國立台灣大學醫學院暨工學院醫學工程研究所 博士論文
Graduate Institute of Biomedical Engineering College of Medicine and College of Engineering
National Taiwan University Doctoral Dissertation
肋膜疾病治療策略: 醫學工程的創新
The Therapeutic Strategies in the Pleural Diseases: Novelties from Biomedical Engineering
陳克誠 Ke-Cheng Chen
指導教授: 謝銘鈞 醫師 楊台鴻 教授
Advisors: Ming-Jium Shieh, M.D., Ph.D.
Tai-Horng Young, Ph.D.
中華民國 106 年 6 月
June, 2017
誌謝
就讀博士班的這七年(2010~2017),是人生迄今最難忘的時光。雖然路不 是平坦易行,終將笨鳥慢飛地抵達終點。最要感謝的,是指導老師謝銘鈞教授 以及楊台鴻教授,沒有你們,我不可能走到今天。此外,特別感謝長期指導我 的李章銘教授,他不但是我臨床和研究上的恩師,同時在生活以及待人接物 上,也是我急欲仿效的對象。此外,一路提攜我的賴鴻緒教授和陳晉興教授,
一直給我許多鼓勵,是我最終堅持下去的最大動力。要感謝的人真的太多,恕 我無法一一列名,但你們都是我一生最深刻的幸福記憶。最後,我要感謝我的 家人和好朋友們,因為你們無怨無悔地關心和保護著我,我才能這醫學這條道 路上,開心地繼續前進。
陳克誠 June, 2017
中文摘要
肋膜疾病,是臨床的一個重要挑戰。肋膜疾病,從良性的氣胸到惡性的肋膜 轉移以及惡性肋膜積水都屬之。原發型自發性氣胸通常發生於瘦、高、無過往 肺臟疾病之年輕男性。在絕大多數原發型自發性氣胸的病患,引起氣胸的原因 是在上肺葉的肺尖部,出現一個或數個氣泡。對於反覆發作之原發型自發性氣 胸之病患,以胸腔鏡手術切除漏氣的氣泡加上肋膜沾粘術是標準的手術方式。
近年來文獻上,開始有學者利用vicryl mesh 覆蓋在切除氣泡之縫合釘上。此法
可以蓋住切除之肺臟組織,促進肋膜沾粘,進一步減少術後氣胸復發機率。臺
大醫院以及長庚醫院進行多中心大規模臨床試驗NRPB 計畫已證實確實有效,
且術後追蹤情況良好,無重大併發症發生。初步結果可證實此構思是正確的,
但試驗迄今對於使用vicryl mesh 仍有疑慮。首先,以台灣現今醫療技術與醫材
開發之實力,要發展並改良出更好的產品並非難事;其次,vicryl mesh 並非原
發型自發性氣胸之相對應適應症產品(off-label use);更者,手術操作過程中發
現vicryl mesh 並不完全服貼於手術之部位,因此如能發展更適合原發型自發性
氣胸之相對應適應症劑型產品,對於病患之術後是更有助益。在我們的研究
中,我們證明我們自製的PCL membrane 在紐西蘭大白兔上面成功完成沾黏
術。此外,惡性肋膜轉移也是常見的癌症併發症。目前為止,並沒有一個好的 治療方法可以處理這樣的難題,而這種病人的平均存活時間,只有六到九個 月。因此,一種由光動力手術為主的治療方式逐漸被重視。光動力手術的優勢
在於這種治療方式可以清除掉肉眼看不見的癌細胞,進而延長病人的存活時 間。我們研究了過去十年在台大醫院之臨床經驗,我們發現到針對肺癌或胸腺
瘤併肋膜轉移的患者(M1a),光動力手術能夠提高三年以及五年存活率到 68.9%
以及57.4%。此外,和同時期沒有接受光動力、只接受傳統治療的肺癌族群做
比較,平均存活時間從17.6 個月,提高到 39.0 個月(
P=.047
)。成功證明了光動力手術確實對肋膜轉移的患者,有可行性,更有臨床上顯著的存活優勢。
關鍵字: 肋膜疾病;自發性氣胸;PCL高分子薄膜;肋膜沾黏術;惡性肋膜擴
散;光動力治療
Abstract
Pleural diseases, including benign or malignant conditions, are clinical challenges.
Benign one, like primary spontaneous pneumothorax, usually occurs in young, lean young men. In most cases, the cause of pneumothorax is rupture of blebs at apex of the lung. A novel method using coverage of the endoscopic suture line by a large absorbable vicryl mesh during thoracoscopic surgery was proved to be safe and feasible. Theoretically, the mesh can strengthen the suture line and induce local fibrosis surrounding the suture line, and reduce the rate of recurrent pneumothorax and prolonged air leakage. We investigate the Poly-ε-caprolactone (PCL) membrane pleurodesis by using New Zealand White rabbits, which was sacrificed for
examination one month later. Gross evaluation of pleurodesis score revealed that dense PCL membrane produced moderate pleural adhesion, while porous PCL membrane exhibited significantly higher pleurodesis scores. (P<0.05) Control group with thoracoscopic examination alone produced almost no pleurodesis (P<0.05). The porous PCL membrane produces more intensive adhesion than dense one. Western blot showed fibronectin expression was more evident in the porous PCL than dense one (P<0.05). Therefore, fibronectin plays an important role in the process of pleurodesis.
On the other hand, the malignant one, such as pleural spreading from cancer, is
even more difficult to treat. Monotherapy with surgery fails to have a better survival benefit than palliative chemotherapy, the currently accepted treatment. We
retrospectively reviewed the clinical characteristics and treatment outcomes of patients with lung cancer or thymoma with pleural seeding who underwent pleural photodynamic therapy (PDT) and surgery between 2005 and 2013. Eighteen patients enrolled in this study. The mean patient age was 52.9 ± 12.2 years. Lung cancer was the inciting cancer of pleural dissemination in 10 patients (55.6%), and thymoma in 8 (44.4%). There was no procedure-related mortality. Using Kaplan-Meier survival analysis, the 3-year survival rate and the 5-year survival rate were 68.9% and 57.4%, respectively. We compared the PDT lung cancer patients with those receiving
chemotherapy or target therapy (n=51) and found that the PDT group had better survival than non-PDT patients (mean survival time: 39.0 versus 17.6 months;
P=.047). With proper patient selection, radical surgical resection combined with
intrapleural photodynamic therapy for pleural spread in patients with non-small cell lung cancer or thymoma is feasible and may provide a survival benefit.
Keywords: pleural diseases; spontaneous pneumothorax; PCL membrane;
pleurodesis; malignant pleural spreading; photodynamic therapy
Table of Content
口試委員審定書...I
誌謝...II
中文摘要...III
Abstract...V
Part I. Benign: Study of Poly-ε-caprolactone (PCL) Membranes for Pleurodesis
Chapter 1. Introduction...1
Chapter 2. Materials and Methods...3
2.1 PCL membrane preparation………...3
2.2 Cell culture………...3
2.3 Hs68 cell proliferation on PCL membranes……….4
2.4 Immunocytochemistry………...4
2.5 Western blot analysis (in vitro) ...5
2.6 Western blot analysis (in vivo)………...6
2.7 Animal Subjects………....6
2.8 Pilot abdominal adhesion study in Rat……….7
2.9 General Design………...7
2.10 Surgical Techniques………7
2.11 Macroscopic Evaluation……….………9
2.12 Microscopic Evaluation………10
2.13 Statistical Analyses………...………10
Chapter 3. Results...11
3.1 PCL membrane morphology………...11
3.2 Fibroblast proliferation and fibronectin expression………....11
3.3 PCL membrane-induced adhesion in a rat abdominal model...12
3.4 PCL membrane-treated pleurodesis in a lapin thoracic model…...12
Chapter 4. Discussion...14
Part II. Malignant: Pleural Photodynamic Therapy and Surgery in Lung Cancer and Thymoma Patients with Pleural Spread Chapter 5. Introduction...17
Chapter 6. Materials and Methods...19
6.1 The eligibility criteria……….19
6.2 Operative procedure………...19
6.3 Photodynamic therapy………20
6.4 Statistical analysis………...21
Chapter 7. Results...22
7.1 The characteristics of the patients………...22
7.2 Short-term result……….22
7.3 Long-term result………..22
Chapter 8. Discussion...24
Chapter 9. Supplementary Data: Animal Model for Malignant Pleural Effusion...26
References...30
Figure legends...36
Figures...43
Tables………58
Publication list...64
Part I. Benign: Study of Poly-ε-caprolactone (PCL) Membranes for Pleurodesis
Chapter 1. Introduction
Recent advances in thoracoscopic surgery have made it a commonly used technique for treating spontaneous pneumothoraces and preventing recurrence [1–3]. The goal of
surgical treatment is to find the offending bleb, remove it, and do some manipulation to encourage pleural symphysis [4]. Blebs are generally removed or ligated under standardized procedures. Methods of thoracoscopic pleural symphysis have included mechanical abrasion and instillation of chemical irritants. Each method reduces the rate of pneumothorax recurrence to a certain degree [5–7], but the recurrence rates after thoracoscopic surgery are widely varied in the literature. Although several articles show significantly lower rates [8, 9], there are also articles demonstrating that the recurrence rates of pneumothorax after thoracoscopic surgery ranged between 5 and 12%, which are higher than the rates reported after open thoracotomy. It is suggested that a less intense pleural inflammatory reaction is induced by thoracoscopic procedure than by thoracotomy [10, 11]. Besides, post-pleurodesis severe pain and bleeding were encountered frequently. A potential alternative to increase the intensity of pleural inflammation and thereby prevent pneumothorax recurrence is film pleurodesis. Only
13], and the mechanism of film pleurodesis remains unclear.
