Maternal arsenic exposure and DNA damage biomarkers—the associations with birth outcomes in a general population from Taiwan [Please note that your target journal requires you to include a study design descriptive in the title.]
Wei-Chun Chou1,2, Yu-The Chung2, Hsiao-Yen Chen2, Chien-Jen Wang2, Tsung-Ho Ying3, Chun-Yu Chuang1*, Shu-Li Wang2,4*
1Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan
2Division of Environmental Health and Occupational Medicine, National Health Research Institutes, Zhunan, Miaoli County, Taiwan
3Department of Obstetrics and Gynecology, Chung Shan Medical University Hospital, Taichung, Taiwan
4Epidemiology Branch, National Institutes and Environmental Health Sciences, National Institutes of Health, Department of Health and Human Services, Research Triangle Park, North Carolina, USA
Short title: Maternal arsenic, DNA damage, and birth outcomes
Abstract (243 words)
Inorganic arsenic (iAs) is an established transplacental agent known to affect fetal 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
development in animal studies. However, iAs has not been adequately studied in the general population with respect to iAs exposure during pregnancy and its impact on the health status of newborns. The aims of this study were to 1) elucidate the association between arsenic exposure and oxidative/methylated DNA damage in pregnant women, and 2) determine the association with birth outcomes. A birth cohort study of 299 pregnant mother-newborn pairs was recruited during 2001–2002 in Taiwan. We collected maternal urine samples during the 3rd trimester for measuring iAs and its metabolites. We used high-performance liquid
chromatography/inductively coupled plasma mass spectrometry (HPLC-ICP-MS) for quantifications of the arsenic species. Liquid chromatography/tandem mass
spectrometer (LC-MS/MS) was used to measure the 8-oxo-7,8-dihydro-2′-deoxyguanosine (8-oxodG) and N7-methylguanosine (N7-MeG) DNA damage biomarkers. Birth outcomes were collected to assess the associations with maternal arsenic exposure and the DNA damage biomarkers. Multiple regression analyses showed that maternal urinary iAs had positive associations with the methylated N7 -MeG (beta = 0.35, p < 0.001) and oxidative 8-oxodG (beta = 0.24, p < 0.001) DNA damage biomarkers, and a decreased one-minute (1-min) Apgar score (beta = -0.23, p = 0.041). Maternal N7-MeG was also associated with a decreased 1-min Apgar score (beta = -0.25, p = 0.042). Mutual adjustment for iAs and N7-MeG showed an
22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
independent and significant prediction for a decreased 1-min Apgar score of iAs (beta = -0.28, p = 0.036). Maternal iAs exposure was associated with both maternal DNA damage and adverse newborn health. We report that maternal N7-MeG levels are a biomarker for monitoring fetal health.
Key Words: Maternal exposure, arsenic, Apgar score, DNA damage, birth weight 41 42 43 44 45 46
Introduction
Health status at birth is an important determinant of morbidity and mortality in early childhood [1] and of chronic disease in adulthood [2]. For example, birth weight is not only reflective of maternal health status, but also predictive of the probability for newborn survival, development, and long-term health [3]. The Apgar score is a routine for evaluating the physical condition of the newborn, including heart rate, respiratory effort, muscle tone, reflex irritability, and skin color shortly after delivery. A score ≥ 7 indicates that the condition of the newborn is good-to-excellent [4]. Otherwise, immediate extra medical care or even an intensive care unit admission would be necessary. Newborns with low birth weight (LBW) or low Apgar scores often develop various negative health consequences. Long-term effects of LBW include increased risk of cardiovascular disease, type 2 diabetes mellitus, and
impaired reproductive function [5]. Several studies have shown that low Apgar scores may be associated with an increased risk of reduced cognitive function and increased learning difficulties later in life [6]. Arsenic is a well-known toxicant and carcinogen, and increasing evidence indicates that arsenic may adversely affect pregnancy
outcomes and development of the newborn.
Arsenic easily crosses the placenta [7], and even moderate exposure to arsenic during 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66
pregnancy has been associated with adverse health outcomes in the fetus [8]. Studies have shown that prenatal arsenic exposure is inversely associated with birth weight in Bangladesh , and Inner Mongolia [11]. Prenatal arsenic exposure at low-to-moderate levels might also have effects on the fetus, but more evidence is needed [12].
Disrupted placentation [13] and endocrine disturbance [14] have been reported for arsenic-related adverse pregnancy outcomes. However, the mechanisms require further investigation. Studies of mice have reported that arsenic leads to an increase in oxidative stress and a subsequent increase in 8-oxo-7,8-dihydro-2′-deoxyguanosine (8-oxodG), resulting in oxidative DNA damage in tissues [15,16]. Increased urinary 8-oxodG in pregnant women has been linked to arsenic exposure [17]. Recently, maternal DNA damage mediated by arsenic exposure has been proposed as one mechanism responsible for fetal programming [18]. There is, however, little information on the formation of methylated DNA damage induced by arsenic exposure. Arsenic-treated mice have an arsenic-related increase in hepatic N7 -methylguanine (N7-MeG), a marker of methylated DNA damage that reflects the overall rate of DNA methylation [19,20], but this finding has not been confirmed in humans.
