科技部補助專題研究計畫成果報告 期末報告
以家庭為中心之概念的縱貫性研究:探討接受人工生殖技術 治療夫妻之產後憂鬱(第二年)
計 畫 類 別 : 個別型計畫
計 畫 編 號 : NSC 102-2410-H-040-002-
執 行 期 間 : 102 年 08 月 01 日至 103 年 07 月 31 日 執 行 單 位 : 中山醫學大學護理學系(所)
計 畫 主 持 人 : 李淑杏
共 同 主 持 人 : 李茂盛、蕭秋月、李孟智
計畫參與人員: 碩士班研究生-兼任助理人員:林秀儀
處 理 方 式 :
1.公開資訊:本計畫涉及專利或其他智慧財產權,2 年後可公開查詢 2.「本研究」是否已有嚴重損及公共利益之發現:否
3.「本報告」是否建議提供政府單位施政參考:否
中 華 民 國 103 年 10 月 27 日
中 文 摘 要 : 目的:本兩年期研究計畫目的在於以家庭為中心概念探討接 受人工生殖技術治療夫妻之產後憂鬱,並以縱貫性研究了解 夫妻個體及整個家庭產後憂鬱變化且分析其預測因子。
方法:研究設計採縱貫式研究法(Longitudinal study design),以郵寄問卷方式分別於夫妻產後第 1 個月、第 6 個月及 1 年進行調查。於中部某生殖技術治療中心及某醫學 中心同步進行收案。收案生殖技術受孕夫妻 116 對,完成問 卷回收者共 94 對,回收率為 81%;自然受孕夫妻 119 對夫 妻,完成問卷回收者共 105 對,回收率 88%。問卷內容含夫 妻基本資料、愛丁堡產後憂鬱量表、自尊量表、社會支持量 表及簡式親職壓力量表。
結果:愛丁堡產後憂鬱量表以≧10 分為切點,生殖技術受孕 組妻與自然受孕組妻於產後 1 個月、6 個月及 1 年之憂鬱傾 向百分比分別為 46.2% vs. 47.6%、36.9% vs. 45%、45
% vs. 48.9%,二者未達統計顯著差異。生殖技術受孕組夫 與自然受孕組夫於產後 1 個月、6 個月及 1 年之憂鬱傾向百 分比分別為 26.9% vs. 23.1%、27.4% vs. 26%、20%
vs. 22.1%,二者未達統計顯著差異。
以 GEE 分析影響妻與夫長期產後憂鬱的預測因子,影響 妻憂鬱程度長期變化的相關因子為家庭經濟狀況(負相關;
OR=0.680)、夫憂鬱程度(OR=1.266)、妻自尊程度(負相關;
OR=0.903)、妻親職壓力程度(OR=1.049)等四個變項。影響夫 憂鬱程度長期變化的相關因子為夫教育程度(正相關;
OR=1.909)、妻憂鬱程度(正相關;OR=1.247)、妻自尊程度 (正相關;OR=1.025)、夫自尊程度(負相關;OR=0.904)、夫 親職壓力程度(正相關;OR=1.050)等五個變項。夫妻長期產 後憂鬱的預期因子與是否為生殖技術治療(組別)無關。
應用:生殖技術受孕妻與夫產後憂鬱傾向高盛行率值得重 視,所得結果瞭解影響夫妻憂鬱程度長期變化的預測因子,
此部分可作為臨床或社區以家庭為中心照護介入之依據。
中文關鍵詞: 人工生殖技術、不孕夫妻、家庭為中心、產後憂鬱
英 文 摘 要 : Purpose:With the family-centered concept, the study aims at investigating the distribution and predictors of PPD among previously infertile couple through a longitudinal study. In the 2-year project, the couples will be followed up 1 month, 6 month, and 1 year after their deliveries, using couples of natural birth as the control group.
Method:116 couples in study group and 119 couples in
control group during 1 month after their deliveries were recruited. After approval by IRB, the study subjects were interviewed by a mailing questionnaire.
There was a total of 94(81%) and 105(82%) of study group and control group, respectively, responded to this survey. The self-administer questionnaire is composed of subjects' profiles, Edinburgh postpartum depression scale, self-esteem questionnaire, Brief parenting stress questionnaire and social support questionnaire.
Result: Using the cutoff point of ≧10 scores for Edinburgh postpartum depression scale, the
differences in the prevalence of depression tendency 1 month, 6 months and 1 year after birth between wives of ART and non-ART respectively, were 46.2%
vs. 47.6%, 36.9% vs. 45% and 45% vs. 48.9%, which were all not reached a statistically
significant level. On the other hand, the differences were 26.9% vs. 23.1%, 27.4% vs. 26% and 20% vs.
22.1% for husbands of ART and non-ART, which were all not reached a statistically significant level, either.
Using generalized estimating equation(GEE)to find out the predictors for the change of postpartum depression over time, it's showed that economic condition of family, depression status of the
husband, self-esteem of the wife and stress status on parenting of the wife were significant predictors for the wives' postpartum depression over time.
Educational level of the husband, depression status of the wife, self-esteem of the wife, self-esteem of the husband and stress status on parenting of the husband were significant predictors for the
husbands' postpartum depression over time. Whether or not receiving ART was not a significant predictor for both wives' and husbands' postpartum
depression.
Application:There is a high prevalence of postpartum depression among previously infertile couples, and understanding of predictors postpartum depression is the key for effective family-centered intervention prevent or solve the problem.
英文關鍵詞: Assisted Reproductive Technology (ART), infertile couple, family-centered, postpartum depression
科技部補助專題研究計畫成果報告
(□期中進度報告/■期末報告)
計畫名稱:以家庭為中心的縱貫性研究概念:探討接受人工生殖技術 治療夫妻之產後憂鬱(第二年)
計畫類別:■個別型計畫 □整合型計畫 計畫編號:MOST 102-2410-H -040-002-
執行期間: 102 年 8 月 1 日至 103 年 7 月 31 日 執行機構及系所:中山醫學大學 護理學系
計畫主持人:李淑杏教授
共同主持人:李茂盛教授、李孟智教授、蕭秋月副教授 計畫參與人員:林秀儀碩士生、王瓊儀、楊雯如大學生
本計畫除繳交成果報告外,另含下列出國報告,共 0 份:
□執行國際合作與移地研究心得報告
□出席國際學術會議心得報告
期末報告處理方式:
1. 公開方式:
□非列管計畫亦不具下列情形,立即公開查詢
■涉及專利或其他智慧財產權,□一年□二年後可公開查詢 2.「本研究」是否已有嚴重損及公共利益之發現:■否 □是
3.「本報告」是否建議提供政府單位施政參考 ■否 □是, (請列舉提供 之單位;本部不經審議,依勾選逕予轉送)
中 華 民 國 103 年 10 月 27 日
科技部補助專題研究計畫成果報告自評表
請就研究內容與原計畫相符程度、達成預期目標情況、研究成果之學術或應用價 值(簡要敘述成果所代表之意義、價值、影響或進一步發展之可能性) 、是否適 合在學術期刊發表或申請專利、主要發現(簡要敘述成果是否有嚴重損及公共利 益之發現)或其他有關價值等,作一綜合評估。
1. 請就研究內容與原計畫相符程度、達成預期目標情況作一綜合評估 ■ 達成目標
□ 未達成目標(請說明,以 100 字為限)
□ 實驗失敗
□ 因故實驗中斷
□ 其他原因 說明:
2. 研究成果在學術期刊發表或申請專利等情形:
論文:□已發表 ■未發表之文稿 □撰寫中 □無 專利:□已獲得 □申請中 □無
技轉:□已技轉 □洽談中 □無
其他: (以 100 字為限)
3. 請依學術成就、技術創新、社會影響等方面,評估研究成果之學術或應用價 值(簡要敘述成果所代表之意義、價值、影響或進一步發展之可能性) ,如已 有嚴重損及公共利益之發現,請簡述可能損及之相關程度(以 500 字為限)
(1) 愛丁堡產後憂鬱量表以≧10 分為切點,比較二組憂鬱傾向之分佈與差異。
生殖技術受孕組妻與自然受孕組妻於產後 1 個月、6 個月及 1 年之憂鬱傾 向百分比分別為 46.2% vs. 47.6%、36.9% vs. 45%、45% vs. 48.9%,二 者未達統計顯著差異。生殖技術受孕組夫與自然受孕組夫於產後 1 個月、
6 個月及 1 年之憂鬱傾向百分比分別為 26.9% vs. 23.1%、27.4% vs. 26
%、20% vs. 22.1%,二者未達統計顯著差異。產後憂鬱傾向盛行率結果 與自然受孕組雖無統計差異,然整體來說妻與夫之憂鬱傾向盛行率偏高,
因此產後家庭之身心健康情形需特別重視,針對此議題應研擬介入方案以 協助產後家庭。
(2) 以 GEE 分析影響妻與夫長期產後憂鬱的預測因子,影響妻憂鬱程度長期變 化 的 相 關 因 子 為 家 庭 經 濟 狀 況 ( 負 相 關 ; OR=0.680) 、 夫 憂 鬱 程 度 (OR=1.266)、妻自尊程度(負相關;OR=0.903)、妻親職壓力程度(OR=1.049) 等四個變項。影響夫憂鬱程度長期變化的相關因子為夫教育程度(正相關;
OR=1.909) 、 妻 憂鬱 程 度 (正 相 關 ;OR=1.247) 、 妻 自尊 程 度 (正 相 關 ; OR=1.025)、夫自尊程度(負相關;OR=0.904)、夫親職壓力程度(正相關;
OR=1.050)等五個變項。上述結果顯示產後家庭妻與夫長期產後憂鬱乃互為
影響,印證本研究之家庭理論架構,因此未來應研擬以家庭為中心的介入
措施提供產後夫妻合適的照護內容。
中文摘要
目的:本兩年期研究計畫目的在於以家庭為中心概念探討接受人工生殖技術治療 夫妻之產後憂鬱,並以縱貫性研究了解夫妻個體及整個家庭產後憂鬱變化且分析 其預測因子。
方法:研究設計採縱貫式研究法(Longitudinal study design),以郵寄問卷方式分 別於夫妻產後第 1 個月、第 6 個月及 1 年進行調查。於中部某生殖技術治療中心 及某醫學中心同步進行收案。收案生殖技術受孕夫妻 116 對,完成問卷回收者共 94 對,回收率為 81%;自然受孕夫妻 119 對夫妻,完成問卷回收者共 105 對,
