Hypoaesthesia occurs with sensory hypersensitivity in chronic whiplash – further evidence of a neuropathic condition
Andy Chien, B.Phty (Hons)
PhD Candidate, Division of Physiotherapy
The University of Queensland QLD 4072 Australia Eli Eliav, DMD, PhD
University of Medicine and Dentistry New Jersey Newark, New Jersey, 07101, United States
Michele Sterling, PhD MPhty BPhty Grad Dip Manip Phty Associate Director
Centre of National Research on Disability and Rehabilitation Medicine (CONROD) The University of Queensland, Mayne Medical School
Herston Road, Herston QLD 4066 Australia &
Senior Lecturer, Division of Physiotherapy
The University of Queensland, QLD 4072 Australia Corresponding Author: Michele Sterling Tel: +61 7 3365 5344 (direct) Fax: +61 7 3346 4603 Email: [email protected] Keywords:
ABSTRACT
Hypersensitivity to a variety of sensory stimuli has been shown to exist in whiplash associated disorders and may be indicative of peripheral nerve involvement. This cross-sectional study utilized Quantitative Sensory Testing including vibration, thermal and electrical detection thresholds to provide an indirect measure of primary afferents that mediate innocuous and painful sensation. Pain thresholds and psychological distress (SCL-90-R) was also measured. Thirty one subjects with chronic whiplash (>3 months, NDI: 49 ± 17) and 31 controls participated. The whiplash group demonstrated elevated vibration, heat and electrical detection thresholds at most hand sites when compared to controls (p<0.05). Electrical detection thresholds in the lower limb were no different from controls (p=0.83). Mechanical and cold pain thresholds were lower in the whiplash group (p<0.05) with no difference between the groups for heat pain thresholds (p>0.1). SCL-90 scores were higher in the whiplash group but this did not impact on any of the sensory measures. A combination of pain threshold and detection measures best predicted the whiplash group from the controls. Sensory hypoaesthesia and hypersensitivity co-exist in the chronic whiplash condition. The hypoaesthetic changes (elevated detection threshold) consistent with other clinically established neuropathic conditions may indicate
INTRODUCTION
Whiplash associated disorders (WAD) remain one of the most debated musculoskeletal conditions. Sensory disturbances including hypersensitive responses to mechanical, thermal and electrical stimulation have been consistently shown to be a feature of both the acute and chronic stages of the whiplash condition (Curatolo et al 2001, Moog et al 2002, Sterling et al 2003a). Importantly some of the sensory changes have been shown to be associated with poor functional recovery (Kasch et al 2004, Sterling et al 2005). It is generally acknowledged that the sensory hypersensitivity represents augmented central nervous system pain processing mechanisms (Curatolo et al. 2001, Sterling et al. 2003a). However, some of the changes, particularly cold hyperalgesia and sympathetic nervous system dysfunction,may be indicative of peripheral nerve pathology (Sterling et al. 2003a). This proposal has some basis as animal and cadaver models simulating whiplash impact have shown that the nonphysiologic kinematic movement during the impact induces stresses in cervical neural tissue such as the nerve roots and spinal ganglia resulting in mechanical compromise sufficient to cause structural damage (Cusick et al 2001, Ortengren et al 1996, Taylor and Taylor 1996). Furthermore, mechanosensitivity has been demonstrated with clinical tests designed to provoke the brachial plexus as well as mechanical hyperalgesia over upper limb nerve trunks (Greening et al 2005, Ide et al 2001, Sterling et al 2002a).
Despite these findings, standard clinical neurological examination is often normal and deficits in nerve conduction studies are rarely found (Alpar et al 2002, Barnsley et al 1998). Although nerve conduction studies are reliable and reproducible when carried out
by a single examiner (Chaudhry et al 1994), they are limited by their ability to assess only large myelinated nerve fibres and the invasive nature of the technique.
Quantitative Sensory Testing (QST) is proving to be a valuable tool to advance the classification of specific disorders and may be useful in illuminating the underlying mechanism of pain disorders (Edwards et al 2005). Rolke et al., (2006) have
demonstrated the validity of using comprehensive QST to obtain a complete somatosensory profile in order to characterize patients with suspected neuropathic conditions but such testing has never been undertaken in a WAD cohort.
In a cross-sectional study design, comprehensive QST was used to further investigate the sensory presentation of chronic WAD. Different modalities were incorporated to provide an indirect measure of primary afferents that mediate both innocuous and painful
sensation. We hypothesised that patients with chronic WAD would demonstrate elevated detection thresholds as well as widespread sensory hypersensitivity.
MATERIALS AND METHODS Subjects
Thirty one volunteers (25 females, mean (SD) age 35.3 ± 10.7 years) with neck pain (3 months to 3 years duration) as a result of a motor vehicle crash were recruited. Subjects fulfilled the Quebec Task Force Classification criteria of WAD II, neck complaints and musculoskeletal signs but without conduction loss on clinical neurological examination (Spitzer et al 1995). Subjects were excluded if they experienced concussion, loss of consciousness or head injury as a result of the accident, a previous history of neck or upper quadrant pain that required treatment and/or a diagnosed psychiatric disorder. The
whiplash subjects were recruited via primary care practices and from advertisement within radio and print media. Thirty one healthy volunteers (25 females, mean age 31.4 ± 8.9) also participated in the study. The control group was recruited from the general community provided they had never experienced trauma or injuries to the cervical spine, head, and upper quadrant requiring treatment.
