Effect of Liraglutide on Patients with Type 2 Diabetes in Real Practice: Experience from
A Regional Hospital
Bao-Mei Wang
1, Wen-Ya Ma
1, and Ching-Chieh Su
1,
2,31Division of Endocrinology and Metabolism, Department of Internal Medicine, Cardinal Tien Hospital, Xindian, New Taipei City, Taiwan;
2School of Medicine, 3Graduate Institute of Applied Science and Engineering, Fu Jen Catholic University, New Taipei City, Taiwan
Abstract
Liraglutide is a new injectable anti-diabetic medicine. It can lower blood glucose and also result in a neutral or lowered body weight. However, the interaction of changes in blood glucose and body weight is not clear. This study is a retrospective chart review study. Patients with type 2 diabetes who initiated liraglutide therapy from 1, Sep. 2016 to 30 Nov. 2016 were enrolled. We assessed the change in blood glucose and body weight after liraglutide treatment. Results: The study found that most patients had lower A1C and body weight simultaneously but no relationship between body weight and blood glucose change was found. In multivari- able linear regression models, variables such as male, diabetes duration, and baseline A1C are all positively correlated and numbers of anti-diabetic drugs is negatively correlated to the change of A1C. Age is positively correlated and the number of anti-diabetic drugs is negatively correlated to body weight change. We found that liraglutide could decrease body weight and blood glucose. However, there is no relationship between the glucose reduction and body weight lowering effects. In respect of glucose reduction, male patients with longer diabetes durations, using less oral anti-diabetic drugs or higher baseline A1C are good candidates for liraglutide treatment. In respect of body weight reduction, younger patients with more anti-diabetic drugs are less likely to lose their body weight. (J Intern Med Taiwan 2020; 31: 202-209)
Key Words: Liraglutide, Type 2 diabetes, Body weight change
Introduction
Type 2 diabetes is not only a growing epidemic in all ages but also all around the globe1. It can cause tremendous economic loss from both medical expenditures and reduced productivity. The largest components of medical expenditures are hospital inpatient care2. Fortunately, the economic loss can
be minimized since diabetes complications can be reduced if it is controlled well3,4. However, the effect of anti- diabetic agents cannot last long because the progressive loss of beta cell function of type 2 dia- betes5. Accordingly, many kinds of anti- diabetic agents were developed in the last two decades6.
Traditionally, insulin resistance was thought to be the main characteristic of type 2 diabetes. But
Reprint requests and correspondence:Dr. Ching-Chieh Su
Address:Division of Endocrinology and Metabolism, Department of Internal Medicine, Cardinal Tien Hospital, Xindian, No 362,Zhongzheng Rd. Xindian District, New Taipei City, 231 Taiwan
then more and more defections of type 2 diabetes were found7. Reduced incretin effect in type 2 dia- betes is one of the defections8. Dipeptidyl peptidase 4 (DPP-4) inhibitors and glucagon-like peptide 1 receptor agonists (GLP-1 RA) both target incretin effects. However, these new drugs are expensive.
Therefore, choosing the appropriate one will be an important issue in both treating diabetes efficiently and reducing medical cost.
In this retrospective study, we tried to find the characteristics of type 2 diabetes patients who have better responses to liraglutide.
Materials and Methods
Study participants
The present study was done at the diabetes outpatient clinic of Cardinal Tien hospital. Ethical approval was given by the Cardinal Tien hospital.
The electronic medical records were reviewed from 1 Sep. 2016 to 30 Nov. 2016 and all patients with type 2 diabetes who used liraglutide de novo were enrolled. Patients who had no regular follow up or didn’t use liraglutide for 1 year were excluded.