回收率 88%。問卷內容含夫妻基本資料、愛丁堡產後憂鬱量表、自尊量表、社 會支持量表及簡式親職壓力量表。
結果:愛丁堡產後憂鬱量表以≧10 分為切點,生殖技術受孕組妻與自然受孕組 妻於產後 1 個月、6 個月及 1 年之憂鬱傾向百分比分別為 46.2% vs. 47.6%、36.9
% vs. 45%、45% vs. 48.9%,二者未達統計顯著差異。生殖技術受孕組夫與自 然受孕組夫於產後 1 個月、6 個月及 1 年之憂鬱傾向百分比分別為 26.9% vs. 23.1
%、27.4% vs. 26%、20% vs. 22.1%,二者未達統計顯著差異。
以 GEE 分析影響妻與夫長期產後憂鬱的預測因子,影響妻憂鬱程度長期變 化的相關因子為家庭經濟狀況(負相關;OR=0.680)、夫憂鬱程度(OR=1.266)、妻 自尊程度(負相關;OR=0.903)、妻親職壓力程度(OR=1.049)等四個變項。影響夫 憂鬱程度長期變化的相關因子為夫教育程度(正相關;OR=1.909)、妻憂鬱程度(正 相關;OR=1.247)、妻自尊程度(正相關;OR=1.025)、夫自尊程度(負相關;
OR=0.904)、夫親職壓力程度(正相關;OR=1.050)等五個變項。夫妻長期產後憂 鬱的預期因子與是否為生殖技術治療(組別)無關。
應用:生殖技術受孕妻與夫產後憂鬱傾向高盛行率值得重視,所得結果瞭解影響 夫妻憂鬱程度長期變化的預測因子,此部分可作為臨床或社區以家庭為中心照護 介入之依據。
關鍵詞:人工生殖技術、不孕夫妻、家庭為中心、產後憂鬱
Abstract
There is an inverse in the utilization of Assisted Reproductive Technology(ART) by infertile couples who may carry a higher risk of psychosocial distress, and adverse birth outcomes during pregnancy as well as a higher mobility of postpartum depression(PPD), it has been less concerned about the whole couple including the husbands pertaining to PPD, though obstetric nursing should highlight the family-centered concept and care.
Purpose:With the family-centered concept, the study aims at investigating the
distribution and predictors of PPD among previously infertile couple through a longitudinal study. In the 2-year project, the couples will be followed up 1 month, 6 month, and 1 year after their deliveries, using couples of natural birth as the control group.
Method:116 couples in study group and 119 couples in control group during 1 month
after their deliveries were recruited. After approval by IRB, the study subjects were interviewed by a mailing questionnaire. There was a total of 94(81%) and 105(82%) of study group and control group, respectively, responded to this survey. The self-administer questionnaire is composed of subjects’ profiles, Edinburgh postpartum depression scale, self-esteem questionnaire, Brief parenting stress questionnaire and social support questionnaire.
Result: Using the cutoff point of ≧10 scores for Edinburgh postpartum depression
scale, the differences in the prevalence of depression tendency 1 month, 6 months and 1 year after birth between wives of ART and non-ART respectively, were 46.2% vs.
47.6%, 36.9% vs. 45% and 45% vs. 48.9%, which were all not reached a statistically significant level. On the other hand, the differences were 26.9% vs. 23.1
%, 27.4% vs. 26% and 20% vs. 22.1% for husbands of ART and non-ART, which were all not reached a statistically significant level, either.
Using generalized estimating equation(GEE)to find out the predictors for the change of postpartum depression over time, it’s showed that economic condition of family, depression status of the husband, self-esteem of the wife and stress status on parenting of the wife were significant predictors for the wives’ postpartum depression over time.
Educational level of the husband, depression status of the wife, self-esteem of the wife, self-esteem of the husband and stress status on parenting of the husband were significant predictors for the husbands’ postpartum depression over time. Whether or not receiving ART was not a significant predictor for both wives’ and husbands’
postpartum depression.
Application:There is a high prevalence of postpartum depression among previously infertile couples, and understanding of predictors postpartum depression is the key for effective family-centered intervention prevent or solve the problem.
Key words: Assisted Reproductive Technology (ART), infertile couple,
family-centered, postpartum depression
報告內容、參考文獻、計畫成果自評、可供推廣之研發成果資料表、附錄。
前言
產後憂鬱(postpartum depression;PPD)是產後心理健康的重要議題,
對於個人、家庭及小孩發展均可能造成負向的影響,常發生於產後一個月甚 至持續至產後一年(Chien, Tai, Hwang, & Huang, 2009)。產後憂鬱之相關負 向症狀,如憂鬱情緒、失去生活樂趣、體重睡眠改變、疲憊、無精打采、無 價值感、罪惡感、無法集中注意甚至有自殺意圖,於美國精神醫學會(American Psychiatry Association,1994)、Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) International Classification of Diseases, 10th Edition (ICD-10)等,對於其診斷都有相關定義。目前多數研究對於產後憂鬱 多以自我檢測之篩檢工具進行,因不同的篩檢工具,產後憂鬱的盛行率約為 5.5~25%(Centers for Disease, 2008; Gotlib, Whiffen Mout, Milne, & Cordy, 1989; Halbreich, 2005; Nielsen, Videbech, Hedegaard, Dalby, & Secher, 2001;
Söderquist, Wijma, Thorbert, & Wijma, 2009),台灣產後憂鬱的盛行率約為 11.8~42.6%(Chen, Tseng, Wang , & Lee, 1994; Teng, et al, 2005; Chen, Kuo, Chou, & Chen, 2007)。愛丁堡產後憂鬱量表(Edinburgh Postpartum Depression Scale;EPDS)由 Cox、Holden、與 Sagovsky 等人發展(Cox, Holden, & Sagovsky, 1987),其敏感度(sensitivity)及特異度(specificity)均佳,目前廣泛被使 用(Hewitt et al, 2009)。有關心理社會文化的研究顯示:產後憂鬱的危險因 子包括、低自尊、育兒壓力、低社會支持、婚姻關係差,之前憂鬱病史及生 活壓力事件(Chen, Tseng, Wang , & Lee, 1994; Beck, 2001; Dimitrovsky, Hirshberg, & Itskowitz, 1986)。
懷孕與生產雖以母親為主體,父親參與其中的角色卻不容忽視,目前臨床上 對於孕產家庭的照顧雖強調以家庭為中心的照護概念,然而實務面卻缺乏實證之 基礎,父親也僵化地被視為母親之社會支持的最佳人選。父親的需求及其心理變 化 甚 至有關父親的憂鬱研 究( paternal depression)較少受注意。Paulson &
Bazemore(2010)於 JAMA 發表的統合研究發現父親產前產後的憂鬱盛行率為 10.4%,且與母親之憂鬱有中等程度正相關。此研究結果引發的省思是產後家庭 包含母親與父親,他們的心理反應是一致的,彼此的關連度很高。在提供產後照 護時,應以家庭為中心的概念含蓋夫與妻視為一個整體。然而目前產後憂鬱的研 究多以個別的以母親為主,父親較少提及,母親與父親為一整體的以家庭為中心 概念來探討產後憂鬱的研究則更闕如。
近來不孕夫妻接受人工生殖技術治療成功懷孕生子有逐年增加趨勢(國健局,
2011;Gerris, 2002;Kremer, 2002;Olivius, Friden, Lundin, & Bergh, 2002)。夫妻 一但成功懷孕,還需面對較高的孕期合併症,以及因多胞胎而導致早產、低出生 體重等較差嬰兒之出生結果(Poikkeus, Gissler, Unkila-Kallio, Hyden-Granskog, Tiitinen, 2007;Romoundstad, et al, 2006;Sunderam, et al, 2009)。因懷孕、生產過 程的特殊性及較差的嬰兒出生結果,接受人工生殖技術治療夫妻之產後憂鬱情形
是否與自然受孕夫妻不同,值得進一步探討。李淑杏等人(2011)以貝氏憂鬱量 表調查 60 位接受試管嬰兒治療母親於產後 5-7 周之產後憂鬱情形;其盛行率為 25%,輕度憂鬱佔 16.7%、中度憂鬱佔 6.7%、重度憂鬱佔 1.7%,產後憂鬱的預 測因子為試管嬰兒治療次數、社會支持及剖腹產次數。Vilska 等人(2009)的長 期追蹤研究顯示對人工生殖技術治療產下雙胞胎之母親比產下單胞胎之母親於 產後 2 個月有更高的產後憂鬱症狀且持續至產後 1 年。國內有關接受人工生殖技 術治療之產後憂鬱情形之研究有限;僅筆者(李淑杏、劉玲娟、郭碧照、李茂盛,
2011)針對接受試管嬰兒治療母親之小樣本、橫斷性研究。而以筆者所提,對於 此特殊族群以家庭為中心概念並做長期之追蹤等研究,目前並未有相關文獻探討!
