The use of fluoride varnish and its determining factors among children with disability in Taiwan
Rhay-Hung Weng1, Pei-Tseng Kung 2, Wen-Chen Tsai3, Hsien-Hsiung Chiang4, Li-Ting Chiu3
1 Department of Public Health, Kaohsiung Medical University, 100, Shih-Chuan 1st Road,
Kaohsiung, 80708, Taiwan, R.O.C. E-mail: [email protected]
2 Department of Healthcare Administration, Asia University, Taichung, Taiwan, R.O.C. E-mail:
3 Department of Health Services Administration, China Medical University, Taichung, 404,
Taiwan, R.O.C. E-mail: [email protected]
4
Dental Department, China Medical University Hospital, Taichung, 404, Taiwan, R.O.C.
Running title:The use of fluoride varnish among children with disability
Corresponding author: Wen-Chen Tsai, Dr.PH, Department of Health Services Administration, China Medical University, No. 91 Hsueh-Shih Road, Taichung, Taiwan 40402, R.O.C. TEL: + 886 4 22073070, Fax:+ 886 4 22028895, E-mail: [email protected]
Abstract
The oral health of children with disability is often not as good as that of other children. In view of improving their oral health, this study aims to explore the utilization of fluoride varnish services among children with disability in Taiwan and its relevant influencing factors. With children under the age of 5 as subjects, this study is conducted based on the database of Ministry of the Interior, Executive Yuan, R.O.C. in 2008, coupled with information gathered between 2006–2008 on preventive health care and health insurance from the Bureau of Health Promotion and the National Health Research Institute, respectively. In addition to descriptive statistics and bivariate analysis, this study examined the factors determining the use of fluoride varnish with logistic regression analysis. Research revealed that fluoride varnish is used by up to 9.84% of children with disability; the use increases with age and decreases with increased level of disability, but is remarkably higher in those with catastrophic illness/injury. The probability of fluoride varnish use is lower among those living in areas of lower urbanization (levels 5 to 7) and higher among those whose parents have higher premium-based monthly salaries.
Recommendations include (1) providing a differential pricing scheme for fluoride varnish based on the level of disability of the child, (2) promoting proactively among dentists to carry out regular fluoride varnish in rural areas and collaboration with pediatricians to provide convenient services and (3) targeting families in low socioeconomic brackets, improving knowledge of fluoride varnish.
1. Introduction
Due to physical and psychological barriers, patients with disability may be unable to communicate their physical complaints accurately, thus reducing their access to health care. There is also a need for longer consultation times with increased complexity, leading to delay or even neglect of necessary treatments. Such phenomenon also applies to the utilization of preventive health services (Diab & Johnston, 2004; Lin, Yen, & Wu, 2005). Healthy People 2010 has made health promotion among disabled individuals a focus area. Studies in the past have revealed that children with disability are in greater need of treatment and prevention of oral diseases; their oral health is poorer than average school children (Hennequin, et al., 2008; Macnab, et al., 2008). Rodrigues et al. (2003) discovered that children with cerebral palsy (CP) have much higher decayed, missing and filled permanent surfaces (DMFS) and dental plaque index compared to children without CP. De Camargo and Antunes (2008) concluded that children with CP show a poorer dental status compared to age and geography-standardized non-CP children, with up to 49.5 % of them having had at least one tooth affected by untreated caries. Disparity in dental hygiene status is also seen between children with and without disability (Liu, et al., 2010). Therefore, the improvement of oral health has become an important subject in the field of preventive medicine for children with disability.
It is evident that early prevention planning for children leads to significant improvement in oral health, increasing caries-free children from 8% to 32% (Macnab, et al., 2008). Rodriguezy (2002) also proved that children with disability showed visible reduction of decayed, missing, and filled teeth (DMFT) index following the implementation of an oral health prevention plan. Thus, preventive measures play an important role in the oral health of children with disability. Houtrow et al. (2007) highlighted the differences in preventive health service utilization among
children with intellectual and/or developmental disability (IDD) and those without IDD. In spite of the increased susceptibility to oral diseases, Chi et al. (2010) observed that the rate of preventive dental service utilization is much lower among IDD children compared to non-IDD children. In order to effectively improve the oral health of children with disability, it is necessary to conduct a large-scaled evaluation of the utilization of oral preventive service and its influencing factors.
From the beginning of July 2004, fluoride varnish was made one of the important oral preventive health services provided by the Department of Health in Taiwan. Children under five years old are eligible for the biannual dental examination coupled with fluoride varnish. Fluoride varnish is now globally recognized and approved by dental experts for its prevention against dental caries. According to the statistics as of the end of 2008, the rate of fluoride varnish among Taiwanese children is only 10.36%, indicating that a majority of the children have yet to utilize this service (Department of Health, 2009). Physical and psychological barriers are potential factors affecting disabled children’s ability to access fluoride varnish services. However, further studies are required to confirm this. In view of the disparity in the access of oral preventive health services between children with and without disability and the lack of national studies on the utilization of fluoride varnish services, a discussion on the utilization of fluoride varnish services among Taiwanese children with disability and the analysis of relevant determining factors will be conducted in this study.
2. Materials and methods
2.1. Data source and processing
With children under the age of 5 as subjects, this study is conducted based on the database of Ministry of the Interior, Executive Yuan, R.O.C. 2008, coupled with information gathered
between 2006–2008 on preventive health care and health insurance from the Bureau of Health
Promotion and the National Health Research Institute, respectively. The variables recorded include: (1) Demographic characteristics: gender, age, aboriginal status; (2) health and disability status: catastrophic illness/injury, relevant chronic illnesses (including cancer, endocrine and metabolic diseases, mental disorders, diseases of the nervous system, diseases of the circulatory system, diseases of the respiratory system, diseases of the digestive system, diseases of the genitourinary system, diseases of the musculoskeletal system and connective tissue, disorders of the eye and adnexa, infectious disease, congenital anomalies, diseases of skin and subcutaneous tissue, diseases of blood and blood-forming organs, diseases of the ear and mastoid process); (3) classification of disability: type of disability, severity of disability; (4) the utilization of children’s preventive health services; (5) fluoride varnish status: any usage of fluoride varnish, frequency of usage. As parents are pivotal in influencing the children’s health care utilization, variables pertaining to their parents were also acquired. This includes gender, age, residence, premium-based monthly salary, and low-income household status.