Data management
The demographics and laboratory data of all patients were collected and analyzed. The changes of body weight and A1C were represented by per- centages of reduction from the baseline. Percentage of reduction was calculated as below: Percentage of body weight reduction (%)= (the lowest body weight after liraglutide- body weight at baseline)/
body weight at baseline) x 100 x (-1). Percentage of A1C reduction (%)= (the lowest A1C after liraglu- tide- A1C at baseline)/A1C at baseline) x 100) x (-1)
The therapeutic agents were classified into 6 classes of OAD and insulin. The regimen was recorded according to medical charts before and after liraglutide add-on.
Statistical analysis
Continuous variables that were distributed normally are presented as means (SD). Due to the small sample size, continuous variables were ana- lyzed with a nonparametric test or were analyzed after logarithmic transformations. The distribution of continuous variables was examined by the Sha- piro-Wilk test. Categorical variables are reported as the percentage of patients in the subgroup. The Wilcoxon rank-sum (Mann-Whitney) test and chi- square test were used to identify the differences in clinical characteristics by gender. Pearson’s corre- lation coefficients were used to determine the rela- tionship between the change of body weight and the change to A1C and clinical characteristics. A multivariate linear regression model was used for adjusting percentage reduction with other vari- ables. The relationship between A1C and body weight change were illustrated in scatter plots and analyzed by linear regression. Figures and graphs were performed using GraphPad Prism 6 for Windows (GraphPad Software Inc., San Diego, CA, USA). A 2-tailed p-value below 0.05 was con- sidered significant. Stata/SE 14.0 for Windows (StataCorp LP, College Station, TX) was used for statistical analyses.
Results
A total of 65 patients were screened and 45 patients were included in the analysis. Baseline characteristics were shown in table 1. Of those 45 patients, those who are female are slightly more than those who are male. The body weight index and other factors such as biochemistry and blood pressure are similar. In table 2, the medication used before lira- glutide were summarized. Most than 90% of patients were on metformin. Besides, more than three-quar- ters of patients were using more than 2 kinds of oral anti- diabetic drugs because of the reimbursement policy of the national health insurance.
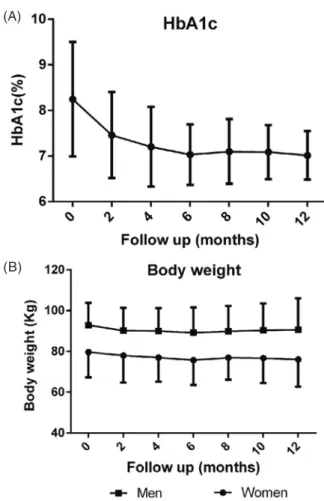
In terms of the glucose lowering effect of lira-
glutide, A1C decreased progressively and reached the nadir (-1.22%) at 12 months (Figure 1a). In terms of the body weight losing effect, body weight lost from 85.0 ± 13.4 kg at baseline to 81.3 ± 13.8 kg at 6 months (-3.7 kg) and 83.1 ± 15.8 kg at 12 months (-1.9 kg).
For men, A1C decreased from 8.49 ± 1.67%
to 7.11 ± 0.47% at 12 months and body weight lost from 92.9 ± 10.9 kg to 89.3kg ± 12.4 kg at 6 months and 90.7kg ± 15.3kg at 12 months. For women, A1C
Table 1. Patient demographics and baseline character- istics. Data are expressed as mean ± standard deviation. HDL-C high density lipoprotein cho- lesterol, LDL-C low density lipoprotein choles- terol, GPT glutamic-pyruvic transaminase
N 45
Age 57.6 ± 10.8
Diabetes duration (year) 10.2 ± 4.8
Body height (cm) 163.2 ± 8.9
Body weight (Kg) 85.0 ± 13.4
Body mass index 30.9 ± 8.9
Systolic blood pressure (mmHg) 132.4 ± 14.7 Diastolic blood pressure (mmHg) 76.1 ± 9.3
HbA1c (%) 8.24 ± 1.3
Fasting plasma glucose (mg/dL) 161.2 ± 57.6 Postprandial plasma glucose (mg/dL) 216.9 ± 72.3 Total cholesterol (mg/dL) 162.9 ±30.1
Triglyceride (mg/dL) 167.3 ± 66.6
HDL-C (mg/dL) 43.7 ± 11.1
LDL-C (mg/dL) 93.8 ± 29.6
GPT 39.3 ± 22.4
creatinine 0.88 ± 0.24
eGFR 87.9 ± 25.2
urine albumin-creatinine ratio 83.8 ± 209.1 Complication
Diabetic neuropathy 15.5%
Diabetic nephropathy 28.8%
Diabetic retinopathy 22.2 %
Comorbidities
Coronary artery disease 6.6%
Stroke 0%
Figure 1. (a) A1C change during 12 months liraglutide treatment period. (b) Body weight change during 12 months liraglutide treatment period.