We sought to determine whether prenatal exposure to low-to-moderate levels of 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86
arsenic is associated with maternal oxidative/methylated DNA damage, and to evaluate the associations with birth outcomes, including LBW and low Apgar scores in a general population from central Taiwan. [Did you succeed? Your target journal wants a statement about your level of success.]
Methods
Ethics statement
The Human Ethical Committee of the National Health Research Institutes in Taiwan approved this study. Before participating in the study, all pregnant women signed informed consent forms after receiving detailed explanations of the benefits and risks.
Study participants
There is no record of high arsenic exposure in this study region; and, a representative sample for the general population was planned. [Is this the correct word here?] Subject recruitment [21] and preliminary results [22] were described previously. Briefly, all pregnant women who received care at the local medical center serving the general population were invited to join our study between December 2000 and 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106
November 2001 (Figure 1). The pregnant women were generally healthy and living in the local area with good prenatal appointment compliance. Initially, 430 of 610 pregnant women were volunteers recruited at 8 weeks gestation on average. The subjects provided urine samples during the third trimester (28–38 weeks gestation). Of the 430 pregnant women, 107 did not have sufficient data or provide urine, and 10 women who smoked cigarettes were excluded. To facilitate compliance with an independent outcomes assumption, one of the two subjects was randomly selected for the nine pairs of twins. In addition, we had missing data on 5 newborn heath
assessments due to loss to follow-up. Consequently, a total of 299 mother-newborn pairs were reported.
Determination of arsenic metabolites
The pregnant women collected urine in a 200-ml paper cup. The research assistant then allocated the urine specimens to 10-ml polypropylene tubes and stored them in a -20°C freezer until analysis. The concentrations of arsenite (As3+), arsenate (As5+), monomethylarsonic acid (MMA), and dimethyl arsenate (DMA) in the urine samples were measured using high-performance liquid chromatography/inductively coupled plasma mass spectrometry (HPLC-ICP-MS). We used anion exchange columns (Hamilton PRP X-100 [10 μm particle size, 250 mm × 4.1 mm]) for arsenic 107 108 109 110 111 112 113 114 115 116 117 118 119 120 121 122 123 124 125 126
speciation. The mobile phase was 100 mmol/ L Na2HPO4/ NaH2PO4 (pH = 5.75) at a flow rate of 1 mL/min. The limitations of detection (LOD) for the various species were 0.09 μg/L for As3+, 0.05 μg/L for As5+, 0.05 μg/L for MMA, and 0.04 μg/L for DMA.
Blanks were analyzed every 10 samples and the results were < 0.01 µg/L of arsenic. Five standards spanning the range of urinary arsenic concentrations were used to set the calibration curve in each run of 10 samples. The analysis of samples proceeded only when the correlation coefficients of the standard curves with outcomes were > 0.999. Duplicates were run every 10 samples and the coefficients of variance (CV %) were < 5%. The recovery rate was between 90% and 110% with standard addition relevant to samples ranging from 2–5 µg/L for all arsenic species. The interbatch CVs were < 10% in all samples ranging from 4.9%–7.8%. The inter-lab comparisons were conducted by participating in the Round Table Program organized by Recipe
Chemicals and Instruments GmbH (Munich, Germany). We fulfilled the reference values for all tested samples.
Creatinine was measured by the Beckman Synchron LX20 auto-system (Beckman Coulter, Brea, CA, USA) in the central lab of Chung-Ho Memorial Hospital of Kaohsiung Medical University using a spectrophotometric method with picric acid as 127 128 129 130 131 132 133 134 135 136 137 138 139 140 141 142 143 144 145 146
the reactive at 520 nm. We used total arsenic (tAs) as the sum of inorganic arsenic (As3+ and As5+) and organic arsenic (MMA and DMA) divided by the urinary creatinine in the subsequent analysis [23].
