Management of Patients Requiring Prolonged Mechanical Ventilation
Tissot Low 1 , Yi-Jing Lin 2 , Chun-Lan Law 3 , and Chih-Bin Lin 1
1 Division of Chest Medicine, Department of Internal Medicine, 2 Department of Nursing,
3 Section of Respiratory Therapy, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation
Abstract
Advances in life-sustaining technologies in critical care have resulted in more survivors from cata- strophic illness, yet 4-13% of them fail weaning attempts, sometimes resulting in prolonged dependency on mechanical ventilation. This growing population has drawn much attention not only because of increased healthcare resource utilization, but also because of their poor quality of life and high mortality rate. The management of patients requiring prolonged mechanical ventilation should not be considered an extrapola- tion from mindsets and studies in the field of critical care. Specialized intermediate care units, respiratory care centers, have been established for comprehensive care of this population, and a growing body of literature in this field has emerged. In this review, we summarize the best available evidence for managing this specific group of patients, including weaning strategies, tracheostomy, nutritional support, and rehabilitation. We also summarize the clinical outcomes and prognostic information from studies based on data from the National Health Insurance Research Database of Taiwan, as this information is important in goal-of-care communica- tion and shared decision making concerning not sustaining ventilator dependency. (J Intern Med Taiwan 2017; 28: 24-32)
Key Words: Prolonged mechanical ventilation, Ventilator dependency, Respiratory care center
Introduction
Most patients receiving mechanical ventilation in intensive care units (ICUs) require short-term ventilation for less than a week. However, 4-13% of them fail weaning attempts, resulting in prolonged mechanical ventilation (PMV)
1,2. This population is rapidly increasing worldwide, likely because of an aging population with multiple comorbidi- ties, coupled with advances in life-sustaining tech- nologies in critical care
3-5. PMV is associated with high health care costs, morbidity, and mortality
1,2.
Because these “chronically critical ill” patients recover slowly, development of weaning facili- ties that are cost-effective and suited to the needs of these patients’ needs is required
6. In 2000, the Taiwan Bureau of National Health Insurance imple- mented a prospective payment system to deliver comprehensive care for patients requiring mechan- ical ventilation. This integrated delivery system offers cost-effective, outcome-oriented respiratory care services in a step-down manner: ICUs (acute stage, <21 days of mechanical ventilation); respira- tory care centers ( [RCC], for patients at a subacute
Reprint requests and correspondence:Dr. Chih-Bin Lin
Address:Division of Chest Medicine, Department of Internal Medicine, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, No. 707, Sec. 3, Chung-Yang Road, Hualien, 970, Taiwan,
stage for aggressive weaning, 21-42 days); respira- tory care wards (for patients at a chronic stage or requiring long-term care, >42 days); and homecare services (for patients at a stable stage during which they are visited routinely by a respiratory care team).
Definition of PMV
The most widely accepted consensus defini- tion of PMV is invasive mechanical ventilation for more than 21 consecutive days over 6 hours per day
7, although there is great variation in the dura- tion of mechanical ventilator use in different studies, ranging from 2 days to 4 weeks
7-9. The same con- sensus definition has been adopted by the National Health Insurance Administration of Taiwan.
Epidemiology
The number of PMV patients in Taiwan has increased significantly in the past decade, from 9,296 to 21,818 between 1998 and 2004. There was a slight drop after 2005
10. The incidence of PMV increased with aging, a finding consistent with studies in western countries
3,4. Patients over 85 years had the highest incidence rate. The cumulative incidence rate (from 17 to 85 years old) increased from 0.103 to 0.145 between 1998 and 2007, which indicates that an adult Taiwanese has a 10 to 15%
chance of requiring PMV by the age of 85 years
10.