(A)
(B)
Table 2. Baseline therapeutic regimens. Most patients (86.67%) use 2 or 3 kinds of OADs at baseline.
OAD oral anti-diabetic drugs, SU sulfonylureas, DPP4 Dipeptidyl peptidase, TZD thiazolidinedi- one, AGI alpha glucosidase inhibitor
Medication N (%)
Metformin 43 (95.56%)
SU 31 (68.89%)
Glinides 3 (6.67%)
DPP4 inhibitor 6 (13.33%)
TZD 23 (51.11%)
AGI 8 (17.78%)
Basal insulin 6 (13.33%)
Statin 41 (91.11%)
One OAD + insulin 3 (6.67%)
Two OADs + insulin 12 (26.67%)
Three OADs + insulin 27 (60%)
Four OADs + insulin 3 (6.67%)
decreased from 8.08 ± 0.87% to 6.92 ± 0.60% at 12 months and body weight lost from 79.7 ± 12.4 kg to 75.8kg ± 12.1 kg at 6 months and 76.1kg ± 13.3kg at 12 months. No significant difference was noted between men and women (-2.2 kg vs -3.6 kg at 12 months) (Figure 1b). Then we analyzed the rela- tionship between body weight and glucose lower- ing effect. Most patients had both lowered A1C and body weight simultaneously, but some were gaining weight with better glucose control and some were losing weight with worse glucose control (Figure 2a).
Then we analyzed the relationship between glucose reduction and body weight lowering effect. There is no relationship between them (Figure 2b).
Univariate correlations of A1C and body
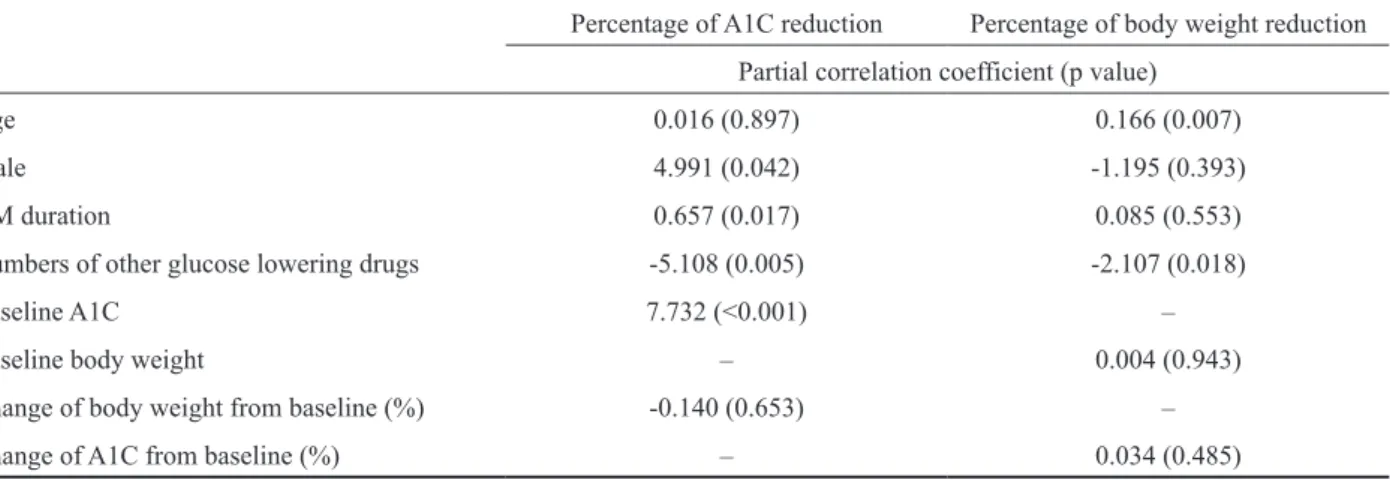
weight change were done. Baseline A1C was nega- tively correlated to the change of A1C. Age, gender, duration of diabetes, numbers of oral anti- diabetic drugs, baseline body weight and BMI are not cor- related to change of A1C. In terms of the change of body weight, younger patients lost more body weight. The number of anti- diabetic drugs showed a trend of being correlated to body weight change (Table 3). In multivariable linear regression models, we found that being male, diabetes duration, and baseline A1C are all positively correlated and the number of anti- diabetic drugs is negatively corre- lated to change of A1C. Age is positively correlated and the number of anti -diabetic drugs is negatively correlated to body weight change (Table 4).
Table 3. Univariate correlations of the percentage reduction of A1C the body weight change between various factors. BMI body mass index
Percentage of A1C reduction Percentage of body weight reduction
ra p r p
Age -0.0942 0.5382 0.4382 0.0026
Male 0.2264 0.1347 -0.2559 0.0898
DM duration 0.0037 0.9809 0.2109 0.1643
Numbers of other glucose lowering drugs -0.0968 0.527 -0.2845 0.0582
Baseline A1C b 0.7798 <0.001 -0.2191 0.1481
Baseline body weight 0.089 0.5611 -0.2417 0.1097
Baseline BMI -0.1508 0.3595 0.0423 0.7983
a Pearson correlation coefficient.
b Log-transformed for normality.
Figure 2. (a) Relationship of A1C and body weight change. (b) Linear regression of A1C and body weight change.
