C. Stephanidis (Ed.): Universal Access in HCI, Part IV, HCII 2011, LNCS 6768, pp. 448–457, 2011.
© Springer-Verlag Berlin Heidelberg 2011
The Relationships between Morphology and Work for the Nursing Performance of Hand Controls in
Emergency Surgery
Chao-Yuan Tseng and Fong-Gong Wu
Department of Industrial Design, National Cheng Kung University, Tainan, Taiwan {P38991034,fonggong}@mail.ncku.edu.tw
Abstract. Coming from the point of emergency room environment, this research studies the motion behavior, the control panel conformation, and the virtual operating movements of surgical nursing staff in the emergency room, in order to provide a reference for instrument design. The research began with professional interviews, followed by experiments on hand motion of surgical nursing staff in the emergency room. Test participants consist of surgical nursing staff from emergency rooms and the surgical department. A total of 20 participants, 10 females from each department were chosen to take the tests.
The research is divided into three categories. Results of this study presented a difference in operation height range between different control panel directions amongst emergency room and non-emergency room surgical nursing staff.
From the results we can see that participants with the same height do not necessary present the same wrist angles.
Keywords: emergency surgery, nursing, hand controller, motion analysis, virtual command.
1 Introduction
The Emergency Medical Services System in Taiwan, abbreviated EMSS, was found since 1989. From the results of the Average Daily Medical Services of Taiwan Hospitals – by Ownership, Department of Health, Executive Yuan, we can see that the daily average of emergency room patients in hospitals around Taiwan is close to 13,677 people. Li[19] in terms of emergency room facilities, close contacts are setup between the examination counter contact systems, such as telephones and intercoms, and the emergency vehicle, in order to be ready for varies emergency operations.
Armstrong[1] presented results that proved different hand postures causing different levels of injury; Kroemer[14] also claimed a varies hand motions that cause long-term injuries. Amongst which, long-term fatigue usually causes excessive work of hand muscles during facility operations, including excessive strain or contraction; long- term pressure around the hands can lead to Carpal Tullnel Syndrome (Armstrong[1]), Tendinitis or Tenosynovitis (Kroemer[14]). This research can be explained in the following aspects: (1) In terms of research procedures: a) Constructing static hand
testing data of emergency room surgical nursing staff and other related staff for the data base. b) Recognizing hand movement relationships during facility operation by emergency surgical nursing staff, further understand and analyze the relative hand relationship using motion analysis equipment. c) Understanding the distribution of hand operation movement groups of emergency room nursing staff. (2) In the aspect of future research and development: a) Constructing database for the static hand data of nursing staff in Taiwan. The procedures and methods of this research may be helpful to the prototype construction of hand data of nursing staff in Taiwan. b) Promoting local and independent medical equipment design.
Barnes, R. M.[2] mentioned that the range of wrist movement is roughly 80°~90°.
When the back is bent sideways, extensor carpi radialis longus muscles, brevis, and ulnaris muscle have a movement range of about 50°. During ulnar flexion, the ulnar muscle group effect creates a movement range of about 60°. During radialis flexion, the radialis muscle group effect creates a movement range of about 30°.
McCormick & Sanders[15] categorized the descriptions of movements during activities into the following categories: Positioning Movements, Continuous Movements, Manipulative Movements, Repetitive Movements, Sequentia1 Movements, and Static Adjustment. Hence, according to the hand movement features described by the above scholars, this research thoroughly examine the hand control conditions through observation. At this point, the research group categorizes the results of McCormick and Sanders, and Hsu, Sheng-Hsiung et al.[18] studies, and generalizes into Operation Motion Analysis of Emergency Surgical Nursing Staff, including movements of extension, pressing, rubbin, pinching, and twisting.