DNA damage biomarker quantification
Urinary 8-oxodG and N7-MeG were determined using liquid chromatography/tandem mass spectrometry (LC-MS/MS). Urine samples were thawed at room temperature and centrifuged at 10000g for 5 min. Then, 20 µL samples of urine were diluted 20 times with 96% acetonitrile containing 0.1% formic acid (FA; 380 µL). An 80-µL aliquot of diluted urine was spiked with 20 µL of a mixed solution consisting of 15N
5 -N7-MeG and 15N
5-8-oxodG as an internal standard and then vortexed. A 100-μL sample of prepared urine was injected directly into the on-line solid-phase extraction column (Sep-Pak C18 cartridges, 1 g/6 mL; Waters, Milford, MA, USA). After automatic sample cleanup, LC-MS/MS analysis was done using a PE Series 200 HPLC system interfaced with a PE Sciex API 3000 triple quadruple mass
spectrometer with an electrospray ion source [24]. [Manufacturers?] The LOD of the 8-oxodG and N7-MeG was 0.01 μg/L and the coefficient of variation (CV) was 2.5% and 5.5% for the 8-oxo-dG and N7-MeG, respectively.
147 148 149 150 151 152 153 154 155 156 157 158 159 160 161 162 163 164 165 166
Birth outcomes and covariates
The physical parameters of the newborns, including gestational age, sex, birth weight and height, head and chest circumference, and Apgar score, were measured and recorded by the same pediatrician and a well-trained assistant. The nurses in the maternity ward measured birth weight using a scale for babies (Misaki baby scale, Japan) that was calibrated before each use. Calibration with a standard weight (5 kg) at regular intervals showed that all scales were stable and precise. Birth length was measured to the nearest 0.1 cm using a wooden length board, and the head and chest circumferences were measured using a metal measuring tape. The Apgar score was determined for each baby to ascertain physical condition and determine the immediate need for extra medical or emergency care. A pediatrician or trained nurse assigned Apgar scores based on breathing effort, heart rate, muscle tone, reflexes, and skin color. Each category was scored with a 0, 1, or 2, according to the observed
conditions. The Apgar test was given to babies at 1 and 5 minutes [25]. The scoring scheme is shown in Appendix 1.
In the current study, adverse birth outcomes in newborns involved a low birth weight and low Apgar scores. We suggest that birth length might be correlated with the physical condition of the baby, such as body relaxation, and head and chest girth with 167 168 169 170 171 172 173 174 175 176 177 178 179 180 181 182 183 184 185 186
the mode of delivery (i.e., normal spontaneous delivery, cesarean). In the present study, adverse birth outcomes in newborns were based on LBW and low Apgar scores. LBW newborns were defined as newborns with a birth weight < 2,500 g. Newborns with low Apgar scores had a 1- or 5-min Apgar score < 7 [4]. Information on demographic or socioeconomic factors, or other factors that confounded the associations between maternal arsenic exposure, maternal DNA damage, and newborn birth outcomes was collected. We used an administrative questionnaire to obtain the demographic data of the pregnant women, such as age, parity, education, and health-related data (medical history, as well as cigarette smoking and alcohol use before and after pregnancy).
Statistical analysis
We assessed the associations between maternal arsenic exposure (iAs, MMA, and DMA), maternal DNA damage (8-oxodG and N7-MeG), and newborn health parameters (birth weight, birth length, head circumference, chest girth, and Apgar scores). Arsenic metabolites and DNA damage biomarker levels under LOD were recorded as one-half of the LOD values. All variables were assessed for normal distribution or natural logarithmic-transformation to approximate a normal
distribution. Specifically, all urinary arsenic species levels were log-transformed, and 187 188 189 190 191 192 193 194 195 196 197 198 199 200 201 202 203 204 205 206
the urinary levels of 8-oxodG and N7-MeG were natural log-transformed to obtain a normal distribution. Covariates assessed included maternal age at delivery, mode of delivery, pre-pregnancy BMI, gestational age, newborn sex, prenatal alcohol
consumption, and maternal education.
To assess differences in the characteristics between subjects who were followed and subjects lost to follow-up, we used an independent sample t-test for continuous variables and the χ2 method for categorical variables (see Supplemental Material, Table S1). Pearson correlations were used to explore the associations between maternal arsenic levels, DNA damage, newborn health status, and other covariates. Significantly correlated variables were further analyzed in multivariable regression models adjusting for potential confounders. Potential confounders were identified based on correlations (p < 0.1) with arsenic exposure and birth outcomes. There were no significant differences in the relationships in the birth outcomes and maternal iAs between the sexes; we combined data from female and male newborns to increase the statistical power.
Maternal age, pre-pregnant BMI, gestational age, mode of delivery, and newborn sex were included in the final model. We used birth outcomes as both continuous and binary variables in the linear regression model and the Cox’s proportional hazards 207 208 209 210 211 212 213 214 215 216 217 218 219 220 221 222 223 224 225 226
model, respectively. Statistical significance was set at a p < 0.05. For the Cox’s proportional hazards model estimates, we transformed continuous variables into a two-level scale to compare the above and below medians of the arsenic metabolites and DNA damage biomarkers. [Is this rewrite accurate?] We calculated the 95% CIs of the relative risks from the corresponding regression coefficients and standard errors. All statistical analyses were performed using SPSS 18.0 software (SPSS, Inc., Chicago, IL, USA).
