Title: Association of Copy Number Variation in Fc gamma receptor IIIb gene with risk of Graves’ Ophthalmopathy
The name of Authors: Wen-Ling Liao1*, Yu-Huei Liu2, 3*, Lei Wan2, 4, 5, Chwen-Tzuei Chang6,7, Ching-Chu Chen6,7, Fuu-Jen Tsai2, 4, 5,8
Author’s Affiliations:1 Center for Personalized Medicine, China Medical University Hospital, Taichung, Taiwan; 2Department of Medical Research and Medical Genetics, China Medical University Hospital, Taichung, Taiwan; 3Graduate Institute of
Integrated Medicine, China Medical University, Taichung, Taiwan; 4School of Chinese Medicine, China Medical University, Taichung, Taiwan; 5Department of Health and Nutrition Biotechnology, Asia University, Taichung, Taiwan; 6Division of Endocrinology and Metabolism, Department of Medicine, China Medical University Hospital, Taichung, Taiwan; 7Department of Endocrinology and Metabolism, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 8Department of Pediatrics, China Medical University Hospital, Taichung, Taiwan
*Wen-Ling Liao and Yu-Huei Liu contributed equally to this work.
Corresponding author Fuu-Jen Tsai, MD, PhD.
Department of Medical Genetics, Pediatrics and Medical Research, China Medical University Hospital
No.2 Yuh-Der Road, 404 Taichung, Taiwan
Telephone: 886-4-22062121 Ext 2041; Fax: 886-4-22033295 E-mail: [email protected] 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Abstract
Background The functional polymorphism that explains the established association of Fc gamma receptor IIIb (FCGR3B) with Graves’ disease (GD) and Graves’ ophthalmopathy (GO) remains unidentified, but copy number variation (CNV) might be relevant. The aim of this study was to determine whether CNV for FCGR3B is associated with GD and GO.
Methods A total of 624 GD patients, including 397 without GO (GDnonGO) and 227 with GO (GDGO), and 160227 healthy controls were enrolled in this case-control study. The relative copy number (CN) of FCGR3B was determined using a relative real-time quantitative polymerase chain reaction.
Results The distribution of the relative CN of FCGR3B significantly differ between the GDGO patients and the healthy controls (p = 0.03 0.02) but no difference between the total GD patientsand the healthy controls (p = 0.14 0.06). Individuals with less than 2 CN and more than 2 CN of FCGR3B were at significantly decreased risk of developing GDGO. In addition, GD patients with less than 2 copies of FCGR3B were at reduced risk for developing nodular hyperplasia and vitiligo, but at increased risk for myxedema.
Conclusions: The data provide new information that CNV of FCGR3B is associated with the development or progression of GD in Taiwan Chinese population.
Keywords
Copy number variation, Fc gamma receptor IIIb gene, Graves’ disease, Graves’ ophthalmopathy 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48
Introduction
Graves’ disease (GD) is an autoimmune disease characterized by
hyperthyroidism, diffuse goiter, thyroid-specific autoantibodies with or without Graves’ ophthalmopathy (GO), and dermopathy due to the circulating autoantibodies 1. GO is the most common extrathyroid manifestation of GD and affects 25%–50% of GD patients 2-5. Approximately 28% of patients with GO present with severe disease, with restricted mobility, diplopia, keratopathy, and optic neuropathy 6-7. Numerous functionally relevant single-nucleotide polymorphism (SNP) variants have been characterized in GD and GO, although none have yet proven causative 8. Other forms of variation that might affect gene expression should also be considered.
Copy number variation (CNV) is recognized as a common form of genomic variation in which DNA segments (>1 kb) are presented in a variable number of copies compared to a reference genome. A CNV caused by genomic rearrangements such as deletions, duplications, inversions, and translocations may contribute to alteration of gene expression and subsequent phenotypic variation, which results in susceptibility or resistance to disease 9-11. CNV has also been associated with autism 12-15, schizophrenia 16-19, cancer 20-25, and autoimmune disease 11; 26-30.
Fc gamma receptor IIIB (FCGR3B; the CD16 cell surface immunoglobulin receptor), located on chromosome 1q23, is a low-affinity IgG receptor that binds with IgG complexes at the Fc region31. FCGR3B belongs to the Fc gamma receptor family, which contributes to the regulation of acquired and innate immunity31. Studies have showed that a lower copy number of FCGR3B can increase susceptibility to systemic autoimmune diseases such as systemic lupus erythematosus and other autoimmune disorders27. Although there have been major advances in understanding the genetic basis of GD 27, the association between CNV in FCGR3B and GO remains unclear. In 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73
the present study, the variant in the FCGR3B gene that may explain theassociation between, and the physiological impact of, CNV in this region and the development of GD and GO was found.