Sperling et al.[16] found in their research that the longer the operation time, the higher the probability of injury occurrence. Operating a tool in the same motion for more than 4 hours a day or 30 minutes continuously is likely to cause accumulative injury to the hands; while operating for less than an hour per day or 10 minutes continuously will reduce the chance of accumulative injuries. Also, according to the results of our observations, most of the controllers in the emergency surgical department consist of rotation and button controllers. Hence, it is vital to study and observe the relationship between hand operation motions and controller formations, and the effects on possible injuries caused by movements.
The adduction and abduction of shoulders should be under 45°, and angle of more than 90° should be avoided. Barnes, R. M.[2] claimed in his research, that hand movements can be categorized into five levels according to the hand movement range and energy consumption: level 1 includes finger movements; level 2 includes finger and wrist movements; level 3, 4, and 5 includes forearm, upper arm, and other body part movements consecutively. Categorizing emergency surgical nurses according to these levels, it is found that emergency surgical nurses fall into level 5, which is large movement range and energy consumptions. Being in this level also meant that other body parts are required to move on top of hand movements. Many other scholars and organizations have done similar controller appearance recognition studies, analyzing in detail the relationship between hand and human-machine interfaces.
2 Method
The entire experiment procedure will be carried out in the human engineering laboratory of our faculty, with the air of 3D motion analysis system to derive data. In the aspect of research investigation, the information regarding emergency surgical nursing members will be collected in two parts. The first being the professional interview; interviews are conducted with emergency surgical staff in major medical facilities around the Tainan area (Tainan, hospital, National Cheng Kung University hospital, Chi Mei medical center), to investigate the types of instruments and the possible instruments employed during emergency surgical situations. The second part being the hand movement experiment of emergency surgical nursing staff; the experiment instruments are chosen in respect of the instrument and control categories investigated in the first part of the information collection.
2.1 Participant Numbers
The participants were chosen to be 10 female emergency surgical nurses and 10 female non-emergency surgical nurses from the major medical facilities in the Tainan area. A total of 20 female nursing staff with no handicap in their hands and their right hands being the preferred hand will be participating in the experiment.
2.2 Record and Measurement Items
Principle independent variables: (1) Controller formations. (2) Body measurement values; randomly selected without any limitations. (Measurements include height, palm length and width, shoulder width, elbow height, and hand length). (3) Controlling directions (categorized by left, center, and right with a 45cm panel width).
(4) Actual and virtual controls. (5) Nursing staff categories (Emergency surgery and non-emergency surgery). (6) Relative height during instrument operation. Secondary independent variables include (1) Procedure related variable. Experiment procedures and steps are explained prior to the experiment; participants are given a chance to adapt to controller formations and heights; a one-minute practice is given to participants for each controller formations, plus a three-minute recess before the formal experiment. (2) Environment variable. In order to avoid other light sources affecting the image deriving, all lights in the laboratory were turned off and the window covered with black curtains during the experiment. Room temperature was maintained at around 25℃ in order to ensure the most comfortable experiment condition for the participants. (3) Participant related variable. a) Participants were chosen from female, right-handed emergency and non-emergency surgical nursing staff, able to endure 30 minutes of experiment process. b) Comfortable and dark colored clothing was required for the experiment (to avoid reflections caused by light colors, creating error in data deriving). Independent variables: (1) The diameter range of fingertips grabbing the controller. (2) The difference between operating angle and panel angle. (3) Operating height during virtual operations. (4) Wrist joint angles formed (flexion and extension angles).
2.3 Experiment Hypothesis
Hypothesis 1: The wrist joint angle when operating instruments standing (flexion angle) is dependent on the height and elbow height. This means when the hand comes in touch with the instrument under normal standing positions (fixed instrument height position), the taller the person is, the larger the wrist angle and vice versa.
Hypothesis 2: In the emergency and non-emergency surgical nursing staff operating under actual and virtual situations from three directions (left, central, right), the angles formed under virtual situations would appear to have bigger differences than angles formed under actual situations (panel angle of 66°).
Hypothesis 3: Under virtual operation situations, the relative hand height would be taller under actual operation situations.
