplement of neosugar alters the fecal flora and decreases activities of some reductive enzymes in human subjects. Am J Clin Nutr 1996; 63: 709-16.
[8] Hopkins M, Sharp R, Macfarlane G. Age and disease related changes in intestinal bacterial populations assessed by cell culture, 16S rRNA abundance, and community cellular fatty acid profiles. Gut 2001; 48: 198-205.
[9] Ames BN, Shigenaga MK, Hagen TM. Oxidants, antioxidants, and the degenerative diseases of aging. P Natl Acad Sci USA 1993; 90: 7915-22.
[10] Wang C-H, Lai P, Chen M-E, Chen H-L. Antioxidative capacity produced by Bifidobacterium- and Lactobacillus acidophilus-mediated fermentations of konjac glucomannan and glucomannan oligosaccharides. J Sci Food Agric 2008; 88: 1294-1300.
[11] Seidel C, Bovhm V, Vogelsang H, Wagner A, Persin C, Glei M, et al. Influence of
prebiotics and antioxidants in bread on the immune system, antioxidative status and antioxidative capacity in male smokers and non-smokers. Br J Nutr 2007; 97: 349-56.
[12] Mahoney FI, Barthel DW. Functional evaluation: The Barthel Index. Maryland State Med Journal 1965; 14: 56-61
[13] Nutrient composition data bank for foods of Taiwan area. Taipei Taiwan: Department of Health, 1998.
[14] Jansen G, Wildeboer-Veloo AC, Tonk RH, Franks AH, Welling GW. Development and validation of an automated, microscopy-based method for enumeration of groups of intestinal bacteria. J Microbiol Method 1999; 37: 215-21.
[15] Nagahama M, Nagayasu K, Kobayashi K, Sakurai J. Binding component of Clostridium perfringens iota-toxin induces endocytosis in Vero cells. Infect Immun 2002;70:1909-14.
[16] Draper HH, Hadley M. Malondialdehyde determination as index of lipid peroxidation.
Methods Enzymol 1990; 186: 421-31.
[17] Chen H-L, Lu Y-H, Lin J-J, Ko L-Y. Effects of fructooligosaccharide on bowel function and indicators of nutritional status in constipated elderly men. Nutr Res 2000; 20:
1725-33.
[18] Chen H-L, Haack VS, Janecky CW, Vollendorf NW, Marlett JA. Mechanisms by which wheat bran and oat bran increase stool weight in humans. Am J Clin Nutr 1998;
68:711-719.
[19] Bouhnik Y, Raskine L, Simoneau G, Vicaut E, Neut C, Flourie B, et al. The capacity of nondigestible carbohydrates to stimulate fecal bifidobacteria in healthy humans: a double-blind, randomized, placebo-controlled, parallel-group, dose-response relation study. Am J Clin Nutr 2004; 80: 1658-64.
[20] Gibson GR, Roberfroid MB. Dietary modulation of the human colonic microbiota:
introducing the concept of prebiotics. J Nutr 1995; 125: 1401-12.
[21] Tuohy, KM, Kolida S, Lustenberger AM, Gibson GR. The prebiotic effects of biscuits containing partially hydrolysed guar gum and fructo-oligosaccharides--a human volunteer study. Br J Nutr 2001; 86:341-8.
[22] Busserolles J, Gueux E, Rock E, Demigné C, Mazur A, Rayssiguier Y. Oligofructose protects against the hypertriglyceridemic and pro-oxidative effects of a high fructose diet in rats. J Nutr 2003; 133: 1903-8.
[23] Lin M-Y, Chang F-J. Antioxidative effect of intestinal bacteria Bifidobacterium longum ATCC 15708 and Lactobacillus acidophilus ATCC 4356. Dig Dis Sci 2000; 45: 1617-22.
[24] Lin M-Y, Yen C-L. Inhibition of lipid peroxidation by Lactobacillus acidophilus and Bifidobacterium longum. J Agric Food Chem 1999; 47: 3661-4.
[25] Yagi R, Doi M. Isolation of an antioxidative substance produced by Aspergillus repens.
Biosci Biotechnol Biochem 1999; 63: 932-3.
[26] Fiordaliso M, Kok N, Desager JP, Goethals F, Deboyser D, Roberfroid M, et al. Dietary oligofructose lowers triglycerides, phospholipids and cholesterol in serum and very low density lipoproteins of rats. Lipids 1995; 30: 163-7.
[27] Rault-Nania MH, Gueux E, Demougeot C, Demigné C, Rock E, Mazur A. Inulin attenuates atherosclerosis in apolipoprotein E-deficient mice. Br J Nutr 2006; 96: 840-4.
[28] Chen H-L, Hsiang Y-Y, Wu W-T, Lin M-S. Hypolipidemic effects of inulin and synthetic oligofructose in Balb/c mice. Nutr Sci J (Taiwan) 2005; 30:99-107.
[29] Demigné C, Morand C, Levrat MA, Besson C, Moundras C, Rémésy C. Effect of propionate on fatty acid and cholesterol synthesis and on acetate metabolism in isolated rat hepatocytes. Br J Nutr 1995; 74:209-19.
[30] Pereira D, Gibson G. Effects of consumption of probiotics and prebiotics on serum lipid levels in humans. Crit Rev Biochem Mol Biol 2002; 37: 259-81.