(A) (B)
Discussion
In our study, we found that both A1C and body weight decreased after liraglutide use. In addition to glucose reduction, body weight reduction is also important in treating diabetes. Obesity or body weight gain is associated with insulin resistance and development of type 2 diabetes9. Non-esteri- fied fatty acids, proinflammatory cytokines and other hormones or factors are released from adipose tissue of obese individuals. Insulin resistance devel- ops and abnormal glucose intolerance, even diabetes appears thereafter10. When obese patients become diabetes patients and receives some kinds of anti- diabetes drugs, like sulfonylurea, thiazolidinedi- one, blood glucose improves along with the cost of body weight gain6. Therefore, some anti-diabetic drugs, like GLP-1 RAs or sodium-glucose co-trans- porter 2 (SGLT2) inhibitors, are promising when they become clinically available since they can both decrease body weight and blood glucose at the same time11.
In liraglutide effect and action in diabe- tes (LEAD) studies, A1C decreases from -0.6% to -1.5% under 1.2 mg liraglutide and body weight changes from +0.3kg to -2.6 kg 12-17. Body weight gain only appears when liraglutide is not combined with metformin in LEAD-1 SU study12. In LEAD studies, the duration is usually 26 weeks except in LEAD-3 study, which is 52 weeks. No correla-
tion analysis between body weight change and A1C reduction were made in LEAD studies. In the Diabe- tes Therapy Utilization: Research Changes in A1C, Weight and Other factors Through Intervention with Exenatide Once Weekly (DURATION) studies, the long-acting release (LAR) formation of exena- tide decreases body weight from -2.0 to -4.4 kg and A1C from -1.28 to -1.6% in around 6 months treat- ment18-23. In DURATION 3, the association of base- line body weight and A1C change or body weight change was analyzed. The baseline body weight was not associated with either body weight change or A1C change20. In Assessment of Weekly Adminis- tration of dulaglutide in Diabetes (AWARD) studies, dulaglutide weekly injection decreases A1C from -0.62 to -1.48%. Body weight changes from 0.9 kg to -2.9 kg. Body weight gains in the end of AWARD 1 where dulaglutide is combined with pioglitazone and AWARD4 where rapid-acting insulin is used with dulaglutide24-29. The association between body weight change and A1C reduction was not calcu- lated. In our study, most patients do lose their body weight and decrease their blood glucose in the same time. However, there is no correlation between body weight loss and blood glucose lowering. Patients who have more blood glucose reduction do not have more body weight reduction, and vice versa.