因此建立此照護概念的實證研究相形重要!本研究之目的即在建立從夫妻個體 及以夫妻為整體的家庭中心概念,探討接受人工生殖技術治療夫妻之產後憂鬱及 其長期性之變化。
研究目的
本研究計畫的目的如下:
1. 分析接受人工生殖技術治療懷孕生產後一個月、六個月及一年夫妻產後憂鬱 情形及其預測因子。
2. 比較接受人工生殖技術治療懷孕與自然受孕生產後一個月、六個月及一年夫 妻的產後憂鬱情形及其預測因子之模式。
研究方法
本研究為二年期計畫,研究設計採縱貫式研究法(Longitudinal study
design),研究時間點為夫妻產後一個月、六個月及產後一年。研究組為接受
人工生殖技術治療生產後含夫與妻之家庭(study group)及對照組自然生產 產後含夫與妻之家庭(control group)。
1. 研究對象
研究對象選取條件為:(1)研究組:接受人工協助生殖技術治療初次懷 孕生產之夫妻,能閱讀中文並同意填寫問卷者,排除條件為已有生育小孩者。
(2)對照組:第一胎自然生產產後夫妻,能閱讀中文並同意填寫問卷者。研 究組收案共 116 對夫妻,完成問卷填寫者共 94 對,回收率為 81%。對照組 收案共 119 對夫妻,完成問卷填寫者共 105 對,回收率 88%。
2. 研究場所
研究組於中部某一生殖治療中心收案,該中心於 2010 年約有 1399 治療 週期(全國約 9266 週期,約占全國個案之 15%)(國健局,2011),是國內重 要的生殖治療中心之一。對照組以中部某醫學中心產後病房為收案場所,該 醫學中心每月約有 100 位婦女生產,個案來源含市區及屯區等不同社區居
民。
3. 研究步驟
通過 IRB 審查後,符合研究對象之選取條件後進行如下:研究組:經由 病歷紀錄,在個案生產後以電話聯繫,經由研究者說明研究目的,徵求產後夫 妻之同意,並填寫知情同意書後,於產後一個月、六個月及一年時,以郵寄問 卷方式,請夫妻分別填答,完成後再以回郵信封寄回。對照組:於產後病房選 取個案,經由研究者說明研究目的,徵求產後夫妻之同意,並填寫同意書後,
於產後一個月、六個月及一年時,以郵寄問卷方式,請夫妻分別填答,完成後 再以回郵信封寄回。
5. 研究工具
本研究所採用之工具,為研究者參考國內外有關文獻、本團隊研究經驗、
人文與社會學專家建議及下列各標準量表加以編制成的結構式問卷,經測試 信、效度後開始施測,內容包括:
(1)不孕症夫妻的基本資料:年齡、教育程度、經濟狀況、不孕原因、不 孕時間及生殖技術相關資料、生產方式、生產合併症、母嬰同室及哺餵母乳。
(2)愛丁堡產後憂鬱量表(Edinburgh Postpartum Depression Scale;EPDS):
由 Cox、Holden、與 Sagovsky 等人所發展出來的愛丁堡產後憂鬱量表,
可快速篩檢出產後憂鬱症的患者。該量表共 10 題,每題以 Likert scale 的四 點量表設計,為 3 分、2 分、1 分及 0 分。此量表最高分數為 30 分,≧10 分 表示可能有憂鬱情形,目前廣泛使用於產後心理健康的測試(Cox, Holden, &
Sagovsky, 1987)。量表於本研究之內部一致性信度 Cronbach's Alpha 值為 0.85。
(3)自尊量表(Coopersmith’s Self-Esteem Inventory; SEI):
乃由 Stanley Coopersmith 發展測量自我對於社交及一般個人領域滿意 之經驗,此為標準化量表,具有良好信效度。經購買版權後使用。本研究使 用簡版問卷,含 25 題,計分方式依工具使用指引計算,分數越高代表自尊 越高,滿分為 100 分。量表於本研究之庫李信度值為 0.86。
(4)社會支持量表(Interpersonal Support Evaluation List;簡稱 ISEL)
此量表是由 Cohen,Mermelstein,Kamarch 及 Hoberman(1985)所設計,用以 測量個人所知覺潛在性社會資源的可利用性,原始量表含 40 題,是根據可以促 進個體因應壓力事件的支持性社會資源而發展出的量表。量表涵蓋四個向度:即 實質性的幫助、評價、自尊和歸屬感。此量表具有良好的再測信度、內在一致性 信度和建構效度。計分方式採 Likert Scale 四分法,「非常不同意」(0 分),「有點 不同意」(1 分),「有點同意」(2 分),「非常同意」(3 分);總分最高為 48 分,
總分越高則表示其社會支持度越好。16 題是簡式量表,陳氏將之譯成中文,用 於產後憂鬱的研究,顯示具有良好的再測信度、內在一致性和建構效度(Chen,
1994,1996)。本研究使用陳氏的中文版社會支持量表。量表於本研究之內部一 致性信度 Cronbach's Alpha 值為 0.86。
(5)短式親職壓力量表(Parenting Stress Index-Short Form ; PSI/SF)
本研究採用任文香(1995)翻譯的短式親職壓力量表。此量表是由 Richard R.