[31] Younes H, Demigné C, Behr S, Rémésy C. Resistant starch exerts a lowering effect on plasma urea by enhancing urea n transfer into the large intestine. Nutr Res 1995; 15:
1199-210.
[32] Younes H, Rémésy, Behr S, Demigné C. Fermentable carbohydrate exerts a urea-lowering effect in normal and nephrectomized rats. Am J Physiol 1997; 272:
G515-21.
[33] Younes H, Alphonse J C, Hadj-Abdelkader M, Rémésy C. Fermentable carbohydrate and digestive nitrogen excretion. J Ren Nutr 2001; 11: 139-48.
[34] Geboes KP, De Hertogh G, De Preter V, Luypaerts A, Bammens B, Evenepoel P, et al.
The influence of inulin on the absorption of nitrogen and the production of metabolites of protein fermentation in the colon. Br J Nutr 2006; 96: 1078-86.
-1 0 1 2 3 4 5 6 7 8
0 0.05 0.1 0.15 0.2 0.25 0.3 0.35
-20 -10 0 10 20 30 40 50 60
0 0.05 0.1 0.15 0.2 0.25 0.3 0.35
A
B
Change in bifidobacteria
( Log CFU/d FOS period –Log CFU/d Placebo period) Decrease in plasma cholesterol (M) Decrease in plasma TBARS (M)
=0.67, P=0.02
=0.69, P=0.04
Fig. 1. Correlation between the changes in daily excretion of fecal bifidobacteria (Log CFU/d in FOS Log CFU/d in placebo period) and the decrease in plasma (A) TBARS or (B) cholesterol concentration. The association between fecal bifidobacteria excretion and plasma measurement was determined using Pearson’s correlation. Effect was considered significant as P < 0.05.
Table 1. Seven-day cycle menu*
Day Menu
Day 1
Breakfast Rice porridge, pork shred, Chinese cabbage
Lunch Rice/ porridge , fried tofu, Swordfish, Chinese spinach Snack Canned fruit cocktail
Dinner Fried chicken, chicken wing, corn, ham, cabbage, Yuba, Snack Milk/soy milk, brown rice powder
Day 2
Breakfast Rice porridge, pork shred, bean sprout
Lunch Rice/porridge, sweet potato leaves, pickle, Tofu, scrambled pork and carrot
Snack Guava
Dinner Rice/ porridge, bok choy, Chinese cabbage, kiss larval Snack Milk/soy milk, brown rice powder
Day 3
Breakfast Rice porridge, pork shred, canned peanut gluten, squash
Lunch Rice /porridge, stewed pork, bamboo shoot, Chinese spinach, fish fillet, mushroom
Snack Banana
Dinner Rice/ porridge, egg, chicken nugget, bok choy, Chinese mushroom Snack Milk/soy milk, brown rice powder
Day 4
Breakfast Rice porridge, pork shred, pickle
Lunch Rice/ porridge, roasted drumstick, bok choy, mushroom Snack Apple
Dinner Rice/ porridge, pan-fried milk fish, carrot, pork slice, bamboo shoot
Snack Milk/soy milk, brown rice powder Day 5
Breakfast Rice porridge, pork shred, seaweed sauce
Lunch Stir-fried noodles with carrot, onion, pork, cabbage Snack Watermelon
Dinner Meatball, imitated chicken (soy product), sunset egg, bok choy Snack Milk/soy milk, brown rice powder
Day 6
Breakfast Rice porridge, pork shred, pickle, stewed peanut gluten Lunch Dumpling, vegetable soup
Snack Grape
Dinner Rice/porridge, pan-fried meat fish, bean sprout, carrot, sunset egg Snack Milk/soy milk, brown rice powder
Day 7
Breakfast Rice porridge, pork shred, stewed tofu
Lunch Scrambled noodle with carrot, onion, pork, shrimp, cabbage Snack Banana
Dinner Rice/porridge, stewed fish, ground pork, bean noodle, cucumber Snack Milk/soy milk, brown rice powder
*The weight of each food provided to volunteers were individually designed to meet their dietary habit and energy requirement.
Table 2. The daily fluid, energy and nutrient intakes of subjects in the placebo, fructooligosaccharide-supplemented (FOS) and the post periods*
Placebo FOS Post
Fluid (L) 1.5 ± 0.1 1.5 ± 0.1 1.5 ± 0.1
Calories (MJ) 5.4 ± 0.6 5.4 ± 0.8 5.4 ± 0.8
Carbohydrate (g) 157.9 ± 4.5 157.2 ± 4.2 158.0 ± 4.4
Protein (g) 56.2 ± 3.0 56.4 ± 2.4 56.2 ± 2.7
Fat (g) 49.4 ± 1.3 49.2 ± 2.0 49.3 ± 1.8
Dietary fiber (g) 8.4 ± 0.3 8.4 ± 0.4 8.4 ± 0.3 Calcium (mg) 613.4 ± 24.6 613.0 ± 24.5 613.0 ± 24.5 Phosphorous (mg) 853.1 ± 45.5 853.1 ± 45.5 853.1 ± 45.5 Vitamin A (R.E.) 926.9 ± 84.2 927.9 ± 60.4 928.0 ± 59.2 Vitamin B1 (mg) 0.5 ± 0.1 0.5 ± 0.1 0.5 ± 0.1 Vitamin B2 (mg) 1.1 ± 0.1 1.1 ± 0.1 1.1 ± 0.1
Niacin (mg) 10.0 ± 0.7 10.0 ± 0.7 10.0 ± 0.7
Vitamin C (mg) 93.6 ± 2.9 93.6 ± 2.9 93.6 ± 2.9 Percentage of total calories (%)
Carbohydrate 48.7 ± 0.9 48.4 ± 0.8 48.7 ± 0.7 Protein 17.3 ± 0.7 17.4 ± 0.7 17.2 ± 0.7 Fat 34.3 ± 0.6 34.2 ± 0.6 34.1 ± 0.6
*Data shown were the average of 3 nonconsecutive days during each period and expressed as means ± standard error of mean (n=10).