2.2. Subjects
According to the ‘Disability Rights Protection Acts’ of Taiwan, disability can be classified into 18 categories, namely visual impairment, hearing impairment, balance impairment, sound or speech impairment, physical disability, mental retardation, major organ malfunction, facial injury, persistent vegetative state, refractory epilepsy, dementia, autism, chromosomal abnormalities, congenital metabolic disorders, other congenital defects, multiple disabilities, chronic mental illness and other disabilities caused by rare diseases recognized by central health authorities. Three categories of disability are deemed less suitable or too small in sample size and thus are excluded from this study: persistent vegetative state (18 individuals), dementia (1 individual),
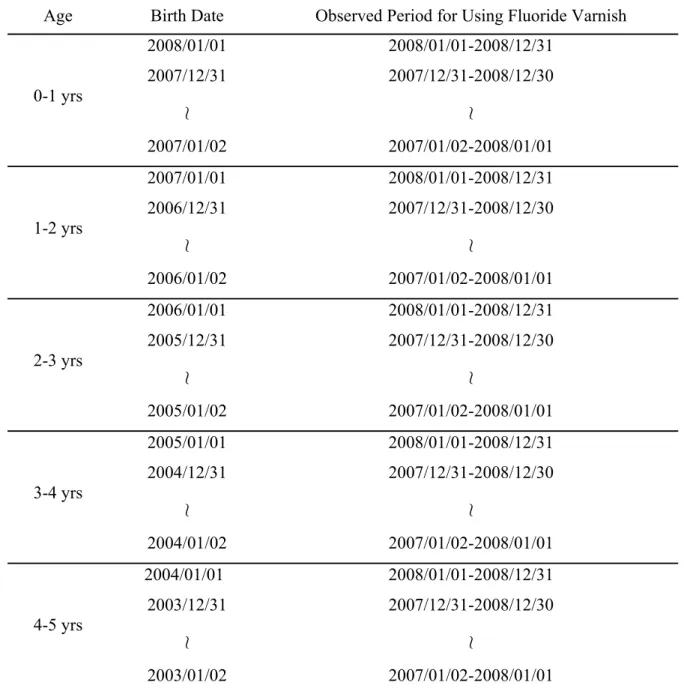
and chronic mental illness (4 individuals), all of whom have not utilized the fluoride varnish. Severity of disability is classified into 4 groups: very severe, severe, moderate, and mild. Table 1 provides an example of the selection criteria. A total of 7604 children (<5 years old) with disability have been identified to have met the requirement for fluoride varnish services.
2.3. Statistical analysis
All data were analyzed with the SAS version 8.2. This study firstly involves a descriptive analysis of the identified variables. Frequency of fluoride varnish use and the differences in their percentage of each variable will be examined using t-test, one-way ANOVA, and χ2 test to check for statistical significance. Lastly, logistic regression analysis is used to examine influencing factors on the usage of fluoride varnish.
3. Results
Males made up 63.77% of the sample. The children aged between 4 to 5 years old constitute the largest group (33.5%). 1.54% of the sample are aborigines and 64.74% of the sample do not have any catastrophic illness/injury. In terms of the classification of disability, intellectual disability made up the largest group (19.41%) followed by multiple disabilities (19.17%), and a majority of the sample suffered from mild disability (36.03%). 85.01% of the sample have utilized preventive health services in the past. A majority of the children’s parents are aged between 31 to 40 years old. Individuals living in areas of level 2 urbanization form the largest group (25.62%). The parents with premium-based monthly salary of NT$16,500–22,800 form the largest group (40.33%). 4.41% of the children’s parents belong to low-income household (Table 2).
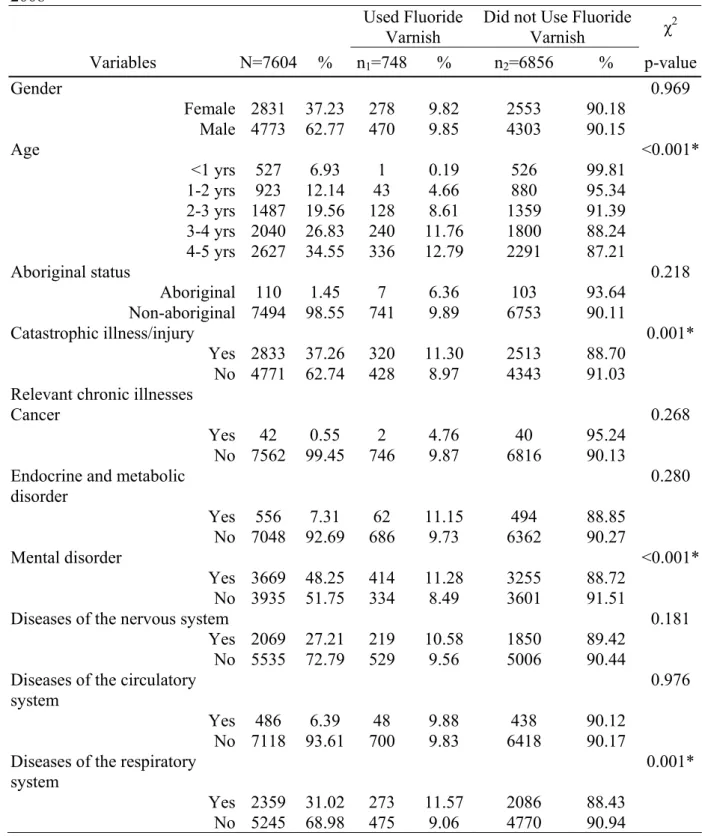
The percentage of children with disability who utilized fluoride vanish is 9.84%, slightly below the national average of 10.36%. The use of fluoride varnish is the highest among children
aged between 4 and 5 years (12.79%) and the percentage of use increases with age. The percentage of use among those with catastrophic illnesses is 11.3%, significantly higher than those without catastrophic illnesses (8.87%). Among the sufferers of relevant chronic illnesses, children with diseases of the musculoskeletal system and connective tissue exhibit the highest usage (13.61%). Among the different categories of impairment, children with facial injuries have the highest usage (17.31%) while visual impairment is only 5.73%. Those with mild disability show a greater usage (12.88%) compared to other levels of disability; a direct relationship between the increase of severity and the decrease in usage is seen. 10.19% of those who had children preventive health services in the past have use of fluoride varnish while those without children preventive health services have only 7.81%. Among the parents, children of insured females show a greater usage compared to their male counterparts. The use of fluoride varnish is higher in children whose parents are aged 31-40 years (11.33%) compare to other age groups. Also, the use of fluoride varnish is the highest in those residing in areas graded level 1 of urbanization (11.86%). When categorized according to their parents’ premium-based salary, those with premium-based monthly salary of NT$76,500–87,600 show the greatest utilization (16.78%) (Table 2).