Pathophysiology of ventilator dependence
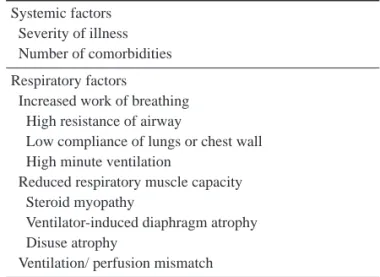
Failure of multiple weaning attempts usually signifies incomplete resolution of the disease that contributed to respiratory failure, however, the eti- ologies may be multifactorial, as categorized in Table 1. Physiological studies have demonstrated that prolonged ventilator dependence is associated with a marked imbalance in respiratory loads/capac- ities, resulting from excessive respiratory demands and reduced force-generating capacity of the inspi- ratory muscles
11-14. Recovery of maximum trans-
diaphragmatic pressure allows patients to breathe below the fatigue threshold of the diaphragm, which facilitates successful weaning later
12.
Patient selection and assessment
Patients who are expected to need the assistance of mechanical ventilation beyond 3 weeks of intuba-
Table 1. Etiologies associated with prolonged mechani- cal ventilation
Systemic factors Severity of illness Number of comorbidities Respiratory factors
Increased work of breathing High resistance of airway
Low compliance of lungs or chest wall High minute ventilation
Reduced respiratory muscle capacity Steroid myopathy
Ventilator-induced diaphragm atrophy Disuse atrophy
Ventilation/ perfusion mismatch Cardiovascular factors
High cardiac output due to increase work of breathing Increase afterload secondary to negative pleural pressure
swings
Increase venous return during spontaneous ventilation and pressure reduction
Metabolic factors Poor nutrition status
Overfeeding with elevated CO
2production Electrolyte imbalances with muscle weakness
(hypokalemia, hypophosphatemia) Hypothyroidism, myxedema Neurological factors
Impaired respiratory central drive Obstructive sleep apnea
Critical illness polyneuropathy Psychological factors
Fear of loss of life support Sleep deprivation Acute delirium,
Affective disorder: depression, anxiety Iatrogenic or caring factors
Failure to recognize withdrawal potential Inappropriate ventilator settings Absence of weaning protocols
Absence of sedation protocols; prolonged sedation
Inadequate nursing staffing
tion in an ICU should be considered for transfer to an RCC, which is specialized in respiratory care and aggressive ventilator liberation using an interdis- ciplinary team approach
15. A level of medical and respiratory stability should be met before admis- sion to an RCC. Patients should be hemodynami- cally stable with no need for invasive monitoring, no uncontrolled sepsis, hemorrhage, arrhythmia, or heart failure, and no anticipated surgical interven- tion in the near future
16. In addition to the patient’s current medical condition, the likelihood of even- tual weaning, quality of life, and life expectancy should also be assessed
6. Alternatives to ventilator dependency, such as time-limited weaning trials or palliative care, should be offered in family confer- ence when deliberating a post-ICU care plan
17.
Weaning strategies
Readiness for weaning should be assessed daily to determine whether patients fulfill the fol- lowing criteria: (1) reversal of the underlying cause of respiratory failure, (2) stable hemodynamic status, (3) reliable respiratory drive, and (4) adequate oxygenation (PaO
2/FiO
2>150-300, PEEP ≤5-10 cm H
2O, FiO
2≤0.4)
15. A commonly reported weaning strategy for patients requiring PMV involves two processes: (1) progressive reduction of assistance level, such as pressure support ventilation (PSV) and (2) progressive lengthening of the duration of spontaneous breathing trials (SBTs), usually beyond 120 minutes.
7Two randomized controlled studies compared different weaning methods in patients requiring PMV
18,19. A tracheostomy collar resulted in shorter time to wean than PSV (15 vs 19 days), although there were no significant differences in the 6 and 12-month survival
18. However, in another multicenter study comparing PSV and T-piece SBT using weaning protocols in patients with chronic obstructive lung disease (COPD), no significant differences were found in the time of ventilation (181±161 vs 130±106 h), weaning rate (73% vs 77%),
and mortality rate (11.5% vs 7.6%). When the results (using weaning protocols) were compared with his- torical usual practice, the time of ventilation was shorter (103±144 vs 170±127 h), and 30-day weaning rate was higher (87% vs 70%)
19. A study by Schein- horn et al. also showed significant benefits of using a therapist-implemented protocol, with a shorter weaning time (17 vs 29 days) in 252 patients requir- ing PMV over a 2-year period, compared with his- torical controls
20. Taken together, these studies suggest that implementation of a defined protocol may have a greater effect on weaning outcomes than the weaning strategy itself.