Table 3. Fecal output and bowel movement of subjects in the placebo, fructooligosaccharide-supplemented (FOS) and the post periods
Placebo FOS Post
Fecal output
Dry weight (g/wk ) 53.2 ± 8.4 a 82.0 ± 11.1 b 71.8 ± 10.5 ab Dry weight (g/stool) 13.3 ± 3.0 20.1 ± 3.3 16.7 ± 3.5 Bowel movement (no./wk)
Spontaneous defecation 4.5 ± 0.8 4.2 ± 0.5 4.3 ± 0.8 Enema 0.4 ± 0.2 b 0.2 ± 0.1 a 0.5 ± 0.2 b
*Values in a row not sharing the same superscript denotes for significant difference (P<
0.05) as analyzed by repeated ANOVA followed by LSD test. Values are means ± SEMs (n=9).
Table 4. Fecal bifidobacteria, clostridia and total bacteria counts (Log counts/g dry feces) of subjects in the placebo, fructooligosaccharide-supplemented (FOS) and the post periods
Fecal bacteria Placebo FOS Post
Bifidobacterium 9.6 ± 0.1 a 9.8 ± 0.1 b 9.7 ± 0.1 a
Clostridium 9.8 ± 0.1 b 9.6 ± 0.1 a 9.8 ± 0.1 b
Total 10.8 ± 0.1 11.0 ± 0.1 10.9 ± 0.1
*Values in a row not sharing the same superscript denotes for significant difference (P<
0.05) as analyzed by repeated ANOVA followed by LSD test. Values are means ± SEMs (n=9).
Table 5. Plasma biochemical parameters at the end of the placebo, fructooligosaccharide-supplemented (FOS) and the post periods
Placebo FOS Post
Biochemical parameters
Cholesterol (mmol/L) 4.8 0.2b 4.5 0.2a 4.5 0.2a Triglyceride (mmol/L) 1.9 0.8 1.4 0.2 1.8 0.8 Urea nitrogen (mmol/L) 7.0 0.8b 6.0 0.6 a 6.9 1.0b Creatinine (μmol/L) 106.1 13.8 102.7 34.5 106.1 13.8 Albumin (g/L) 36.4 0.5 35.7 0.5 34.5 0.8 Uric Acid (μmol /L) 331.3 43.5 336.7 44.4 306.3 32.5
AST (U/L) 19.6 ± 1.0 19.9 ± 1.8 18.2 ± 1.3
ALT (U/L) 16.1 ± 2.6 17.1 ± 4.3 13.6 ± 1.4
AST, aspartate aminotransferase; ALT, alanine aminotransferase.
*Values in a row not sharing the same superscript denotes for significant difference (P<
0.05) as analyzed by repeated ANOVA followed by LSD test. Values are means ± SEMs (n=9).
YEAR OF 2008
中文摘要
本研究探討生技寡醣異麥芽寡醣對安養中心低活動力老人腸道生理、菌相的調節作 用,以及血液過氧化狀態的影響。本研究於台中市安養中心進行,以固定飲食型態下分 為安慰劑期、補充 1 期、補充 2 期及恢復期,各為期四周。研究成果已被接受刊登(Nutrition) 並且已先行於網路上刊登,敬附論文於下。
關鍵詞:異麥芽寡醣、老人、糞便細菌酵素、氧化壓力、短鏈脂肪酸、腸道功能
Long-term supplementation of isomalto-oligosaccharides improved colonic microflora profile, bowel function and blood cholesterol levels in constipated elderly people—A
placebo-controlled, diet-controlled trial 將刊登於 Nutrition 2010 (in press) ABSTRACT
Objectives: The main purpose of this study is to determine the long-term (8 wk) effects of isomalto-oligosaccharide (IO) supplementation on fecal microflora, bowel function, and biochemical indicators of nutritional status in constipated elderly subjects. We also assessed whether the effect of IO was sustained after its withdrawal.
Methods: Thirteen (5 male) constipated subjects (age 82.5 1.9 years) participated in this diet-controlled study that consisted of a 4-wk placebo period, two 4-wk IO (10 g/d)-supplementation periods (IO1 and IO2), and a 4-wk post period. Fasting blood was collected on the last day of each period. Stools were collected during the last week of each period. The bowel function was monitored throughout the study.
Results: The fecal bifidobacteria, lactobacilli, and bacteroides counts (log counts/g wet feces) significantly increased and clostridia count decreased at the end of the IO1 period. The effects were more pronounced in the IO2 period, and then returned to the levels of the IO1 period at the end of the post period. Daily fecal excretion of acetate and propionate increased along with IO supplementation. The frequency of spontaneous defecation increased in the IO2 period, and wet fecal mass increased by 24% in both the IO1 and IO2 periods. The effects of IO on bowel function diminished in the post period. Plasma total and LDL-cholesterol levels were lower with 4- or 8-wk IO supplementation as compared with the placebo and post period, respectively.