Abidin 教授(1990)經過多年與多次修定發展而來,在國內外有關親職壓力議題之 倫理驗證或應用均廣泛使用(翁毓秀,1995)。本量表主要目的在於測量親子系統中,
父母親在扮演親職角色時所面臨的壓力。該量表含三個次量表,分別為:(1)親
職愁苦(parental distress):包括父母的愁苦、角色的束縛、社會孤立及夫妻關係 不良等問題。(2)親子互動失調(dysfunctional parent-child interaction):包括與 子女互動的滿足情形、子女給父母的正增強及依附關係等問題。(3)困難兒童
(difficult child):包含兒童的適應能力、需求、情緒、注意力分散及活動量問題。
各分量表均含 12 題,共 36 題。本量表以 Likert scale 的五點量表設計,每一題 項以「極同意」、「同意」、「不肯定」、「不同意」、「極不同意」5 個程度之分,反 向題分別給予 5 分、4 分、3 分、2 分、1 分;正向題則給 1 分、2 分、3 分、4 分、5 分(翁毓秀,1995)。得分越高者表示其親職壓力越大。任文香(1995)
之研究顯示該量表總量表及次量表之內部一致性信度Cronbach α 值為 0.93、0.85、
0.86 及 0.87。以因素分析考驗其建構效度,效果亦佳。於本研究整體量表之內部 一致性信度 Cronbach's Alpha 值為 0.94;次量表之內部一致性信度 Cronbach's Alpha 值分別為 0.86、0.90、0.94。
6. 統計分析:
所得資料將予譯碼輸入電腦,以 SPSS/PC Window 18.0 進行統計分析,方法 為:
(1)描述性統計:包括夫妻的基本資料、產後憂鬱、自尊、社會支持及親 職壓力等情形,之頻率分佈、百分比、平均值±標準差。
(2)階層線性模型(Hierarchical Linear Modeling;HLM): 探討自尊、社 會支持、親職壓力對於夫妻個體及以夫妻為整體之產後憂鬱情形。
(3)廣義估計方程式(Generalized Estimating Equation;GEE):進行含時間 因素之多變項分析,瞭解夫妻長期產後憂鬱的預期因子。
7. 研究倫理
本研究經中山醫學大學附設醫院人體試驗委員會(Institutional Review Board ; IRB)通過後開始執行(編號 CS11278)。擬定受試者同意書,確保受試者完全了解 研究目的、進行步驟、及隨時可中斷參與研究,且瞭解到其所受醫療照顧不因是 否參與研究而受影響,達到知情同意原則,並簽立同意書後,開始進行研究。
結果 1.人口學資料(Table1)
Table1 基本人口學變項的差異性分析
變項名稱
生殖技術受孕組(n=94) 自然受孕組(n=105)
p 值 平
均 值
標 準 差
人 數
百 分 比
平 均 值
標 準 差
人 數
百 分 比
夫年齡(年) 38.1 4.5 33.2 4.7 <0.001***
妻年齡(年) 34.8 3.8 31.1 3.6 <0.001***
夫妻年齡差(年)# 3.3 4.5 2.1 3.5 0.032*
結婚年數 5.8 2.7 2.2 1.4 <0.001***
夫教育程度 0.589
高中/職以下 20 21.3 21 20.0
大專 54 57.4 67 63.8
研究所 20 21.3 17 16.2
妻教育程度 0.001**
高中/職以下 25 26.6 12 11.4
大專 55 58.5 86 81.9
研究所 14 14.9 7 6.7
家庭月收入 0.026*
<4 萬 8 8.5 21 20.0
4-6 萬 29 30.9 33 31.4
6-8 萬 20 21.3 29 27.6
8-10 萬 18 19.1 10 9.5
>10 萬 19 20.2 12 11.4
# Mann-Whitney U 檢定,α=0.05,*p<0.05 **p<0.01 ***p<0.001 類別變項採用卡方檢定,α=0.05,*p<0.05 **p<0.01 ***p<0.001
2.生產相關變項資料(Table2)
Table2 生產相關變項的描述性統計與差異性分析
變項名稱
生殖技術受孕組(n=94) 自然受孕組(n=105)
p 值 平
均 值
標 準 差
人 數
百 分 比
平 均 值
標 準 差
人 數
百 分 比
不孕年數 4.2 2.8 - - -
治療年數 1.8 1.9 - - -
治療次數 1.9 1.4 - - -
生產週數 37.7 1.9 38.2 2.4 0.105
產後合併症 0.971
有 8 8.5 9 8.7
無 86 91.5 95 91.3
胎數
單胞胎 67 71.3 101 97.1 <0.001***
多胞胎 27 28.7 3 2.9
生產方式 <0.001***
自然產 30 31.9 76 72.4
剖腹產 64 68.1 29 27.6
親子同室 <0.001***
有 41 43.6 76 72.4
無 53 56.4 29 27.6
哺育母乳(1M) 0.022*
有 68 78.2 92 90.2
無 19 21.8 10 9.8
哺育母乳(6M) 0.007**
有 39 47.0 66 66.7
無 44 53.0 33 33.3
哺育母乳(12M) 0.025*
有 22 26.2 42 42.0
無 62 73.8 58 58.0
連續變項採用獨立樣本 t 檢定,α=0.05,*p<0.05 **p<0.01 ***p<0.001 類別變項採用卡方檢定,,α=0.05,*p<0.05 **p<0.01 ***p<0.001
3.生殖技術組與自然受孕組產後憂鬱傾向盛行率(Table3)
Table3 生殖技術受孕組及自然受孕組之憂鬱傾向盛行率及差異性分析(1M, 6M, 12M)
變項名稱
有憂鬱傾向 (EPDS≧10)
無憂鬱傾向
(EPDS<10) p 值 OR
人數 百分比 人數 百分比
妻(1M) 0.852 0.948
生殖技術受孕組 43 46.2 50 53.8
自然受孕組 49 47.6 54 52.4
妻(6M) 0.267 0.715
生殖技術受孕組
組 31 36.9 53 63.1
自然受孕組 45 45.0 55 55.0
妻(12M) 0.604 0.854
生殖技術受孕組 36 45.0 44 55.0
自然受孕組 46 48.9 48 51.1
夫(1M) 0.537 1.225
生殖技術受孕組 25 26.9 68 73.1
自然受孕組 24 23.1 80 76.9
夫(6M) 0.833 1.073
生殖技術受孕組 23 27.4 61 72.6
自然受孕組 26 26.0 74 74.0
夫(12M) 0.734 0.883
生殖技術受孕組 16 20.0 64 80.0
自然受孕組 21 22.1 74 77.9
家庭(1M) 0.599 1.177
生殖技術受孕組 30 32.6 62 67.4
自然受孕組 30 29.1 73 70.9
家庭(6M) 0.568 0.828
生殖技術受孕組 22 26.2 62 73.8
自然受孕組 30 30.0 70 70.0
家庭(12M) 0.259 0.674
生殖技術受孕組 18 22.5 62 77.5
自然受孕組 28 30.1 65 69.9
採用卡方檢定,α=0.05,*p<0.05 **p<0.01 ***p<0.001 OR: 勝算比(odds ratio)
Table4 生殖技術受孕組與自然受孕組在產後 1 個月、6 個月及 1 年之憂鬱程度分 析
變項名稱 生殖技術受孕組 自然受孕組
平均值 標準差 平均值 標準差 p 值 妻憂鬱
1M 9.9 5.4 9.5 5.2 0.605
6M 9.0 5.4 9.2 5.0 0.769
12M 9.5 4.5 9.6 5.2 0.879
夫憂鬱
1M 7.1 4.2 6.6 4.4 0.398
6M 6.8 4.2 6.8 4.2 0.992
12M 6.4 4.2 7.0 5.1 0.377
家庭憂鬱
1M 8.5 4.0 8.1 3.9 0.463
6M 7.9 3.9 8.0 3.8 0.840
12M 7.9 3.6 8.3 4.4 0.529
獨立樣本 t 檢定,α =0.05
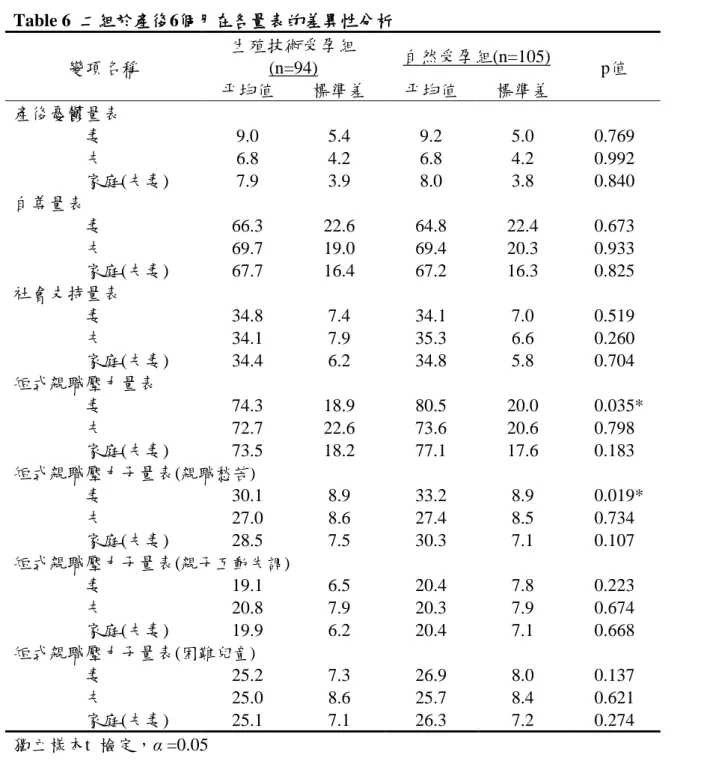
4.生殖技術受孕組與自然受孕組在產後 1 個月、6 個月及 1 年之憂鬱量表、自尊 量表、社會支持量表及短式親職壓力量表之差異性分析(Table5、Table6、Table7)
Table 5 二組於產後1個月在各量表的差異性分析
變項名稱
生殖技術受孕組
(n=94) 自然受孕組(n=105)
p值
平均值 標準差 平均值 標準差
產後憂鬱量表
妻 9.9 5.4 9.5 5.2 0.605
夫 7.1 4.2 6.6 4.4 0.398
家庭(夫妻) 8.5 4.0 8.1 3.9 0.463 自尊量表
妻 64.5 20.5 64.7 20.4 0.933 夫 68.6 17.1 67.4 19.7 0.636 家庭(夫妻) 66.5 13.6 66.0 14.9 0.830 社會支持量表
妻 35.1 6.5 34.9 6.9 0.851 夫 34.0 7.0 34.8 6.7 0.468 家庭(夫妻) 34.6 5.5 34.8 5.2 0.717 短式親職壓力量表
妻 84.5 21.6 84.7 20.7 0.958 夫 81.8 23.5 77.0 21.1 0.148 家庭(夫妻) 82.9 20.1 80.6 18.1 0.444 短式親職壓力子量表(親職愁苦)
妻 31.6 9.2 31.7 7.9 0.951 夫 27.9 9.0 27.0 7.5 0.474 家庭(夫妻) 29.7 7.9 29.4 6.4 0.768 短式親職壓力子量表(親子互動失調)