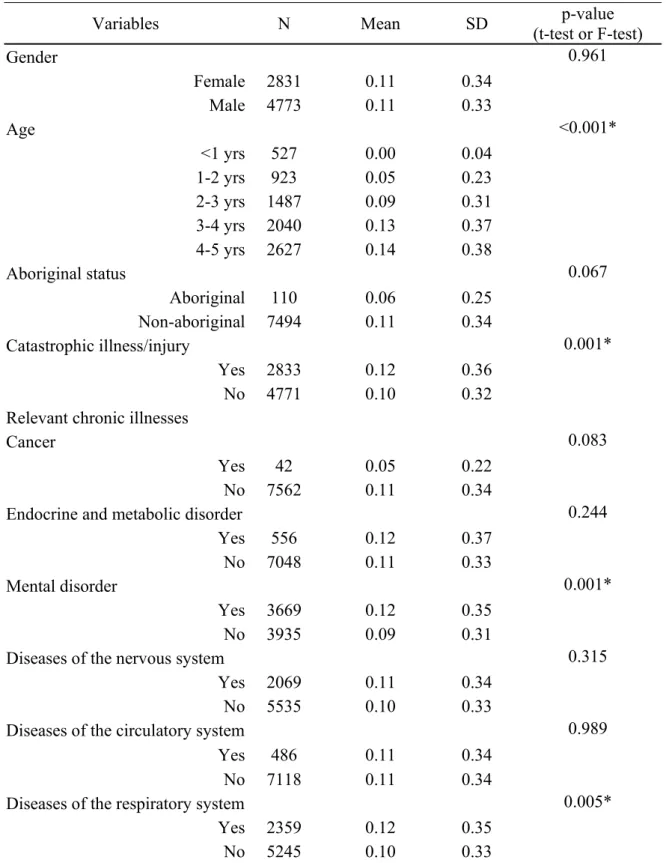
In terms of the frequency of use of fluoride varnish, disabled children aged 3 to 5 years is significantly higher than other age groups (p<0.05), showing positive correlation between age and frequency of use. The average frequency of use among individuals with catastrophic illness (0.12) is significantly higher than those without (p<0.05).The use of fluoride varnish is higher among sufferers of mental disorders, respiratory system diseases, musculoskeletal and connective tissue diseases as well as diseases of the ear and mastoid process. The average usage of those with mild disability (0.14) is significantly higher than other severities (p<0.05). Past
users of the children preventive health service show higher frequency of fluoride varnish use (0.11). Utilization is significantly higher (p<0.05) among children whose parents are aged 31–40 years (0.12). Residents in areas of level 1 urbanization have a significantly greater usage frequency (0.13) than residents of levels 5–7 (p<0.05). The average frequency of use among those who have the premium-based monthly salary of NT$76,500–87,600 is as high as 0.17 (Table 3).
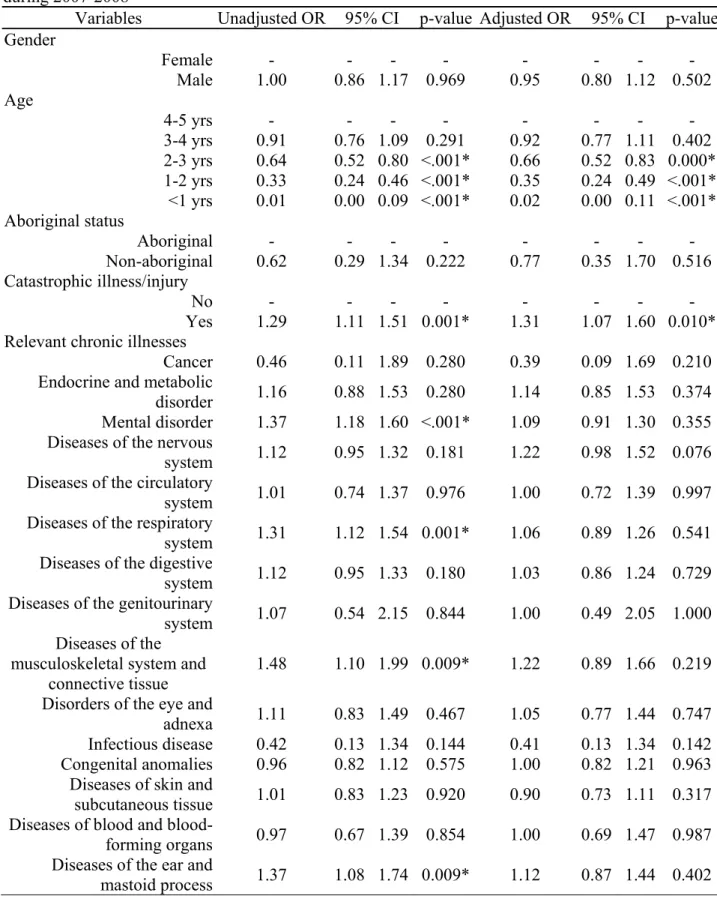
In Table 4, logistic regression analysis reveals that usage probability increases with age that the disabled children below the age of 3 have a much reduced probability of using fluoride varnish compare to those aged 4–5 years after controlling for other variables. The probability of fluoride varnish usage among children with catastrophic illness/injury is 1.31 times more than that of those without catastrophic illness/injury (95% CI: 1.07-1.60). There is no significant difference in usage probability among the different categories of disability and relevant chronic illnesses (p>0.05). However, differences are seen among the different severities, in which the ‘very severe’ group has the lowest usage probability (OR=0.26; 95% CI: 0.17-0.41). The probability of usage among children of parents aged 31-40 years is 1.30 times more than that of parents aged below 30 years. Children residing in urbanization areas level 6 and 7 show a much lower usage probability compared to children residing in area level 1. Furthermore, those with premium-based monthly salary of NT$76,500–87,600 have the highest usage probability, with up to 2.34 fold of those with monthly salary of NT$<15,840, proving a high degree of correlation between parental income and fluoride varnish usage in children with disability.