Conclusions: IO supplementation into a low-fiber diet improved colonic microflora profile and bowel movement in a time-dependent fashion in constipated elderly subjects. These beneficial effects decreased after discontinuation of the supplements.
Key words: isomalto-oligosaccharide; bifidobacteria; Clostridium perfringens, cholesterol, bowel function, elderly
INTRODUCTION
Impaired bowel function, particularly constipation, is a common complaint of ill or inactive elderly people (1, 2). Populations with poor chewing ability need suitable dietary fiber supplements that can easily be incorporated into their ordinary diet to maintain regular bowel movements. Isomalto-oligosaccharides (IO), such as isomaltose, panose,
isomaltotriose and isomaltotetraose, naturally exist in Japanese fermented foods such as miso, soy sauce and sako and are commercially produced from corn starch to be a functional food ingredient (3). These oligomers contain 1 6 glucosidic linkages (3) that resist endogenous digestion (4) and may exert a biological function similar to dietary fiber.
Administration of 10 g of active components of IO for four week has been shown to improve the defecation frequency in a placebo-controlled and diet-controlled study that included only a small group of severely constipated elderly men (5). Therefore, IO is potentially a functional food to relieve constipation in the elderly. The elderly are likely to require long-term use of laxatives. However, the long-term effects of IO supplementation have not been determined.
Aging has been associated with decreased fecal bifidobacteria concentrations (6), which may partially be associated with dysfunction of the intestine, decreased immunity, and greater susceptibility to disease. Colonic microflora are responsible for a wide variety of metabolic activities that modulate human health. For instance, fermentation of dietary fibers by colonic microflora beneficially modulates colonic health through its metabolites, including the organic acids and short chain fatty acids that protect and support the normal turnover of the colonocytes (7, 8). Several studies have suggested that supplementation of IO in healthy adults increases the fecal bifidobacteria concentration (3, 9). However, there are a lack of studies demonstrating the modulatory effects of IO on colonic bacteria profile and the prolonged effects of the supplementation after its withdrawal in older populations.
The aim of this study was to evaluate the effects of eight weeks of ingestion of IO on fecal microflora, bowel function, fecal short chain fatty acids (SCFAs), and plasma biochemical indices in constipated elderly subjects, and to observe whether these effects were sustained after withdrawal for four weeks, in a diet-controlled, placebo-controlled trial.
SUBJECTS AND METHODS Subjects
Residents living in a local nursing home were recruited into this study. The criteria for recruitment were; stable physiological condition, long-term residence (> 6 months), chronic constipation (> 6 months), ability to chew a soft or blended diet, not bed-ridden, and no tobacco or antibiotic use. In addition, subjects agreed to comply with the cycled menus and fecal specimen collection. The exclusion criteria were; subjects who were with plasma AST >
80 U/L, Cr > 132.6 μmol/L (1.5 mg/dL), or with a clinically terminal or wasting illness.
Thirteen elderly subjects (5 males) with age (means ± SEM) 82.5 ± 1.9 years completed the study with good compliance. The mean weight and body mass index were 52.5 ± 2.9 kg and 20.9 ± 1.1 kg/m2, respectively. Seven subjects had history of cerebrovascular accident. Ten of the subjects were treated for constipation with MgO, bisacodyl, sennoside, or a combination of any two. All medical treatments were kept constant throughout the study.
Experimental design
This double-blind, placebo-controlled, diet-controlled study consisted of a run-in period, 4-wk placebo (3 mL fructose syrup) period, two 4-wk IO periods (first and second 4 wk as IO1, IO2 period), and a 4-wk post period. Diets were designed for individual subjects based on an assessment before the run-in period. Subjects consumed their refined diet from the run-in period through the end of the post period. Isomalto-oligosaccharide was consumed as an afternoon drink, and the dose was gradually increased from 11 g/d (equivalent to 5.0 g of active component) to 22 g/d (equivalent to 10.0 g of active component) in the first seven days
of the IO1 period, and was kept at 22 g/d throughout the remaining IO period to avoid potential intestinal distension. IO was withdrawn during the post period. Body weight and height were determined on the last day of each period.
Three-days of food intake were assessed in each period to assure the constant nutrient and dietary fiber intake. Subjects were treated with enemas if spontaneous defecation did not occur in three days or as requested by the subjects. The incidence of spontaneous defecation and enema use was recorded every day and is expressed as incidence (no./wk) in this study.
Stools voided during the last week of each period were individually collected in plastic bags and sent to the laboratory immediately to determine the fecal characteristics and microflora.
The experimental protocol was approved by the Committee on Human Study at the Chung Shan Medical University Teaching Hospital. All subjects gave written informed consent.
Diet
Subjects were given a 7-day cycle menu (Table 1) designed by a registered dietitian in the ward, from one month before the experiment to the end of the post period in order to prevent the confounding effect of dietary variation. Four subjects consumed a blended diet while the remaining a soft or regular diet. Any other supplements, including antioxidants, other oligosaccharides- or lactic acid bacteria-containing foods, were not allowed during the study. The IO powder (Tamaru Enterprise Co., Taichung, Taiwan) contained 45% (w/w) IO active component, isomaltose 11.7%, panose 26.2%, isomaltotriose 1.95% and isomaltotetraose 5.15%. Fructose syrup (Pay Inc., Taipei, Taiwan), composed (w/w) of fructose (55%), glucose (20%), and moisture (25%), was used as the placebo. Both IO and fructose were administered to subjects in 100 mL drinking water as an afternoon snack.