Materials and Methods Subjects
A disease group with 624 patients with a confirmed diagnosis of GD and an appropriate control group with 160227 healthy volunteers with matched gender according to the female predominance of GD including 32 male (20.0%) and 128 female (80.0%) at China Medical University Hospital in Taiwan were enrolled and actively followed. The methods of diagnosis of GD and classification of GO were as previously described 32. All individuals classifiedas affected were interviewed and examined by experienced clinicians. Demographic and clinical characteristics of 624 patients with GD were summarized in Table 1. The study was approved by the institutional review board and the ethics committee of China Medical University Hospital. Written informed consent was obtained from each participants in
accordance with institutional requirement and the Declaration of Helsinki Principles.
Genomic DNA extraction
The genomic DNA was extracted from peripheral blood leukocytes of
participants using the Genomic DNA kit (Qiagen) according to the manufacturer’s instructions. Aware of the quantitative polymerase chain reaction (qPCR) technical is sensitive to small variations in DNA quality33, the quality of each genomic DNA was verified on an agarose gel and the template DNA were freshly diluted from 200μg/ml stock and used within 2 weeks.
74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99
Analysis of FCGR3B copy number variants
The relative CN of the FCGR3B gene in each individual was estimated using a relative real-time qPCR method that is suited to Larger-scale genotyping. This method has been tested and proven to provide reliable results. Specific primers and TaqMan® probes (Assay ID: Hs04211858_cn) for FCGR3B and for a reference gene RNase P
(RNaseP part number 4403326) were purchased from ABI Biosciences (Applied Biosystems, Foster City, CA, USA). The TaqMan® probes for FCGR3B and RNase P were labeled with FAMTM and VIC®, respectively. Polymerase chain reactions were run on an ABI 9700 machine. Amplification reactions (15 μl) were carried out using genomic DNA (10 ng), TaqMan® Copy Number Reference Assay for FCGR3B and RNase P, and TaqMan® Master Mix. Thermal cycling was initiated with an initial denaturation step of 10 min at 95°C, followed by 40 cycles each of 15 sec at 95°C and of 1 min at 60°C. A dissociationprocedure was performed to generate a melting curve for the confirmationof amplification specificity. The relative FCGR3B CN for each individual was estimated using the2-Ct method (where Ct is cycle threshold, -ΔCt = (Ctgene - Ctreference) as describedpreviously 34. The PCR products were quantified in triplicate, and the standard deviation (SD) and coefficient of variation (CV) were calculated based on 3 runs. To control for reaction quality, each reaction plate also included a calibrator, a positive control, and a no-template control (NTC). Data from a plate were included if the calibrator CV was less than 5%, the positive control CV and sample CVs were all less than 10%, and the NTC was negative. To include across-plate data, the CVs of the positive control had to be similar and the NTC had to be negative.
Statistical analysis
Significance of the differences between the distributions of FCGR3B CN in 100 101 102 103 104 105 106 107 108 109 110 111 112 113 114 115 116 117 118 119 120 121 122 123 124 125
cases and controls was estimated by Chi square test or fisher exact test. Odds ratios (OR) and confidence intervals (CI) were estimated by logistic regression models using SPSS 12.0. The CN equal to two (CN = 2) was chosen as reference category for FCGR3B.To estimate OR, bins of CN were grouped as 0-1 CNs for FCGR3B (<2 category), 3-5 CN for FCGR3B (>2 category). We estimated the risk of acquiring disease associated with CNs for FCGR3B categories by comparing them with a reference CN category. For each of these categories, an OR >1 indicates a detrimental effect of CNV on disease susceptibility, and OR <1 indicates a protective effect of CNV.