Poly-ε-caprolactone (PCL) is a FDA-approved biomaterial with a slow degradation time of approximately 24 months when degraded by hydrolysis only [14-18]. Recently,
some investigators combined PCL with other biomaterials such as chitosan, polyethylene glycol, hyaluronic acid to produce anti-adhesion barrier for clinical applications [19]. However, only few studies report PCL only could provide anti- adhesion effect [20]. In contrast to common complications of postoperative abdominal
adhesions, adhesion (or pleurodesis) is an important therapeutic tool to control the incidence of recurrent pneumothorax. We suppose that if a biomaterial induces adhesion following abdominal surgery, perhaps it may be applied to pleurodesis tool for preventing recurrence of spontaneous pneumothorax. Thus, the first aim of this study is to investigate the efficacy of PCL membrane in reducing adhesion following abdominal surgery. If not, the second aim is to investigate whether PCL membrane can promote adhesion, testing the efficacy of pleurodesis to treat recurrent pneumothorax. We hypothesized that PCL membrane-induced pleurodesis can be achieved intrapleurally.
In the present study, rat and lapin models were used to test our hypothesis.
Chapter 2. Materials and Methods
2.1 PCL membrane preparation
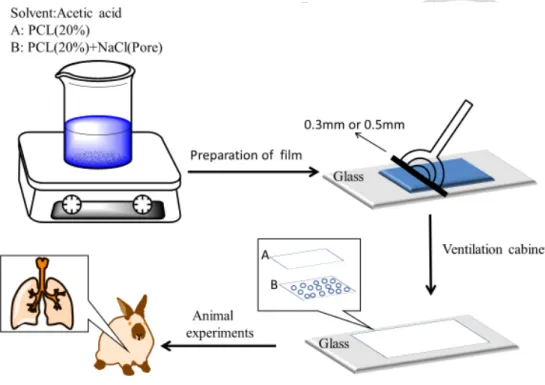
PCL (Sigma-Aldrich, USA) membranes were fabricated using solvent-casting method. Briefly, 20% PCL solution dissolved in acetic acid was cast on glass plate at room temperature, dried in the oven at 60°C overnight, immersed in the water, and neutralized by 0.5 N NaOH aqueous solution to obtain the dense membrane with a thickness of 200±50 µm. The porous PCL membrane was prepared by adding 8.8%
sodium chloride to the PCL solution. In this study, sodium chloride was used as the pore former to produce porous morphology with a thickness of 250±50 µm. Detailed membrane structure was examined using a scanning electron microscope (SEM) (Hitachi S-4800).
2.2 Cell culture
Human fibroblast Hs68 cells were purchased from Bioresource Collection and Research Center (BCRC, Taiwan). Cells were expanded in Dulbecco’s modified Eagle’s medium (DMEM) supplemented with 10% fetal bovine serum (FBS; Biological industries) and antibiotic/antimycotic (penicillin G sodium 100 U/ml, streptomycin 100 m g/ml, amphotericin B 0.25 m g/ml, Gibco-BRL Life Technologies, UK) at 37°C
in a humidified atmosphere containing 95% air and 5% CO2. Once 90% confluent, cells were trypsinized using 0.2% trypsin with 0.1% ethylenediaminetetraacetic acid (EDTA) (Sigma-Aldrich, USA) and re-suspended in the same medium until ready for experiments.
2.3 Hs68 cell proliferation on PCL membranes
The alamar blue assay was employed for proliferation estimation of Hs68 cells cultured on dense and porous PCL membranes. Circular samples (1.5cm in diameter) were cut from the PCL membranes, rinsed extensively with phosphate-buffered saline (PBS) and then placed in the 24-well tissue culture plate (Corning, USA). After ultraviolet light sterilization overnight, 2 x 104 cells were added to the well. On days 1, 4, and 7, alamar blue solution (AbD Serotec, UK) was added into culture well and incubated at 37ºC for 2 hours. The fluorescent intensity, correlated with the number of viable cells, was monitored using a spectrophotometer (Tecan, Taiwan) at the wavelengths of excitation and emission of 570 and 600 nm, respectively.
2.4 Immunocytochemistry
After 4 days of incubation, cells were washed with PBS, fixed in 4%
paraformaldehyde for 20 min and permeabilized with 0.1% triton X-100 for 10 min.
The cells were blocked in 2% bovine serum albumin overnight and stained by incubation with anti-fibronectin antibody (MAB1937, EMD Millipore, USA).
Fibronectin was then visualized using fluorescence-conjugated secondary anti-mouse IgG (Santa Cruz, USA). DAPI (Invitrogen) was used as the nuclear marker. Images were taken with a fluorescent microscope (Leica DMI 6000).
2.5 Western blot analysis (in vitro)
After 7 days of incubation, cells were lysed with a lysis buffer containing Complete Protease Inhibitor Cocktail Tablets (Roche Diagnostics GmbH, Germany) for 30 min on ice and then proteins were collected followed by centrifugation. The protein concentration in the supernatants was measured by a Bicinchoninic acid (BCA) protein quantification kit (Pierce Biotechnology, USA). Proteins were separated by Sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE) and then transferred onto nitrocellulose membranes. The membranes were immersed in the primary antibodies, anti-fibronectin & anti-Glyceraldehyde-3-Phosphate Dehydrogenase (GAPDH), overnight at 4°C. After washing several times, the membranes were immersed in the horseradish peroxidase-conjugated secondary antibodies for 2 h and visualized with an enhanced chemiluminescence detection system (Millipore, USA).
2.6 Western blot analysis (in vivo)
Pleurodesis induced by PCL mesh in pleural cavity of rabbit were harvested.
Protein from pleurodesis was extracted by Mammalian Protein Extraction Reagent (Pierce, Rockford, IL, USA). Equal amounts of protein were separated in SDS-PAGE gels and transferred to PVDF membrane. Then the membrane was incubated with primary antibodies against FNDC4 (fibronectin type III domain containing 4; Novus Biologicals, NBP1-59690) and β-Actin ( Novus Biologicals, NB600-501) overnight at 4 °C. After washing with TBST three times, the specific bands were detected by goat anti-rabbit IgG or goat anti-mouse IgG conjugated to horse radish peroxidase. The immune complexes were visualized with an enhanced chemiluminescent system (Western Lightning® Plus-ECL; PerkinElmer Inc.).
2.7 Animal Subjects
The protocol was approved by the Institution’s Committee on Investigations Involving Animal Subjects at National Taiwan University. All animals were housed in, and the procedures were performed at the facilities of National Taiwan University. The methods were carried out in accordance with the relevant guidelines, including any relevant details.
2.8 Pilot abdominal adhesion study in Rat
We use C57BL/6 rats for pilot study. The abdominal incision was made at midline.
The PCL membrane, 2 X 2 cm2, was inserted through the wound. The PCL membrane was well covering the intestine. We evaluate the adhesion degree ten days after the operation.
2.9 General Design
Thirty-six New Zealand White rabbits weighing 2.5-4.0 kg were randomized into three groups to undergo thoracoscopic procedures in the hemithorax as follows: (a) dense PCL membrane pleurodesis [dense PCL group (n=12)]; (b) porous membrane pleurodesis [porous PCL group (n=12)]; (c) control [control group (n=12)].