2.4 Data Analysis Method
For the convenience of data analysis, hereby describe the joint angle calculation process. (1) The space dot product mode can be used to calculate the angle presented by the wrist and the control panel (Figure 1 ` Formula 1.) (2) The space between two points can be used to calculate the diameter between thumb and finger pinching the controller, in order to obtain the controller diameter of each emergency surgical nursing staff during actual and virtual controlling. (Figure 2 ` Formula 2) (3) To calculate the consistency between hand and panel angles during control, the included angle θ could be obtained by assuming finger control as the XY plane created by the experiment panel top. (Formula 3).
Fig. 1. Wrist angle calculation hypothesis
Assuming the space vector formed by P and Q are a、b respectively, then
cos a b
|a| |b| (1)
Actual control Virtual control
Fig. 2. Actual control and virtual control hypothesis
Assuming P(a1` b1 ` c1) ` Q(a2 ` b2` c2) then
PQ a a b b c c (2)
Assuming the included angle between the XY plane equation alX + b1Y + c1Z = d1
and the plane equation created by the thumb, middle finger, and the index finger a2X + b2Y + c2Z = d2 is θ, then
cos a a b b c c
a b c a b c (3)
3 Results
3.1 Static Measurements of Nursing Staff
Amongst the emergency surgical nursing staff, the average age was 31, average height was 159.1cm, the average elbow height was 99.1cm, the average hand length was 16.85cm, the average shoulder width was 35.84cm, the average palm width was 7.31cm, the average palm length was 9.66cm, and the average year of experience was 8.2 years. Amongst the non-surgical nursing staff, the average age was 26.7, average height was 161cm, the average elbow height was 100.48cm, the average hand length was 17.03cm, the average shoulder width was 35.95cm, the average palm width was 7.04cm, the average palm length was 9.6cm, and the average year of experience was 5.1 years.
3.2 Regression Analysis of Elbow and Wrist Joint Angle of Emergency and Non-emergency Surgical Nursing Staff during Operation from the Central Position
The R value represents the relationship between independent and dependent variables, and the descriptive relationship range between the two is as follow: 0~0.2 represents a low relationship, 0.2~0.5 represents a minimal relationship, 0.5~0.7 represents a sure relationship, while 0.7~1.0 represents a deep relationship. Hence, the R2 value of 0.414 shown in table 1 is within the range of a sure relationship. From Figure 5(a), we can see that the elbow height of between 102~108cm is closer to the range of the second regression linearity range, meaning that the wrist joint angle value (flexion) could be obtained for nursing staff with an elbow height within this range. Amongst the non-emergency surgical nursing staff, the value R2 shown in the figure is 0.516, which falls in the deep relationship range, representing a deep relationship between elbow heights and wrist joint angles. The ideal regression equation for non- emergency surgical nursing members shows that elbow heights of between 102cm and 104 cm obtains a bigger wrist joint angle (about 155°), while in reality, non- emergency surgical nurses presented bigger wrist joint angles when their elbow height is between 98 and 104 cm. However, from Figure 3(a), we can see that participants with elbow height of 98cm are outside of the confidence level.
Y = F1X2 + F2X + F3 (4) Amongst which, Y : wrist joint angle ; R2 :differentiation coefficient ; X : elbow
height (Table 1) / height(Table 2) ; F1, F2, F3 : regression coefficient.
Table 1. Emergency and non emergency nursing staff elbow height and wrist joint angle regression equation statistic summary chart
Regression equation R2 df F
Y = - 0.2702X2+56.7252X-2818.6 0.414 8 2.47
Y = - 0. 256X2+52.544X-2545.4 0.516 7 3.72
(a) (b)
Fig. 3. Elbow height and wrist joint angles during operation from the central position.