Results
Correlation between CNV of FCGR3B and the development of GD and GO
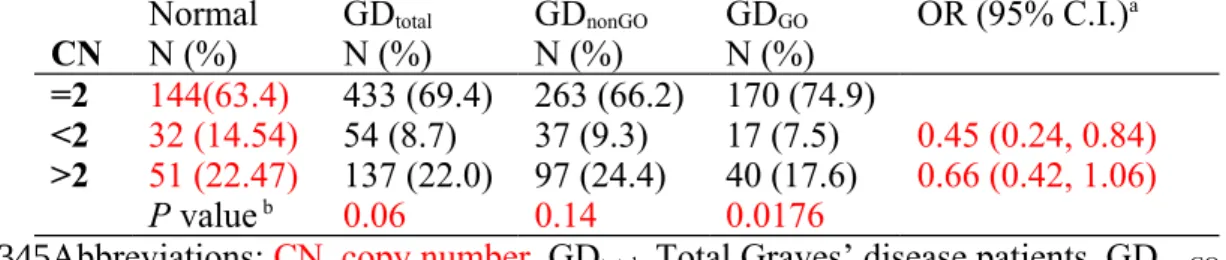
The distribution of FCGR3B copy number (CN) according to the presence of GD or GO is summarized in Table 12. The distribution of FCGR3B CN was not
statistically significant different between health controls and GD (p = 0.140.06). Further, we separated GD patients into 2 groups according to GO status. The distribution of FCGR3B CN was significantly differeddifferent between healthy control and GDGO patients (p = 0.030.0176) but not with GDnonGO patients (p =
0.400.14). Results revealed that individuals with less than 2 copies and more than 2 copies of FCGR3B were at significantly decreased risk of developing GDGO when compared individuals with 2 copies of FCGR3B (odds ratio (OR) = 0.480.45, 95% confidence interval (C.I.): 0.24, 0.950.24, 0.84and OR = 0.600.66, 95% C.I.: 0.36, 1.000.42, 1.06 for CN<2 and CN>2, respectively) (Table 12). However, tThe result (control vs. GDGO patients) was on the borderline of statistical significant after bonfferoni correction (p = 0.0540.0352). Regression analysis with or without gender and age as covariates did not affect the significance of the reported association results. 126 127 128 129 130 131 132 133 134 135 136 137 138 139 140 141 142 143 144 145 146 147 148 149 150 151
The results suggest that FCGR3B CNV might not be associated with the development or progression of GD, but could be associated with the development or progression of GDGO.
Correlations between CNVs of FCGR3B and clinical phenotypes
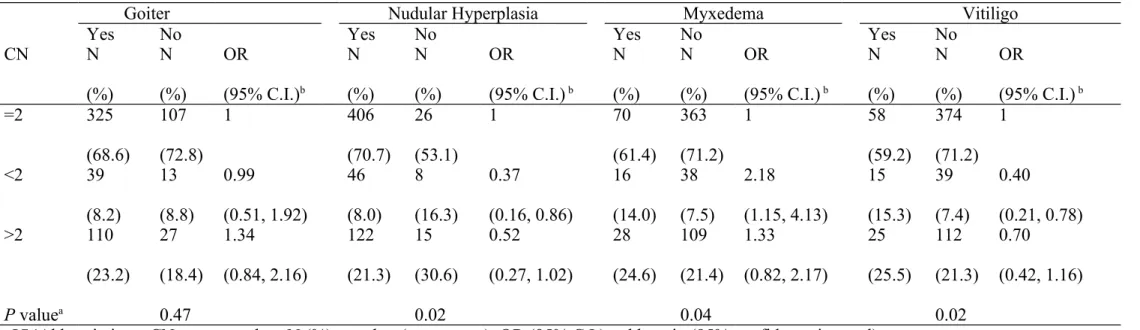
The association between clinical features of GD patients and CNV of FCGR3B was analyzed. The results are summarized in Table 23. No significant difference for FCGR3B CNV was found between GD patients and different stages of goiter (p = 0.47). Interestingly, the distribution of FCGR3B CNV significantly differed between GD patients with different patterns of nodular hyperplasia (p = 0.02), myxedema (p = 0.04), and vitiligo (p = 0.02). As shown in Table 23, individuals with less than 2 copies of FCGR3B were at reduced risk for the development of nodular hyperplasia (OR = 0.37, 95% C.I.: 0.16, 0.86) and vitiligo (OR = 0.40, 95% CI: 0.21, 0.78), but at increased risk for myxedema (OR = 2.18, 95% C.I.: 1.15, 4.13) compared with individuals with 2 copies of FCGR3B.