4. Discussion
Levy et al. (2003) and Slayton et al. (2002) stated that younger children exhibit relatively lower overall fluoride applications. This study discovered that both the usage probability and
frequency of fluoride varnish among the disabled children of younger age groups (<3 years) is much lower than children older than 4 years old. Likewise, Chi et al. (2010) discovered that children’s preventive dental service utilization increases with age in the United States, and it is utilized by less than 10% of children below the age of 1, followed by about 10% of children aged 1–2 and up to 37.8% of those aged 3–7 years. However, this study revealed that such service is utilized by 0.19%, 4.66% and 12.79%, respectively, showing much lower usage in all 3 corresponding age groups. Despite fluoride varnish being the main preventive dental measure promoted by the Department of Health, the utilization of such services remains low among children with disability of all age groups. Furthermore, it is discovered that children with catastrophic illnesses/injuries tend to show greater usage probability. Since the utilization of fluoride varnish is ultimately dependent on the parents, this indicates that preventive oral health is greatly emphasized among parents whose children have significant illnesses.
It is established in this study that having chronic illnesses and the category of disability are not important factors influencing the use of fluoride varnish among children. Though children with disability have a greater and more diverse health care need compared to children without disability (Jeng, et al., 2009), these factors do not significantly affect the use of fluoride varnish. Nevertheless, the severity of disability is an important factor; the usage of fluoride varnish tends to decrease with increasing severity. Such findings are consistent with the study by Diab and Johnston (2004) among American children with disability. This is believed to be attributable to their health status and medical needs, leading to challenges in accessing preventive health services. General health is poorer with increasing severity of disability and the need for therapeutic medical care is often prolonged and demanding. Ongoing medical care mainly revolves around the maintenance or recovery of basic daily function, thus lacking the urgency for
non-emergency and preventive health services like fluoride varnish. Such phenomenon is accentuated with increasing level of severity of disability. Also, greater obstacles/challenges are faced by children with greater levels of disability (Diab & Johnston, 2004), discouraging their willingness to use fluoride varnish. Since severe disability decreases the probability of fluoride varnish usage, it would lead to further deterioration of oral health among these children, whose general health is known to be poorer to begin with. Therefore, the planning and implementation of oral health policies should be focused on the improvement of fluoride varnish usage among children with disability of higher severity. In order to increase the dentists’ willingness and time spent on oral health of people with severe disability, global budgeting payment was employed to promote oral health for those with ‘severe’ and ‘very severe’ disability in Taiwan, thus increasing payments and encouraging treatment and care for the disabled people’s oral health problems (Tsai, et al., 2007). Hence, a similar financial incentive could be implemented to equally emphasize preventive dental health. By increasing the subsidy of care for children with disability, the utilization of preventive health services would also increase.
In terms of parental characteristics, gender differences do not seem to affect fluoride varnish usage. However, it is noted that a majority of the parents are aged between 30-40 years. Similar to this study, Lin et al. (2004) gathered that the average age of primary carers of preschool children with disabilities is 36.3 years. Apart from seeing a significantly higher fluoride varnish usage among children with parents aged 31–40 years, children residing in less urbanized areas (levels 6–7) tend to have a lower usage. Chi et al. (2010) observed that children living in urban or rural counties were significantly less likely to have had a preventive dental visit than those living in metropolitan areas. This is likely to be associated with poorer access to preventive dental care in rural areas. The level of premium-based salary is indicative of the
household income. Fluoride varnish usage is significantly higher among those having higher premium-based salary. Kenney, Kogan, and Crall (2008) confirmed that children’s utilization of preventive dental care varies with household income. Household financial and socioeconomic status is closely associated with the health and development of children with disability. Families of good financial and socioeconomic status tend to place more emphasis on preventive health, showing greater ability in ensuring the health of disabled children (Inkelas, et al., 2007; Lin, et al., 2004). In contrast, the usage of fluoride varnish among the children of low socioeconomic groups has much room for improvement. Time and physical constraints are commonly cited by primary carers to affect the effective usage of preventive health services. Adequate knowledge and correct concepts among primary carers are believed to have a positive impact on the children’s health and development (Hudson, et al., 2003). Since education often correlates with socioeconomic status, parents of lower socioeconomic groups may have inadequate knowledge on preventive health, leading to limited use of fluoride varnish. Parental characteristics play a large role in the utilization of fluoride varnish. Thus, health policy-makers should consider formulating effective parental support measures.
5. Conclusions
In order to improve the utilization of fluoride varnish, parents of children with disability aged under 3 years old should be targeted. Due to the differences in costs (in terms of time, labor and financial costs) for different levels of disability needed to help children with disability access health care and treatment, it is recommended that a differential subsidy should be set for different levels of disability severity. This would improve the acceptance of children with disability to undergo fluoride varnish. The usage of fluoride varnish among children with disability is also lower if parents reside in less urbanized areas. Besides actively promoting the use of fluoride
varnish among children specifically to less urbanized areas or rural areas, relevant incentives should be given. In addition to encouraging dentists to establish dental clinics, the dental associations should actively render coordination to regular dental care and fluoride varnish services in rural areas. Children whose parents have the highest premium-based salary show a much greater usage probability compared to those of low socioeconomic background. Though fluoride varnish services are available free of charge, there is a further need for health authorities to identify families of low socioeconomic groups to improve knowledge of fluoride varnish and to strengthen the concept of preventative oral health. In targeting families of lower
socioeconomic background, having medical staff regularly visits homes and communities to provide fluoride varnish services could be considered.