Dietary intake
In order to assess the average intake of fluid, energy, nutrients and dietary fiber, meals and fluids served to and left over by the subjects were weighed and recorded for three non-consecutive days during each period. The nutrient content of all food ingested by the subjects was determined using local nutrient composition tables (10).
Measurement of fecal pH and moisture
Feces voided were immediately collected in plastic bags, vacuumed, sealed, and immediately sent to our laboratory in ice buckets within 4 hr of defecation. The pH was determined by inserting the probe to the center of the fecal homogenate. The fecal pH of each subject was taken from the mean values of 7-d fecal samples collected during the final week of each period. Aliquots of fresh feces were pooled together for analysis of short chain fatty acids. The remaining feces were homogenized with an equal weight of deionized water in a stomacher, lyophilized and stored at –20 C. All lyophilized feces excreted by an individual were pooled together as a fecal composite for further analysis of fecal microflora. The fecal moisture was determined by comparing the wet and dry weights of fecal samples.
Quantitation of fecal bacteria
Fecal bacteria populations were assessed using the fluorescence in situ hybridization method (FISH), in which genotypic probes targeting 16S rRNA are designed for specific bacteria (11). The probes used in this study were Bif164 (5’-CAT CCG GCA TTA CCA CCC-3’), Laa1 (5’-CAT CCA GTG CAA ACC TAA GAG-3’), Bac303 (5’-CCA ATG TGG GGG ACC TT-3’), and Ib1 (5’-GAT GGA ACT GTA ACA AAA CT-3’), specific for
bifidobacteria (11), lactobacilli (12), bacteroides (13) and clostridia (14), respectively. The nucleic acid stain 4’, 6-diamidino-2-phenylindole (DAPI) was used for total bacterial counts.
The bacterial solution obtained during the fractionation of feces was fixed in a 3-fold volume of 4% paraformaldehyde solution overnight at 4 C. The lyophilized fecal composite was individually fractionated using the method described previously (5) to separate fecal plant material from the bacteria. Aliquots (5 L) of the fecal bacteria fraction were fixed on wells of microscopic slides following the method described previously (11, 15). To quantify the total fecal bacteria, slides were incubated with a nucleic acid stain, 4’, 6-diamidino-2-phenylindole, as described previously (11, 15). Probe fluorescence was detected with a Zeiss Axioskop2 microscope (Carl Zeiss, Jena, German) fitted for epifluorescence microscopy with a 100 W mercury bulb (HBO 103), a 20 Plan-Neofluar objective, a filter set 01, 09 and 20, and a cooled charge-coupled device (CCD) video camera (MacroFire, Model S99831, Optronics, Goleta, CA). The microbial counts were expressed as log10 counts/g feces.
Measurement of fecal short chain fatty acids
Aliquots (0.5 g) of fecal composite were analyzed for acetate, propionate, i-butyrate and n-butyrate with 4-methyl-n-valeric acid as an internal standard, as described previously (16). The SCFAs extracted from the fecal samples were dissolved in 10% orthophosphoric acid solution immediately before they were injected onto a gas chromatograph (GC-14B, Shimadzu, Tokyo, Japan) fitted with a glass capillary column (0.25 mm, 30 m Stabilwax-DA, Restek Corp., Bellefonte, PA) and a flame ionization detector. The initial temperature of the oven was 100 C and was raised to 200 C at 6 C /min. The temperature of the injection port and detector were both at 250C. The flow rate of the carrier gas, N2,was adjusted to be 1 mL/min. Peak areas were analyzed with a C-R6A Chromatopac (Shimadzu Corp., Tokyo, Japan).
Blood preparation and measurements of plasma biochemical indices
Venous blood samples (4 mL) were collected on the last day after a 12-h fast into a 10 mL vacutainer tube containing heparin, and centrifuged at 1000 g to obtain the plasma for analysis. Blood was assured to be non-hemolytic. Plasma sugar, total cholesterol, HDL-cholesterol, triglyceride, urea nitrogen, creatinine, albumin, and ALT levels were determined using an automatic analyzer (CX5 Synchron, Beckman, USA). LDL cholesterol levels were calculated based on the equation described by Friédewald et al. (17).
Statistical analysis
All data were expressed as means ± SEM and analyzed with SPSS version 14.0 for Windows (SPSS, Inc., Chicago, IL). The log-transformed bacteria counts and all other data were analyzed using General Linear Model repeated measures ANOVA followed by pair-wise LSD tests (18). A P value less than 0.05 was considered statistically significant.
Results
Fecal bacteria
Fecal counts (log counts/g wet feces) of bifidobacteria, lactobacilli, bacteroides, and total bacteria significantly increased at the end of the IO1 period, further increased at the end of the IO2 period, and remained greater in the post period than the level in the placebo period
(Table 2). In contrast, the fecal clostridia count significantly decreased at the end of the IO1 period as compared with the level in the placebo period, but this reduction was the most pronounced at the end of the IO2 period. At the end of the post period, the fecal clostridia counts remained lower than the level of the placebo period.