Discussion
Several functionally relevant SNP variants are characteristic of GD and GDGO 8, but few studies have demonstrated an association between CNV and GD 27; 35-36. Here, we found that CNV in FCGR3B significantly differs between GDGO patients and healthy controls. Individuals with more or fewer than 2 copies of FCGR3B may have reduced susceptibility to GDGO. In addition, our data showed the protective effect of
FCGR3B CNV on GD which was consistent with previous studies in the Caucasian
population 27, although the results in both studies did not reach the statistical
significance. The sample size of this study did not reach 80% power for the given effect size and is a limitation. In addition, the genetic backgrounds of ethnically
152 153 154 155 156 157 158 159 160 161 162 163 164 165 166 167 168 169 170 171 172 173 174 175 176 177
diverse populations should be considered. In Niederer et al.37 identified significant
differences in FCGR3B CNV distribution among Caucasian, East Asian, and Kenyan population. Therefore, confirmation of these results by studies with larger sample sizes and in different population is warranted. Mamtani et al.26 observed that both low and high FCGR3B CN might contribute to an autoimmune phenotype compared to 2 CN. Moreover, GD patients with 2 copies of FCGR3B are at significantly increased risk for the development of nodular hyperplasia and vitiligo, but at reduced risk for myxedema.
FCGR3B, which is expressed by neutrophils and eosinophils, functionally links the humoral and cellular branches of the immune system and plays an important role in the activation and modulation of the immune response 31. FCGR3B CNV correlates with protein expression, soluble serum FcγRIIIb, neutrophil uptake of and adherence to immune complexes, andmacrophage overactivity 38. Dysregulation of FcγRIIIb expression may contribute to the impaired clearance of immune complexes. In GD/GDGO, in which immune complexes may not play an important role, the relation betweeen FCGR3B CNV, FCGR3B expression, and neutrophil activation may require further investigation.
More, FCGR3B CNV could play a different role, which may involve other co-regulatory genes, in the development of systemic and organ-specific autoimmunity. An association between low FCGR3B CNV and systemic lupus erythematosus has been reported in Caucasians 27. However, anti-neutrophil cytoplasmic antibody-associated systemic vasculitis, an autoimmune disease in which immune complex deposition plays only a minor role, seems to be diversely associated with FCGR3B CN 27. Also, linkage disequilibrium between multi-allelic FCGR3B CNV and SLE-associated SNPs in the FCGR locus was defined 37. However, the associations 178 179 180 181 182 183 184 185 186 187 188 189 190 191 192 193 194 195 196 197 198 199 200 201 202
between NA1/NA2 allelic variant of FCGR3B with GO or GD in our study were not significant (p value>0.05). Further study of the genetic interaction between FCGR3B and other genes, such as FCGR2A, FCGR2B, and complement receptor 3 (CR3) should be considered.
In summary, this study suggests that FCGR3B CNV is associated with the development or progression of GD and GO, thereby providing new information on the implications of FCGR3B CNV in patients with GD.
Acknowledgement s
This study was supported by research grants CMU-98-asia-04 from China Medical University, Taichung, Taiwan and 98-2320-B-039-008-MY3 from National Science Council, Taipei, Taiwan.
References
1. Mishra, A., and Mishra, S.K. (2001). Multicentre study of thyroid nodules in patients with Graves' disease (Br J Surg 2000; 87: 1111-13). Br J Surg 88, 313.
2. Gianoukakis, A.G., Khadavi, N., and Smith, T.J. (2008). Cytokines, Graves' disease, and thyroid-associated ophthalmopathy. Thyroid 18, 953-8. 3. Perros, P., Neoh, C., and Dickinson, J. (2009). Thyroid eye disease. BMJ 338,
b560.
4. Kuriyan, A.E., Phipps, R.P., and Feldon, S.E. (2008). The eye and thyroid disease. Curr Opin Ophthalmol 19, 499-506.
5. Khoo, T.K., and Bahn, R.S. (2007). Pathogenesis of Graves' ophthalmopathy: the role of autoantibodies. Thyroid 17, 1013-8.
6. Kloprogge, S., Kowal, L., Wall, J., and Frauman, A.G. (2005). The clinicopathologic basis of Graves' ophthalmopathy: a review. Eur J Ophthalmol 15, 315-23.
7. Bartalena, L. (2005). Editorial: glucocorticoids for Graves' ophthalmopathy: how and when. J Clin Endocrinol Metab 90, 5497-9.