Second regression linearity chart (a) emergency surgical nursing staff (b) non emergency surgical nursing staff
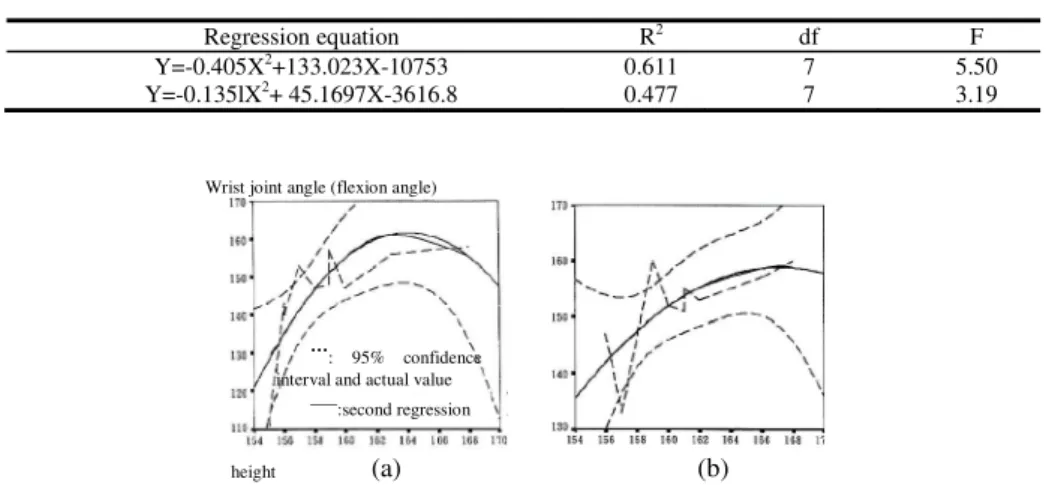
Table 2. Emergency and non emergency nursing staff height and wrist joint angle regression equation statistic summary chart
Regression equation R2 df F
Y=-0.405X2+133.023X-10753 0.611 7 5.50
Y=-0.135lX2+ 45.1697X-3616.8 0.477 7 3.19
(a) (b)
Fig. 4. Height and wrist joint angles during operation from the central position. Second regression linearity chart (a) emergency surgical nursing staff (b) non emergency surgical nursing staff.
Elbow height
Wrist joint angle (flexion angle)
…: reality value ___: second regression
Wrist joint angle (flexion angle)
height
…: 95% confidence interval and actual value
___:second regression
3.3 Regression Analysis of Height and Wrist Joint Angles for Emergency and Non-emergency Surgical Nursing Staff during Operation from the Central Direction
The differentiation coefficient R2 shown in Table 2 is 0.611, which falls in the deep relationship range. This means significant relationship is present between height and wrist joint angles. From Figure 4 (a) we can see that ideal second regression presents the largest wrist angle at participant height 164cm. Participants with height 164cm and above, on the contrary, shows a smaller wrist angle than 160°.
3.4 Variance Analysis of Actual and Virtual Operation on Controllers
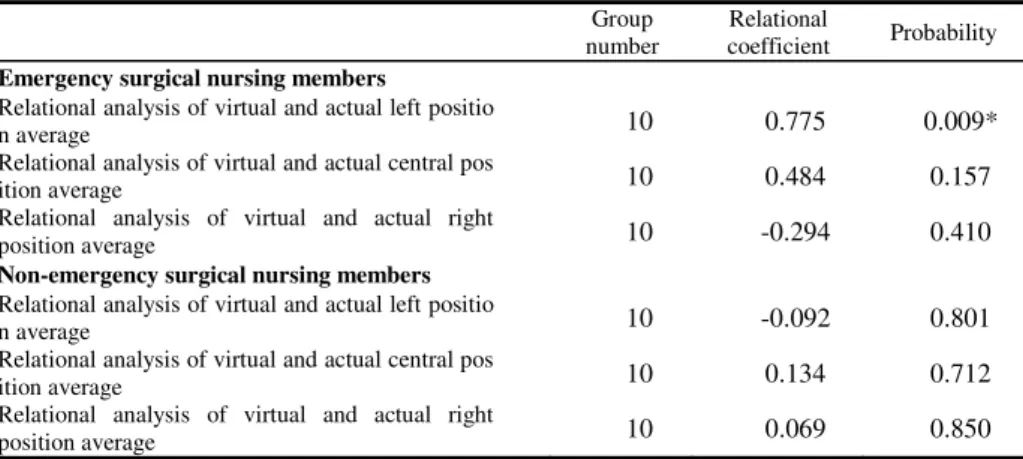
From Table 5 we can see that the correlation between actual and virtual operations in three different positions was significant (F=13.840, P<0.05). The results were also significant amongst participants (F=10.408, P<0.05). In the aspect of the correlation between actual and virtual operations with emergency and non-emergency surgical nursing members, the results were significant (F=19.775, P<0.05), however the chief effect amongst participants were insignificant.