妻 22.9 7.1 23.0 8.7 0.899 夫 23.7 8.3 22.1 7.9 0.166 家庭(夫妻) 23.3 6.5 22.6 7.0 0.465 短式親職壓力子量表(困難兒童)
妻 30.3 9.0 29.7 8.6 0.689 夫 29.5 9.6 27.9 9.1 0.248 家庭(夫妻) 29.9 8.3 28.8 7.7 0.361 獨立樣本t 檢定,α =0.05
Table 6 二組於產後6個月在各量表的差異性分析
變項名稱
生殖技術受孕組
(n=94) 自然受孕組(n=105)
p值
平均值 標準差 平均值 標準差
產後憂鬱量表
妻 9.0 5.4 9.2 5.0 0.769
夫 6.8 4.2 6.8 4.2 0.992
家庭(夫妻) 7.9 3.9 8.0 3.8 0.840 自尊量表
妻 66.3 22.6 64.8 22.4 0.673 夫 69.7 19.0 69.4 20.3 0.933 家庭(夫妻) 67.7 16.4 67.2 16.3 0.825 社會支持量表
妻 34.8 7.4 34.1 7.0 0.519 夫 34.1 7.9 35.3 6.6 0.260 家庭(夫妻) 34.4 6.2 34.8 5.8 0.704 短式親職壓力量表
妻 74.3 18.9 80.5 20.0 0.035*
夫 72.7 22.6 73.6 20.6 0.798 家庭(夫妻) 73.5 18.2 77.1 17.6 0.183 短式親職壓力子量表(親職愁苦)
妻 30.1 8.9 33.2 8.9 0.019*
夫 27.0 8.6 27.4 8.5 0.734 家庭(夫妻) 28.5 7.5 30.3 7.1 0.107 短式親職壓力子量表(親子互動失調)
妻 19.1 6.5 20.4 7.8 0.223 夫 20.8 7.9 20.3 7.9 0.674 家庭(夫妻) 19.9 6.2 20.4 7.1 0.668 短式親職壓力子量表(困難兒童)
妻 25.2 7.3 26.9 8.0 0.137 夫 25.0 8.6 25.7 8.4 0.621 家庭(夫妻) 25.1 7.1 26.3 7.2 0.274 獨立樣本t 檢定,α =0.05
Table 7 二組於產後12個月在各量表的差異性分析 變項名稱
生殖技術受孕組
(n=94) 自然受孕組(n=105)
p值
平均值 標準差 平均值 標準差
產後憂鬱量表
妻 9.5 4.5 9.6 5.2 0.879
夫 6.4 4.2 7.0 5.1 0.368
家庭(夫妻) 7.9 3.6 8.3 4.4 0.529 自尊量表
妻 64.1 23.3 61.1 24.2 0.419 夫 71.9 18.9 68.7 20.0 0.291 家庭(夫妻) 67.8 16.5 64.8 17.9 0.247 社會支持量表
妻 33.1 7.4 33.1 7.1 0.991 夫 34.3 7.3 33.9 7.0 0.679 家庭(夫妻) 33.7 6.2 33.5 6.0 0.801 短式親職壓力量表
妻 79.4 17.7 81.4 22.1 0.536 夫 72.1 20.4 75.2 22.1 0.352 家庭(夫妻) 75.8 16.2 78.7 19.9 0.316 短式親職壓力子量表(親職愁苦)
妻 31.4 7.6 33.2 10.0 0.181 夫 26.5 8.3 27.6 8.6 0.388 家庭(夫妻) 28.9 6.6 30.6 8.0 0.140 短式親職壓力子量表(親子互動失調)
妻 20.2 6.3 20.1 7.1 0.967 夫 19.8 7.0 20.7 7.8 0.404 家庭(夫妻) 20.0 5.4 20.5 6.7 0.587 短式親職壓力子量表(困難兒童)
妻 27.6 7.9 28.3 9.1 0.592 夫 25.8 8.1 26.9 8.7 0.388 家庭(夫妻) 26.8 6.9 27.7 7.8 0.422 獨立樣本t 檢定,α =0.05
5.產後不同階段妻憂鬱之線性複迴歸分析(Table8、Table9、Table10)
Table8 產後 1 個月妻憂鬱的線性複迴歸分析
模式 變項名稱 未標準化係數 標準化係數
t 值 p 值 95%信賴區間 共線性統計量
B 估計值 標準誤 Beta 分配 下限 上限 允差 VIF
1 常數 20.811 1.167 17.839 0.000** 18.506 23.117
妻自尊 1M -0.169 0.017 -0.636 -9.928 0.000** -0.203 -0.135 1.000 1.000 2
常數 17.774 1.296 13.716 0.000** 15.212 20.335
妻自尊 1M -0.157 0.016 -0.593 -9.699 0.000** -0.189 -0.125 0.974 1.026 夫憂鬱 1M 0.324 0.073 0.270 4.419 0.000** 0.179 0.468 0.974 1.026
3
常數 12.616 2.548 4.951 0.000** 7.580 17.653
妻自尊 1M -0.132 0.019 -0.497 -6.823 0.000** -0.170 -0.094 0.665 1.503 夫憂鬱 1M 0.290 0.074 0.242 3.942 0.000** 0.145 0.435 0.937 1.067 妻親職壓力
1M 0.044 0.019 0.174 2.339 0.021* 0.007 0.081 0.640 1.562 線性複回歸分析,採用 stepwise 法,α =0.05,*p<0.05 **p<0.01
應變項:妻憂鬱 1M
自變項:組別(0=自然受孕,1=人工受孕)、妻年齡 1M、夫妻年齡差、妻教育程度、產後合併症、家庭經濟狀況 1M、生產方式(0=剖腹 產,1=自然產)、生產週數、親子同室(0=無,1=有)、哺育母乳 1M(0=無,1=有)、夫憂鬱 1M、妻自尊 1M、夫自尊 1M、妻社會支持 1M、
夫社會支持 1M、妻親職壓力 1M、夫親職壓力 1M 調整後的 R2為 0.485 (模式 3, F 值=46.741)
回歸方程式:妻憂鬱 1M = 12.616-0.132×(妻自尊 1M)+0.290×(夫憂鬱 1M)+0.044×(妻親職壓力 1M)
Table9 產後 6 個月妻憂鬱的線性複迴歸分析
模式 變項名稱
未標準化係數 標準化係數
t 值 p 值
95%信賴區間 共線性統計量
B 估計
值 標準誤 Beta 分配 下限 上限 允差 VIF
1 (常數) 20.322 0.859 23.663 0.000** 18.627 22.018
妻自尊 6M -0.170 0.012 -0.723 -13.693 0.000** -0.195 -0.146 1.000 1.000 2
(常數) 13.297 1.949 6.822 0.000** 9.449 17.145
妻自尊 6M -0.139 0.014 -0.589 -9.656 0.000** -0.167 -0.110 0.691 1.447 妻親職壓力 6M 0.063 0.016 0.242 3.976 0.000** 0.032 0.095 0.691 1.447 3
(常數) 26.269 4.996 5.258 0.000** 16.407 36.131
妻自尊 6M -0.143 0.014 -0.608 -10.105 0.000** -0.171 -0.115 0.682 1.466 妻親職壓力 6M 0.058 0.016 0.224 3.726 0.000** 0.027 0.089 0.683 1.464 生產週數 -0.325 0.115 -0.141 -2.810 0.006** -0.553 -0.097 0.984 1.016 4 (常數) 26.951 4.929 5.468 0.000** 17.221 36.682
妻自尊 6M -0.138 0.014 -0.587 -9.824 0.000** -0.166 -0.110 0.670 1.493 妻親職壓力 6M 0.059 0.015 0.226 3.817 0.000** 0.028 0.090 0.683 1.465 生產週數 -0.313 0.114 -0.136 -2.751 0.007** -0.538 -0.089 0.983 1.018 家庭經濟狀況 -0.510 0.205 -0.123 -2.481 0.014** -0.915 -0.104 0.975 1.026 5 (常數) 26.117 4.883 5.349 0.000** 16.478 35.757
妻自尊 6M -0.134 0.014 -0.570 -9.580 0.000** -0.162 -0.107 0.659 1.517 妻親職壓力 6M 0.053 0.016 0.202 3.404 0.001** 0.022 0.083 0.662 1.511 生產週數 -0.311 0.112 -0.135 -2.765 0.006** -0.533 -0.089 0.983 1.018 家庭經濟狀況 -0.519 0.203 -0.125 -2.555 0.012* -0.919 -0.118 0.975 1.026 夫憂鬱 6M 0.146 0.064 0.116 2.273 0.024* 0.019 0.273 0.903 1.107 線性複回歸分析,採用 stepwise 法,α =0.05,*p<0.05 **p<0.01
應變項:妻憂鬱 6M
自變項:組別(0=自然受孕,1=人工受孕)、妻年齡 6M、夫妻年齡差、妻教育程度、產後合併症(0=無,1=有)、家庭經濟狀況 6M、生產方 式、生產週數、親子同室(0=無,1=有)、哺育母乳 6M(0=無,1=有)、夫憂鬱 6M、妻自尊 6M、夫自尊 6M、妻社會支持 6M、夫社會支持 6M、妻親職壓力 6M、夫親職壓力 6M