The study was approved by the institutional medical research ethics committee. All the subjects were unpaid volunteers and all gave written informed consent before inclusion. Brachial Plexus Provocation Test (BPPT)
The BPPT which has been used in previous studies of whiplash (Sterling et al. 2003a, Sterling et al 2002b) was performed. The angle of elbow extension was measured at pain threshold using a standard goniometer aligned along the mid-humeral shaft, medial epicondyle and ulnar styloid (Balster and Jull 1997, Sterling et al. 2002b). Subjects indicated their pain during the test on a 10cm visual analogue scale (VAS) where 0 indicated no pain and 10 was the worst pain imaginable.
Quantitative sensory testing (QST)
Pressure pain thresholds (PPTs)
PPT’s were measured using a pressure algometer (Somedic AB, Farsta, Sweden) with a probe size of 1 cm2 and application rate of 40 kPa/s. Test sites included the articular pillars of C5/6, nerve trunk of the median nerve at the elbow bilaterally (palpated on the medial side of the biceps just before it forms its tendon) and at a bilateral remote site (muscle belly of tibialis anterior). The subjects depressed a button when the sensation under the probe changed from one of pressure alone to one of pressure and pain (Sterling
et al 2002b). Triplicate recording were taken at each site and the mean values used for analysis.
Thermal (hot, cold) pain thresholds (TPTs)
TPTs were measured using the Thermotest system (Somedic AB, Farsta, Sweden) over the mid-cervical spine and the distal aspect of C7/8 dermatomes (dorsal aspect of the hand). The temperature was preset to either increase or decrease at a rate of 1°C/sec from a baseline of 30°C. The subject pressed a switch when the cold or warm sensation first became painful (Hurtig et al 2001). The mean of three trials at each site were calculated for analysis.
Vibration detection thresholds (VTs)
A vibrometre (Somedic AB, Sweden) with a tissue displacement range of 0.1±400 μm and a constant frequency of 120 Hz was used. In order to familiarise the subjects with the vibration stimulus, 3 trials of the test stimuli, or until the subject was able to consistently indicate the onset of the stimulus, were applied over the muscle belly of brachioradialis. Measures were taken over areas of the hand innervated by distal aspect of the C6 (palmar aspect of the 1st metacarpal), C7 (palmar aspect of 2nd metacarpal; dorsum of the 2nd
metacarpal) and C8 dermatomes (dorsum of the 5th metacarpal). Subjects indicated when the vibration first appeared, the perception threshold (VPT), and when it disappeared, the disappearance threshold (VDT). The vibration threshold (VT) was the average of VPT and VDT. Triplicate recordings were taken at each site and the mean values used for analysis.
TDTs assess the function of afferent small myelinated A-delta fibres (cold sense) and unmyelinated C-fibres (warm sense) (Adriaensen et al 1983, Fowler et al 1988, Hallin et al 1982). Incorporating the method of limits, the Thermotest (Somedic AB, Sweden) was used to measure TDTs over areas of the hand innervated by the C7 (dorsum over the 2nd
metacarpal) and C8 (dorsum of the 5th metacarpal) dermatomes. The temperature was
preset to either increase or decrease at a rate of 1°C/sec from a baseline of 30°C. The patient pressed a switch when they first detected the sensation of warmth or cold.
Electrocutaneous detection and pain thresholds
A non-noxious method of electrocutaneous stimulation was used in a method of limits procedure using the Neurometer device (Neurotron., Baltimore, USA). Sites tested were those innervated by C5/6 (anterior shoulder, inferior to shoulder joint line), C7 (distal phalanx of index finger); C8 (distal phalanx of 5th digit) and Tibialis Anterior as a remote
site. Three different sinusoidal frequencies (2000Hz , 250Hz and 5Hz) were applied to each site in order to evoke a response from a different subpopulation of sensory fibre (Katims et al 1986, Katims et al 1987). The subjects reported when they first perceived the sensation (perception threshold) and again at the intensity at which they can no longer feel the sensation (disappearance threshold). The mean of these two values were
calculated and recorded three times for analysis.
The same sites used to determine current detection thresholds were used to determine pain threshold but only a frequency of 250Hz was used. As the stimulus intensity
increased, the subject released a button when they first perceived the stimulus as painful. The procedure was repeated three times with the mean score recorded as electrical pain threshold.
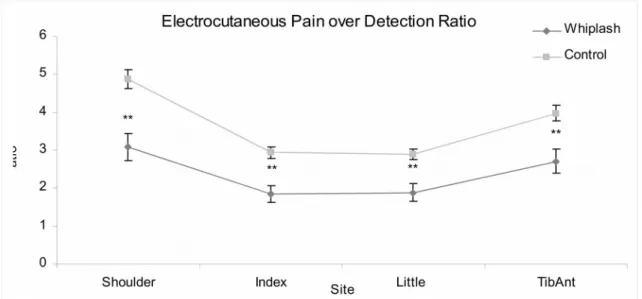
Ratios were obtained by dividing the electrocutaneous pain threshold over the
electrocutaneous detection threshold. Low intensity electrical stimulation activates large A-beta nerve fibres. Current evoked pain at or close to detection threshold (ratio of less than 2:1) has been suggested to be a substrate of A-beta fibre allodynia (Sang et al 2003). Sympathetic Vasoconstrictor Reflex (SVR)
A laser Doppler (Moor Instruments, Devon UK) was used to assess sympathetic nervous system (SNS) function (Schurmann et al 1999). Electrodes were attached to the thenar eminence of both hands. The test was performed with subjects in a comfortable supine position, arms resting at heart level. After a period of acclimatization and normal breathing, participants were asked to take a sudden deep breath. This provocation manoeuvre (inspiratory gasp) is known to cause a short sympathetic reaction and cutaneous vasoconstriction (Schurmann et al. 1999) and has been used in previous investigation of whiplash (Sterling et al 2005). The procedure was repeated three times. Two quotients (SRF and QI) which describe vasomotor reflexes following the inspiratory gasp were calculated. SRF value represents the relative drop of the curve after the
manoeuvre with the QI parameter also being influenced by the duration of perfusion decrease (Schurmann et al. 1999).