Predictors of weaning success
Research on weaning predictors has been
limited to observational, retrospective, and single-
institute-based studies. There is no single univer-
sally accepted weaning parameter which predicts
successful liberation from PMV
21. The rapid-shal-
low-breathing index (RSBI) with a threshold value
of 105, which has been widely used in the ICU,
had poor predictability for successful weaning in
patients requiring PMV (predictive accuracy 59%)
in one study. However, when the RSBI (using a
threshold value 130) was measured 2-3 hours after
SBT, the predictive accuracy improved to 92%
22. A
model was proposed to predict the chance of suc-
cessful weaning using a scoring system incorporat-
ing the alveolar arterial (A-a) gradient, blood urea
nitrogen and gender, with an accuracy of 70% in the
authors’ population of PMV patients
23. However,
later studies found that this model was no better than
chance in predicting weaning success
24. In a phys-
iological study, patients requiring PMV who were
successfully weaned showed significant improve-
ment in maximum transdiaphragmatic pressure
(Pdi
max), a better load/capacity ratio (Pdisw/Pdi
max)
and breathed below a fatigue threshold (tension-time
index of the diaphragm, TTdi), compared with the
unsuccessful weaning group
12. However, measure-
ment of these physiological indexes is too sophisti- cated for clinical use and a more practical surrogate should be developed.
Optimization for weaning
Tracheostomy
A tracheotomy is generally considered after failure of several weaning attempts and in patients who are expected to require PMV in the immediate future
15. However, the decision to perform a trache- ostomy should be made with caution before adequate goal-of-care communication has been conducted between clinicians and patients/ families, as the pro- cedure might increase the rate of unnecessary depen- dency on life-sustaining treatments
25. The potential benefits of tracheostomy include easier tracheal approach and suction, greater patient comfort with less sedative use, better communication, early mobi- lization, and improved lung mechanics and it facili- tates weaning from the ventilator
26,27. The optimal timing of tracheostomy in patients requiring PMV is still debated. Meta-analyses comparing early versus late or no tracheostomy did not show differ- ences in all-cause mortality at 1 year or long-term severe disability
28-32. Although early tracheostomy was associated with a shorter ICU stay and duration of mechanical ventilation, the total hospital stay was not reduced. The tracheotomy rate of PMV patients in Taiwan is about 60%
10, which is much lower than in studies conducted in western countries
33,34. This may be explained by common myths about trache- ostomy and ethnic Chinese culture which seek to avoid creating a stoma in patients with a short life expectancy.
Nutrition
The optimal nutritional intake in critically ill patients remains controversial. Some recent ran- domized trials demonstrated that intentional under- feeding for the first week in the ICU resulted in better short-term outcomes
35-37. In contrast, a large-
scale observational dataset showed that increased nutritional intake (>two-thirds of caloric prescrip- tion) was associated with a significant reduction in mortality
38. In a multicenter cohort study spe- cifically focusing on patients requiring PMV, ade- quate caloric intake as early as the first week of ICU stay was associated with better 6-month survival and faster physical recovery to 3 months
39. While some of the current guidelines recommend inten- tional underfeeding for the first week in the ICU, caution should be taken as this may cause harm in some high risk chronically ill patients, such as those requiring PMV.