調整後的 R2為 0.598 (模式 5, F 值=52.216)
回歸方程式:妻憂鬱 6M = 26.117-0.134×(妻自尊 6M)+0.053×(妻親職壓力 6M)-0.134×(生產週數)-0.519×(家庭經濟情況)+0.146×(夫憂鬱
6M)
Table10 產後 12 個月妻憂鬱的線性複迴歸分析
模式 變項名稱 未標準化係數 標準化係數
t 值 p 值 95%信賴區間 共線性統計量
B 估計值 標準誤 Beta 分配 下限 上限 允差 VIF
1 常數 18.957 0.768 24.674 0.000** 17.439 20.474
妻自尊 12M -0.151 0.011 -0.723 -13.189 0.000** -0.174 -0.129 1.000 1.000 2
常數 16.363 0.886 18.459 0.000** 14.612 18.114
妻自尊 12M -0.139 0.011 -0.665 -12.679 0.000** -0.161 -0.117 0.951 1.052 夫憂鬱 12M 0.275 0.055 0.261 4.972 0.000** 0.166 0.384 0.951 1.052
3
常數 10.603 1.871 5.666 0.000** 6.906 14.299
妻自尊 12M -0.112 0.013 -0.537 -8.561 0.000** -0.138 -0.086 0.621 1.610 夫憂鬱 12M 0.209 0.057 0.199 3.693 0.000** 0.097 0.321 0.845 1.184 妻親職壓力
12M 0.056 0.016 0.230 3.463 0.001** 0.024 0.088 0.552 1.810 線性複回歸,採用 stepwise 法,α =0.05,*p<0.05 **p<0.01
應變項:妻憂鬱 12M
自變項:組別(0=自然受孕,1=人工受孕)、妻憂鬱 12M、妻年齡 12M、夫妻年齡差、妻教育程度、產後合併症(0=無,1=有)、家庭經濟狀 況 12M、生產方式(0=剖腹產,1=自然產)、生產週數、親子同室、哺育母乳 12M(0=無,1=有)
、夫憂鬱 12M、妻自尊 12M、夫自尊 12M、妻社會支持 12M、夫社會支持 12M、妻親職壓力 12M、夫親職壓力 12M 調整後的 R2為 0.609(模式 3, F 值=84.078)
回歸方程式:妻憂鬱 12M = 10.603-0.112×(妻自尊 12M)+0.290×(夫憂鬱 12M)+0.056×(妻親職壓力 12M)
6.以 GEE 分析影響妻與夫長期產後憂鬱的預測因子(Table11、Table12)
Table11 以 GEE 分析影響妻長期產後憂鬱的預測因子
變項名稱 B 估計值 標準誤 95% Wald 信賴區間 假設檢定
Exp(B) Exp(B)的 95% CI
下限 上限 Wald df 顯著性 下限 上限
常數項 16.521 4.634 7.438 25.605 12.708 1 0.000** - - -
產後 12M -0.467 0.370 -1.194 0.259 1.592 1 0.207 0.627 0.303 1.295 產後 6M -0.294 0.333 -0.947 0.359 0.778 1 0.378 0.745 0.388 1.432 組別=自然受孕 -0.085 0.496 -1.057 0.887 0.029 1 0.864 0.919 0.347 2.428 產後合併症=無 -0.139 0.883 -1.869 1.592 0.025 1 0.875 0.871 0.154 4.915 生產方式=剖腹 0.345 0.449 -0.537 1.226 0.587 1 0.443 1.411 0.585 3.406 親子同室=無 0.733 0.441 -0.133 1.509 2.755 1 0.097 2.082 0.876 4.950 哺育母乳=無 0.453 0.336 -0.206 1.113 1.814 1 0.178 1.574 0.814 3.044 夫妻年齡差 -0.006 0.061 -0.126 0.115 0.008 1 0.927 0.994 0.882 1.122 妻教育程度 -0.209 0.409 -1.012 0.594 0.261 1 0.609 0.811 0.363 1.811 家庭經濟狀況 -0.386 0.192 -0.764 -0.009 4.024 1 0.045* 0.680 0.466 0.991 生產週數 -0.106 0.082 -0.267 0.056 1.641 1 0.200 0.900 0.765 1.058 妻年齡 -0.024 0.065 -0.153 0.104 0.138 1 0.710 0.976 0.858 1.110 夫憂鬱程度 0.236 0.055 0.126 0.345 17.885 1 0.000** 1.266 1.135 1.412 妻自尊程度 -0.102 0.011 -0.124 -0.079 80.346 1 0.000** 0.903 0.883 0.924 夫自尊程度 0.010 0.012 -0.015 0.035 0.594 1 0.441 1.010 0.985 1.035 妻社會支持程度 -0.074 0.039 -0.151 0.004 3.485 1 0.062 0.929 0.860 1.004 夫社會支持程度 0.048 0.031 -0.014 0.109 2.330 1 0.127 1.049 0.987 1.115 妻親職壓力程度 0.048 0.010 0.027 0.069 20.177 1 0.000** 1.049 1.027 1.071 夫親職壓力程度 0.005 0.013 -0.022 0.032 0.135 1 0.713 1.005 0.978 1.033 概化估計方程式,α =0.05,*p<0.05 **p<0.01
應變項:妻憂鬱程度變化
自變項:組別、產後合併症、生產方式、親子同室、哺育母乳、夫妻年齡差、妻教育程度、家庭經濟狀況、生產週數、妻年齡、夫憂 鬱程度、妻自尊程度、夫自尊程度、妻社會支持程度、夫社會支持程度、妻親職壓力程度、夫親職壓力程度
Table12 以 GEE 分析影響妻長期產後憂鬱的預測因子
變項名稱 B 估計值 標準誤 95% Wald 信賴區間 假設檢定
Exp(B) Exp(B)的 95% CI
下限 上限 Wald df 顯著性 下限 上限
常數項 7.881 3.416 1.187 14.576 5.324 1 0.021* - - --
產後 12M 0.138 0.345 -0.539 0.815 0.160 1 0.689 1.148 0.584 2.259 產後 6M 0.316 0.286 -0.244 0.876 1.224 1 0.269 1.372 0.784 2.401 組別=自然受孕 -0.011 0.493 -0.976 0.955 0.000 1 0.983 0.989 0.377 2.599 夫妻年齡差 -0.021 0.061 -0.141 0.099 0.119 1 0.730 0.979 0.868 1.104 夫教育程度 0.647 0.324 0.012 1.282 3.983 1 0.046* 1.909 1.012 3.604 家庭經濟狀況 -0.119 0.171 -0.454 0.217 0.481 1 0.488 0.888 0.635 1.242 夫年齡 0.017 0.061 -0.103 0.138 0.081 1 0.776 1.018 0.902 1.148 妻憂鬱程度 0.021 0.061 0.101 0.341 13.025 1 0.000** 1.247 1.106 1.406 妻自尊程度 0.024 0.012 0.002 0.047 4.387 1 0.036* 1.025 1.002 1.048 夫自尊程度 -0.101 0.013 -0.126 -0.076 62.784 1 0.000** 0.904 0.881 0.927 妻社會支持程度 -0.051 0.035 -0.121 0.018 2.116 1 0.146 0.950 0.886 1.018 夫社會支持程度 -0.013 0.031 -0.073 0.047 0.187 1 0.665 0.987 0.929 1.048 妻親職壓力程度 -0.010 0.011 -0.031 0.012 0.767 1 0.381 0.990 0.969 1.012 夫親職壓力程度 0.048 0.012 0.024 0.073 15.322 1 0.000** 1.050 1.024 1.075 概化估計方程式,α =0.05,*p<0.05 **p<0.011
應變項:夫憂鬱程度變化
自變項:組別、夫妻年齡差、夫教育程度、家庭經濟狀況、夫年齡、妻憂鬱程度、妻自尊程度、夫自尊程度、妻社會支持程度、夫社 會支持程度、妻親職壓力程度、夫親職壓力程度
結論及應用 依本研究目的所得研究結果之綜合結論如下:
1. 愛丁堡產後憂鬱量表以≧10 分為切點,比較二組憂鬱傾向之分佈與差異。
生殖技術受孕組妻與自然受孕組妻於產後 1 個月、6 個月及 1 年之憂鬱 傾向百分比分別為 46.2% vs. 47.6%、36.9% vs. 45%、45% vs. 48.9%,
二者未達統計顯著差異。生殖技術受孕組夫與自然受孕組夫於產後 1 個 月、6 個月及 1 年之憂鬱傾向百分比分別為 26.9% vs. 23.1%、27.4% vs.