Questionnaires
All participants completed the Neck Disability Index (NDI) (Vernon and Mior 1991) and The Symptom Check List 90-R (SCL-90-R). The NDI was used to assess the extent of perceived functional disability. The SCL-90-R assessed the psychological well being of participants.
Procedure
Once the informed written consent was obtained, testing was performed in the following order: SVR, BPPT, PPT (tibialis anterior, median nerve, C5/6), TDTs, TPTs, VTs, electrocutaneous detection (2000, 250, 5 Hz) and pain thresholds (250 Hz). The SVR testing was performed in a temperature-controlled laboratory. The temperature was set at 20°C, lights were dimmed and ambient noise was kept low. The rest of the testing was completed in a standard air-conditioned laboratory. For all the measures, the left side was tested first followed by the right side.
Statistical analysis
The SPSS 12.0 statistical package for Windows was used for analyses. A two sample t-tests determined within subject side to side differences for all measures. A multi-variate analysis of covariance (MANCOVA) was used to compare differences between the chronic whiplash group and controls. SCL-90-R scores were entered as covariates in the analysis.
Receiver Operating Characteristic (ROC) Analysis was determined to examine the ability of each variable to discriminate between the groups. Variables with a greater predictive capacity based on the significance level (p < 0.01) were entered in a logistic regression analysis to determine the best combination to predict group membership. The regression analysis was then subjected to cross-validation analysis (leave one out) to examine its reliability and generalisability.
To determine differences in sensory measures between whiplash participants with or without arm pain, Mann-Whitney U test was used. The presence of arm pain was
defined as any pain (spontaneous or evoked) distal to the shoulder reported by the participants. For all analyses significance was set at p<0.05.
RESULTS Demographic details
For the whiplash group, the mean (SD) symptom duration post injury was 16 ± 11 months. Twenty-four patients were involved in ongoing compensation claims; four had settled their claims and three had no compensation involved. The mean (SD) NDI score was 45.9% ± 18.8%, a moderate level of disability (Vernon and Mior 1991). Forty-five percent of whiplash patients reported arm pain at the time of testing and 66%
experienced headache. Side to side differences
There were no side to side differences for any variable in both groups (all p>0.05). The mean of left and right sides were calculated and used for further analysis.
BPPT
The whiplash group demonstrated less elbow extension at pain threshold (-22.3 ± 27.4º) (p=0.05) and higher VAS scores (2.4 ± 2.3) compared to the control group (elbow extension: -11.0 ± 5.9º; VAS: 0.7 ± 1.1) (p=0.05).
Quantitative sensory testing
Pain thresholds
The whiplash group demonstrated lower PPT’s at all test sites compared to controls (p<0.05) (Table 1)
There was no significant difference between the two groups for heat pain thresholds (p > 0.1), while cold pain thresholds were significantly reduced (pain at a higher temperature) at both sites in the whiplash group (p < 0.01) (Table 1).
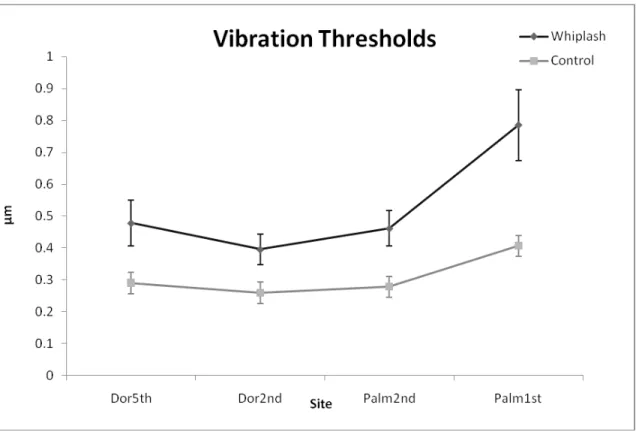
Vibration threshold
Figure (1) shows the average parameters for vibration threshold (mean and SD data shown in Table 1). The whiplash group demonstrated elevated detection thresholds for all sites compared to the control group (p < 0.05).
Thermal detection thresholds
Heat detection thresholds were higher in the whiplash group for all test sites compared to the control group (p < 0.01). Cold detection thresholds were reduced (detection at a lower temperature) in the whiplash group at the 5th metacarpal site (p < 0.05) but no different
from the controls at the 2nd metacarpal area (p>0.1) (Figure 2).