2.10 Surgical Techniques
Light general anesthesia was induced with intramuscular ketamine hydrochloride (Ketalar, 35 mg/kg; Pfizer, Shinchu, Taiwan) plus xylazine hydrochloride (Rompun®, 5 mg/kg, Bayer, Leverkusen, Germany). Arterial blood pressure and transcutaneous oxygen saturation were continuously monitored via percutaneous ear arterial catheter and pulse oximeter, respectively. ECG monitoring using standard limb leads was continuous. Penicillin G benzathine (40,000 U/kg IM) was administered
prophylactically. An antimicrobial skin preparation (povidone-iodine) was used prior to all invasive procedures, all performed with aseptic surgical techniques. A tracheostomy using a 3-mm endotracheal tube was made through a transverse incision between the third and fourth tracheal ring, with the tube advanced into the right main bronchus. The animals were ventilated (Servo 900 C, Siemens-Elema AB, Solna, Sweden) based on body weight and oxygen saturation, with a respiratory rate of 35–45 breaths/min, I:E ratio of 1:2, and inspiratory and expiratory pressures of 8–10 and 2 cm H2O, respectively.
Three 5-mm incisions were made in the chest overlying the sixth and eighth intercostal spaces for insertion of the telescope and instruments. Visual examination of the hemithorax was performed using a 5-mm, 30° rigid telescope (Karl Storz, Tuttlingen, Germany). After instillation of 2 mL 2% lidocaine hydrochloride (40 mg) into the pleural cavity, three types of thoracoscopic procedures were performed. Rabbits in the film group underwent thoracoscopic film placement at the parietal pleura. The upper half of the parietal surface, including areas above the 5th rib anteriorly and 7th rib posteriorly, was covered by the film. The incision was then sutured in layers. Animals in the control group underwent thoracoscopic examination of the pleural cavity only. At the conclusion of each thoracoscopic procedure, a chest tube made from sterile suction catheter (14 Fr; Symphon Chemical Corporation, Taipei, Taiwan) was inserted into the pleural space for aspiration of the retained air and fluid. After resumption of
spontaneous breathing, the endotracheal tube was removed and the tracheostomy incision closed using 6-O Prolene. The rabbits were then sent to the animal center for post-operative care.
2.11 Macroscopic Evaluation
The rabbits were euthanatized 30 days after the operation by injection of pentobarbital sodium (Nembutal; 120 mg/kg) into an ear vein. The thorax was removed from the remainder of the animal en bloc. Small incisions were made in the diaphragm to allow better access of the fixative (10% formalin) into the pleural cavities. Attempts were made to expand the lungs by injection of the fixative into a plastic catheter (6-mm- diameter) inserted into the exposed trachea. The entire thorax was then submerged in 10% formalin solution for 72 h. Necropsy and macroscopic evaluation were
performed blinded with respect to method. The degree of pleurodesis observed grossly was graded according to the following scheme: 0, normal pleural space; 1, no adhesions but pleural space inflamed as evidenced by redness and fibrin deposition; 2, a few scattered adhesions (25%); 3, generalized scattered adhesions (25-75%); and 4, complete obliteration of the pleural space by adhesions (75%) [21, 22].
2.12 Microscopic Evaluation
During the gross assessment of the thorax, samples of the parietal pleura, contiguous visceral pleura, and lung from each hemithorax were obtained from the areas of greatest adhesion and placed in neutral-buffered 10% formalin. If there were no adhesions, samples of the parietal pleura, contiguous visceral pleura, and lung were taken from the middle portion of the fourth intercostal space. These tissue samples were sent for routine histological examination and stained with hematoxylin-eosin.
The microscopic slices were evaluated blindly by two of the investigators (M.-S.H., K.-C.C.) for the presence of inflammation and fibrosis and graded on a five-point scale (0-4: absent, equivocal, mild, moderate, or marked, respectively) [21, 22].
2.13 Statistical Analyses
Categorical variables were compared using χ2 and Fisher’s exact tests and continuous variables, with Student’s t test. P values of less than 0.05 were regarded as significant.
Statistical analyses were performed using SPSS release 18 (SPSS Inc., Chicago, Ill), and all statistical tests were two-sided.
Chapter 3. Results
3.1 PCL membrane morphology
Dense and porous PCL membranes were prepared and compared in this study. Figure 1 shows dense PCL membrane without obvious pores under SEM examination, whereas micro-pores of porous PCL membrane due to the removal of dissolved salt could be seen with the naked eyes. Since these two membranes were identical except for their pore structure, the difference of tissue/cell response of PCL membranes in the subsequent results might be attributed to the membrane morphology, regulated by adding salt in the PCL solution during membrane formation.
3.2 Fibroblast proliferation and fibronectin expression
Hs68 fibroblast proliferation on dense and porous PCL membranes was evaluated by the application of alamar blue. Figure 2 shows cells proliferated gradually on both membranes with culture time. Compared to dense membrane, fibroblasts exhibited a slightly lower activity index on porous membrane, but there was no significant difference between them at every time points.
Figure 3 shows the staining of fibronectin was obviously enhanced on porous PCL membrane, indicating that more fibronectin was secreted by Hs68
fibroblasts when stimulated with porous structure. Western blot analysis further clarified this difference. Figure 4 shows fibroblasts cultured on porous PCL membrane exhibited higher expression of fibronectin than on dense one (p<0.05), suggesting the ability of porous PCL membrane structure could promote fibronectin secretion of fibroblasts.
3.3 PCL membrane-induced adhesion in a rat abdominal model
Figure 5 shows rats treated with the dense PCL membrane developed moderate adhesions to the sutured intestine after implantation for 20 days. However, animals with porous PCL membrane showed large and severe adhesions to the abdominal wall. According to adhesion severity from macroscopic observations, porous PCL membrane showed higher degree than dense one in the intra- abdominal adhesion. (2.33 vs 1.33)
3.4 PCL membrane-treated pleurodesis in a lapin thoracic model
Preparation of PCL film before the lapin experiments is illustrated as Figure 6.
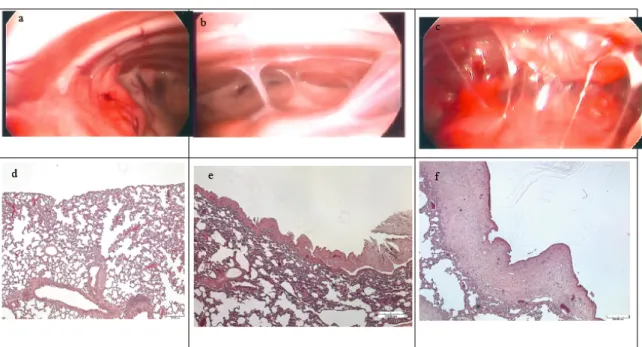
Representative images of the hemithorax after the various thoracoscopic procedures are presented in Figure 7. Gross evaluation of pleurodesis score (Table 1) revealed that dense PCL membrane produced moderate pleural adhesion, while porous PCL
membrane exhibited significantly higher pleurodesis scores. (P<0.05) Control group with thoracoscopic examination alone produced almost no pleurodesis (P<0.05).
The results of microscopic examination of the parietal and visceral pleura are shown in Figure 7 and Table 2. Both dense and porous PCL membranes induced significant inflammation and fibrosis in the parietal and visceral pleura when compared with the control group (P<0.05). Similarly, the highest scores of inflammation and fibrosis of the parietal and visceral pleura in this study was observed on the porous PCL membrane group.
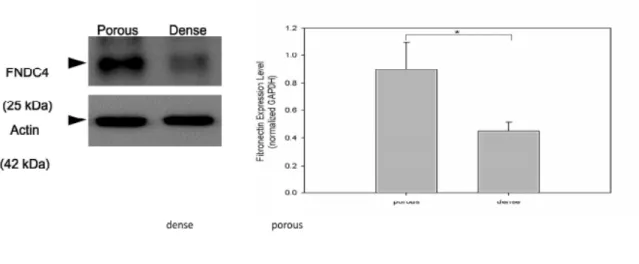
Finally, we evaluated the fibronectin expression in the adhesion band during pleurodesis induced by porous and dense PCL membrane. Western blot showed fibronectin expression was more evident in the porous PCL than dense one. Semi- quantification analysis showed that the difference was significant (P<0.05), as shown in Figure 8
We also performed PCL mesh pleurodesis in pig (Figure 9) and found that pleurodesis is achieved successfully in pig. The T peel test showed that the strength produced by pleurodesis is reliable and can prevent recurrence in primary spontaneous pneumothorax. (Figure 10 and 11)
Chapter 4. Discussion
More and more need for a better pleurodesis material is noted. In recent years, thoracoscopic pleurodesis gradually become the standard method for surgery of pneumothorax. The choice of thoracoscopic method should depend on the specific disease entity, as determined by the degree and extent of pleurodesis required to prevent recurrence. For example, when treating primary spontaneous pneumothorax with localized apical blebs, pleurodesis of the upper thoracic cavity prevents recurrence while preserves maximal pulmonary function. However, mechanical pleurodesis or apical pleurectomy may cause some complications, such as severe pain or bleeding.
[22-28]. Therefore, it is reasonable to design an appropriate membrane to cover lung bullae with inducing adhesion, but without mechanical stimulation and trauma, to treat pneumothorax.