26%、20% vs. 22.1%,二者未達統計顯著差異。所得產後憂鬱傾向盛 行率結果與自然受孕組雖無統計差異,然整體來說妻與夫之憂鬱傾向盛 行率偏高,因此產後家庭之身心健康情形需特別重視,針對此議題應研 擬介入方案以協助產後家庭。
2. 產後 6 個月生殖技術受孕組妻之親職壓力量表平均分數及其親子愁苦子 量表顯著低於自然受孕組妻之平均分數。除上述差異外,二組夫妻在不 同時間點各量表的差異性均未達統計顯著水準。
3. 以線性複回歸分析各階段妻之產後憂鬱相關因子結果顯示妻之自尊、親 職壓力及夫之憂鬱程度,均為重要影響因子。
4. 以 GEE 分析影響妻與夫長期產後憂鬱的預測因子,影響妻憂鬱程度長期 變化的相 關因子 為 家 庭 經濟狀 況 ( 負相 關 ;OR=0.680)、 夫憂鬱 程度 (OR=1.266)、妻自尊程度(負相關;OR=0.903)、妻親職壓力程度(OR=1.049) 等四個變項。影響夫憂鬱程度長期變化的相關因子為夫教育程度(正相關;
OR=1.909)、妻憂鬱程度(正相關;OR=1.247)、妻自尊程度(正相關;
OR=1.025)、夫自尊程度(負相關;OR=0.904)、夫親職壓力程度(正相關;
OR=1.050)等五個變項。上述結果顯示產後家庭妻與夫長期產後憂鬱乃互 為影響,印證本研究之家庭理論架構,因此未來應研擬以家庭為中心的 介入措施提供產後夫妻合適的照護內容。
參考文獻
內政部統計處(2011)‧內政統計年報:育齡婦女生育率‧Retrieved November 20, 2011, from http://sowf.moi.gov.tw/stat/year/list.htm
任文香(1995)。幼兒母親親職壓力,因應策略與親子關係滿意之關係研究.未 出版碩士論 文.台北:國立台灣師範大學家政教育研究所。
李淑杏、李孟智、郭碧照、李茂盛(1991). 接受人工生殖科技治療之不孕症 婦女的心理壓力及其相關因子.公共衛生,18(2),148-163。
李淑杏、郭碧照、李孟智、李茂盛(1995). 接受人工生殖科技治療的不孕症 夫妻之心理社會反應.台灣醫學會雜誌,94(Suppl.1),S26-33。
李淑杏、郭碧照、李孟智、賴慶祥、李茂盛(1998).不孕症夫妻成為父母後的 心理反應變化.台灣醫學,2(2),133-140。
李淑杏、郭碧照、黃梨香、王郁茗、李茂盛(2000). 接受試管嬰兒治療之不孕
症婦女在不同治療階段的心理社會反應.護理研究,8(5),515-528。
翁毓秀(1995).親職壓力量表指導手冊.台北:心理出版社。
國健局(2011)‧ 民國九十八七年台灣地區人工生殖施行結果分析報告‧
台 北 :行 政 院 衛 生 署 國 民 健 康 局 。 2011 年 12 月 1 日 取 自 http://www.bhp.doh.gov.tw
American Psychiatric Association (ed). Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Press, 1994, 720–721.
Abindin, R. R. (1990). Parenting Stress Index, 3rd Edition: Psychological Assessment Resources.
Beck C, T. (2001). Predictors of postpartum depression: an update. Nursing Resreach,50(5), 275-285.
Centersfor Disease, C. and Prevention. (2008). Prevalence of self-reported postpartum depressive symptoms--17 states, 2004-2005. Morbidity & Mortality Weekly Report, 57, 361-366.
Chien, L. Y, Tai, C. J., Hwang, F. M., & Huang, C. M. (2009). Postpartum physical symptoms and depressive symptomatology at 1 month and 1 year after delivery:
A longitudinal questionnaire survey. International Journal of Nursing Studies, 46, 1201-1208.
Chen, C. H., Tseng, Y. F., Wang, S. Y., & Lee, J. N. (1994). The prevalence and predictors of postpartum depression. Journal of Nursing Research, 2(3), 263-274.
Chen, C. M., Kuo, S. F., Chou, Y. H., & Chen, H. C. (2007). Postpartum Taiwanese women: their postpartum depression, social support and health-promoting lifestyle profiles. Journal of Clinical Nursing,16(8), 1550-1560.
Cohen, S., Mermelstein, R., Kamarch, T., & Hoberman, H. M. (1985). Measuring
the functional components of social support.In I.G.Sarason,&
B.R.Sarason(Eds.), Social support:Theory,research and application(pp.73-94).Boston:M.Nihjoff.
Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Dection of postpartum depression:
development of the 10-item Edinburgh Postnatal Depression Scale. The British Journal of Psychiatry,150, 782-786.
Dimitrovsky, L., Hirshberg, M. P., Itskowitz, R. (1986). Depression during and following pregnancy: Quality of family relationships. The Journal of Psychology,121, 213-218.
Duvall, E. M., & Miller, B. C. (1986). Marriage and family development. New York: Harper & Row.
Eugster, A., & Vingerhoets, A. J. J. M. (1999). Psychological aspects of in vitro fertilization: a review. Social Science & Medicine, 48, 575-589.
Gerris, J., De Neubourg, D., Mangelschots, K., Van Royen, E., Vercruyssen, M., Barudy-Vasquez, J., Valkenburg, M., & Ryckaert, G. (2002). Elective single day 3 embryo transfer halves the twinning rate without decrease in the ongoing pregnancy rate of an IVF/ICSI programme. Human Reproduction, 17, 2626–31.
Glazerbrook, C., Cox, S., Oates, M. & Ndukwe, G. (2001). Psychological adjustment during pregnancy and the postpartum period in single and multiple in vitro fertilization births: a review and preliminary findings from an ongoing study.
Reproduction Technology, 10, 112.
Glazerbrook, C., Sheard, C., Cox, S., Oates, M. & Ndukwe, G. (2004). Parenting stress in first-time mothers of twins and triplets conceived after in vitro fertilization. Fertility & Sterility, 81(3),
505-511.
Goodman, J. H. (2004). Paternal postpartum depression, its relationship to maternal postpartum depression, and implications for family health. Journal of Advance Nursing, 45(1), 26-35.
Gotlib, I. H., Whiffen Mout, J. H., Milne, K., & Cordy, N. I. (1989). Prevalence rates and demographic characteristics associates wish depression in pregnancy and the postpartum. Journal of Consulting and Clinical Psychology, 57, 269-274.
Greil, A. L. (1997). Infertility and psychological distress: a critical review of the literature. Social Science & Medicine, 45, 1679-1704.
Halbreich U. (2005).Postpartum disorders: multiple interacting underlying mechanisms and risk factors. Journal of Affective Disorders, 88, 1-7.
Hammarberg K, Fisher, J. R. W. & Wynter, K. H. (2008).Psychological and social aspects of pregnancy, childbirth and early parenting after assisted conception: a systematic review. Human Reproduction Update, 14, 395–414.
Hahn, C. S. (2001). Review: Psychosocial well-being of parents and their children born after assisted reproduction. Journal of Pediatric Psychology, 26(8), 525-538.
Hanson, S. M. H. (2001). Family health care nursing- theory, practice, and research (2 ed). Davis company: philadephia.
Hewitt, C., Gilbody, S., Brealey, S., Paulden, M., Palmer, S., Mann, R., Green, J., Morrell, J., Barkham, M., Light, K. et al. (2009). Methods to identify postnatal depression in primary care: an integrated evidence synthesis and value of information analysis. Health Technology Assessment, 13(1) –230.