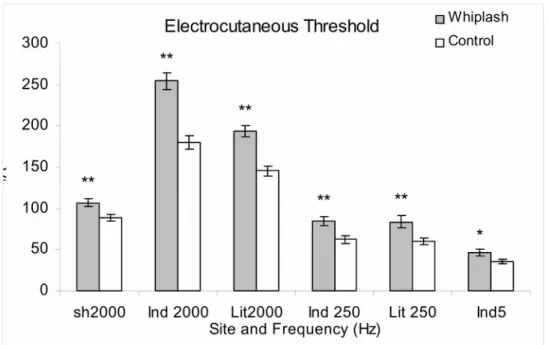
Electrocutaneous stimulation thresholds
At 2000Hz, the whiplash group demonstrated elevated electrical detection thresholds at the shoulder, index and little finger sites (p<0.01). At 250 Hz the whiplash group
demonstrated elevated electrical detection thresholds at the index and little finger sites (p < 0.01) and at 5Hz the same group showed elevated detection thresholds at the index finger site (p < 0.05) (Figure 3). There was no difference between the groups for electrical detection thresholds measured at Tibialis Anterior (p=0.83).
At 250 Hz, the whiplash group demonstrated lowered pain thresholds at all sites (p < 0.05). At tibialis anterior a 37% decrease was found, while at all other sites, the whiplash group demonstrated a 20% decrease in pain thresholds.
For the electrocutaneous pain over detection threshold ratios, the whiplash group showed differences at all sites when compared to controls (p < 0.01) (Figure 4). The index and little finger sites were found to have a pain over detection threshold ratio of less than two (Table 1).
Sympathetic vasoconstrictor reflex
The whiplash group demonstrated higher QI (76.00 ± 12.54) (p=0.05) and lower SRF (0.55 ± 0.17) (p=0.05) indicating reduced vasoconstriction when compared to the control group (QI: 68.17 ± 7.58; SRF: 0.65 ± 0.08).
ROC analysis
Areas under the curve for ROC analysis for all of the sensory tests are presented in Table 2. Summary of the ROC analysis is presented in table 2. Logistic regression showed that C5/) and median nerve PPT, 2nd metacarpal heat detection threshold and index finger
2000Hz detection and pain over detection ratio were the strongest variables and predicted group membership at 96.77%.
Cross validation demonstrated that the four variables combined revealed high sensitivity and specificity to predict group membership (90.32%).
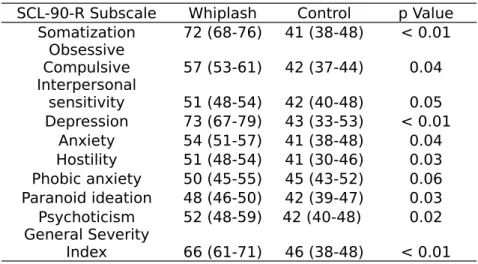
Psychological Distress (SCL-90-R)
The whiplash subjects showed elevated distress, in particular the subscales of
somatization (72 ± 4 vs 41± 5), depression (73 ± 6 vs 43 ± 5) and general severity index (66 ± 5 vs 46 ± 5) compared to controls (p = 0.01) (Table 3). Comparing the means of the General Severity Index, 21 out of the 31 whiplash participants (68%) demonstrated elevated scores above the population norms (Derogatis 1977). However, when
SCL-90-R scores were entered into the analysis as a covariate, group differences remained significant for all measures (p<0.05) and the effect size on the sensory measures was small (ŋ2 ranged from 0.031 to 0.157).
Arm pain vs no arm pain
There was no difference between patients with reported arm pain (n=13) and those without for age, gender and all QST measures (p > 0.05). There was no difference between the groups for NDI scores (arm pain 42.8 ± 15.0; no arm pain 44.8 ± 20.9) (p = 1.27).
DISCUSSION
The results of this study confirm the presence of generalised sensory hypersensitivity in chronic whiplash. Consistent findings of widespread decreased pain thresholds to a variety of sensory stimuli (pressure, thermal, electrical) likely reflects augmented central pain processes as a contributing factor to whiplash pain (Curatolo et al. 2001, Moog et al. 2002). For the first time, the results of this study demonstrate the additional presence of elevated detection thresholds or hypoaesthesia.
Hypoaesthesia was found for vibration, electrical and thermal stimulation. Vibration thresholds were elevated by an average of 40% and present across areas of the hands innervated by the lower cervical nerve roots. This is consistent with dysfunction of large myelinated or A-beta sensory fibres (Greening and Lynn 1998, Lang et al 1995). Altered vibration detection sense is thought to be an early indicator of neural pathology (Greening et al 2003). Electrical stimulation at detection threshold levels bypasses receptors and directly stimulates A-beta fibre afferents (Eliav et al 2003). Thus the elevation of
electrical detection thresholds, across the innervation zones of the three upper limb peripheral nerve trunks is also consistent with A-beta fibre dysfunction.
Our findings of elevated electrical detection thresholds with three stimulus frequencies may indicate the presence of both large and small sensory fibre dysfunction. Whilst it has never been reliably shown in humans, it has been suggested that electrical detection threshold testing may be able to discriminate large and small fibre function based on the frequency of current utilised. Large myelinated fibres (A-beta fibres), small myelinated fibres (A-delta fibres) and unmyelinated fibres (C-fibres) may be selectively activated by 2000Hz, 250Hz and 5Hz frequencies respectively (Rendell et al 1989). Whilst the
prevalence of elevated electrical detection thresholds was higher with a frequency of 2000Hz, similar changes were also found at frequencies of 250Hz and 5Hz indicating potential involvement across nerve fibre types. Results from thermal detection threshold testing support this, where elevated warmth detection thresholds and to a lesser extent cold detection threshold were demonstrated suggesting disturbances in both C and A-delta fibre function respectively. The whiplash injured participants also demonstrated reduced sympathetic nervous system vasoconstriction indicating further neural dysfunction in terms of sympathetic fibre impairment and is consistent with previous investigations of whiplash (Sterling et al. 2003a).