Physical therapy
Patients requiring PMV are frequently decon- ditioned, possibly due to catastrophic illness, pro- longed immobilization, and adverse effects of medications
40,41. A randomized controlled study showed that a 6-week physical training program in patients requiring PMV resulted in improvements of limb and respiratory muscle strength (P
Imax, P
Emax), ventilator-free time, and functional status, compared with the control group
42. Although the mechanisms underlying the beneficial effects of physical training on respiration are not clear, strengthening exercises for the upper extremities may facilitate the actions of the pectoralis major, as well as other accessory respiratory muscles
43. A strategy of initiating physi- cal and occupational therapy in the earliest days of critical illness, coupled with discontinuation of sed- ative agents, resulted in better functional outcomes, a shorter duration of delirium, and more ventila- tor-free days
44. On the basis of these reports, early physiotherapy should be considered as an integral part of the management of patients requiring PMV.
Clinical outcomes and prognoses
In a meta-analysis of 124 studies from 16 coun-
tries, 50% (95% CI 47–53%) of PMV patients were
successfully liberated from mechanical ventila-
tion
45. However, successful weaning did not ensure long-term survival. While pooled mortality at hos- pital discharge was 29% (95% CI 26–32), more than half of these patients died within 1 year (pooled 1-year mortality 62%, 95% CI 57–67%)
45. This was possibly due to multiple underlying co-morbidities in patients with PMV. A population cohort study based on the National Health Insurance Research Database of Taiwan from 1998 to 2007 showed that the median survival of 50,481 PMV patients was 0.37 years, and overall life expectancy was 2.68 years
10. The prognosis was influenced by different underlying diseases, co-morbidities, and age. The life expectancies were shortest for PMV patients with chronic renal failure (1.32 years) and cancer (1.49 years), compared with degenerative neuro- logical diseases (4.08 years), stroke (3.32 years), liver cirrhosis (3.5 years), and injuries (6.19 years) (Table 2)
10,46. Among PMV patients with multiple co-morbidities, those with COPD survived longer than those with other co-morbidities. PMV patients over 85 years old had the shortest survival, with a median survival <4.6 months and life expectancy
<21.8 months, compared with younger age groups
10Approximately 62% of PMV patients had impair- ment of cognitive function. Even among PMV patients with fair to good cognitive function, more than 80% were confined to bed, had impaired self- care ability, and were dependent in activities of daily living. Taking these factors into account, the overall quality-adjusted life expectancy was only 0.3 to 0.4 years, while quality-adjusted life-years was 0.6 to 0.7 years
47,48.
Communication of goal-of-care planning
Although the outcomes of PMV are gener- ally poor, most patients and their surrogates in one prospective observational study expressed over- optimistic expectations in terms of 1-year survival (93%), functional status (71%), and quality of life
(83%)
49. Meanwhile, up to three-quarters of surro- gates reported receiving no prognostic information on PMV from their clinicians
49. In another ques- tionnaire-based prospective study
17, more than half of surrogates reported receiving no information on majority topics (10 out of 18 items) which were con- sidered essential for communication and decision making in goal-of-care planning for patients with PMV, including 1-year survival (93%), expected functional status (80%), alternatives to continu- ing mechanical ventilation (83%), services needed after discharge (82%), and financial burden (75%).
Deficiency in communication between clinicians and patients/surrogates may cause inappropriate use of life-sustaining treatment, although the decision may be inconsistent with the preferences of patients or surrogates
50. Since an optimal clinical decision takes into account both evidence-based information and the patient’s goals, values and preferences, the majority of critical care organizations recommend shared decision- making (SDM) as a model when practicing patient-centered care, particularly when making value-laden decisions and defining overall goals of care (including decisions on time-limited weaning trials and timing of palliative care)
51-54. Table 2 provides useful evidence-based prognostic information for PMV patients in Taiwan, including life expectancy and quality-adjusted life expectancy (which take cognitive function into account), as well as lifetime financial burden (health care costs and out-of-pocket expenses for family)
46. This infor- mation, along with specific weaning outcomes for individual RCCs, should be provided to patients/
surrogates in SDM in goal-of-care communication.