8. Bednarczuk, T., Gopinath, B., Ploski, R., and Wall, J.R. (2007). Susceptibility 203 204 205 206 207 208 209 210 211 212 213 214 215 216 217 218 219 220 221 222 223 224 225 226 227 228 229 230 231 232 233
genes in Graves' ophthalmopathy: searching for a needle in a haystack? Clin Endocrinol (Oxf) 67, 3-19.
9. Zhang, F., Gu, W., Hurles, M.E., and Lupski, J.R. (2009). Copy number variation in human health, disease, and evolution. Annu Rev Genomics Hum Genet 10, 451-81.
10. Wain, L.V., Armour, J.A., and Tobin, M.D. (2009). Genomic copy number variation, human health, and disease. Lancet 374, 340-50.
11. Schaschl, H., Aitman, T.J., and Vyse, T.J. (2009). Copy number variation in the human genome and its implication in autoimmunity. Clin Exp Immunol 156, 12-6.
12. Glessner, J.T., Wang, K., Cai, G., Korvatska, O., Kim, C.E., Wood, S., Zhang, H., Estes, A., et al. (2009). Autism genome-wide copy number variation reveals ubiquitin and neuronal genes. Nature 459, 569-73.
13. Maestrini, E., Pagnamenta, A.T., Lamb, J.A., Bacchelli, E., Sykes, N.H., Sousa, I., Toma, C., Barnby, G., et al. (2010). High-density SNP association study and copy number variation analysis of the AUTS1 and AUTS5 loci implicate the IMMP2L-DOCK4 gene region in autism susceptibility. Mol Psychiatry 15, 954-68.
14. Noor, A., Gianakopoulos, P.J., Fernandez, B., Marshall, C.R., Szatmari, P., Roberts, W., Scherer, S.W., and Vincent, J.B. (2009). Copy number variation analysis and sequencing of the X-linked mental retardation gene
TSPAN7/TM4SF2 in patients with autism spectrum disorder. Psychiatr Genet 19, 154-5.
15. Sykes, N.H., Toma, C., Wilson, N., Volpi, E.V., Sousa, I., Pagnamenta, A.T., Tancredi, R., Battaglia, A., et al. (2009). Copy number variation and association analysis of SHANK3 as a candidate gene for autism in the IMGSAC collection. Eur J Hum Genet 17, 1347-53.
16. St Clair, D. (2009). Copy number variation and schizophrenia. Schizophr Bull 35, 9-12.
17. Sutrala, S.R., Goossens, D., Williams, N.M., Heyrman, L., Adolfsson, R., Norton, N., Buckland, P.R., and Del-Favero, J. (2007). Gene copy number variation in schizophrenia. Schizophr Res 96, 93-9.
18. Sutrala, S.R., Norton, N., Williams, N.M., and Buckland, P.R. (2008). Gene copy number variation in schizophrenia. Am J Med Genet B Neuropsychiatr Genet 147B, 606-11.
19. Tam, G.W., Redon, R., Carter, N.P., and Grant, S.G. (2009). The role of DNA copy number variation in schizophrenia. Biol Psychiatry 66, 1005-12.
20. Liu, W., Sun, J., Li, G., Zhu, Y., Zhang, S., Kim, S.T., Wiklund, F., Wiley, K., et 234 235 236 237 238 239 240 241 242 243 244 245 246 247 248 249 250 251 252 253 254 255 256 257 258 259 260 261 262 263 264 265 266 267 268 269 270 271
al. (2009). Association of a germ-line copy number variation at 2p24.3 and risk for aggressive prostate cancer. Cancer Res 69, 2176-9.
21. Shlien, A., Tabori, U., Marshall, C.R., Pienkowska, M., Feuk, L., Novokmet, A., Nanda, S., Druker, H., et al. (2008). Excessive genomic DNA copy number variation in the Li-Fraumeni cancer predisposition syndrome. Proc Natl Acad Sci U S A 105, 11264-9.
22. Nielsen, K.V., Ejlertsen, B., Moller, S., Jorgensen, J.T., Knoop, A., Knudsen, H., and Mouridsen, H.T. (2008). The value of TOP2A gene copy number
variation as a biomarker in breast cancer: Update of DBCG trial 89D. Acta Oncol 47, 725-34.
23. Venkatachalam, R., Ligtenberg, M.J., Hoogerbrugge, N., Geurts van Kessel, A., and Kuiper, R.P. (2008). Predisposition to colorectal cancer: exploiting copy number variation to identify novel predisposing genes and mechanisms. Cytogenet Genome Res 123, 188-94.