In AWARD studies, the study duration ranges from 52 weeks to 104 weeks. In AWARD studies,
Table 4. Multivariable linear regression models for the A1C and body weight reduction
Percentage of A1C reduction Percentage of body weight reduction Partial correlation coefficient (p value)
Age 0.016 (0.897) 0.166 (0.007)
Male 4.991 (0.042) -1.195 (0.393)
DM duration 0.657 (0.017) 0.085 (0.553)
Numbers of other glucose lowering drugs -5.108 (0.005) -2.107 (0.018)
Baseline A1C 7.732 (<0.001) –
Baseline body weight – 0.004 (0.943)
Change of body weight from baseline (%) -0.140 (0.653) –
Change of A1C from baseline (%) – 0.034 (0.485)
A1C decreased and reached their nadir at 13 to 26 weeks and became progressively higher in the study period. In DURATION studies, A1C reached their nadir at around 12-16 weeks and became stable or slightly higher afterwards. In LEAD studies, A1C also reached the nadir at around 12-16 weeks and became stable or slightly higher, too. In our study, the A1C reached the nadir at 24 weeks and also kept stable or slightly higher till 52 weeks. Therefore, physicians should be aware of the timeline of A1C change and intensify their therapy if A1C is not at the goal after 24 weeks treatment ofliraglutide.
Choosing the right medicine for patients is always critical. Precision medicine for diabetes is well established in monogenic diabetes30. Pharma- cogenetics in type 2 diabetes is still underdevel- oped31. Therefore clinical characteristics are still important clues we can currently use for choosing the right patient with the right medicine. For pre- diction of glucose lowering effect of liraglutide, we found patients who are male, with shorter diabetes duration and higher baseline A1c benefit more after liraglutide therapy and patients who are using more kinds of anti-diabetic drugs benefit less. In terms of body weight lost, patients who are younger and using less oral anti-diabetic drugs will lose more body weight after liraglutide injection.
There are some limitations in our study. First, the study population is small and the males and females were not equal in numbers. Secondly, the observation period is only 12 months. Thirdly, our study is retrospective.
In conclusion, in our one-year retrospec- tive study, we find liraglutide could decrease body weight and blood glucose. However, there is no relationship between glucose reduction and body weight lowering effect. In terms of glucose reduc- tion, patients who are male, with longer diabetes duration or higher baseline A1C are good candidates for liraglutide treatment and patients who use more kinds of anti-diabetic drugs are not. In respect of
body weight reduction, patients who are younger or use more kinds of anti-diabetic drugs are less likely to lose their body weight.
Acknowledgement
The study is supported by Cardinal Tien hospi- tal (No. CTH-104-1-2A15).
Disclosure
The authors declare that there are no conflicts of interest. C.C Su has received lecture/advisor fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novartis, NovoNordisk and Sanofi.
References
1. Hu FB. Globalization of diabetes: the role of diet, lifestyle, and genes. Diabetes Care 2011;34:1249-57.
2. American Diabetes Association. Economic costs of diabetes in the U.S. in 2007. Diabetes Care 2008;31:596-615.
3. The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;
329:977-86.
4. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin com- pared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;
352:837-53.