In this study, we supposed that if a biomaterial could induce adhesion in other surgeries, it might be applied to pleurodesis treatment for preventing recurrence of
spontaneous pneumothorax. In the pilot abdominal study, we tested whether FDA- approved PCL without combining other biomaterials could provide adhesion or anti- adhesion effect following abdominal surgery. We found PCL membrane could not provide anti-adhesive effect in a rat abdominal model (Figure 5), which is not consistent
with previous finding [20]. In contrast, PCL membrane not only could induce postoperative abdominal adhesion, but also could enhance the effect by changing the membrane from dense to porous structure. The activity of fibroblast showed equality in
porous and dense PCL, but the fibronectin level is more prominent in porous PCL.
Hence, the pore size does influence the degree of adhesion. This appeared to suggest that PCL membrane might be an alternative in controlling the incidence of recurrent pneumothorax.
Rabbits were used to test whether PCL membrane-induced adhesion also could be achieved intrapleurally. We demonstrated that thoracoscopic PCL membrane was able to induce pleurodesis and, with ventilator support and meticulous monitoring, thoracoscopic membrane pleurodesis could be safely performed in rabbits, with the results comparable to those achieved using large animals. Further, we confirmed that PCL membrane caused significant effect of adhesion and the porous one could cause greater adhesion than dense one. The seal integrity was achieved in two ways. First, PCL membrane induced significant inflammation and thickening of the visceral pleural, which seal leaking holes in the visceral pleura, causing adhesion between the visceral and parietal pleura. The highest pleurodesis and pleural inflammation scores were observed in the porous PCL membrane group. Second, we thought the molecule
responsible to the adhesion effect is fibronectin.
Fibronectin has been known to play an important role during wound healing and tissue repair [35-38]. Fibronectin is synthesized by numerous cells, primarily fibroblasts [36]. In the literature, fibronectin is proved to be the agent of pleurodesis.
[39] Fibronectin is also important mediators in the pathogenesis of fibrotic diseases, especially pulmonary fibrosis. Fibronectin is chemotactic for fibroblasts and provides a scaffoldfor matrix deposition and fibroblast binding. [39] In our studies, we found that fibronectin plays an important role in the adhesion formation, both in the rat and lapin study.
In conclusion for part I, our study showed that PCL membrane induced significant degree of adhesion, both in abdomen and chest. The porous PCL membrane produces more intensive adhesion than dense one. Fibronectin plays an important role in the process of adhesion. Further study is required for the clinical application of the promising material.
Part II. Malignant: Pleural Photodynamic Therapy and Surgery in Lung Cancer and Thymoma Patients with Pleural Spread
Chapter 5. Introduction
Pleural spread without distant metastases in thoracic malignancy is difficult to manage. In non-small cell lung cancer (NSCLC), it was stage IIIb in the previous International System for Staging Lung Cancer [40]. The International Association for the Study of Lung Cancer (IASLC) published the seventh edition of the TNM classification of NSCLC in 2009 and changed the sixth edition of this document. The current IASLC lung cancer staging project committee recommended that pleural spreads, either malignant pleural effusions or pleural nodules, be upgraded from T4 to M1a. In patients with pleural carcinomatosis, the median survival time ranged from 6 to 9 months [41–47]. Currently, the management options for pleural spread include chemotherapy, surgery with pleurectomy, and photodynamic therapy. Thymoma is neoplasm arising from epithelial thymic cells. Distant metastasis is rare but it more frequently shows pleural implantation upon diagnosis or after primary treatment.
Thymoma with pleural spread is a difficult clinical situation to manage, and the treatment is controversial [38-50].
sensitive compounds that are exposed selectively to light, whereupon they become toxic to targeted malignant and other diseased cells. PDT anticancer effect occurs when the photosensitizer captures light energy and transfers that energy to oxygen. The excited oxygen species are important for the effect and can cause direct cell destruction, damage of the tumor vessels, or both [49]. In our study, we used Porfimer sodium (Photofrin;
Axcan Pharma Inc, Birmingham, AL, USA), a first-generation photosensitizer. 630 nm red light can activate the photosensitizer. Successful treatment of malignant mesothelioma by photodynamic therapy has been reported as a new approach for pleural malignancy dissemination [51]. Moreover, like mesothelioma, PDT could be one of the multimodality treatment for NSCLC with pleural disseminations. A phase II trial for pleural spread, patients underwent surgery with complete resection or tumor debulking, followed by intrapleural PDT or PDT alone. The overall survival was significantly better than similar patients of historical controls [52].
However, the efficacy of PDT therapy when compared with a control group located at the same institute is unknown. Moreover, the usefulness of PDT as a treatment for thymoma with pleural spread is also unknown. Therefore, we analyzed clinical outcomes in patients who underwent PDT for pleural spread due to lung cancer or thymoma at our institute during an 8-year period.
Chapter 6. Materials and Methods
6.1 The eligibility criteria
Patients with pathologic diagnosis of lung cancer or thymoma with pleural spread, medical feasibility for operation between 2005 to 2013. The exclusion criteria are as follows: younger than 18 years old, leukopenia, or thrombocytopenia; chronic renal insufficiency with serum creatinine > 2.5 mg/dL; significantly impaired liver function;
pregnancy or lactation.
Besides history taking and physical examination, preoperative evaluation included the chest CT, pulmonary function test, and laboratory examination. Moreover, the abdomen, pelvis and brain CT and bone scan were performed to identify distant metastasis. The participants provide their written informed consent to participate in this study. The Research Ethics Committee of National Taiwan University Hospital approved this study.
6.2 Operative procedure
Thoracotomy was performed on all patients by attending chest surgeons. The criteria for choosing a particular pulmonary resection were the same as those used for performing curative resections in patients with early lung cancer. Patients underwent anatomic resections in whom it was possible to remove all gross tumor. After finishing the procedure, the parietal pleura were stripped from the bony hemithorax as radical
parietal pleurectomy. Debulking of all gross tumor was performed in the mediastinum, too. For thymoma patients, the radical thymothymectomy was performed concurrent with radical pleural pleurectomy. The goal was to remove all detectable tumor in the operation field before proceeding to the photodynamic therapy [53].
6.3 Photodynamic therapy
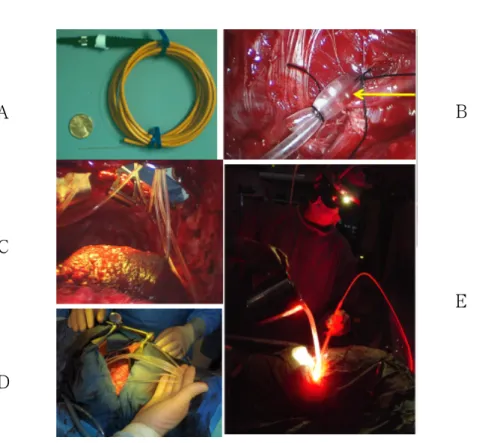
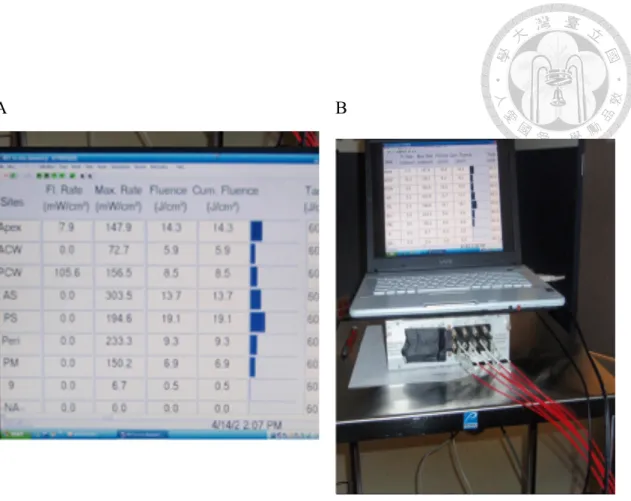
We sew flat photodiodes into seven regions of the hemothorax: the apex, anterior chest wall, posterior chest wall, posterior costophrenic sulcus, anterior costophrenic sulcus, posterior mediastinum and pericardium. Both the real-time luminescence and the cumulative PDT dose for each region were provided by a dosimetry system. After sewing the photodiodes, dilute intralipid solution (0.01%) was used as scattering agent, giving more homogeneous light therapy. We delivered the light with an optical fiber sheathed within an endotracheal tube. Besides, the balloon cuff was filled with intralipid solution (0.1%). We move around this device in the hemithorax until a light dose of 40 J/cm2 was reached at all regions. During the light delivery portion of the procedure, we remove the chest retractors to avoid shielding. We use about 20 L of intralipid solution to maintain a clear intrathoracic area and minimize light absorption by hemoglobin. After completion of light administration, the sterile photodiodes were all removed. The intrapleural PDT took about 1 hour. Dr. Steve Hahn at University of Pennsylvania School of Medicine kindly provided the dosimetry system [52]. During
the same period of time, 51 NSCLC patients with pleural spread were undergoing traditional chemotherapy, radiotherapy or target therapy as a control group.