Bifidobacteria composed approximately 10% of total fecal bacteria at the end of the placebo period, which gradually increased to ~15% at the end of the IO2 period, and then decreased to a level slightly greater than the placebo level at the end of the post period. The relative counts (% total bacteria) of lactobacilli were double that of the placebo level at the end of the IO2 period. The relative counts of bacteroides remained constant throughout the study. Clostridia composed ~35% of total bacteria in the placebo period, to ~16% and ~9% in the IO1 and IO2 periods, respectively. The relative counts of clostridia remained at ~14% in the post period, similar to the level observed in the IO1 period.
Bowel function
The average frequency of spontaneous defecation and enema use throughout each period is shown in Table 3. The spontaneous defecation was low, only 1.2 per wk in the placebo period, which did not differ in the IO1 period, but significantly increased to 2.0 per wk in the IO2 period. However, the laxative effect of IO diminished in the post period. The frequency of enema usage tended to decrease with IO supplementation, but did not significantly differ among periods. Stool output was ~24% greater with either 4- or 8-wk IO supplementation as compared with the placebo. The increase in wet fecal mass was not sustained in the post period. Supplementation of IO for 4 and 8 weeks significantly increased the dry fecal mass by 16% and 12%, respectively, but this effect was not sustained to the post period. The fecal moisture and pH did not differ among groups.
Fecal short chain fatty acids
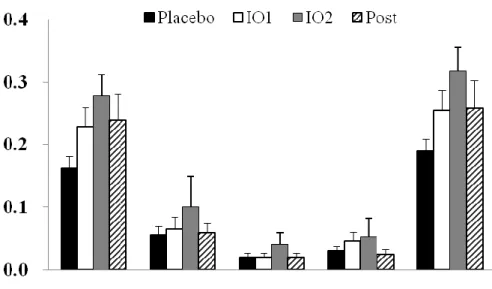
Acetate was the most dominant short chain fatty acid in feces collected in each period, with concentrations 42.6%, 89.2%, and 32% greater in the IO1, IO2, and post periods as compared with the level in the placebo period, respectively (Fig. 1A). Propionate was the second most dominant short chain fatty acid with a concentration 3.5-fold that of the level in the placebo period with 8-wk IO supplementation. The total short chain fatty acid concentrations were 42.6%, 89.2%, and 32.6% greater in the IO1, IO2, and post periods than that of the level of the placebo period, respectively. However, the fecal i-butyrate and n-butyrate concentrations did not differ significantly between periods. Furthermore, the daily fecal acetate excretion was 70.8%, 103.8%, and 45.2% greater in the IO1, IO2, and post periods than the level of the placebo period, respectively (Fig. 1B). The daily propionate output was significantly increased by 81.3% in the IO1 period, which further increased by 2-folds in the IO2 period, as compared with the output in the placebo period. The fecal n-butyrate outputs increased to 2- and 3-folds of the placebo level in the IO1 and IO2 periods, respectively. The daily outputs of total short chain fatty acids significantly increased by 75.9%, 134.0%, and 36.1% in the IO1, IO2, and post periods, respectively, as compared with the level in the placebo period. The fecal i-butyrate outputs did not significantly differ among periods.
Biochemical indices
The mean plasma biochemical measures of the subjects observed in this study were in the normal range for all periods (Table 4). The total and LDL cholesterol levels were lower at
the end of the IO1 and IO2 periods as compared with those in the placebo period. Plasma glucose, triglyceride, HDL-cholesterol, urea nitrogen, creatinine, albumin, and ALT levels remained constant among periods.
Energy and nutrient intakes
The subjects consumed similar amounts of fluid, energy and nutrients among the placebo, IO1, IO2 and post periods (Table 5). Carbohydrates, protein, and fat contributed to 59.9 ± 0.6%, 13.4 ± 0.2%, and 27.0 ± 0.4% of total energy, respectively, in the placebo period.
Anthropometric measurement
The body weight (kg) was similar among periods, 52.5 3.0, 52.6 3.0, 53.5 2.8 and 52.4 3.1, while the body mass index (kg/m2) was 20.9 1.1, 20.9 1.1, 21.4 1.1 and 20.9
1.1, in the placebo, IO1, IO2 and post periods, respectively.
Discussion
The profile of fecal microflora in these older subjects were different from those observed in young adults (15). The fecal clostridia composed more than 35% of the total fecal bacteria, which is almost 2-folds the level of that observed in young constipated adults, while the bifidobacteria ratio was only slightly lower than that in young constipated adults (15). This shift in microbial profile with age agrees with the observation described by Hopkins et al. (6).
The genus of Clostridium is pathogenic to humans (19). Therefore, decreasing clostridia can protect humans from diseases.
Supplementation of IO into a typical Chinese low-fiber diet was demonstrated in this study to exert beneficial time-course effects on the colonic microflora in older subjects. The profile of microflora was improved with 4-wk dietary IO supplementation, and the clostridia population was further reduced with 8-wk supplementation. This lactic-acid-bacteria promotive effect of IO suggests this oligosaccharide acts as a prebiotic in chronically-constipated older people and may help maintain their health. The microbial activity was also shown in the fecal short chain fatty acid levels. The increased fecal acetate and propionate concentrations, and the daily output of acetate, propionate and butyrate, suggest that IO was well-utilized by the colonic bacteria in our subjects. The bacteroides, major saccharolytic bacteria (20), also increased with IO supplementation, suggesting that IO can be utilized by bacteroides, which in turn increases the production of short chain fatty acids.