With regards to funding, children with disability are often in need of pediatric care besides needing visitation by medical personnel and fluoride varnish (Lewis, et al., 2000). Collaboration between dentists and pediatricians should be encouraged. Besides providing education pertaining to preventive oral health and explaining the importance of fluoride varnish during pediatric outpatient visits, pediatric staff should be active in requesting, reminding and arranging for fluoride varnish. Regular follow-ups to check on children’s oral health status and active referrals to fluoride varnish services are also recommended. Lastly, in addition to implementing accessible space planning in clinics, other active services can be included to bring about greater
convenience to parents. For instance, free transportation and consultation priority could be given to children with disability, relieving the parents of this burden and lost time.
Acknowledgements
This study was supported by the grant (No.9805006A) from Bureau of Health Promotion, Department of Health, Taiwan, and was based on data from the National Health Insurance
Research Database provided by National Health Research Institute, the preventive health care files provided by Bureau of Health Promotion, the disabled persons file provided by Ministry of the interior in Taiwan. The interpretations and conclusions contained herein do not represent those of the Bureau of Health Promotion, National Health Research Institutes or Ministry of the interior in Taiwan.
References
Chi, D. L., Momany, E. T., Kuthy, R. A., Chalmers, J. M., & Damiano, P. C. (2010). Preventive dental utilization for medicaid-enrolled children in iowa identified with intellectual and/or developmental disability. Journal of Public Health Dentistry, 70, 35-44.
De Camargo, M. A., & Antunes, J. L. (2008). Untreated dental caries in children with cerebral palsy in the Brazilian context. International Journal of Paediatric Dentistry, 18, 131−138. Department of Health. (2009). 2008 health promotion statistics in taiwan. In D. o. Health (Ed.),
(Vol. 2009). Taiwan: Department of Health, Executive Yuan.
Diab, M. E., & Johnston, M. V. (2004). Relationships between level of disability and receipt of preventive health services. Archives of Physical Medicine and Rehabilitation, 85, 749-757.
Hennequin, M., Moysan, V., Jourdan, D., Dorin, M., & Nicolas, E. (2008). Inequalities in oral health for children with disabilities: A French national survey in special schools. PLoS
ONE, 3, e2564.
Houtrow, A. J., Kim, S. E., Chen, A. Y., & Newacheck, P. W. (2007). Preventive health care for children with and without special health care. Pediatrics, 119, 821-828.
Hudson, A. M., Matthews, J. M., Gavidia-Payne, S. T., Cameron, C. A., & Mildon, R. L. (2003). Evaluation of an intervention system for parents of children with intellectual disability and challenging behaviour. Journal of Intellectual Disability Research, 47, 238-249. Inkelas, M., Raghavan, R., Kandyce, K., Kuo, A. A., & Ortega, A. N. (2007). Unmet mental
health need and access to services for children with special health care needs and their families. Ambulatory Pediatrics, 7, 431-438.
Jeng, W. L., Wang, T. M., Cher, T. L., Lin, C. P., & Jeng, J. H. (2009). Strategies for oral health care for people with disabilities in Taiwan. Journal of Dental Sciences, 4, 165-172. Kenney, M. K., Kogan, M. D., & Crall, J. J. (2008). Parental perceptions of dental/oral health
among children with and without special health care needs. Ambulatory Pediatrics, 8, 312-320.
Levy, S. M., Broffitt, B., Slayton, R., Warren, J. J., & Kanellis, M. J. (2003). Dental visits and professional fluoride applications for children ages 3 to 6 in Iowa. Pediatric Dentistry, 25, 565-571.
pediatrician in the oral health of children: A national survey. Pediatrics, 106, E84. Lin, J. D., Lin, Y. W., Yen, C. F., Wu, J. L., & Chwo, M. J. (2004). Healthcare utilization and
barriers assessment for preschool children with disabilities in Taipei. Taiwan Journal of
Public Health 23, 412-418.
Lin, J. D., Yen, C. F., & Wu, J. L. (2005). Importance and satisfaction of preventive health strategies in institutions for people with intellectual disabilities: A perspective of institutional directors. Research in Developmental Disabilities, 26, 267-280.
Liu, H. Y., Chen, C. C., Hu, W. C., Tang, R. C., Chen, C. C., Tsai, C. C., & Huang, S. T. (2010). The impact of dietary and tooth-brushing habits to dental caries of special school children with disability. Research in Developmental Disabilities, 31, 1160-1169.
Macnab, A. J., Romus, J., Benton, D., & Gaqnon, F. A. (2008). 3-years results of a collaborative school based oral health program in remote first nations community. Rural Remote
Health, 8, 882.
Rodrigues, d. S. M., Masiero, D., Novo, N. F., & Simionato, M. R. (2003). Oral conditions in children with cerebral palsy. Journal of Dentistry for Children, 70, 40-46.
Rodriguezy, V. C., Garcillan, R., Rioboo, R., & Bratos, E. (2002). Prevalence of dental caries in an adult population with mental disabilities in spain. Special Care in Dentistry, 22, 65-69. Slayton, R. L., Warren, J. J., Levy, S. M., Kanellis, M. J., & Islam, M. (2002). Frequency of
reported dental visits and professional fluoride applications in a cohort of children followed from birth to age 3 years. Pediatric Dentistry, 24, 64-68.
Tsai, W. C., Kung, P. T., Chiang, H. H., & Chang, W. C. (2007). Changes and factors associated with dentists’ willingness to treat patients with severe disabilities. Health Policy, 83, 363– 374.