6.4 Statistical analysis
The primary outcome assessed in this study was survival. Categorical variables were compared using χ2 or Fisher’s exact tests, and continuous variables were evaluated using Student’s t test. P values of less than 0.05 were regarded as significant. Statistical analyses were performed using SPSS release 18 (SPSS Inc., Chicago, Ill), and all statistical tests were two-sided.
Chapter 7. Results
7.1 The characteristics of the patients
There were 10 women and 8 men in the study (Table 3). The mean patient age was 52.9 ± 12.2 years. The inciting cancer of pleural dissemination was lung cancer in 10 patients (55.6%) and thymoma in 8 (44.4%) patients.
7.2 Short-term result
The average hospital stay was 13.5 ± 4.4 days. The average duration of the operation was 305.1 ± 63.3 minutes. There was no procedure-related mortality. There was post-operative ARDS complication in one of our PDT patients. She is a 57-year- old lady who had lung adenocarcinoma with pleural spread. She underwent concurrent chemoradiotherapy before PDT and surgery. The ARDS occurred immediately after the procedure. After medical treatment, the condition gradually improved. Other minor complications included prolonged air-leakage (one patient) and skin redness (two patients). The complications were successfully treated using medication.
7.3 Long-term result
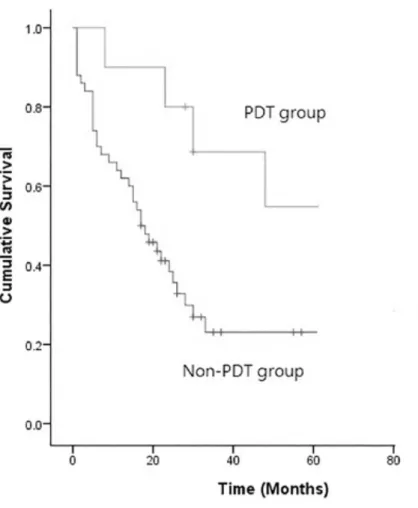
The average follow up time was 38.1 months. Using Kaplan-Meier survival analysis, the 3-year survival rate and 5-year survival rate were 68.9% and 57.4%, respectively. Six out of 10 NSCLC patients treated with PDT died, while one had a local recurrence and one had a distant metastasis. One out of 8 thymoma patients treated
with PDT died due to tumor progression by distant metastasis 32 months after initial treatment, one had a local recurrence and 2 had distant metastases. When compared with lung cancer patients treated with chemotherapy, target therapy or radiotherapy without surgical resection and PDT, the survival difference was significant (P= 0.047) (Figure 12). The neoadjuvant and adjuvant treatment profile for the two groups of lung cancer patients with pleural spread is listed in Table 4. Seven patients died during the follow-up period. One patient died due to pneumonia and the other deaths were cancer- related. Regarding the cancer-related failure pattern (n=6), one was a local recurrence and the other 5 were distant metastases. The schematic pictures shown in PDT in Figure 13 and 14
.
Chapter 8. Discussion
The pleural spread of thoracic malignancy is difficult to manage. It is usually treated with palliative chemotherapy but is barely cured. Because residual invisible tumor remains in the pleural space after what seems to be a curative resection, surgery alone has been of little benefit in treating cancer with pleural spread [41-47]. Several potential advantages was offered by PDT in treating thoracic malignancy. First, specified targeting tumor caused by a greater retention of photosensitizers in cancer cell compared with normal cell was demonstrated by preclinical studies [54]. Second, only several millimeters into tissue was penetrated by visible light. It results in superficial cell killing, while saving the underlying tissues, letting PDT suitable in the treatment of cancers with superficial spreading, like pleura dissemination [55, 56]. Moreover, it is a localized treatment which can be performed after primary resection. It is used as part of the multimodal treatment for patients with pleural spread. Our hypothesis was that, upon complete resection of all gross disease, immediate irradiation may improve survival by additional control of the residual microscopic tumor. For lung cancer, the phase II trial at the University of Pennsylvania proved our point of view. It showed 73.3% of half-year localized disease control for the PDT group and a median overall survival of 21.7 months, which is significantly prolonged compared with those for patients (6-9 months) treated with the non-operative standard of care and based upon
historical controls [52]. The median overall survival of our lung cancer patients was 39.0 months. Compared with surgery without PDT for patients of lung cancer with pleural spread in literature, the outcome of patients receiving surgery plus PDT is better [57, 58]. The comparison of these results is listed in Table 5. The mean survival time (17.6 months) of the non-PDT patients in our cohort was comparable with previously reported survival (mean 6~9 months) [41-47]. Our outcome is better than has been previously reported, and the difference may be due to a number of factors, such as genetic background, patient population, and a different phase of treatment, as well as more choices of multi-disciplinary of treatment including chemotherapy, target therapy and radiotherapy. Furthermore, the optimal treatment for thymoma with pleural spreading is even more controversial [50, 59]. Murakawa reported 13 cases of thymoma with pleural spread treated by surgical resection including the visible pleural nodules, 9 of them (69%) suffered from pleural recurrence after surgery [60]. A previous study showed that chemotherapy with extrapleural pneumonectomy might be a way to cure this disease; however, pneumonectomy carries a high risk and high complication rate [50]. A better local control of the disease (88%) in our thymoma patients may be associated with PDT treatment. Therefore, PDT may be a beneficial alternative for the treatment of thymoma patients with pleural spread on diagnosis.
Pleural spread represents a clinical challenge due to extensive metastasis of the
tumors. The results of this analysis are promising. With proper patient selection, surgery with intralpleural PDT for pleural spread in patients with lung cancer or thymoma is feasible and might improve survival.
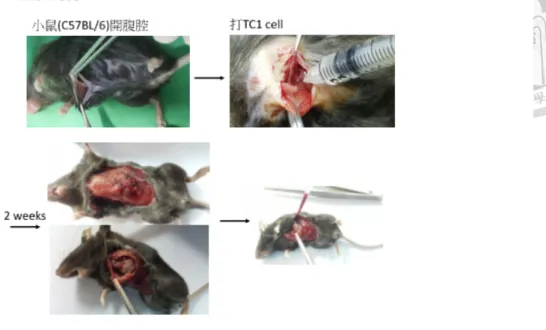
Chapter 9. Supplementary Data: Animal Model for Malignant Pleural Effusion
Malignant pleural effusions resulting from lung cancer define stage IV disease and unresectability. In addition, metastatic pleural disease from other cancers is associated with serious morbidity and mortality consequences. Despite the importance of primary and secondary pleural malignancies, progress in treatment advances has been limited in part by lack of suitable moderate-sized (3 to 4 kg) pleural cancer animal models for research. The pleural space is a large and complex anatomic region within the thorax adjacent to vital structures; the anatomy of the pleural space presents substantial access and dosimetry challenges for cancer diagnostics as well as therapeutics. Moderate-sized, immunocompetent animal models of pleural malignancy are needed to address these issues because the pleural space of these animals can accommodate instruments designed for human use in pediatric care. Compared with mice and rats, New Zealand white rabbits that weigh 3 to 4 kg have a pleural space that is more analogous to that found in humans. This similarity makes the model more practical for studying
diagnostic techniques and emerging therapies. We try to develop a consistent, reproducible model of pleural carcinoma in moderate-sized (3 to 4 kg) immunocompetent rabbits. This model likely will be useful in developing diagnostic and treatment methodologies, such as high-resolution thoracoscopic optical technologies, surgical procedures, and therapeutics, such as photodynamic therapy, that cannot be investigated sufficiently in existing smaller animal models. In previous study, we investigate cancer cell culture model in rats for malignant pleural effusion (FIGURE 15). In the current study, we setup the malignant pleural effusion in New Zealand rabbit and preparation of the cisplatin-loaded PCL gel.
Materials and Methods
The protocol was approved by the Institution’s Committee on Investigations Involving Animal Subjects at National Taiwan University. All animals will be housed in, and the procedures will be performed at the facilities of National Taiwan
University. The methods will be carried out in accordance with the relevant guidelines, including any relevant details.