Table 3. Comparison chart of virtual and actual operation relation analysis data (emergency / non-emergency surgical nursing members)
Group number
Relational
coefficient Probability Emergency surgical nursing members
Relational analysis of virtual and actual left positio
n average 10 0.775 0.009*
Relational analysis of virtual and actual central pos
ition average 10 0.484 0.157
Relational analysis of virtual and actual right
position average 10 -0.294 0.410
Non-emergency surgical nursing members Relational analysis of virtual and actual left positio
n average 10 -0.092 0.801
Relational analysis of virtual and actual central pos
ition average 10 0.134 0.712
Relational analysis of virtual and actual right
position average 10 0.069 0.850
3.5 Nursing Staff Operational Panel Height Analysis
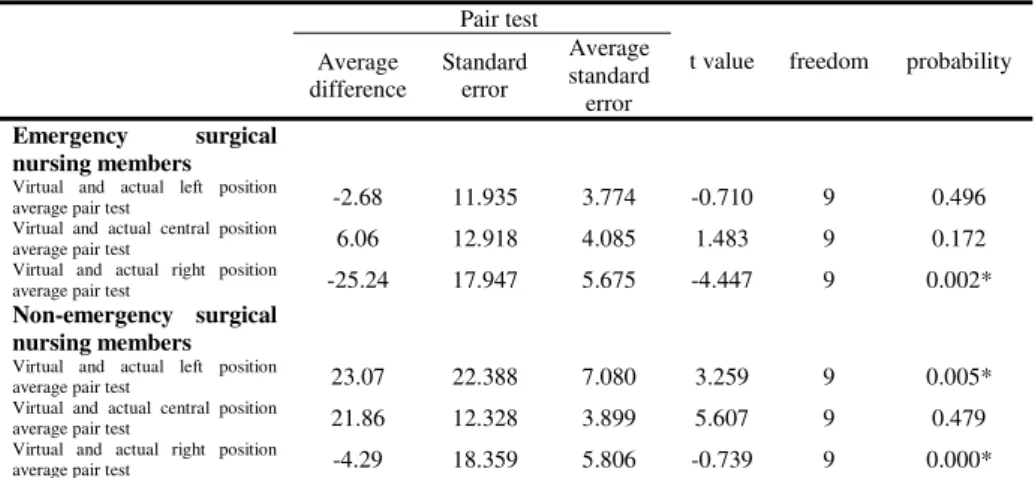
In the data of the emergency surgical nursing members, the actual operation height from the left position ranged from 92.97 to 95.64cm; height from the central position ranged from 92.1 to 98.72cm; height from the right position ranged from 91.62 to 99.14cm. The virtual operation height from the left position ranged from 94.19 to 96.92cm; height from the central position ranged from 93.84 to 97.78cm; height from the right position ranged from 89.73 to 94.6cm. While in the data of non-emergency surgical nursing members, the actual operation height from the left position ranged from 91.79 to 96.64cm; height from the central position ranged from 93.01 to 98.27cm; height from the right position ranged from 91.26 to 98.59cm. The virtual operation height from the left position ranged from 89.54 to 100.73cm; height from
the central position ranged from 89.21 to 94.89cm; height from the right position ranged from 92.97 to 95.64cm. From the above data, we can summarize the data and information into the following: amongst all the participants, the virtual button height ranged from 89.21 to 100.73cm. This means, in both emergency surgical and non- emergency surgical nursing staff groups, the objective control height range is larger than the present instrument height range of 92 to 95cm.