Table 1 Study subjects finding criteria
Age Birth Date Observed Period for Using Fluoride Varnish
0-1 yrs 2008/01/01 2007/12/31 ≀ 2007/01/02 2008/01/01-2008/12/31 2007/12/31-2008/12/30 ≀ 2007/01/02-2008/01/01 1-2 yrs 2007/01/01 2006/12/31 ≀ 2006/01/02 2008/01/01-2008/12/31 2007/12/31-2008/12/30 ≀ 2007/01/02-2008/01/01 2-3 yrs 2006/01/01 2005/12/31 ≀ 2005/01/02 2008/01/01-2008/12/31 2007/12/31-2008/12/30 ≀ 2007/01/02-2008/01/01 3-4 yrs 2005/01/01 2004/12/31 ≀ 2004/01/02 2008/01/01-2008/12/31 2007/12/31-2008/12/30 ≀ 2007/01/02-2008/01/01 4-5 yrs 2004/01/01 2003/12/31 ≀ 2003/01/02 2008/01/01-2008/12/31 2007/12/31-2008/12/30 ≀ 2007/01/02-2008/01/01
Table 2 Chi-square analysis of the use of fluoride varnish in children with disability during 2007-2008
Used Fluoride Varnish
Did not Use Fluoride
Varnish χ2 Variables N=7604 % n1=748 % n2=6856 % p-value Gender 0.969 Female 2831 37.23 278 9.82 2553 90.18 Male 4773 62.77 470 9.85 4303 90.15 Age <0.001* <1 yrs 527 6.93 1 0.19 526 99.81 1-2 yrs 923 12.14 43 4.66 880 95.34 2-3 yrs 1487 19.56 128 8.61 1359 91.39 3-4 yrs 2040 26.83 240 11.76 1800 88.24 4-5 yrs 2627 34.55 336 12.79 2291 87.21 Aboriginal status 0.218 Aboriginal 110 1.45 7 6.36 103 93.64 Non-aboriginal 7494 98.55 741 9.89 6753 90.11 Catastrophic illness/injury 0.001* Yes 2833 37.26 320 11.30 2513 88.70 No 4771 62.74 428 8.97 4343 91.03
Relevant chronic illnesses
Cancer 0.268
Yes 42 0.55 2 4.76 40 95.24
No 7562 99.45 746 9.87 6816 90.13
Endocrine and metabolic disorder 0.280 Yes 556 7.31 62 11.15 494 88.85 No 7048 92.69 686 9.73 6362 90.27 Mental disorder <0.001* Yes 3669 48.25 414 11.28 3255 88.72 No 3935 51.75 334 8.49 3601 91.51
Diseases of the nervous system 0.181
Yes 2069 27.21 219 10.58 1850 89.42
No 5535 72.79 529 9.56 5006 90.44
Diseases of the circulatory system
0.976
Yes 486 6.39 48 9.88 438 90.12
No 7118 93.61 700 9.83 6418 90.17
Diseases of the respiratory system
0.001*
Yes 2359 31.02 273 11.57 2086 88.43
Table 2 (continued)
Used Fluoride Varnish
Did not Use Fluoride
Varnish χ2
Variables N=7604 % n1=748 % n2=6856 % p-value
Diseases of the digestive system
0.180
Yes 2029 26.68 215 10.60 1814 89.40
No 5575 73.32 533 9.56 5042 90.44
Diseases of the genitourinary system
0.844
Yes 86 1.13 9 10.47 77 89.53
No 7518 98.87 739 9.83 6779 90.17
Diseases of the musculoskeletal system and connective tissue
0.009*
Yes 404 5.31 55 13.61 349 86.39
No 7200 94.69 693 9.63 6507 90.38
Disorders of the eye and adnexa 0.467
Yes 511 6.72 55 10.76 456 89.24 No 7093 93.28 693 9.77 6400 90.23 Infectious disease 0.131 Yes 68 0.89 3 4.41 65 95.59 No 7536 99.11 745 9.89 6791 90.11 Congenital anomalies 0.575 Yes 2898 38.11 278 9.59 2620 90.41 No 4706 61.89 470 9.99 4236 90.01
Diseases of skin and subcutaneous tissue
0.920
Yes 1423 18.71 141 9.91 1282 90.09
No 6181 81.29 607 9.82 5574 90.18
Diseases of blood and blood-forming organs
0.853
Yes 356 4.68 34 9.55 322 90.45
No 7248 95.32 714 9.85 6534 90.15
Diseases of the ear and mastoid process 0.008* Yes 703 9.25 89 12.66 614 87.34 No 6901 90.75 659 9.55 6242 90.45 Type of disability 0.046* Mental retardation 1476 19.41 140 9.49 1336 90.51 Multiple disabilities 1458 19.17 124 8.50 1334 91.50 Physical disability 1135 14.93 112 9.87 1023 90.13 Autism 1023 13.45 122 11.93 901 88.07 Hearing impairment 582 7.65 54 9.28 528 90.72
Major organ malfunction 556 7.31 55 9.89 501 90.11
Table 2 (continued)
Used Fluoride Varnish
Did not Use Fluoride
Varnish χ 2 Variables N=7604 % n1=748 % n2=6856 % p-value Chromosomal Abnormalities 342 4.50 27 7.89 315 92.11 Rare diseases 218 2.87 17 7.80 201 92.20 Visual impairment 122 1.60 7 5.74 115 94.26 Congenital defects 74 0.97 8 10.81 66 89.19 Facial injury 52 0.68 9 17.31 43 82.69 Refractory epilepsy 41 0.54 6 14.63 35 85.37 Others 52 0.68 7 13.46 45 86.54 Severity of disability <0.001* Mild 2740 36.03 353 12.88 2387 87.12 Moderate 2578 33.90 248 9.62 2330 90.38 Severe 1643 21.61 113 6.88 1530 93.12 Very severe 643 8.46 34 5.29 609 94.71 Utilization of children’s preventive health services