Animal preparation: pathogen-free New Zealand white rabbits will be used in this study. The animals will be anesthetized with a 2:1 ratio of ketamine HCl (100 mg/ml;
Ketaset, Fort Dodge Animal Health, Fort Dodge, IA) and xylazine (20 mg/ml;
After injection, a 23-gauge, 1-in. catheter will be placed in a marginal ear vein for administration of IV anesthesia. The depth of anesthesia will be evaluated by monitoring the physical reflexes of the animal (no voluntary head, limb, or eye movements) and pulse rate. Maintenance anesthetic dosed at 0.3 ml of a 1:1 mixture of ketamine and xylazine (ketamine, 100 mg/ml; xylazine, 20 mg/ ml) will be administered accordingly. A dose of analgesic (0.1 to 0.5 mg/kg SC; Torbutrol, Torbugesia-SA, Fort Dodge Animal Health, Fort Dodge, IA) will be given prior to intubation. The animals will be intubated with a 3.0 French cuffed endotracheal tube.
Animals undergoing surgical implantation of tumor will be prepared for surgery.
Cell line: This study uses VX2 tumors, which are classified as carcinomas and which were derived initially in 1940. These tumors are considered to be a wholly anaplastic carcinoma whose keratinocytes never keratinize. VX2 tumor cells grow rapidly in allogenic adult recipients and frequently metastasize to the lungs. They are known for rapid growth and can be transplanted serially. These tumor cells can also be propagated in the thigh muscle. The tumor used in this study will be of rabbit origin and will be isolated from rabbit skin warts produced by the Shope cottontail rabbit papillomavirus. Tumors will be excised from lung tissue, placed in a small amount of warm (37 °C) DMEM containing 10% fetal bovine serum (GIBCO cell culture, Invitrogen, Carlsbad, CA), and cut into approximately 1-mm pieces. Surplus tumor
tissue will be stored by suspension in DMEM containing 10% DMSO and freezing at –80°. Thirty-six New Zealand White rabbits with malignant pleural effusion weighing 2.5-4.0 kg will be randomized into three groups to undergo procedures in the
hemithorax as follows: (a) PCL gel [PCL gel group (n=12)]; (b) cisplatin-loaded PCL gel [cisplatin-loaded PCL gel group (n=12)]; (c) control [control group (n=12)]. This study uses VX2 tumors, which are classified as carcinomas and which were derived initially in 1940. These tumors are a wholly anaplastic carcinoma whose keratinocytes never keratinize. VX2 tumor cells grow rapidly in allogenic adult recipients and frequently metastasize to the lungs. They are known for rapid growth and can be transplanted serially. These tumor cells can also be propagated in the thigh muscle.
The tumor used in this study is of rabbit origin and isolated from rabbit skin warts produced by the Shope cottontail rabbit papillomavirus. Tumors is excised from lung tissue, placed in a small amount of warm (37 °C) DMEM containing 10% fetal bovine serum (GIBCO cell culture, Invitrogen, Carlsbad, CA), and cut into approximately 1- mm pieces. Surplus tumor tissue is stored by suspension in DMEM containing 10%
DMSO and freezing at –80°. The desired number of cells then are injected into the pleura space of New Zealand white rabbits. After one month, the VX2 tumor causes pleural tumor spreading with malignant pleural effusion. (Figure 16)
References
1. Mouroux J, Elkaim D, Padovani B, et al. Video-assisted thoracoscopic treatment of spontaneous pneumothorax: Technique and results of one hundred cases. J Thorac Cardiovasc Surg 1996; 112:385.
2. Chen JS, Hsu HH, Kuo SW, et al. Needlescopic versus conventional video-assisted thoracic surgery for primary spontaneous pneumothorax: A comparative study. Ann Thorac Surg 2003; 75:1080.
3. Baumann MH, Strange C, Heffner JE, et al. Management of spontaneous pneumothorax: An American College of Chest Physicians Delphi consensus statement. Chest 2001; 119:590.
4. Fry WA, Paape K. Pneumothorax. In: Shields TW, LoCicero J, Ponn RB, Eds.
General thoracic surgery, 5th ed. Philadelphia, PA: Lippincott Williams and Wilkins, 2000:675–686.
5. Inderbitzi RG, Leiser A, Furrer M, et al. Three years’ experience in video-assisted thoracic surgery (VATS) for spontaneous pneumothorax. J Thorac Cardiovasc Surg 1994; 107:1410.
6. Massard G, Thomas P, Wihlm JM. Minimally invasive management for first and recurrent pneumothorax. Ann Thorac Surg 1998; 66:592.
7. Sahn SA, Heffner JE. Spontaneous pneumothorax. N Engl J Med 2000; 342:868.
8. Sawada S, Watanabe Y, Moriyama S. Video-assisted thoracoscopic surgery for primary spontaneous pneumothorax: Evaluation of indications and long-term outcome compared with conservative treatment and open thoracotomy. Chest 2005;127: 2226.
9. Gebhard FT, Becker HP, Gerngross H, et al. Reduced inflammatory response in minimally invasive surgery of pneumothorax. Arch Surg 1996;131:1079.
10. Chen JS, Hsu HH, Chen RJ, et al. Additional minocycline pleurodesis after thoracoscopic surgery for primary spontaneous pneumothorax. Am J Respir Crit Care Med 2006; 173:548.
11. Cardillo G, Carleo F, Giunti R, et al. Videothoracoscopic talc poudrage in primary spontaneous pneumothorax: A single institution experience in 861 cases. J Thorac Cardiovasc Surg 2006; 131:322.
12. Seokkee Lee, MD, Seong Yong Park, MD, Mi Kyung Bae, MD, et al. Efficacy of Polyglycolic Acid Sheet After Thoracoscopic Bullectomy for Spontaneous Pneumothorax. Ann Thorac Surg 2013; 95:1919–23
13. Hidetaka Uramoto and Fumihiro Tanaka1. What is an appropriate material to use with a covering technique to prevent the recurrence of spontaneous pneumothorax?
Journal of Cardiothoracic Surgery 2014, 9:74
14. P. Diemer,1 S. Markoew,1 D. Q. S. Le,2 N. Qvist3. Poly-ε-caprolactone film as a
scaffold for in vivo tissue engineering in rabbit esophagus. Diseases of the Esophagus.
2015 Apr;28(3):240-5
15. Yang S, Leong K F, Du Z, Chua C K. The design of scaffolds for use in tissue engineering. Part I. Traditional factors. Tissue Eng 2001; 7: 679–89.
16. Hakkarainen M, Albertsson A C. Heterogeneous biodegradation of polycaprolactone – low molecular weight products and surface changes. Macromol Chem Phys 2002; 203: 1357–63.
17. Gann Z, Liang Q, Zhang J, Jing X. Enzymatic degradation of poly (E-caprolactone) film in phosphate buffer solution containing lipases. Polym Degrad Staby 1996; 56:
209–13.
18. Anderson J M, Rodriguez A, Chang D T. Foreign body reaction to biomaterials.
Semin Immunol 2008; 20: 86–100.
19. SH Chen, CH Chen, YT Fong, JP Chen. Prevention of peritendinous adhesions with electrospun chitosan-grafted polycaprolactone nanofibrous membranes. Acta Biomaterialia. 2014 Dec;10(12):4971-82.
20. Hsien-Yi Lo, Hsuan-Ting Kuo, Yi-You Huang, Application of Polycaprolactone as an Anti-Adhesion Biomaterial Film, Artificial Organs 2010; 34: 648-653.
21. Lardinois D, Vogt P, Yang L, et al. Non-steroidal antiinflammatory drugs decrease the quality of pleurodesis after mechanical pleural abrasion. Eur J Cardiothorac Surg
2004;25: 865.
22. Chen JS, Hsu HH, Kuo SW, et al. Effects of additional minocycline pleurodesis after thoracoscopic procedures for primary spontaneous pneumothorax. Chest 2004;
125:50.
23. Hatz RA, Kaps MF, Meimarakis G, et al. Long-term results after video-assisted thoracoscopic surgery for first-time and recurrent spontaneous pneumothorax. Ann Thorac Surg 2000;70: 253.
24. Chan P, Clarke P, Daniel FJ, et al. Efficacy study of videoassisted thoracoscopic surgery pleurodesis for spontaneous pneumothorax. Ann Thorac Surg 2001; 71:452.
25. Loubani M, Lynch V. Video assisted thoracoscopic bullectomy and acromycin pleurodesis: an effective treatment for spontaneous pneumothorax. Respir Med 2000;
94:888.
26. Yim AP, Liu HP. Video assisted thoracoscopic management of primary spontaneous pneumothorax. Surg Laparosc Endosc 1997; 7:236.
27. Cardillo G, Facciolo F, Giunti R, et al. Videothoracoscopic treatment of primary spontaneous pneumothorax: A 6-year experience. Ann Thorac Surg 2000; 69:357.
28. Hatta T, Tsubota N, Yoshimura M, et al. Intrapleural minocycline for postoperative air leakage and control of malignant pleural effusion. Kyobu Geka 1990; 43:283.