24. Tchatchou, S., and Burwinkel, B. (2008). Chromosome copy number variation and breast cancer risk. Cytogenet Genome Res 123, 183-7.
25. Speleman, F., Kumps, C., Buysse, K., Poppe, B., Menten, B., and De Preter, K. (2008). Copy number alterations and copy number variation in cancer: close encounters of the bad kind. Cytogenet Genome Res 123, 176-82.
26. Mamtani, M., Anaya, J.M., He, W., and Ahuja, S.K. (2010). Association of copy number variation in the FCGR3B gene with risk of autoimmune diseases. Genes Immun 11, 155-60.
27. Fanciulli, M., Norsworthy, P.J., Petretto, E., Dong, R., Harper, L., Kamesh, L., Heward, J.M., Gough, S.C., et al. (2007). FCGR3B copy number variation is associated with susceptibility to systemic, but not organ-specific,
autoimmunity. Nat Genet 39, 721-3.
28. Zhou, X.J., Lv, J.C., Bu, D.F., Yu, L., Yang, Y.R., Zhao, J., Cui, Z., Yang, R., et al. (2010). Copy number variation of FCGR3A rather than FCGR3B and FCGR2B is associated with susceptibility to anti-GBM disease. Int Immunol 22, 45-51.
29. McKinney, C., Fanciulli, M., Merriman, M.E., Phipps-Green, A., Alizadeh, B.Z., Koeleman, B.P., Dalbeth, N., Gow, P.J., et al. (2010). Association of variation in Fcgamma receptor 3B gene copy number with rheumatoid arthritis in Caucasian samples. Ann Rheum Dis 69, 1711-6.
30. Marques, R.B., Thabet, M.M., White, S.J., Houwing-Duistermaat, J.J., Bakker, A.M., Hendriks, G.J., Zhernakova, A., Huizinga, T.W., et al. (2010). Genetic variation of the Fc gamma receptor 3B gene and association with rheumatoid arthritis. PLoS One 5.
272 273 274 275 276 277 278 279 280 281 282 283 284 285 286 287 288 289 290 291 292 293 294 295 296 297 298 299 300 301 302 303 304 305 306 307 308 309
31. Li, X., Ptacek, T.S., Brown, E.E., and Edberg, J.C. (2009). Fcgamma receptors: structure, function and role as genetic risk factors in SLE. Genes Immun 10, 380-9.
32. Liao, W.L., Chen, R.H., Lin, H.J., Liu, Y.H., Chen, W.C., Tsai, Y., Wan, L., and Tsai, F.J. (2011). The association between polymorphisms of B7 molecules (CD80 and CD86) and Graves' ophthalmopathy in a Taiwanese population. Ophthalmology 118, 553-7.
33. Field, S.F., Howson, J.M., Maier, L.M., Walker, S., Walker, N.M., Smyth, D.J., Armour, J.A., Clayton, D.G., et al. (2009). Experimental aspects of copy number variant assays at CCL3L1. Nat Med 15, 1115-7.
34. Livak, K.J., and Schmittgen, T.D. (2001). Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 25, 402-8.
35. Lv, J., Yang, Y., Zhou, X., Yu, L., Li, R., Hou, P., and Zhang, H. (2010). FCGR3B copy number variation is not associated with lupus nephritis in a Chinese population. Lupus 19, 158-61.
36. Huber, A.K., Concepcion, E.S., Gandhi, A., Menconi, F., Smith, E.P., Keddache, M., and Tomer, Y. (2011). Analysis of Immune Regulatory Genes' Copy Number Variants in Graves' Disease. Thyroid 21, 69-74.
37. Niederer, H.A., Willcocks, L.C., Rayner, T.F., Yang, W., Lau, Y.L., Williams, T.N., Scott, J.A., Urban, B.C., et al. (2010). Copy number, linkage
disequilibrium and disease association in the FCGR locus. Hum Mol Genet 19, 3282-94.