0.013* Yes 6464 85.01 659 10.19 5805 89.81 No 1140 14.99 89 7.81 1051 92.19 Parents' characteristics Sex 0.010* Female 3022 39.74 330 10.92 2692 89.08 Male 4582 60.26 418 9.12 4164 90.88 Age <0.001* ≦30 yrs 2059 27.08 147 7.14 1912 92.86 31-40 yrs 4271 56.17 484 11.33 3787 88.67 ≧41 yrs 1274 16.75 117 9.18 1157 90.82 Urbanization level <0.001* Level 1 995 13.09 118 11.86 877 88.14 Level 2 1948 25.62 224 11.50 1724 88.50 Level 3 1346 17.70 148 11.00 1198 89.00 Level 4 706 9.28 67 9.49 639 90.51 Level 5 1032 13.57 81 7.85 951 92.15 Level 6 673 8.85 44 6.54 629 93.46 Level 7 636 8.36 44 6.92 592 93.08 Level 8 268 3.52 22 8.21 246 91.79
Table 2 (continued)
Used Fluoride Varnish
Did not Use
Fluoride Varnish χ 2 Variables N=7604 % n1=748 % n2=6856 % p-value Premium-based monthly salary (NT$) <0.001* <15,840 1595 20.98 109 6.83 1486 93.17 16,500-22,800 3067 40.33 300 9.78 2767 90.22 24,000-28,800 617 8.11 58 9.40 559 90.60 30,300-36,300 664 8.73 68 10.24 596 89.76 38,200-45,800 734 9.65 91 12.40 643 87.60 48,200-57,800 551 7.25 69 12.52 482 87.48 60,800-72,800 227 2.99 28 12.33 199 87.67 76,500-87,600 149 1.96 25 16.78 124 83.22 Low-income household 0.062 Yes 335 4.41 23 6.87 312 93.13 No 7269 95.59 725 9.97 6544 90.03 *p<0.05
Table 3 Descriptive analysis of the use of fluoride varnish in children with disability during 2007-2008
Variables N Mean SD (t-test or F-test) p-value
Gender 0.961 Female 2831 0.11 0.34 Male 4773 0.11 0.33 Age <0.001* <1 yrs 527 0.00 0.04 1-2 yrs 923 0.05 0.23 2-3 yrs 1487 0.09 0.31 3-4 yrs 2040 0.13 0.37 4-5 yrs 2627 0.14 0.38 Aboriginal status 0.067 Aboriginal 110 0.06 0.25 Non-aboriginal 7494 0.11 0.34 Catastrophic illness/injury 0.001* Yes 2833 0.12 0.36 No 4771 0.10 0.32
Relevant chronic illnesses
Cancer 0.083
Yes 42 0.05 0.22
No 7562 0.11 0.34
Endocrine and metabolic disorder 0.244
Yes 556 0.12 0.37
No 7048 0.11 0.33
Mental disorder 0.001*
Yes 3669 0.12 0.35
No 3935 0.09 0.31
Diseases of the nervous system 0.315
Yes 2069 0.11 0.34
No 5535 0.10 0.33
Diseases of the circulatory system 0.989
Yes 486 0.11 0.34
No 7118 0.11 0.34
Diseases of the respiratory system 0.005*
Yes 2359 0.12 0.35
Table 3 (continued)
Variables N Mean SD (t-test or F-test)p-value
Diseases of the digestive system 0.381
Yes 2029 0.11 0.34
No 5575 0.10 0.33
Diseases of the genitourinary system 0.953
Yes 86 0.10 0.31
No 7518 0.11 0.34
Diseases of the musculoskeletal system and connective tissue
0.011*
Yes 404 0.16 0.42
No 7200 0.10 0.33
Disorders of the eye and adnexa 0.639
Yes 511 0.11 0.34 No 7093 0.11 0.33 Infectious disease 0.236 Yes 68 0.06 0.29 No 7536 0.11 0.34 Congenital anomalies 0.551 Yes 2898 0.10 0.33 No 4706 0.11 0.34
Diseases of skin and subcutaneous tissue
0.723
Yes 1423 0.11 0.34
No 6181 0.11 0.33
Diseases of blood and blood-forming organs
0.596
Yes 356 0.10 0.31
No 7248 0.11 0.34
Diseases of the ear and mastoid process 0.037* Yes 703 0.13 0.36 No 6901 0.10 0.33 Type of disability 0.026* Mental retardation 1476 0.10 0.33 Multiple disabilities 1458 0.09 0.31 Physical disability 1135 0.11 0.34 Autism 1023 0.13 0.36 Hearing impairment 582 0.10 0.31
Major organ malfunction 556 0.11 0.35
Table 3 (continued)
Variables N Mean SD (t-test or F-test)p-value
Chromosomal abnormalities 342 0.08 0.30 Rare diseases 218 0.09 0.31 Visual impairment 122 0.06 0.23 Congenital defects 74 0.11 0.31 Facial injury 52 0.21 0.50 Refractory epilepsy 41 0.15 0.36 Others 52 0.13 0.34 Severity of disability <0.001* Mild 2740 0.14 0.39 Moderate 2578 0.10 0.32 Severe 1643 0.07 0.27 Very severe 643 0.06 0.25 Utilization of children’s preventive health services
0.005* Yes 6464 0.11 0.34 No 1140 0.08 0.29 Parents' characteristics Sex 0.007* Female 3022 0.12 0.36 Male 4582 0.10 0.32 Age <0.001* ≦30 yrs 2059 0.08 0.29 31-40 yrs 4271 0.12 0.36 ≧41 yrs 1274 0.10 0.32 Urbanization level <0.001* Level 1 995 0.13 0.38 Level 2 1948 0.12 0.35 Level 3 1346 0.12 0.37 Level 4 706 0.10 0.30 Level 5 1032 0.09 0.30 Level 6 673 0.07 0.28 Level 7 636 0.07 0.27 Level 8 268 0.08 0.28
Table 3 (continued)
Variables N Mean SD (t-test or F-test)p-value
Premium-based monthly salary (NT$) <0.001* <15,840 1595 0.07 0.28 16,500-22,800 3067 0.11 0.33 24,000-28,800 617 0.10 0.34 30,300-36,300 664 0.11 0.32 38,200-45,800 734 0.14 0.39 48,200-57,800 551 0.14 0.37 60,800-72,800 227 0.14 0.40 76,500-87,600 149 0.17 0.40 Low-income household 0.016* Yes 335 0.07 0.27 No 7269 0.11 0.34 *p<0.05