The sensory changes occurred bilaterally and there was no difference between
participants with or without arm pain. This could be perceived as unusual where some arm pain or other symptoms would be expected in the presence of a neuropathy. However, animal studies have shown that peripheral neural pathology in one area can cause widespread effects, including effects in apparently uninvolved limbs (Kleinschnitz
et al 2005, Koltzenburg et al 1999). Whilst most studies have demonstrated these effects to be positive symptoms such as allodynia and hyperalgesia (Hubbard and Winkelstein 2005, Kleinschnitz et al. 2005), negative symptoms (sensation loss) have also been described (Oaklander and Brown 2004). Greening et al, (2003) have shown that
asymptomatic office workers manifest similar sensory dysfunction to patients with non-specific arm pain indicating a possible subclinical presentation, and a similar
mechanism may be present in our whiplash cohort without arm symptoms.
The hypoaesthetic changes were widespread across dermatomes and as such may be another manifestation of disordered central pain processing rather than an indication of peripheral nerve dysfunction (Tucker et al 2007). One factor negating this is that
electrical detection thresholds at the remote site (Tibialis Anterior) were no different from control data whereas electrical and pressure pain thresholds were lower at this site in the whiplash group. This suggests different underlying mechanisms for the hypoesthesia and hyperalgesia seen in our whiplash cohort. Interestingly fibromyalgia (a condition thought to reflect central nervous system hyperexcitability) seems to manifest pain
hypersensitivity but normal perception thresholds (Arroyo and Cohen 1993, Gracely et al 2003) indicating different underlying mechanisms between these two conditions. It is possible that the whiplash condition includes both central and peripheral mechanisms. Further investigation utilising relatively objective tests such as nerve conduction studies, electromyography and evoked potentials may provide further information of specific processes underlying whiplash.
Nonetheless some of our findings provide further new evidence for the presence of central pain processing changes in WAD. Reduced electrocutaneous pain/detection
threshold ratios occurred at all sites with a ratio of less than two in finger sites. Although yet to be validated, Sang et al (2003) proposed that A-beta fibre mediated allodynia can be identified when the electrical current evokes pain at or close to detection threshold. From investigation of healthy control subjects, these authors propose a ratio of less than two is abnormal and indicates altered central nervous system processing of A-beta input. Our results suggest that such processes are likely involved in whiplash pain and reinforce the consistent findings of central hyperexcitability in this group.
A combination of pain sensitivity (mechanical hyperalgesia in the neck and upper limbs; electrical pain/detection ratio) and detection thresholds (heat, electrical detection in the C6 innervated area) best predicted membership to either the whiplash or control group with a high classification rate (90.32% after cross validation). This suggests a
combination of mechanisms contribute to persistent whiplash pain. The high
classification rate of these measures suggests that the use of QST in the assessment of chronic WAD may be necessary. However, due to the costly nature of the equipment and the lengthy time required for testing, further evaluation of these measures is required before they could be efficiently used in the clinical situation. The QST conducted in this study were not carried out by a blind assessor. This is a short coming of the study and the results should be viewed cautiously until their replication is established.
Our whiplash patient group exhibited psychological distress consistent with previous findings (Curatolo et al. 2001, Kessels et al 1998, Moog et al. 2002, Sterling et al 2003b) and it is well documented that psychological distress may influence pain threshold measures (Rhudy and Meagher 2000). For this reason we included SCL-90 scores as a covariate in the group analyses of sensory data. Group differences for all sensory
measures remained unchanged and the effect sizes were very small. Whilst it is
acknowledged that other psychological constructs were not measured in this study, our previous data would support the current findings that the sensory disturbances of whiplash cannot be fully explained by psychological factors alone and likely reflect physiological changes or a complex interplay between these substrates (Sterling et al. 2003a, Sterling and Kenardy 2006).
In summary, the findings of this study confirm the existence of sensory hypersensitivity in chronic WAD. Moreover, patients with chronic whiplash also demonstrated the presence of hypoaesthesia, particularly in the lower cervical dermatomes. These findings may indicate the additional presence of peripheral afferent nerve fibre involvement in the whiplash condition but could be a further manifestation of disordered central pain
processing. A combination of pain threshold and detection measures discriminated whiplash and control subjects. These findings suggest that assessment of whiplash injured patients may need to include more detailed sensory testing using QST and this could have implications for the management of this condition.
References
Adriaensen H, Gybels J, Handwerker HO and Van Hees J (1983): Response properties of thin myelinated (A-delta) fibers in human skin nerves. Journal of Neurophysiology 49: 111-122.
Alpar EK, Onuoha G, Killampalli VV and Waters R (2002): Management of chronic pain in whiplash injury. Journal of Bone and Joint Surgery-British Volume 84B: 807-811. Arroyo JF and Cohen ML (1993): Abnormal responses to electrocutaneous stimulation in fibromyalgia. Journal of Rheumatology 20: 1925-1931.
Balster SM and Jull GA (1997): Upper trapezius muscle activity during the brachial plexus tension test in asymptomatic subjects. Man Ther 2: 144-149.