29. Park SN, Jang HJ, Choi YS, et al. Preparation and characterization of
biodegradable anti-adhesive membrane for peritoneal wound healing. J Mater Sci Mater Med. 2007 Mar;18(3):475-82.
30. A synthetic bioabsorbable sheet may prevent postoperative intrapleural adhesions following thoracotomy: a canine model. Hamaji M, Kojima F, Komatsu T, Tsuruyama T, Date H, Nakamura T. Interact Cardiovasc Thorac Surg. 2014 Dec;19(6):914-20.
31. Prevention of desiccation induced postsurgical adhesion by thermosensitive micelles. Zhang W, Wu Q, Li L, Cui T, Sun L, Wang N, Liu L, Li X, Gong C. Colloids Surf B Biointerfaces. 2014 Oct 1; 122:309-15. doi: 10.1016/j.colsurfb.2014.06.023.
Epub 2014 Jun 14.
32. Prevention of intra-abdominal adhesion by bi-layer electrospun membrane. Jiang S, Wang W, Yan H, Fan C. Int J Mol Sci. 2013 Jun 4;14(6):11861-70. doi:
10.3390/ijms140611861.
33. Effects on bone union and prevention of tendon adhesion by new porous anti- adhesive poly L-lactide-co-ε-caprolactone membrane in a rabbit model. Sato T, Shimizu H, Beppu M, Takagi M. Hand Surg. 2013;18(1):1-10.
34. Encapsulation of cell-adhesive RGD peptides into a polymeric physical hydrogel to prevent postoperative tissue adhesion. Zhang Z, Ni J, Chen L, Yu L, Xu J, Ding J.
J Biomed Mater Res B Appl Biomater. 2012 Aug;100(6):1599-609. doi:
10.1002/jbm.b.32728. Epub 2012 Jun 12.
35. ST Wing, SM Kim. Plasma and cellular fibronectin: distinct and independent functions during tissue repair, Fibrogenesis & Tissue Repair 2011, 4:21
36. Mao Y, Schwarzbauer JE: Fibronectin fibrillogenesis, a cell-mediated matrix assembly process. Matrix Biol 2005, 24:389-399
37. K Lewandowska, HU Choi, LC Rosenberg, et al. Fibronectin-mediated Adhesion of Fibroblasts: Inhibition by Dermatan Sulfate Proteoglycan and Evidence for a Cryptic Glycosaminoglycan-binding Domain. J Cell Biol. 1987 Sep;105(3):1443-54.
38. Ahmed, S.A., R.M. Gogal, Jr., and J.E. Walsh, A new rapid and simple non- radioactive assay to monitor and determine the proliferation of lymphocytes: an alternative to [3H] thymidine incorporation assay. J Immunol Methods, 1994. 170(2):
p. 211-24.
39. Lee YC, Malkerneker D, Devin CJ, et al. Comparing transforming growth factor beta-2 and fibronectin as pleurodesing agents. Respirology. 2001 Dec;6(4):281-6.
40. Mountain CF. Revisions in the international system for staging lung cancer. Chest.
1997; 111(6): 1710-1717.
41. Werner-Wasik M, Scott C, Cox JD, Sause WT, Byhardt RW, Asbell S. et al.
Recursive partitioning analysis of 1999 Radiation Therapy Oncology Group (RTOG) patients with locally advanced non-small-cell lung cancer (LANSCLC):
Identification of five groups with different survival. Int J Radiat Oncol Biol Phys.
2000; 48(5): 1475-1482.
42. Martini N, Bains MS, Beattie EJ Jr. Indications for pleurectomy in malignant effusion. Cancer. 1975; 35(3): 734-738.
43. Reyes L, Parvez Z, Regal AM, Takita H. Neoadjuvant chemotherapy and operations in the treatment of lung cancer with pleural effusion. J Thorac Cardiovasc Surg. 1991; 101(5): 946-947.
44. Mott FE, Sharma N, Ashley P. Malignant pleural effusion in non-small cell lung cancer--time for a stage revision? Chest. 2001; 119(1): 317-318.
45. Rami-Porta R, Ball D, Crowley J, Giroux DJ, Jett J, Travis WD, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the T descriptors in the forthcoming (seventh) edition of the TNM classification for lung cancer. J Thorac Oncol. 2007; 2(7): 593-602.
46. Postmus PE, Brambilla E, Chansky K, Crowley J, Goldstraw P, Patz EF Jr, et al.
The IASLC Lung Cancer Staging Project: proposals for revision of the M descriptors in the forthcoming (seventh) edition of the TNM classification of lung cancer. J Thorac Oncol. 2007; 2(8): 686-693.
47. Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, et al.
The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of
malignant tumours. J Thorac Oncol. 2007; 2(8): 706-714.
48. Lucchi M, Davini F, Ricciardi R, Duranti L, Boldrini L, Palmiero G, et al.
Management of pleural recurrence after curative resection of thymoma. J Thorac Cardiovasc Surg. 2009; 137(5): 1185-1189.
49. Yu L, Jing Y, Ma S, Li F, Zhang YF. Cytoreductive surgery combined with hyperthermic intrapleural chemotherapy to treat thymoma or thymic carcinoma with pleural dissemination. Onco Targets Ther. 2013; 6: 517-521.
50. Ishikawa Y, Matsuguma H, Nakahara R, Suzuki H, Ui A, Kondo T, et al.
Multimodality therapy for patients with invasive thymoma disseminated into the pleural cavity: the potential role of extrapleural pneumonectomy. Ann Thorac Surg.
2009; 88(3): 952-957.
51. Friedberg JS, Culligan MJ, Mick R, Stevenson J, Hahn SM, Sterman D, et al.
Radical pleurectomy and intraoperative photodynamic therapy for malignant pleural mesothelioma. Ann Thorac Surg. 2012; 93(5): 1658-1665.
52. Friedberg JS, Mick R, Stevenson JP, Zhu T, Busch TM, Shin D, et al. Phase II trial of pleural photodynamic therapy and surgery for patients with non-small-cell lung cancer with pleural spread. J Clin Oncol. 2004; 22(11): 2192-2201.
53. Liu TJ, Lin MW, Hsieh MS, Kao MW, Chen KC, Chang CC, et al. Video-assisted thoracoscopic surgical thymectomy to treat early thymoma: a comparison with the
conventional transsternal approach. Ann Surg Oncol. 2014; 21(1): 322-328.
54. Gomer CJ, Dougherty TJ. Determination of [3H]- and [14C] hematoporphyrin derivative distribution in malignant and normal tissue. Cancer Res. 1979; 39(1): 146- 151.
55. Dougherty TJ, Gomer CJ, Henderson BW, Jori G, Kessel D, Korbelik M, et al.
Photodynamic therapy. J Natl Cancer Inst. 1998; 90(12): 889-905.
56. Hahn S, Glatstein E. The emergence of photodynamic therapy as a major modality in cancer treatment. Rev Contemp Pharmocother. 1999; 10: 69-74.
57. Wang BY, Wu YC, Hung JJ, Hsu PK, Hsieh CC, Huang CS, et al. Prognosis of non-small-cell lung cancer with unexpected pleural spread at thoracotomy. J Surg Res.
2011; 169(1): e1-e5.
58. Mordant P, Arame A, Foucault C, Dujon A, Le Pimpec Barthes F, Riquet M.
Surgery for metastatic pleural extension of non-small-cell lung cancer. Eur J of Cardiothorac Surg. 2011; 40(6): 1444-1449.
59. Ichinose Y, Ohta M, Yano T, Yokoyama H, Asoh H, Hata K. Treatment of invasive thymoma with pleural dissemination. J Surg Oncol. 1993; 54(3): 180-183.
60. Murakawa T, Karasaki T, Kitano K, Nagayama K, Nitadori J, Anraku M, et al.
Invasive thymoma disseminated into the pleural cavity: mid-term results of surgical resection. Eur J Cardiothorac Surg. 2015; 47(3): 567-72.
61. Kreuter KA1, El-Abbadi N, Shbeeb A, Tseng L, Mahon SB, Narula N, Burney T, Colt H, Brenner M. Development of a rabbit pleural cancer model by
using VX2 tumors. Comp Med. 2008 Jun;58(3):287-93.
Figure legends
FIGURE 1. (a) Dense PCL membrane without obvious pores under SEM
examination, whereas micro-pores of porous PCL membrane (b) due to the removal of dissolved salt could be seen with the naked eye.
FIGURE 2. Cell Density: 10^4/cm2, n=6. Cells proliferate gradually on both
membranes with culture time. Compared to dense membrane, fibroblasts exhibited a slightly lower activity index on porous membrane, but there was no significant difference between them at every time points.