Table 4 Logistic regression models for the use of fluoride varnish in children with disability during 2007-2008 a
Variables Unadjusted OR 95% CI p-value Adjusted OR 95% CI p-value
Gender Female - - - - - - - - Male 1.00 0.86 1.17 0.969 0.95 0.80 1.12 0.502 Age 4-5 yrs - - - - 3-4 yrs 0.91 0.76 1.09 0.291 0.92 0.77 1.11 0.402 2-3 yrs 0.64 0.52 0.80 <.001* 0.66 0.52 0.83 0.000* 1-2 yrs 0.33 0.24 0.46 <.001* 0.35 0.24 0.49 <.001* <1 yrs 0.01 0.00 0.09 <.001* 0.02 0.00 0.11 <.001* Aboriginal status Aboriginal - - - - - - - - Non-aboriginal 0.62 0.29 1.34 0.222 0.77 0.35 1.70 0.516 Catastrophic illness/injury No - - - - - - - - Yes 1.29 1.11 1.51 0.001* 1.31 1.07 1.60 0.010*
Relevant chronic illnesses
Cancer 0.46 0.11 1.89 0.280 0.39 0.09 1.69 0.210
Endocrine and metabolic
disorder 1.16 0.88 1.53 0.280 1.14 0.85 1.53 0.374
Mental disorder 1.37 1.18 1.60 <.001* 1.09 0.91 1.30 0.355
Diseases of the nervous
system 1.12 0.95 1.32 0.181 1.22 0.98 1.52 0.076
Diseases of the circulatory
system 1.01 0.74 1.37 0.976 1.00 0.72 1.39 0.997
Diseases of the respiratory
system 1.31 1.12 1.54 0.001* 1.06 0.89 1.26 0.541
Diseases of the digestive
system 1.12 0.95 1.33 0.180 1.03 0.86 1.24 0.729
Diseases of the genitourinary
system 1.07 0.54 2.15 0.844 1.00 0.49 2.05 1.000
Diseases of the musculoskeletal system and
connective tissue
1.48 1.10 1.99 0.009* 1.22 0.89 1.66 0.219
Disorders of the eye and
adnexa 1.11 0.83 1.49 0.467 1.05 0.77 1.44 0.747
Infectious disease 0.42 0.13 1.34 0.144 0.41 0.13 1.34 0.142
Congenital anomalies 0.96 0.82 1.12 0.575 1.00 0.82 1.21 0.963
Diseases of skin and
subcutaneous tissue 1.01 0.83 1.23 0.920 0.90 0.73 1.11 0.317
Diseases of blood and
blood-forming organs 0.97 0.67 1.39 0.854 1.00 0.69 1.47 0.987
Diseases of the ear and
Table 4 (continued)
Variables Unadjusted OR 95% CI p-value Adjusted OR 95% CI p-value
Type of disability
Physical disability - - - -
Visual impairment 0.56 0.25 1.22 0.144 0.68 0.30 1.56 0.363
Hearing impairment 0.93 0.66 1.31 0.696 1.21 0.82 1.78 0.336
Sound or speech impairment 1.33 0.95 1.85 0.097 1.01 0.70 1.45 0.966
Mental retardation 0.96 0.74 1.24 0.743 0.79 0.58 1.06 0.120
Multiple disabilities 0.85 0.65 1.11 0.232 1.05 0.77 1.43 0.743
Major organ malfunction 1.00 0.71 1.41 0.988 1.13 0.76 1.70 0.550
facial injury 1.91 0.91 4.03 0.088 1.19 0.54 2.60 0.672 Autism 1.24 0.94 1.62 0.125 0.83 0.60 1.16 0.278 Chromosomal abnormalities 0.78 0.51 1.21 0.274 1.03 0.63 1.69 0.900 Congenital defects 1.11 0.52 2.37 0.793 1.30 0.58 2.88 0.524 Refractory epilepsy 1.57 0.64 3.80 0.322 0.89 0.35 2.24 0.800 Rare diseases 0.77 0.45 1.32 0.342 0.83 0.47 1.47 0.516 Others 1.42 0.63 3.23 0.401 1.34 0.56 3.19 0.515 Severity of disability Mild - - - - - - - - Moderate 0.72 0.61 0.86 0.000* 0.68 0.56 0.82 <.001* Severe 0.50 0.40 0.62 <.001* 0.44 0.34 0.58 <.001* Very severe 0.38 0.26 0.54 <.001* 0.26 0.17 0.41 <.001* Utilization of children’s
preventive health services
No - - - - - - - - Yes 1.34 1.06 1.69 0.013* 0.97 0.76 1.24 0.815 Parents' characteristics Sex Female - - - - - - - - Male 0.82 0.70 0.95 0.010* 0.81 0.69 0.96 0.012* Age ≦30 yrs - - - - - - - - 31-40 yrs 1.66 1.37 2.02 <.001* 1.30 1.04 1.62 0.019* ≧41 yrs 1.32 1.02 1.70 0.034* 1.02 0.77 1.35 0.919 Urbanization level Level 1 - - - - Level 2 0.97 0.76 1.22 0.773 1.05 0.82 1.36 0.684 Level 3 0.92 0.71 1.19 0.515 0.98 0.75 1.29 0.890 Level 4 0.78 0.57 1.07 0.123 0.89 0.64 1.24 0.489 Level 5 0.63 0.47 0.85 0.003* 0.73 0.53 1.00 0.053 Level 6 0.52 0.36 0.75 0.000* 0.57 0.39 0.83 0.003* Level 7 0.55 0.39 0.79 0.001* 0.65 0.44 0.95 0.027* Level 8 0.67 0.41 1.07 0.093 0.85 0.52 1.41 0.534
Table 4 (continued)
Variables Unadjusted OR 95% CI p-value Adjusted OR 95% CI p-value
Premium-based monthly salary (NT$) <15,840 - - - - - - - - 16,500-22,800 1.48 1.18 1.86 0.001* 1.36 1.05 1.76 0.019* 24,000-28,800 1.42 1.01 1.97 0.041* 1.38 0.96 1.97 0.080 30,300-36,300 1.56 1.13 2.14 0.006* 1.43 1.01 2.02 0.043* 38,200-45,800 1.93 1.44 2.59 <.001* 1.75 1.26 2.42 0.001* 48,200-57,800 1.95 1.42 2.68 <.001* 1.60 1.12 2.27 0.009* 60,800-72,800 1.92 1.23 2.98 0.004* 1.70 1.06 2.72 0.028* 76,500-87,600 2.75 1.72 4.41 <.001* 2.34 1.41 3.88 0.001* Low-income household No - - - - - - - - Yes 0.67 0.43 1.02 0.064 1.01 0.61 1.67 0.978 aN=7622, *p<0.05