38. Willcocks, L.C., Lyons, P.A., Clatworthy, M.R., Robinson, J.I., Yang, W., Newland, S.A., Plagnol, V., McGovern, N.N., et al. (2008). Copy number of FCGR3B, which is associated with systemic lupus erythematosus, correlates with protein expression and immune complex uptake. J Exp Med 205, 1573-82. 310 311 312 313 314 315 316 317 318 319 320 321 322 323 324 325 326 327 328 329 330 331 332 333 334 335 336 337 338 339
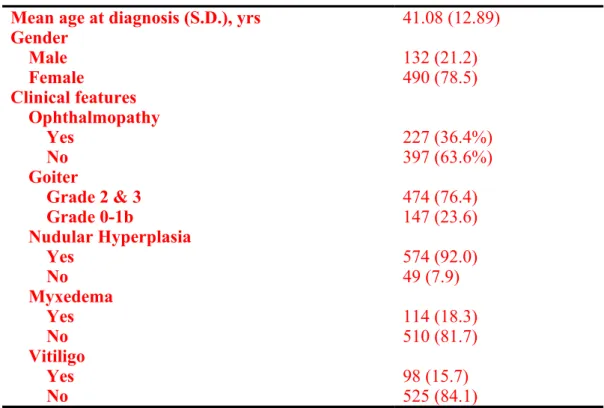
Table 1. Demographic and Clinical Characteristics of 624 patients with Graves’ Disease.
Mean age at diagnosis (S.D.), yrs 41.08 (12.89)
Gender Male 132 (21.2) Female 490 (78.5) Clinical features Ophthalmopathy Yes 227 (36.4%) No 397 (63.6%) Goiter Grade 2 & 3 474 (76.4) Grade 0-1b 147 (23.6) Nudular Hyperplasia Yes 574 (92.0) No 49 (7.9) Myxedema Yes 114 (18.3) No 510 (81.7) Vitiligo Yes 98 (15.7) No 525 (84.1)
Abbreviations: S.D., standard deviation; yrs, years
340 341
Table 12.The distribution of FCGR3B copy number in normal, and Graves’ disease with or without ophthalmopathy.
Normal GDtotal GDnonGO GDGO OR (95% C.I.)a
CN N (%) N (%) N (%) N (%)
=2 144(63.4) 433 (69.4) 263 (66.2) 170 (74.9)
<2 32 (14.54) 54 (8.7) 37 (9.3) 17 (7.5) 0.45 (0.24, 0.84)
>2 51 (22.47) 137 (22.0) 97 (24.4) 40 (17.6) 0.66 (0.42, 1.06)
P value b 0.06 0.14 0.0176
Abbreviations: CN, copy number. GDtotal, Total Graves’ disease patients. GDnonGO, Graves’ disease patients without ophthalmopathy. GDGO, Graves’ disease patients with ophthalmopathy. N (%), number (percentage). OR (95%C.I.), odds ratio (95% confidence interval).
a Odds ratio and 95% C.I. were estimated by applying unconditional logistic regression when compared GDGO with normal control.
b P value was calculated by chi square test (2x3 tables) and were considered significant when the value less than 0.05.
343 344 345 346 347 348 349 350 351 352
Table 23. Estimated risk of several phenotypes of Graves’ disease according to FCGR3B gene copy number.
Goiter Nudular Hyperplasia Myxedema Vitiligo
Yes No Yes No Yes No Yes No
CN N (%) N (%) OR (95% C.I.)b N (%) N (%) OR (95% C.I.) b N (%) N (%) OR (95% C.I.) b N (%) N (%) OR (95% C.I.) b =2 325 (68.6) 107 (72.8) 1 406 (70.7) 26 (53.1) 1 70 (61.4) 363 (71.2) 1 58 (59.2) 374 (71.2) 1 <2 39 (8.2) 13 (8.8) 0.99 (0.51, 1.92) 46 (8.0) 8 (16.3) 0.37 (0.16, 0.86) 16 (14.0) 38 (7.5) 2.18 (1.15, 4.13) 15 (15.3) 39 (7.4) 0.40 (0.21, 0.78) >2 110 (23.2) 27 (18.4) 1.34 (0.84, 2.16) 122 (21.3) 15 (30.6) 0.52 (0.27, 1.02) 28 (24.6) 109 (21.4) 1.33 (0.82, 2.17) 25 (25.5) 112 (21.3) 0.70 (0.42, 1.16) P valuea 0.47 0.02 0.04 0.02
Abbreviations: CN, copy number; N (%), number (percentage). OR (95% C.I.), odds ratio (95% confidence interval). aP values were calculated by chi square test (3x2 table) and were considered significant when the value less than 0.05. b Odds ratio and 95% CIs were estimated by applying unconditional logistic regression.
* Individuals with missing phenotype data were discarded from the logistic regression analysis. 353 354 355 356 357 358