Conclusion
Advances in mechanical ventilation in critical
care have saved lives from catastrophic illnesses,
but on the other hand, have created a new health-
care problem of prolonged dependency on mechani-
cal ventilation. Although the prognosis is generally
Table 2*. Life expectancy, lifetime cost and cost per QALY (quality-adjusted life year) for patients requiring PMV in Taiwan
Single specific disease Life expectancy (years)
Quality-adjusted life expectancy
Lifetime cost (10 thousand TWD)
Cost per QALY (10 thousand TWD) Partial
cognition
Poor cognition
Healthcare cost
Out of pocket
Partial cognition
Poor cognition
Cancer 1.49 0.46 0.20 46.0 40.5 188.0 432.3
Renal failure 1.32 0.40 0.18 70.5 35.5 265.0 588.9
Liver cirrhosis 3.50 1.15 0.50 57.0 94.6 131.9 303.4
Degenerative nerve diseases 4.08 1.28 0.56 228.4 107.2 262.2 599.3
Parkinson’s diseases 2.01 0.59 0.26 129.9 50.7 306.1 694.6
Trauma 6.19 2.04 0.89 125.1 165.0 142.3 326.1
Stroke 3.32 1.05 0.46 123.3 87.0 200.3 457.1
<65 years 5.24 1.60 0.72 158.9 137.9 185.5 412.2
65-74 years 2.93 1.14 0.40 125.9 75.9 177.0 504.5
75-84 years 2.03 0.61 0.27 116.5 52.2 276.6 624.9
>85 years 1.42 0.49 0.21 87.3 36.3 252.2 588.5
Intracranial or spinal injury 6.19 2.04 0.89 125.2 165.0 142.3 326.1
<65 years 10.06 3.40 1.47 165.2 270.0 128.0 269.1
65-74 years 3.71 1.18 0.51 111.2 97.1 176.5 408.3
75-84 years 2.64 0.82 0.33 97.0 68.9 202.4 502.9
>85 years 1.51 0.52 0.22 87.8 38.7 243.2 574.8
COPD <65 years 5.18 1.66 0.72 172.2 136.2 185.8 428.3
65-74 years 2.49 0.76 0.33 107.3 64.5 226.1 520.7
75-84 years 2.05 0.63 0.28 94.3 53.7 235.0 528.8
>85 years 1.46 0.42 0.19 77.7 37.5 274.1 605.9
Heart diseases <65 yrs 4.97 1.61 0.70 137.2 132.1 167.3 384.7
65-74 years 2.49 0.77 0.34 89.9 65.4 201.6 456.6
75-84 years 1.78 0.54 0.24 75.2 46.6 225.6 507.5
>85 years 1.43 0.41 0.18 72.7 36.8 266.9 608.0
Septicemia/shock <65 years 4.42 1.22 0.64 80.8 118.1 163.0 310.7
65-74 years 2.08 0.65 0.28 72.2 54.7 195.2 453.1
75-84 years 1.60 0.49 0.22 65.2 42.4 219.5 488.8
>85 years 1.07 0.31 0.14 55.8 33.2 287.0 635.6
Cases >2 specific diseases 2.90 0.93 0.40 93.4 76.8 183.0 425.5
Cancer and renal failure 1.14 0.36 0.16 67.5 31.3 274.5 617.6
Cancer and others 1.82 0.58 0.26 57.4 48.9 183.4 409.2
Renal failure and others 1.65 0.52 0.23 77.6 45.0 235.7 532.8
* modified under permission
46.
poor, this population represents a heterogeneous group of patients who need to be managed individ- ually. We recommend a patient-centered, outcome- oriented approach. For patients with substantial weaning potential, a protocolized weaning process of daily SBTs integrated with early rehabilitation and nutritional intervention may facilitate stepwise liberation from PMV. For those with multiple failed weaning attempts, alternatives to ventilator depen- dency, such as time-limited weaning trials, a shift to noninvasive positive pressure ventilation, or pal- liative care, should be offered to patients and their surrogates, using SDM when making a goal-of-care plan. As prognostic information and long-term out- comes of PMV become available, they should be pro- vided in family conference, along with information on medical expenses and resources needed after dis- charge. Well-designed multicenter randomized trials are needed to assess the results of specific interven- tions, such as weaning strategies, nutritional inter- vention, and physical therapy. Models with better predictive power which assess weaning potential and long-term outcomes are required for communi- cation and decision making. Basic research on the pathophysiology of PMV, such as ventilator-induced diaphragm dysfunction and critical illness polyneu- ropathy, are essential in the development of preven- tive strategies.