Lee, S. H. (2003). Effects of Using a Nursing Crisis Intervention Program on Psychosocial Responses and Coping Strategies for Infertile Women during In-Vitro Fertilization. The Journal of Nursing Research, 11(3),197-208.
Lee, S. H., Lee, M. Y., Chiang, T. L., Lee, M. C., & Lee, M. S. (2010). Child growth from birth to 18 months old born after assisted reproductive technology – Results of a national birth cohort study. International Journal of Nursing Study. 47(9), 1159-1166.
Lee, S. H.*, Liu, L. C., Kuo, P. C., & Lee, M. S. (2011). Postpartum Depression and Correlated Factors in Women Who Received In-vitro Fertilization Treatment.
Journal of Midwifery and Women Health. 56(4), 347-352.
Lee, S. H., Wang, S.C., Kuo, C. P., Kuo, P. C., Lee, M. S., & Lee, M. C. (2010). Grief responses and coping strategies among infertile women after failed IVF treatment. Scandinavian Journal of Caring Sciences. 24(3), 507-513.
Kremer, J. A., et al. (2002). Results of in vitro fertilization in the Netherlands, 1996–2000. Nederlands Tijdschrift voor Geneeskunde, 146, 2358–2363.
Klein, D. M. & White, J. M. (1995). Family Theories: An Introduction. Sage, Thousand Oaks, CA.
Main, M. (1983). Exploration, play, and cognitive functioning related to infant-mother attachment. Infant Behavior and Development, 6, 167-184.
Miller, B. C., & Sollie, D. L.(1980). Normal stresses during the transition to parenthood. Family Relations, 29(4), 459-465.
Nyboe Andersen A, et al. (2009). Assisted reproductive technology and intrauterine inseminations in Europe, 2005: results generated from European registers by ESHRE: ESHRE. The European IVF Monitoring programme (EIM), for the European Society of Human Reproduction and Embryology (ESHRE). Human Reproduction, 24, 1267-1287.
Nielsen, F. D., Videbech, P., Hedegaard, M., Dalby, S. J., & Secher, N. J. (2001).
Postpartum depression: identification of women at risk. An International Journal of Obstetrics & Gynaecology,108(7), 774-775.
O’Hara, M. W., Varner, M.W., & Johnson, S. R. (1986). Assessing stressful life events associated with childbearing: The peripartum Events Scale. Journal of Reproductive and Infant Psychology, 4, 85-98.
Olivius, C., Friden, B., Lundin, K., & Bergh, C. (2002). Cumulative probability of live birth after three in vitro fertilization/ intracytoplasmic sperm injection cycles.
Fertility & Sterility, 77, 505–510.
Poikkeus, Gissler, Unkila-Kallio, Hyden-Granskog, Tiitinen (2007). Obstetricand neonatal outcome after single embryo transfer. Human Reproduction, 22(4), 1073-1079.
Paulson, J. F. & Bazemore, S. D. (2010). Prenatal and postpartum depression in fathers and its association with maternal depression: a meta-analysis. JAMA, 303(19), 1961-1969.
Punamaki, R-L. et al. (2006). Maternal mental health and medical predictors of infant developmental and health problems from pregnancy to one year: Does former infertility matter? Infant Behavior & Development, 29, 230-242.
Romundstad, L.B., et al. (2006). Increased risk of placenta previa in pregnancies following IVF/ICSI; a comparison of ATR and non-ART pregnancies in the same mother. Human Reproduction, 21(9), 2353-2358.
Ramchandani, P. G., Stein, A., O'Connor, T. G., Heron, J., Murray, L., & Evans, J.
(2008). Depression in men in the postnatal period and later child psychopathology: a population cohort study. Journal of American Academiy Child and Adolescnt Psychiatry, 47(4), 390-398.
Ramchandani, P., Stein, A., Evans, J., & O'Connor, T. G. (2005). Paternal depression in the postnatal period and child development: a prospective population study.
Lancet, 365(9478), 2201-2205.
Söderquist, J., Wijma, B., Thorbert, G., & Wijma, K. (2009). Risk factors in pregnancy for post-traumatic stress and depression after childbirth. BJOG:an International Journal of Obstetrics and Gynecology, 116(5), 672-680.
Sunderam, S., et al. (2009). Assisted reproductive technology surveillance: United States, 2006. MMWR Surveillance Summaries/CDC, 58(5), 1-25.
Teng, H. W., Hsu, C. S., Shih, S. M., Lu, M. L., Pan, J. J., & Shen, W. W. (2005).
Screening postpartum depression with the Taiwanese version of the Edinburgh Postnatal Depression Scale. Comprehensive Psychitry, 46, 261-265.
Verhaak, C.M., Smeenk. J.M., Evers. A.W., Kremer, J.A., Kraaimaat, F.W., & Braat, D. D. (2007). Women’s emotional adjustment to IVF: a systematic review of 25 years of research. Human Reproduction Update, 13, 27-36.
Vilska S, Unkila-Kallio L, Punamäki RL, et al. (2009). Mental health of mothers and fathers of twins conceived via assisted reproduction treatment: a 1-year prospective study. Human Reproduction, 24(2), 367-377.
Von Bertalanffy, L. W. (1968). General systems theory: foundations, development, and application. New York, NY: George Braziller.
Wang, Y. A., Dean, J. A., Grayson, N., & Sullivan, E. A. (2004). Assisted reproduction technology in Australia and New Zealand. Assisted Reproduction Technology Series No. 10. Cat. no. PER 39. Sydney: AIHW National Perinatal Statistics Unit, 2006.
科技部補助計畫衍生研發成果推廣資料表
日期:2014/10/27
科技部補助計畫
計畫名稱: 以家庭為中心之概念的縱貫性研究:探討接受人工生殖技術治療夫妻之產後憂 鬱(第二年)
計畫主持人: 李淑杏
計畫編號: 102-2410-H-040-002- 學門領域: 臨床與諮商心理學
無研發成果推廣資料
102 年度專題研究計畫研究成果彙整表
計畫主持人:李淑杏 計畫編號:102-2410-H-040-002-
計畫名稱:以家庭為中心之概念的縱貫性研究:探討接受人工生殖技術治療夫妻之產後憂鬱(第二年) 量化
成果項目 實際已達成
數(被接受 或已發表)
預期總達成 數(含實際已
達成數)
本計畫實 際貢獻百
分比
單位
備 註 ( 質 化 說 明:如 數 個 計 畫 共 同 成 果、成 果 列 為 該 期 刊 之 封 面 故 事 ...
等)
期刊論文 0 0 0%
研究報告/技術報告 0 1 100%
研討會論文 0 0 0%
論文著作 篇
專書 0 0 0%
申請中件數 0 0 0%
專利 已獲得件數 0 0 0% 件
件數 0 0 0% 件
技術移轉
權利金 0 0 0% 千元
碩士生 0 0 0%
博士生 0 0 0%
博士後研究員 0 0 0%
國內
參與計畫人力
(本國籍)
專任助理 0 0 0%
人次
期刊論文 2 1 0%
研究報告/技術報告 0 0 0%
研討會論文 1 1 0%
論文著作 篇
專書 0 0 0% 章/本
申請中件數 0 0 0%
專利 已獲得件數 0 0 0% 件
件數 0 0 0% 件
技術移轉
權利金 0 0 0% 千元
碩士生 0 0 0%
博士生 0 0 0%
博士後研究員 0 0 0%
國外
參與計畫人力
(外國籍)
專任助理 0 0 0%
人次
其他成果
(
無法以量化表達之成果如辦理學術活動、獲 得獎項、重要國際合 作、研究成果國際影響 力及其他協助產業技 術發展之具體效益事 項等,請以文字敘述填 列。)
本研究分析影響妻與夫長期產後憂鬱的預測因子,影響妻憂鬱程度長期變化的 相關因子為家庭經濟狀況(負相關;OR=0.680)、夫憂鬱程度(OR=1.266)、妻自 尊程度(負相關;OR=0.903)、妻親職壓力程度(OR=1.049)等四個變項。影響夫 憂鬱程度長期變化的相關因子為夫教育程度(正相關;OR=1.909)、妻憂鬱程度 (正相關;OR=1.247)、妻自尊程度(正相關;OR=1.025)、夫自尊程度(負相關;
OR=0.904)、夫親職壓力程度(正相關;OR=1.050)等五個變項。上述結果顯示產 後家庭妻與夫長期產後憂鬱乃互為影響,印證本研究之家庭理論架構,因此未 來應研擬以家庭為中心的介入措施提供產後夫妻合適的照護內容。
成果項目 量化 名稱或內容性質簡述
測驗工具(含質性與量性) 0
課程/模組 0
電腦及網路系統或工具 0
教材 0
舉辦之活動/競賽 0
研討會/工作坊 0
電子報、網站 0
科 教 處 計 畫 加 填 項
目 計畫成果推廣之參與(閱聽)人數 0