A previous study indicated that daily supplementation of 10 g of active IO component for 4 weeks significantly increased the defecation frequency in frail nursing-home residents, while the frequency of enemas was accordingly decreased by half (5). Our study extended the feeding period to two months and demonstrated time-dependent benefits in moderately-active older subjects. We observed a significant increase in the frequency of spontaneous defection, but no significant decrease in the frequency of enema usage with 8-wk IO supplementation, which did not agree with the previous study. The reason for the difference may be that the enema usage was not tightly controlled in this study and they could be administered on request of subjects who had relied on them for a long period of time. The effect of IO on fecal mass was first shown in the IO1 period, extending to the IO2 period, which suggests that IO can be a laxative in these older subjects. IO is fermented by colonic bacteria as shown in the
increased short chain fatty acid production in this study and a previous study (5), which could explain why the dry fecal mass only increased by 0.18 g for each gram of IO ingested. The increased fecal mass with IO supplementation could be partially due to residual IO and an increased colonic bacteria population.
The effect of IO on blood cholesterol level has rarely been studied, and results from previous studies are inconsistent. Supplementation of IO has been shown to reduce the blood cholesterol levels in healthy college men (21), but not in severely dysfunctional and constipated nursing-home residents (5). However, IO supplementation effectively reduced the plasma cholesterol level in our subjects who had a greater physical activity level and constipation was less severe than in subjects in the previous study (5). The mechanism by which IO modulates lipid homeostasis has never been investigated. The hypocholesterolemic effect of prebiotics has been proposed to be mediated by modulating bile acid metabolism in the intestine. Prebiotics may increase fecal steroid excretion and subsequently reduce the body pool of bile acids. A recent report indicated that feeding a fructo-oligosaccharide diet to rats significantly enhanced fecal bile acid output, but this study failed to prove a significant reduction in the pool size of cholate, a major component of bile acid (22). Another potential mediator for the hypocholesterolemic effect of IO could be propionate, which has been shown to inhibit hepatic cholesterol synthesis in isolated hepatocytes (23). The current study indicated decreased plasma cholesterol levels and increased fecal propionate outputs in the IO1 and IO2 periods. However, a greater increase in propionate output in the IO2 period was not associated with a greater decrease in plasma cholesterol levels. An in vitro study has suggested that lactic acid bacteria assimilate cholesterol from the culture medium (24).
Therefore, we hypothesize that IO may increase fecal cholesterol excretion by stimulating bifidobacteria growth, which in turn reduces the blood cholesterol level.
A previous study demonstrated that short-term (28 d) ingestion of 10 g IO did not exert adverse effects on nutritional indicators (5). The current study extended the feeding period to two months and found the body weight, plasma albumin, glucose, triglyceride, urea nitrogen, creatinine and ALT levels did not change among periods. No adverse abdominal symptoms were reported, either. Therefore, this study suggests its safety for use in the elderly.
Conclusions
Beneficial effects of IO on fecal microflora profile, defecation frequency, fecal mass and blood cholesterol levels were shown with 4-wk supplementation in chronically-constipated elderly people. A longer period of supplementation (8 wk) further improved the fecal microflora profile and the bowel function. Withdrawal of this supplement for 28 day reversed the changes that resulted from the supplements.
ACKNOWLEGEMENTS
This study was supported by grant NSC-96-2320-B-040-031-MY3, National Science Council, Taiwan, ROC. No conflicts of interest apply in this work.
REFERENCES
[1] Chen H-L, Huang Y-C. Fiber intake and food selection of the elderly in Taiwan. Nutr 2003;19:332-6.
[2] Read NW, Celik AF, Katsinelos P. Constipation and incontinence in the elderly. J Clin Gastroenterol. 1995;20:61-70.
[3] Kohmoto T, Fukui F, Takaku H, Machida Y, Arai M, Mitsuoka T. Effect of isomalto-oligosaccharides on human fecal flora. Bifidobacteria Microflora. 1988;7:61-9.
[4] Kohmoto T , Tsuji K, Kaneko T, Shiota M, Fukui F, Takaku H, et al. Metabolism of 13C-isomaltooligosaccharides in healthy men. Biosci Biotechnol Biochem.
1992;56:937-40.
[5] Chen H-L, Lu YH, Lin JJ, Ko LY. Effects of isomalto-oligosaccharides on bowel functions and indicators of nutritional status in constipated elderly men. J Am Coll Nutr.
2001;20:44-9.
[6] Hopkins M, Sharp R, Macfarlane G. Age and disease related changes in intestinal bacterial populations assessed by cell culture, 16S rRNA abundance, and community cellular fatty acid profiles. Gut. 2001;48:198-205.
[7] Emenaker N, Calaf G, Cox D, Basson M, Qureshi N. Short-chain fatty acids inhibit invasive human colon cancer by modulating uPA, TIMP-1, TIMP-2, mutant p53, Bcl-2, Bax, p21 and PCNA protein expression in an in vitro cell culture model. J Nutr.
2001;131:3041s-6s.
[8] Sanderson I. Short chain fatty acid regulation of signaling genes expressed by the intestinal epithelium. J Nutr. 2004;134:2450s-4s.
[9] Kohmoto T, Fukui F, Takaku H, Mitsuoka T. Dose-response test of isomaltooligosaccharides for increasing fecal bifidobacteria. Agric Biol Chem.
1991;55:2157-59.
[10] Nutrient composition data bank for food of Taiwan area. Taipei, Republic of China:
Department of Health; 1998.