References
1. Nevins ML, Epstein SK. Weaning from prolonged mechanical ventilation. Clin Chest Med 2001; 22:13-33.
2. Lone NI, Walsh TS. Prolonged mechanical ventilation in crit- ically ill patients: epidemiology, outcomes and modelling the potential cost consequences of establishing a regional weaning unit. Crit Care 2011; 15: R102.
3. Needham DM, Bronskill SE, Sibbald WJ, Pronovost PJ, Lau- pacis A. Mechanical ventilation in Ontario, 1992-2000: inci- dence, survival, and hospital bed utilization of noncardiac surgery adult patients. Crit Care Med 2004; 32: 1504-9.
4. Carson SS, Cox CE, Holmes GM, Howard A, Carey TS. The changing epidemiology of mechanical ventilation: a popula- tion-based study. J Intensive Care Med 2006; 21: 173-82.
5. Carson SS. Outcomes of prolonged mechanical ventilation.
Curr Opin Crit Care 2006; 12: 405-11.
6. Nelson JE, Cox CE, Hope AA, Carson SS. Chronic critical illness. Am J Respir Crit Care Med 2010; 182: 446-54.
7. MacIntyre NR, Epstein SK, Carson S, Scheinhorn D, Chris- topher K, Muldoon S. Management of patients requiring pro- longed mechanical ventilation: report of a NAMDRC consen- sus conference. Chest 2005; 128: 3937-54.
8. Chelluri L, Im KA, Belle SH, et al. Long-term mortality and quality of life after prolonged mechanical ventilation. Crit Care Med 2004; 32: 61-9.
9. Gracey DR, Naessens JM, Krishan I, Marsh HM. Hospital and posthospital survival in patients mechanically ventilated for more than 29 days. Chest 1992; 101: 211-4.
10. Hung MC, Lu HM, Chen L, et al. Life expectancies and inci- dence rates of patients under prolonged mechanical ventila- tion: a population-based study during 1998 to 2007 in Taiwan.
Crit Care 2011; 15: R107.
11. Epstein SK. Decision to extubate. Intensive Care Med 2002;
28: 535-46.
12. Carlucci A, Ceriana P, Prinianakis G, Fanfulla F, Colombo R, Nava S. Determinants of weaning success in patients with prolonged mechanical ventilation. Crit Care 2009; 13: R97.
13. Purro A, Appendini L, De Gaetano A, Gudjonsdottir M, Donner CF, Rossi A. Physiologic determinants of ventilator dependence in long-term mechanically ventilated patients.
Am J Respir Crit Care Med 2000; 161: 1115-23.
14. Chao DC, Scheinhorn DJ. Weaning from mechanical ventila- tion. Crit Care Clin 1998; 14: 799-817, viii.
15. MacIntyre NR, Cook DJ, Ely EW, Jr., et al. Evidence-based guidelines for weaning and discontinuing ventilatory support:
a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine.
Chest 2001; 120: 375S-95S.
16. Make BJ, Hill NS, Goldberg AI, et al. Mechanical ventilation beyond the intensive care unit. Report of a consensus con- ference of the American College of Chest Physicians. Chest 1998; 113: 289S-344S.
17. Nelson JE, Mercado AF, Camhi SL, et al. Communication about chronic critical illness. Arch Intern Med 2007; 167:
2509-15.
18. Jubran A, Grant BJ, Duffner LA, et al. Effect of pressure support vs unassisted breathing through a tracheostomy collar on weaning duration in patients requiring prolonged mechani- cal ventilation: a randomized trial. JAMA 2013; 309: 671-7.