Barnsley L, Lord S and Bogduk N (1998): The pathophysiology of whiplash. Spine: State
of the art reviews 12: 209-242.
Chaudhry V, Corse AM, Freimer ML, Glass JD, Mellits ED, Kuncl RW, Quaskey SA and Cornblath DR (1994): Inter- and intraexaminer reliability of nerve conduction measurements in patients with diabetic neuropathy. Neurology 44: 1459-1462.
Curatolo M, Petersen-Felix S, Arendt-Nielsen L, Giani C, Zbinden AM and Radanov BP (2001): Central hypersensitivity in chronic pain after whiplash injury. Clinical Journal of
Pain 17: 306-315.
Cusick JF, Pintar FA and Yoganandan N (2001): Whiplash syndrome: kinematic factors influencing pain patterns. Spine 26: 1252-1258.
Derogatis LR (1977): SCL-90-R Administration, Scoring and Practice Manual. Clinical
Psychiatric Research.
Edwards RR, Sarlani E, Wesselmann U and Fillingim RB (2005): Quantitative
assessment of experimental pain perception: multiple domains of clinical relevance. Pain 114: 315-319.
Eliav E, Teich S, Nitzan D, El Raziq DA, Nahlieli O, Tal M, Gracely RH and Benoliel R (2003): Facial arthralgia and myalgia: can they be differentiated by trigeminal sensory assessment? Pain 104: 481-490.
Fowler CJ, Sitzoglou K, Ali Z and Halonen P (1988): The conduction velocities of peripheral nerve fibres conveying sensations of warming and cooling. Journal of
Neurology, Neurosurgery and Psychiatry 51: 1164-1170.
Gracely RH, Grant MA and Giesecke T (2003): Evoked pain measures in fibromyalgia.
Best Practice and Research. Clinical Rheumatology 17: 593-609.
Greening J, Dilley A and Lynn B (2005): In vivo study of nerve movement and
mechanosensitivity of the median nerve in whiplash and non-specific arm pain patients.
Pain 115: 248-253.
Greening J and Lynn B (1998): Vibration sense in the upper limb in patients with repetitive strain injury and a group of at-risk office workers. International Archives of
Occupational and Environmental Health 71: 29-34.
Greening J, Lynn B and Leary R (2003): Sensory and Autonomic Function In The Hands Of Patients With non-Specific Arm Pain (NSAP) and Asymptomatic office workers.
Pain 104: 275-281.
Hallin RG, Torebjork HE and Wiesenfeld Z (1982): Nociceptors and warm receptors innervated by C fibres in human skin. Journal of Neurology, Neurosurgery and
Hubbard RD and Winkelstein BA (2005): Transient cervical nerve root compression in the rat induces bilateral forepaw allodynia and spinal glial activation: mechanical factors in painful neck injuries. Spine 30: 1924-1932.
Hurtig I, Raak R, Kendall S, Gerdle B and Wahren L (2001): Quantitative sensory testing in fibromylagia patients and in healthy subjects: identification of subgroups. Clinical
Journal of Pain 17: 316-322.
Ide M, Ide J, Yamaga M and Takagi K (2001): Symptoms and signs of irritation of the brachial plexus in whiplash injuries. Journal of Bone and Joint Surgery. British Volume 83: 226-229.
Kasch H, Qerama E, Bach FW and Jensen TS (2004): Reduced cold pressor pain tolerance in non-recovered whiplash patients: a 1-year prospective study. European
Journal of Pain In Press, Corrected Proof.
Katims JJ, Long DM and Ng LK (1986): Transcutaneous nerve stimulation. Frequency and waveform specificity in humans. Applied Neurophysiology 49: 86-91.
Katims JJ, Naviasky EH, Rendell MS, Ng LK and Bleecker ML (1987): Constant current sine wave transcutaneous nerve stimulation for the evaluation of peripheral neuropathy.
Archives of Physical Medicine and Rehabilitation 68: 210-213.
Kessels RP, Keyser A, Verhagen WI and van Luijtelaar EL (1998): The whiplash syndrome: a psychophysiological and neuropsychological study towards attention. Acta
Neurologica Scandinavica 97: 188-193.
Kleinschnitz C, Brinkhoff J, Sommer C and Stoll G (2005): Contralateral cytokine gene induction after peripheral nerve lesions: dependence on the mode of injury and NMDA receptor signaling. Brain Research. Molecular Brain Research 136: 23-28.
Koltzenburg M, Wall PD and McMahon SB (1999): Does the right side know what the left is doing? Trends in Neurosciences 22: 122-127.
Lang E, Claus D, Neundorfer B and Handwerker HO (1995): Parameters of thick and thin nerve-fiber functions as predictors of pain in carpal tunnel syndrome. Pain 60: 295-302. Moog M, Quintner J, Hall T and Zusman M (2002): The late whiplash syndrome: a psychophysical study. European Journal of Pain-London 6: 283-294.
Oaklander AL and Brown JM (2004): Unilateral nerve injury produces bilateral loss of distal innervation. Annals of Neurology 55: 639-644.
Ortengren T, Hansson HA, Lovsund P, Svensson MY, Suneson A and Saljo A (1996): Membrane leakage in spinal ganglion nerve cells induced by experimental whiplash extension motion: a study in pigs. Journal of Neurotrauma 13: 171-180.
Rendell MS, Katims JJ, Richter R and Rowland F (1989): A comparison of nerve conduction velocities and current perception thresholds as correlates of clinical severity of diabetic sensory neuropathy. Journal of Neurology, Neurosurgery and Psychiatry 52: 502-511.