FIGURE 3. The staining of fibronectin was obviously enhanced on porous PCL membrane, indicating that more fibronectin was secreted by Hs68 fibroblasts when stimulated with porous structure.
FIGURE 4. Fibroblasts cultured on porous PCL membrane exhibited higher
expression of fibronectin than on dense one (p<0.05), indicating the ability of porous PCL membrane structure to promote fibronectin secretion of fibroblasts.
FIGURE 5. (a) dense PCL, (b) porous PCL in the abdomen: There is much more intestinal adhesion was noted in (b) porous PCL compared with (a) dense one. (c) The macroscopic scoring showed that the adhesion was greater in porous PCL than dense one. (2.33 vs 1.33)
FIGURE 6. Preparation of PCL film before the animal experiments
FIGURE 7. (A, B, C) The hemithorax 30 days after various thoracoscopic pleurodesis procedure. (D, E, F) The corresponding microscopic view of the pleura 30 days after mesh pleurodesis. Scale bar: 250 µm.
FIGURE 8. Western blot and semi-quantification study showed that porous PCL produce more fibronectin than dense one (p<0.05).
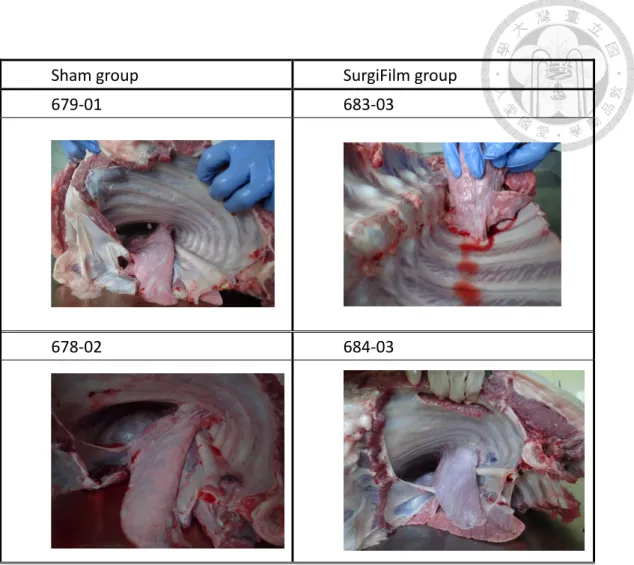
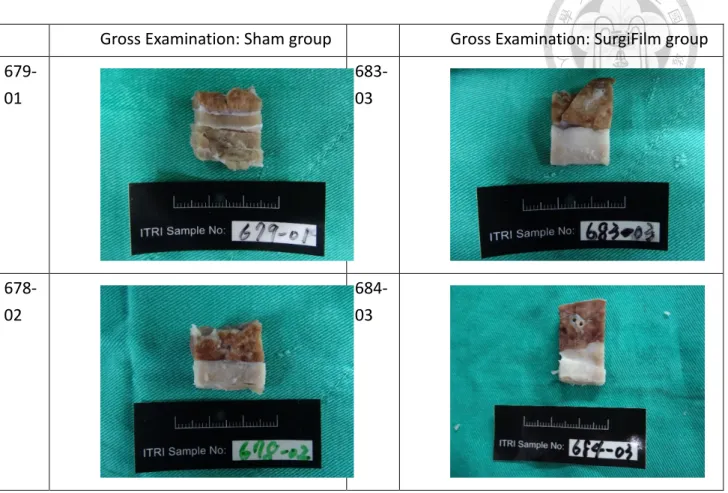
FIGURE 9. Pleurodesis study in pig. Compared Sham group with SugriFilm group, we found the pleurodesis is stronger and create more adhesion in SurgiFilm group.
FIGURE 10. Gross examination showed SurgiFilm group creates more and stronger adhesion, compared with Sham group.
FIGURE 11. T-peel test study for pleurodesis: SurgiFilm group > Sham group
FIGURE 12. Kaplan-Meier survival analysis of the patients undergoing PDT vs. non- PDT for pleural spread (P= 0.047)
FIGURE 13. The schematic views of pleural PDT
FIGURE 14. A) and B) The dosimetry system. The PDT dose was guided by the probe placed in the seven regions.
FIGURE 15. Cell culture model in rats for malignant pleural effusion
FIGURE 16. A) New Zealand rabbit undergoing single port non-intubated VX2 tumor implantation. B) One month later, significant amount of malignant pleural effusion with cancer spreading was noted. An anaplastic carcinoma derived from rabbit (VX2) showed the potent to cause pleural spreading and malignant pleural effusion.
Figures
FIGURE 6. Preparation of PCL film before the animal experiments
FIGURE 7. (A, B, C)The hemithorax 30 days after various thoracoscopic pleurodesis procedure. (D, E, F) The
corresponding microscopic view of the pleura 30 days after mesh pleurodesis. Scale bar: 250 µm.
FIGURE 8. Western blot and semi-quantification study showed that porous PCL produce more fibronectin than
dense one (p<0.05).
FIGURE 9. Pleurodesis study in pig. Compared Sham group with SugriFilm group, we found the pleurodesis is
stronger and create more adhesion in SurgiFilm group.
Sham group SurgiFilm group
679-01 683-03
678-02 684-03
FIGURE 10. Gross examination showed SurgiFilm group creates more and stronger adhesion, compared with Sham group.
Gross Examination: Sham group Gross Examination: SurgiFilm group 679-
01
683- 03
678-
02
684- 03
FIGURE 11. T-peel test study for pleurodesis: SurgiFilm group > Sham group 0
2 4 6 8 10
SurgiFilm Sham
Peel Force (N)
T peel Test
(porcine sacrified 3 Months)
FIGURE 12. Kaplan-Meier survival analysis of the patients undergoing PDT v.s. non-PDT for pleural spread (p
= .047)
FIGURE 13. The schematic views of pleural PDT. The probes were placed in the seven regions intra-pleurally by suture ligation. The dose was guided by the dosimetry system which illustrated in the Figure 15. A) The light cord of laser, B&C) The receptors of dosimetry are sutured to the seven regions of parietal pleura, D) Thoracotomy is performed in every patient, E) Intralipid was added in the pleural space to make the laser light more homogeneous.
D A
C
E B
A B
Figure 14. A) and B) The dosimetry system. The PDT dose was guided by the probe placed in the seven regions.
FIGURE 15. Cell culture model in rats for malignant pleural effusion
A B
FIGURE 16. A) New Zealand rabbit undergoing single port non-intubated VX2 tumor implantation. B) One month later, significant amount of malignant pleural effusion with cancer spreading was noted. An anaplastic carcinoma derived from rabbit (VX2) showed the potent to cause pleural spreading and malignant pleural effusion.
Tables
Table 1. Macroscopic Examination of Pleural Cavities after Pleurodesis
Method Score
Dense PCL (n=12) 2.7 ± 0.4 Porous PCL (n=12) 3.3 ± 0.6#
Control (n=12) 0.3 ± 0.2*
*P<0.05 when compared with PCL mesh or porous PCL mesh
#P<0.05 when compared PCL mesh with porous PCL mesh
Table 2. Microscopic Examination of Pleural Cavities after Pleurodesis
Method Parietal pleura inflammation
score
Visceral pleura inflammation
score
Parietal pleura fibrosis
score
Visceral pleura fibrosis score Dense PCL mesh
(n=12)
2.6±0.5 2.7±0.8 2.9±0.5 3.0±0.7 Porous PCL mesh
(n=12)
3.1±0.4* 3.4±0.6* 3.2±0.5
*
3.5±0.6*
Control (n=12) 0.2±0.4*
*
0.2±0.4** 0.3±0.2
**
0.2±0.1**
*P<0.05 when compared porousn PCL mesh with PCL mesh
**P<0.05 when compared control with others
Table 3. Characteristics, treatment course and outcome of the patients
No Age/Sex Diagnosis Surgical Treatment death Time (months) 1 51/F lung cancer
with pleural seeding
Lobectomy with pleural PDT 1 62
2 57/F
lung cancer with malignant
PE, s/p CT
LLL lobectomy, PDT 0 84
3 33/F
Thymic cancer with pleural seeding s/p CT
Parietal pleurectomy and RML wedge resection + Pleural tumor excision and
PDT
0 66
4 34/F
lung ca with pleural seeding
LUL lobectomy, PDT 0 80
5 57/F
Lung cancer with pleural seeding , s/p CT
Lobectomy, PDT 1 8
6 34/M
Lung ca with pleural seeding
s/p CT
Lobectomy, pleural PDT 1 48
7 48/F
Lung ca with pleural seeding s/p CCRT target
therapy
LLL wedge resection, pleural PDT
1 23
8 53/F RML, RLL, lung ca, pleural
Bilobectomy, pleural PDT 1 30