19. Vitacca M, Vianello A, Colombo D, et al. Comparison of two methods for weaning patients with chronic obstructive pul- monary disease requiring mechanical ventilation for more than 15 days. Am J Respir Crit Care Med 2001; 164: 225-30.
20. Scheinhorn DJ, Chao DC, Stearn-Hassenpflug M, Wallace WA. Outcomes in post-ICU mechanical ventilation: a thera- pist-implemented weaning protocol. Chest 2001; 119: 236-42.
21. Huang CT, Yu CJ. Conventional weaning parameters do not predict extubation outcome in intubated subjects requiring prolonged mechanical ventilation. Respir Care 2013; 58:
1307-14.
22. Krieger BP, Isber J, Breitenbucher A, Throop G, Ershowsky P.
Serial measurements of the rapid-shallow-breathing index as
a predictor of weaning outcome in elderly medical patients.
Chest 1997; 112: 1029-34.
23. Scheinhorn DJ, Hassenpflug M, Artinian BM, LaBree L, Catlin JL. Predictors of weaning after 6 weeks of mechanical ventilation. Chest 1995; 107: 500-5.
24. Scheinhorn DJ, Chao DC, Stearn-Hassenpflug M. Liberation from prolonged mechanical ventilation. Crit Care Clin 2002;
18: 569-95.
25. Cox CE, Carson SS, Holmes GM, Howard A, Carey TS.
Increase in tracheostomy for prolonged mechanical ventila- tion in North Carolina, 1993-2002. Crit Care Med 2004; 32:
2219-26.
26. Kurek CJ, Cohen IL, Lambrinos J, Minatoya K, Booth FV, Chalfin DB. Clinical and economic outcome of patients undergoing tracheostomy for prolonged mechanical ventila- tion in New York state during 1993: analysis of 6,353 cases under diagnosis-related group 483. Crit Care Med 1997; 25:
983-8.
27. Stauffer JL, Olson DE, Petty TL. Complications and conse- quences of endotracheal intubation and tracheotomy. A pro- spective study of 150 critically ill adult patients. Am J Med 1981; 70: 65-76.
28. Siempos, II, Ntaidou TK, Filippidis FT, Choi AM. Effect of early versus late or no tracheostomy on mortality and pneu- monia of critically ill patients receiving mechanical ventila- tion: a systematic review and meta-analysis. Lancet Respir Med 2015; 3: 150-8.
29. Griffiths J, Barber VS, Morgan L, Young JD. Systematic review and meta-analysis of studies of the timing of tracheos- tomy in adult patients undergoing artificial ventilation. BMJ 2005; 330: 1243.
30. Dunham CM, Ransom KJ. Assessment of early tracheostomy in trauma patients: a systematic review and meta-analysis.
Am Surg 2006; 72: 276-81.
31. Durbin CG, Jr., Perkins MP, Moores LK. Should tracheos- tomy be performed as early as 72 hours in patients requir- ing prolonged mechanical ventilation? Respir Care 2010; 55:
76-87.
32. Wang F, Wu Y, Bo L, et al. The timing of tracheotomy in criti- cally ill patients undergoing mechanical ventilation: a system- atic review and meta-analysis of randomized controlled trials.
Chest 2011; 140: 1456-65.
33. Scheinhorn DJ, Hassenpflug MS, Votto JJ, et al. Post-ICU mechanical ventilation at 23 long-term care hospitals: a mul- ticenter outcomes study. Chest 2007; 131: 85-93.
34. Esteban A, Anzueto A, Alia I, et al. How is mechanical ven- tilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med 2000; 161:
1450-8.
35. Rice TW, Mogan S, Hays MA, Bernard GR, Jensen GL, Wheeler AP. Randomized trial of initial trophic versus full- energy enteral nutrition in mechanically ventilated patients with acute respiratory failure. Crit Care Med 2011; 39:
967-74.
36. Rice TW, Wheeler AP, Thompson BT, et al. Initial trophic vs full enteral feeding in patients with acute lung injury: the EDEN randomized trial. JAMA 2012; 307: 795-803.