Rhudy JL and Meagher MW (2000): Fear and anxiety: divergent effects on human pain thresholds. Pain 84: 65-75.
Rolke R, Magerl W, Campbell KA, Schalber C, Caspari S, Birklein F and Treede RD (2006): Quantitative sensory testing: a comprehensive protocol for clinical trials.
European Journal of Pain 10: 77-88.
Sang CN, Max MB and Gracely RH (2003): Stability and reliability of detection thresholds for human A-beta and A-Delta sensory afferents determined by cutaneous electrical stimulation. Journal of Pain and Symptom Management 25: 64-73.
Schurmann M, Gradl G, Andress HJ, Furst H and Schildberg FW (1999): Assessment of peripheral sympathetic nervous function for diagnosing early post-traumatic complex regional pain syndrome type I. Pain 80: 149-159.
Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S and Zeiss E (1995): Scientific Monograph of the Quebec Task-Force on Whiplash-Associated Disorders - Redefining Whiplash and Its Management. Spine 20: S1-S73.
Sterling M, Jull G, Vicenzino B and Kenardy J (2003a): Sensory Hypersensitivity Occurs Soon After Whiplash Injury and Is Associated With Poor Recovery. Pain 104: 509-517. Sterling M, Jull G, Vicenzino B, Kenardy J and Darnell R (2005): Physical and
psychological factors predict outcome following whiplash injury. Pain 114: 141-148. Sterling M and Kenardy J (2006): The relationship between sensory and sympathetic nervous system changes and posttraumatic stress reaction following whiplash injury--a prospective study. Journal of Psychosomatic Research 60: 387-393.
Sterling M, Kenardy J, Jull G and Vicenzino B (2003b): The development of psychological changes following whiplash injury. Pain 106: 481-489.
Sterling M, Treleaven J, Edwards SL and Jull G (2002a): Pressure pain thresholds in chronic whiplash associated disorder: further evidence of altered central pain processing.
Journal of Musculoskeletal Pain 10: 69-81.
Sterling M, Treleaven J and Jull G (2002b): Responses to a clinical test of mechanical provocation of nerve tissue in whiplash associated disorder. Manual Therapy 7: 89-94. Taylor J and Taylor M (1996): Cervical spinal injuries: an autopsy study of 109 blunt injuries. Journal of Musculoskeletal Pain 29: 335-339.
Vernon H and Mior S (1991): The Neck Disability Index - a Study of Reliability and Validity. Journal of Manipulative and Physiological Therapeutics 14: 409-415.
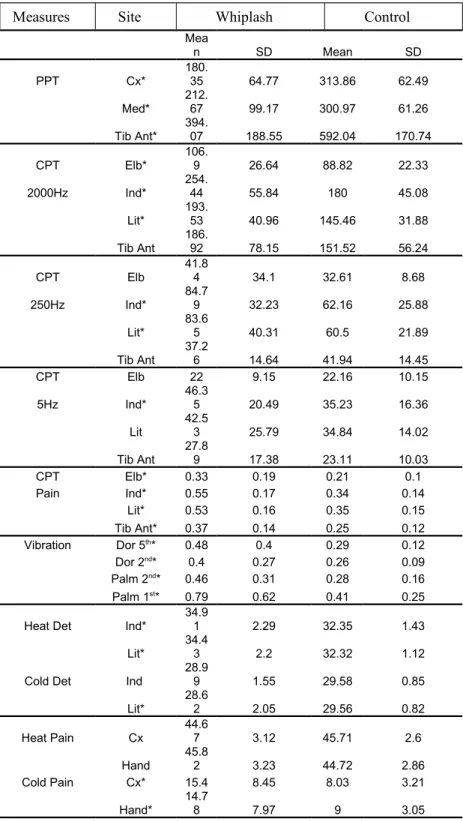
Table 1. Mean and standard deviation values for each variable.
Measures Site Whiplash Control
Mea n SD Mean SD PPT Cx* 180. 35 64.77 313.86 62.49 Med* 212. 67 99.17 300.97 61.26 Tib Ant* 394. 07 188.55 592.04 170.74 CPT Elb* 106. 9 26.64 88.82 22.33 2000Hz Ind* 254. 44 55.84 180 45.08 Lit* 193. 53 40.96 145.46 31.88 Tib Ant 186. 92 78.15 151.52 56.24 CPT Elb 41.8 4 34.1 32.61 8.68 250Hz Ind* 84.79 32.23 62.16 25.88 Lit* 83.6 5 40.31 60.5 21.89 Tib Ant 37.2 6 14.64 41.94 14.45 CPT Elb 22 9.15 22.16 10.15 5Hz Ind* 46.3 5 20.49 35.23 16.36 Lit 42.5 3 25.79 34.84 14.02 Tib Ant 27.8 9 17.38 23.11 10.03 CPT Elb* 0.33 0.19 0.21 0.1 Pain Ind* 0.55 0.17 0.34 0.14 Lit* 0.53 0.16 0.35 0.15 Tib Ant* 0.37 0.14 0.25 0.12 Vibration Dor 5th* 0.48 0.4 0.29 0.12 Dor 2nd* 0.4 0.27 0.26 0.09 Palm 2nd* 0.46 0.31 0.28 0.16 Palm 1st* 0.79 0.62 0.41 0.25
Heat Det Ind*
34.9
1 2.29 32.35 1.43
Lit*
34.4
3 2.2 32.32 1.12
Cold Det Ind
28.9 9 1.55 29.58 0.85 Lit* 28.62 2.05 29.56 0.82 Heat Pain Cx 44.6 7 3.12 45.71 2.6 Hand 45.8 2 3.23 44.72 2.86 Cold Pain Cx* 15.4 8.45 8.03 3.21 Hand* 14.7 8 7.97 9 3.05
PPT = Pressure pain threshold, Cx = cervical spine, Med = median nerve, Tib Ant = Tibialis anterior; CPT = Current perception threshold, Elb = elbow, ind = index finger, Lit = little finger; Dor5th and Dor2nd = dorsum surface of the 5th and 2nd metacarpal,
Palm1st and Palm2nd = palmar surface of the 1st and 2nd metacarpal; Heat Det and Cold
Det = Heat and cold detection thresholds.