Table 4. Pair test comparison chart of actual and virtual operation controls (emergency / non- emergency surgical nursing staff)
Pair test
t value freedom probability Average
difference
Standard error
Average standard error Emergency surgical
nursing members
Virtual and actual left position
average pair test -2.68 11.935 3.774 -0.710 9 0.496
Virtual and actual central position
average pair test 6.06 12.918 4.085 1.483 9 0.172
Virtual and actual right position
average pair test -25.24 17.947 5.675 -4.447 9 0.002*
Non-emergency surgical nursing members
Virtual and actual left position
average pair test 23.07 22.388 7.080 3.259 9 0.005*
Virtual and actual central position
average pair test 21.86 12.328 3.899 5.607 9 0.479
Virtual and actual right position
average pair test -4.29 18.359 5.806 -0.739 9 0.000*
Table 5. Angle variance analysis chart for actual and virtual operations
ANOVAsa,b
Sum of Squares df Square Mean F Sig.
Angles Main Effects Between
participants 1573.386 4 393.347 2.338 0.060
Three-position
recognition 595.395 2 297.698 1.769 0.175
Actual and virtual
control recognition 540.601 1 540.601 3.213 0.076
Emergency surgical
recognition 437.390 1 437.390 2.599 0.110
2-Way Interactions
Amongst
participants 8756.464 5 1751.293 10.408 0.000*
Three-position recognition × actual and virtual control recognition
4557.483 2 2328.742 13.840 0.000*
Three-position × emergency surgical
recognition 771.500 2 385.750 2.292 0.105
Actual and virtual control recognition
×emergency surgical recognition
3327.480 1 3327.480 19.775 0.000*
Model 10329.9 9 1147.761 6.821 0.000*
Residual 18509.4 110 168.267 - -
Total 28839.2 119 242.346 - -
a. Angles by three-position recognition, actual and virtual control recognition, emergency surgical recognition b. *:P<0.05
4 Discussion
According to the results of this research, we can discuss the following: (1) When emergency surgical nurses operate buttons from the central direction, the range of wrist joint angles (dorsal flexion) range from 111° for participants that are 155cm tall and 158° for participants that are 168cm tall. As for non-emergency surgical nurses operation buttons from the central direction, the wrist joint angle ranges from 133° for 157cm tall participants and 160° for 168cm participants. We can see from the results that participants with the same heights do not necessary obtain the same wrist angles;
while the smallest 111° wrist angle sample does belong to the 95% confidence interval. The factor that caused this result could be due to the behavior differences produced by the operating habit of participants. (2) In the aspect of emergency surgical nurses operating actual and virtual buttons, the only movement formations that presented significant differences were the right-hand direction of virtual and actual control; no significant differences were found for the control from the central direction or the left-hand direction. This result shows that emergency surgical nurses adapt better to operating buttons from the central and the left directions. In the aspect of right-hand direction control, the virtual right-hand side difference has a great effect on operation angles. This tells us that buttons operated from the central direction is more acceptable for emergency surgical nurses. (3) In the aspect of non-emergency surgical nurses operating actual and virtual buttons, the most significant differences occurred in the movement formation of virtual and actual controls from the left and the center; while no significant differences were presented for the virtual and actual control from the right-hand direction. This shows that non-emergency surgical nurses adapt better to controls from the right-hand direction.