[11] Jansen GJ, Wildeboer-Veloo AC, Tonk RH, Franks AH, Welling GW. Development and validation of an automated, microscopy-based method for enumeration of groups of intestinal bacteria. J Microbiol Methods. 1999 Sep;37:215-21.
[12] Wang RF, Cao WW, Cerniglia CE. PCR detection and quantitation of predominant anaerobic bacteria in human and animal fecal samples. Appl Environ Microbiol.
1996;62:1242-7.
[13] Manz W, Amann R, Ludwig W, Vancanneyt M, Schleifer KH. Application of a suite of 16S rRNA-specific oligonucleotide probes designed to investigate bacteria of the phylum cytophaga-flavobacter-bacteroides in the natural environment. Microbiology.
1996;142:1097-106.
[14] Nagahama M, Nagayasu K, Kobayashi K, Sakurai J. Binding component of Clostridium perfringens iota-toxin induces endocytosis in Vero cells. Infect Immun.
2002;70:1909-14.
[15] Chen H-L, Cheng H-C, Wu W-T, Liu Y-J, Liu S-Y. Supplementation of konjac glucomannan into a low-fiber Chinese diet promoted bowel movement and improved colonic ecology in constipated adults-- a placebo-controlled, diet-controlled trial. J Am Coll Nutr 2008;27:102-8.
[16] Rémésy C, Demigné C. Specific effects of fermentable carbohydrates on blood urea flux and ammonia absorption in the rat cecum. J Nutr. 1989;119:560-5.
[17] Friédewald W, Levy R, Fredrickson D. Estimation of the concentration of low-density
lipoprotein cholesterol in plasma, without the use of the preparative centrifuge. Clin Chem. 1972;18:499-502.
[18] Ott L. An introduction to statistical methods and data analysis. 3rd ed. Boston, MA:
PWS-Kent Publishing Co.; 1988.
[19] Drasar B, Barrow P. Intestinal Microbiology. Washington, DC: American Society for Microbiology; 1985.
[20] Salyers AA, Vercellotti JR, West SE, Wilkins TD. Fermentation of mucin and plant polysaccharides by strains of Bacteroides from the human colon. Applied and environmental microbiology. 1977;33:319-22.
[21] Liu S, Ling Y, Tasi C. Biotechnically synthesized oligosaccharides and polydextrose reduce constipation and putrefactive metabolites in the human. J Chinese Nutr Soc (Taiwan). 1994;19:221-32.
[22] van Meer H, Boehm G, Stellaard F, Vriesema A, Knol J, Havinga R, et al. Prebiotic oligosaccharides and the enterohepatic circulation of bile salts in rats. Am J Physiol Gastrointest Liver Physiol. 2008;294:G540-7.
[23] Demigné C, Morand C, Levrat M, Besson C, Moundras C, Rémésy C. Effect of propionate on fatty acid and cholesterol synthesis and on acetate metabolism in isolated rat hepatocytes. . Br J Nutr 1995;74:209-19.
[24] Pereira D, Gibson G. Effects of consumption of probiotics and prebiotics on serum lipid levels in humans. Crit Rev Biochem Mol Biol. 2002;37:259-81.
Table 1. Seven-day cycle menu*
Day Menu
Day 1
Breakfast Rice porridge, shredded chicken, Chinese cabbage Lunch Rice/porridge , fried tofu, salted egg, Chinese spinach Snack Canned fruit cocktail
Dinner Fried chicken, chicken wing, corn, ham, cabbage Snack Milk/soy milk, brown rice powder
Day 2
Breakfast Rice porridge, shredded pork, bean sprouts
Lunch Rice/porridge, sweet potato leaves, pickles, Tofu, stir-fried pork with carrot
Snack Guava
Dinner Rice/porridge, bok choy, Chinese cabbage, steamed egg Snack Milk/soy milk, brown rice powder
Day 3
Breakfast Rice porridge, shredded pork, canned peanut gluten, squash Lunch Rice/porridge, stewed pork, bamboo shoot, Chinese spinach, fish
fillet, mushrooms Snack Banana
Dinner Rice/porridge, egg, chicken nuggets, bok choy, Chinese mushrooms Snack Milk/soy milk, brown rice powder
Day 4
Breakfast Rice porridge, shredded pork, pickles
Lunch Rice/porridge, roasted drumstick, bok choy, mushrooms Snack Apple
Dinner Rice/porridge, pan-fried milk fish, carrot, pork slice, bamboo shoots Snack Milk/soy milk, brown rice powder
Day 5
Breakfast Rice porridge, shredded pork, seaweed sauce
Lunch Stir-fried noodles with carrot, onion, pork, cabbage, mung bean soup Snack Watermelon
Dinner Meatball, imitation chicken (soy product), sunny egg, bok choy Snack Milk/soy milk, brown rice powder
Day 6
Breakfast Rice porridge, shredded pork, pickle, stewed peanut gluten Lunch Dumplings, vegetable soup
Snack Grapes
Dinner Rice/porridge, pan-fried meat fish, bean sprouts, carrot, sunny egg Snack Milk/soy milk, brown rice powder
Day 7
Breakfast Rice porridge, shredded pork, stewed tofu
Lunch Stir-fried noodles with carrot, onion, pork, shrimp, cabbage Snack Banana
Dinner Rice/porridge, stewed fish, ground pork, bean noodles, cucumber