Table 2. ROC curves, area under the curve and its significance to discriminate between the whiplash and control groups , for all variables.
Variable Area Standard Error Significance
C5/6 PPT 0.92 0.05 0.00*
Index finger 2000hz detection
threshold 0.9 0.04 0.00*
2nd Metacarpal heat detection
threshold 0.89 0.05 0.00*
5th metacarpal heat detection threshold 0.86 0.05 0.00*
Little finger, 2000Hz detection
threshold 0.86 0.05 0.00*
Index finger, pain over detection ration 0.84 0.06 0.00*
Tib ant PPT 0.8 0.06 0.00*
Little finger, pain over detection ratio 0.79 0.06 0.00*
Median nerve PPT 0.78 0.07 0.00*
Tib Ant, pain over detection ratio 0.76 0.07 0.00*
QI Value 0.73 0.07 0.01
Little finger, 250Hz detection threshold 0.72 0.07 0.01
SVR Value 0.71 0.08 0.01
Cx cold pain threshold 0.71 0.08 0.01
Hand cold pain threshold 0.71 0.08 0.01
Index finger, 250Hz detection
threshold 0.71 0.07 0.01
Shoulder, pain over detection ratio 0.7 0.07 0.01
Index finger, 5Hz detection threshold 0.69 0.07 0.02
5th metacarpal, cold detection
threshold 0.69 0.08 0.02
Shoulder, 2000Hz detection threshold 0.68 0.07 0.03
Dorsum 5th Metacarpal, VDT 0.68 0.08 0.03
Palmr 1st metacarpal, VDT 0.68 0.08 0.02
Palmar 2nd metacarpal, VDT 0.67 0.08 0.03
Tib ant, 2000Hz detection threshold 0.65 0.08 0.06
Dorsum 2nd metacarpal, VDT 0.63 0.08 0.10
Hand, heat pain threshold 0.61 0.08 0.18
Tib ant, 250Hz detection threshold 0.61 0.08 0.18
Little finger, 5Hz detection threshold 0.61 0.08 0.17
2nd Metacarpal, cold detection
threshold 0.6 0.08 0.22
Tib Ant, 5Hz detection threshold 0.57 0.09 0.41
Shoulder, 250Hz detection threshold 0.56 0.08 0.50
Cx heat pain threshold 0.56 0.08 0.45
Table 3. SCL-90-R Psychological subscales (mean ± SD) for whiplash and control groups.
SCL-90-R Subscale Whiplash Control p Value
Somatization 72 (68-76) 41 (38-48) < 0.01 Obsessive Compulsive 57 (53-61) 42 (37-44) 0.04 Interpersonal sensitivity 51 (48-54) 42 (40-48) 0.05 Depression 73 (67-79) 43 (33-53) < 0.01 Anxiety 54 (51-57) 41 (38-48) 0.04 Hostility 51 (48-54) 41 (30-46) 0.03 Phobic anxiety 50 (45-55) 45 (43-52) 0.06 Paranoid ideation 48 (46-50) 42 (39-47) 0.03 Psychoticism 52 (48-59) 42 (40-48) 0.02 General Severity Index 66 (61-71) 46 (38-48) < 0.01
Figures
Figure 1. Mean (± SE) vibration thresholds in the whiplash group and control groups. The stimulus was applied over areas of the hand innervated by C6 (Palm 1st), C7 (Palm 2nd,
Dor 2nd) and C8 dermatomes (Dor 5th). * p < 0.05 significantly different from the control group.
Figure 2. Thermal (warmth and cold) detection thresholds (Means ± SE) in the whiplash group and control groups. The stimulus was applied over the dorsum aspect of the hand corresponding to the C7 (Ind: dorsum over the 2nd metacarpal) and C8 (Lit: dorsum of the
5th metacarpal) dermatomes. ** p < 0.01, * p < 0.05 significantly different from the
Figure 3. Electrocutaneous detection thresholds (Mean ± SE). The figure illustrates the sites and frequencies demonstrating significant difference between the whiplash and control groups. ** p < 0.01, * p < 0.05 significantly different from the control group, respectively.
(Sh2000, anterior shoulder 2000Hz (C5/6); Ind2000, Index finger 2000Hz (C7); Lit2000, Little finger 2000Hz (C8); Ind250, Index finger 250Hz (C7); Lit250, Little finger 250Hz (C8); Ind5, Index finger 5Hz (C8).
Figure 4. Ratio of electrocutaneous detection threshold / electrocutaneous pain thresholds for the whiplash and control groups (Mean ± SE). The whiplash group showed