5. Maedler K, Donath MY. Beta-cells in type 2 diabetes: a loss of function and mass. Horm Res 2004;62 (Suppl 3):67-73.
6. American Diabetes Association. 8. Pharmacologic approaches to glycemic treatment. Diabetes Care 2017; 40(Suppl 1):
S64-S74.
7. Defronzo RA. Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes 2009;58:773-95.
8. Nauck M, Stockmann F, Ebert R, Creutzfeldt W. Reduced incretin effect in type 2 (non-insulin-dependent) diabetes.
Diabetologia 1986;29:46-52.
9. Willett WC, Dietz WH, Colditz GA. Guidelines for healthy weight. N Engl J Med 1999;341(6):427-34.
10. Kahn SE, Hull RL, Utzschneider KM. Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature 2006;
444:840-46.
11. McGill JB. Insights from the Liraglutide Clinical Develop- ment Program--the Liraglutide Effect and Action in Diabetes (LEAD) studies. Postgrad Med 2009;121:16-25.
12. Marre M, Shaw J, Brandle M, et al. Liraglutide, a once-daily human GLP-1 analogue, added to a sulphonylurea over 26
weeks produces greater improvements in glycaemic and weight control compared with adding rosiglitazone or placebo in subjects with Type 2 diabetes (LEAD-1 SU). Diabet Med 2009; 26(3): 268-78.
13. Nauck M, Frid A, Hermansen K, et al. Efficacy and safety comparison of liraglutide, glimepiride, and placebo, all in combination with metformin, in type 2 diabetes: the LEAD (liraglutide effect and action in diabetes)-2 study. Diabetes Care 2009;32:84-90.
14. Garber A, Henry R, Ratner R, et al. Liraglutide versus glime- piride monotherapy for type 2 diabetes (LEAD-3 Mono): a randomised, 52-week, phase III, double-blind, parallel-treat- ment trial. Lancet 2009;373:473-81
15. Zinman B, Gerich J, Buse JB, et al. Efficacy and safety of the human glucagon-like peptide-1 analog liraglutide in combi- nation with metformin and thiazolidinedione in patients with type 2 diabetes (LEAD-4 Met+TZD). Diabetes Care 2009;
32:1224-30.
16. Russell-Jones D, Vaag A, Schmitz O, et al. Liraglutide vs insulin glargine and placebo in combination with met- formin and sulfonylurea therapy in type 2 diabetes mellitus (LEAD-5 met+SU): a randomised controlled trial. Diabetolo- gia 2009;52:2046-55.
17. Buse JB, Rosenstock J, Sesti G, et al. Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6). Lancet 2009;374:39-47.
18. Kim D, MacConell L, Zhuang D, et al. Effects of once-weekly dosing of a long-acting release formulation of exenatide on glucose control and body weight in subjects with type 2 dia- betes. Diabetes Care 2007;30:1487-93.
19. Bergenstal RM, Wysham C, Macconell L, et al. Efficacy and safety of exenatide once weekly versus sitagliptin or piogl- itazone as an adjunct to metformin for treatment of type 2 diabetes (DURATION-2): a randomised trial. Lancet 2010;
376:431-39.
20. Diamant M, Van Gaal L, Stranks S, et al. Once weekly exena- tide compared with insulin glargine titrated to target in patients with type 2 diabetes (DURATION-3): an open-label randomised trial. Lancet 2010;375:2234-43.
21. Russell-Jones D, Cuddihy RM, Hanefeld M, et al. Efficacy and safety of exenatide once weekly versus metformin, piogl- itazone, and sitagliptin used as monotherapy in drug-naive patients with type 2 diabetes (DURATION-4): a 26-week double-blind study. Diabetes Care 2012;35:252-58.
22. Blevins T, Pullman J, Malloy J, et al. DURATION-5: exena- tide once weekly resulted in greater improvements in glyce- mic control compared with exenatide twice daily in patients with type 2 diabetes. J Clin Endocrinol Metab 2011;96:1301- 10.