5 Conclusion
Due to the insufficiency of sample numbers, differences between the above experiment results and the hypothesis could not be avoided. During general dynamic experiments, the better setting for video data deriving is six or more cameras, meaning the larger the camera numbers the easier it is to obtain reactions from the reflection balls, hence the easier it is to be derived. As for the calculation of angles and the judgment of linear distance between two fingertips, the concept of space coordinates was employed. The formula for space vectors were transferred for the program, future studies should try to induce the concept of database into the program in order to obtain the complete data result for hand angle calculation and the relative value. The experiment process of this research is to stick reflection balls on the gloves; reflection balls may shift slightly during the operation process, resulting in error in the coordination derivation by the movement analysis system. Hence, suggestions are made to future researches of hand movement analysis, to consider sticking reflection balls directly on hands to avoid errors.
Acknowledgements. Our deepest appreciations to the emergency room staff of the Tainan Hospital and National Cheng Kung University Hospital for the staff arrangements for experiment participation.
References
1. Armstrong, T., Foulke, J., Joseph, B., Goldstein, S.: Investigation of cumulative trauma disorders in a poultry processing plant. AIHAJ 43(2), 103–116 (1982)
2. Barnes, R.M.: Motion and Time Study: Design and Measurement of Work, vol. 235, pp. 116–128, 366-389. John Wiley, New York (1980)
3. Barnes, R.M.: Motion and time study, 5th edn. Wiley, New York (1963)
4. Bobjer, O.: Screwdriver handle design for power and precision. In: Proceedings of the 1984, International Conference on Occupational Ergonomics, Human Factors Association of Canada, pp. 443–446 (1984)
5. Bradley, J.V.: Tactual coding of cylindrical knobs. Human Factors 9(5) (1967)
6. Chiu, H.Y., Su, F.C.: The motion analysis system and the maximal area of fingertip motion. Journal of Hand Surgery 21(B), 604–608 (1996)
7. Fleiss, J.L.: The design and analysis of clinical experiment. John Yiley & Sons, New York (1986)
8. Young, F.W.: Multidimensional Scaling-history, theory, and applications. L. Erlbaum Associates, Hilisdale (1987)
9. Green, P.E., Carmone Jr., F.J., Smith, S.M.: Multidimensional Scaling, concepts and applications. Allyn and Bacon, Massachusetts (1989)
10. Hunt, D.P.: The coding of aircraft controls, Tech. Rept, U. S. Air Force, Wright Air Development Center, pp. 53–221 (1953)
11. Jobson, J.D.: Applied Multivariate Data Analysis. Springer, Heidelberg (1992) 12. Hartigan, J.A.: Clustering algorithms. Wiley, New York (1975)
13. Kantowitz, B.H., Sorkin, R.D.: Human Factors, Understanding people-system relationship.
John Wiley & Sons, New York (1983)
14. Kroemer, K.H.E.: The state of ergonomic knowledge about cumulative trauma disorders. In:
Marras, Karwowski, Smith, Pacholski (eds.) The Ergonomics of Manual Work, pp. 19–24.
Taylor and Francis, London (1993)
15. McCormick, E.J., Sanders, M.S.: Human Factors in Engineering and Design, p. 181.
McGraw-Hill, New York (1982)
16. Sperling, L., et al.: A cube model for the classification of work with hand tools and the formulation of functional requirements. Applied Ergonomics 24(3), 212–220 (1993) 17. Shi, Y.-J.: Virtual Reality Technology. Computer and Communication 28, 3–15 (1994) 18. Hsu, S.-H., Shieh, K.-K., Yang, W.-D.: Classification of Hand Movements. Journa1 of the
Chinese Institute of Industrial Engineers 13(2), 145–155 (1996)
19. Li, C.-H.: Job characteristics of emergency department and process design of the basic equipment and staffing, department of design planning hospitals and clinics, pp. 114–119 (1988)
20. Lin, G.-M.: Emergency Nursing. Wey Far Books Co., Ltd, Taipei City (1993)