37. Casaer MP, Mesotten D, Hermans G, et al. Early versus late parenteral nutrition in critically ill adults. N Engl J Med 2011;
365: 506-17.
38. Heyland DK, Cahill N, Day AG. Optimal amount of calories for critically ill patients: depends on how you slice the cake!
Crit Care Med 2011; 39: 2619-26.
39. Wei X, Day AG, Ouellette-Kuntz H, Heyland DK. The Asso- ciation Between Nutritional Adequacy and Long-Term Outcomes in Critically Ill Patients Requiring Prolonged Mechanical Ventilation: A Multicenter Cohort Study. Crit Care Med 2015; 43: 1569-79.
40. Moodie LH, Reeve JC, Vermeulen N, Elkins MR. Inspiratory muscle training to facilitate weaning from mechanical ven- tilation: protocol for a systematic review. BMC Res Notes 2011; 4: 283.
41. De Jonghe B, Sharshar T, Lefaucheur JP, et al. Paresis acquired in the intensive care unit: a prospective multicenter study. JAMA 2002; 288: 2859-67.
42. Chiang LL, Wang LY, Wu CP, Wu HD, Wu YT. Effects of physical training on functional status in patients with pro- longed mechanical ventilation. Phys Ther 2006;86:1271-81.
43. Criner GJ. Care of the patient requiring invasive mechanical ventilation. Respir Care Clin N Am 2002; 8: 575-92.
44. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet 2009; 373: 1874-82.
45. Damuth E, Mitchell JA, Bartock JL, Roberts BW, Trzeciak S.
Long-term survival of critically ill patients treated with pro- longed mechanical ventilation: a systematic review and meta- analysis. Lancet Respir Med 2015; 3: 544-53.
46. Hung MC, Lu HM, Chen L, et al. Cost per QALY (quality- adjusted life year) and lifetime cost of prolonged mechanical ventilation in Taiwan. PLoS One 2012; 7: e44043.
47. Hung MC, Yan YH, Fan PS, et al. Measurement of quality of life using EQ-5D in patients on prolonged mechanical venti- lation: comparison of patients, family caregivers, and nurses.
Qual Life Res 2010; 19: 721-7.
48. Hung MC, Yan YH, Fan PS, et al. Estimation of quality- adjusted life expectancy in patients under prolonged mechan- ical ventilation. Value Health 2011; 14: 347-53.
49. Cox CE, Martinu T, Sathy SJ, et al. Expectations and out- comes of prolonged mechanical ventilation. Crit Care Med 2009; 37: 2888-94; quiz 904.
50. Teno JM, Fisher E, Hamel MB, et al. Decision-making and outcomes of prolonged ICU stays in seriously ill patients. J Am Geriatr Soc 2000; 48: S70-4.
51. Thompson BT, Cox PN, Antonelli M, et al. Challenges in end- of-life care in the ICU: statement of the 5th International Con- sensus Conference in Critical Care: Brussels, Belgium, April 2003: executive summary. Crit Care Med 2004; 32: 1781-4.
52. Carlet J, Thijs LG, Antonelli M, et al. Challenges in end-of- life care in the ICU. Statement of the 5th International Con- sensus Conference in Critical Care: Brussels, Belgium, April 2003. Intensive Care Med 2004; 30: 770-84.
53. Davidson JE, Powers K, Hedayat KM, et al. Clinical practice guidelines for support of the family in the patient-centered
intensive care unit: American College of Critical Care Medi- cine Task Force 2004-2005. Crit Care Med 2007; 35: 605-22.
54. Lanken PN, Terry PB, Delisser HM, et al. An official Ameri-
can Thoracic Society clinical policy statement: palliative care for patients with respiratory diseases and critical illnesses.
Am J Respir Crit Care Med 2008; 177: 912-27.
長期使用呼吸器病患之處置
劉迪塑1 林宜靜2 羅春蘭3 林智斌1
佛教慈濟醫療財團法人花蓮慈濟醫院
1
內科部胸腔內科2
護理部3
呼吸治療組摘 要