23. Buse JB, Nauck M, Forst T, et al. Exenatide once weekly versus liraglutide once daily in patients with type 2 diabe- tes (DURATION-6): a randomised, open-label study. Lancet 2013;381:117-24.
24. Wysham C, Blevins T, Arakaki R, et al. Efficacy and safety of dulaglutide added onto pioglitazone and metformin versus exenatide in type 2 diabetes in a randomized controlled trial (AWARD-1). Diabetes Care 2014;37:2159-67.
25. Giorgino F, Benroubi M, Sun JH, Zimmermann AG, Pech- tner V. Efficacy and safety of once-weekly dulaglutide versus insulin glargine in patients with type 2 diabetes on metformin and glimepiride (AWARD-2). Diabetes Care 2015;38:2241- 49.
26. Umpierrez G, Tofe Povedano S, Perez Manghi F, Shurzinske L, Pechtner V. Efficacy and safety of dulaglutide monother- apy versus metformin in type 2 diabetes in a randomized con- trolled trial (AWARD-3). Diabetes Care 2014;37:2168-76.
27. Blonde L, Jendle J, Gross J, et al. Once-weekly dulaglu- tide versus bedtime insulin glargine, both in combination with prandial insulin lispro, in patients with type 2 diabetes (AWARD-4): a randomised, open-label, phase 3, non-inferi- ority study. Lancet 2015;385:2057-66.
28. Weinstock RS, Guerci B, Umpierrez G, Nauck MA, Skrivanek Z, Milicevic Z. Safety and efficacy of once-weekly dula- glutide versus sitagliptin after 2 years in metformin-treated patients with type 2 diabetes (AWARD-5): a randomized, phase III study. Diabetes Obes Metab 2015;17:849-58.
29. Dungan KM, Povedano ST, Forst T, et al. Once-weekly dulaglutide versus once-daily liraglutide in metformin- treated patients with type 2 diabetes (AWARD-6): a ran- domised, open-label, phase 3, non-inferiority trial. Lancet 2014;384:1349-57.
30. Hattersley AT, Patel KA. Precision diabetes: learning from monogenic diabetes. Diabetologia 2017;60:769-77.
31. Florez JC. Pharmacogenetics in type 2 diabetes: precision medicine or discovery tool? Diabetologia 2017;60:800-07.
第二型糖尿病病人使用胰妥善成效評估
王寶妹1 馬文雅1 蘇景傑1,2,3
1財團法人天主教新店耕莘醫院 內科及新陳代謝內分泌科 輔仁大學 2醫學系 3應用科學及工程研究所
摘 要
胰妥善為一種較新型的注射型降血糖藥物。它除了降血糖以外甚至有 降體重的效果。目
前對於類升糖素胜肽-1受體的促效劑使用上作用於血糖和體重變化之間的交互作用目前還不
是很清楚。本研究是病歷回顧研究,回顧從2016年9月1日至2016年11月30日期間,有使用
胰妥善( 一種類升糖素胜肽 -1受體的促效劑 ) 的第二型糖尿病病人列入評估。回顧其使用胰妥
善後的血糖及體重變化。其中大部份的病人糖化血色素和體重同時下降,但體重及糖化血色 素下降幅度之間並無相關。在多元線性回歸模型分析變數發現,第二型糖尿病病人使用胰妥 善治療後糖化血色素的下降幅度和某些變數,例如男性、糖尿病罹病時間長短及初始糖化血 色素值,呈現正相關;但和降血糖藥物數目多寡呈現負相關。至於治療後體重變化,則與使
用年齡呈正相關,但降血糖藥物數目呈負相關。我們發現胰妥善(liraglutide) 可以使血糖及體
重下降,然而血糖下降幅度及體重下降幅度之間並無呈現出相關性。關於血糖下降此研究發 現、男性病患、糖尿病發病時間較長、相對少使用降血糖藥物或初期糖化血色素高的病患是 適合使用胰妥善的候選人。在體重下降方面,則是年輕人合併使用降血糖藥物數目多者,其 體重下降機會較低。