Results
General characteristics of the subjects
Table 1 presents the characteristics of pregnant women and the newborns by sex. Of the 299 newborns, 151 (51%) were male and 148 (49%) were female. Female newborns had significantly lower birth weights than the male newborns (3170 vs. 2985 gm, p = 0.001). Twenty-one (7%) newborns had a LBW (< 2,500 g), 13 (61.9%) of which were female. Sixty-nine (20%) newborns had 1-min Apgar scores < 40, of which [How many?] were male (p = 0.15 for sex difference). In addition, the number of female newborns with low 5-min Apgar scores was significantly higher than the male newborns. [What are the numbers?] Only 5 (1.7 %) of women consumed alcohol 227 228 229 230 231 232 233 234 235 236 237 238 239 240 241 242 243 244 245 246
during pregnancy. The characteristics for the excluded twins were similar to the included twins.
Women lost to follow-up had a significantly lower average gestational age and greater income than the women who were followed. In addition, the mothers followed tended to be older and had slightly lower pre-pregnant BMIs than the mothers lost to follow-up (p < 0.1). No significant differences existed in parity, newborn birth outcomes, or arsenic levels between the groups (see Supplemental Material Table S1).
Maternal arsenic exposure and DNA damage
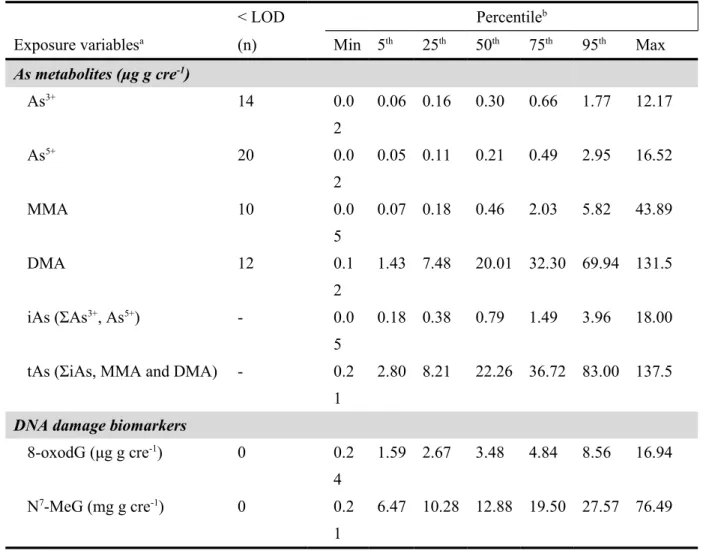
The levels and distribution of arsenic metabolites in maternal urine are shown in Table 2. The median (5th–95th) levels of creatinine-adjusted urinary As3+, As5+, MMA, DMA, iAS, and tAS were 0.30 (0.06–1.77), 0.21 (0.05–2.95), 0.46 (0.07– 5.82), 20.01 (1.43–69.94), 0.79 (0.18–3.96), and 22.26 (2.80–83.0) μg g cre-1, respectively. Among all arsenic metabolites, the frequency of samples with arsenic metabolite levels above the LODs was > 92%. The median (5th–95th) concentrations of creatinine-adjusted urinary 8-oxodG and N7-MeG were 3.48 (1.59–8.56) μg g-1 cre and 12.88 (6.47–25.57) mg g-1, respectively (Table 2).
247 248 249 250 251 252 253 254 255 256 257 258 259 260 261 262 263 264 265 266
Maternal arsenic exposure, oxidative/methylated DNA damage, and birth outcomes
Table 3 shows a significant positive correlation between maternal 8-oxodG levels and iAs (r = 0.24, p < 0.001), MMA (r = 0.16, p < 0.001), DMA (r = 0.13, p < 0.05), and tAs (r = 0.17, p < 0.001). Similarly, a significant positive correlation was shown between the maternal N7-MeG levels and iAs (r = 0.35, p < 0.001) and the metabolites. In addition, a significant positive correlation was shown between maternal 8-oxodG levels and N7-MeG (r = 0.62, p < 0.001). However, only a marginally significant negative correlation was shown between maternal iAs levels and the 1-min Apgar scores of newborns (r = -0.13, p = 0.08), whereas a significant positive correlation was noted between the maternal MMA levels and the 1-min Apgar scores of newborns (r = 0.15, p = 0.03). A marginally significant negative correlation existed between the maternal N7-MeG levels and the 1-min Apgar scores of newborns (r = -0.18, p = 0.06). The maternal MMA and DMA levels were not significantly correlated with the birth outcomes of birth weight, length, and head and chest circumferences. [Data with “marginal” significance is not really considered significant.]
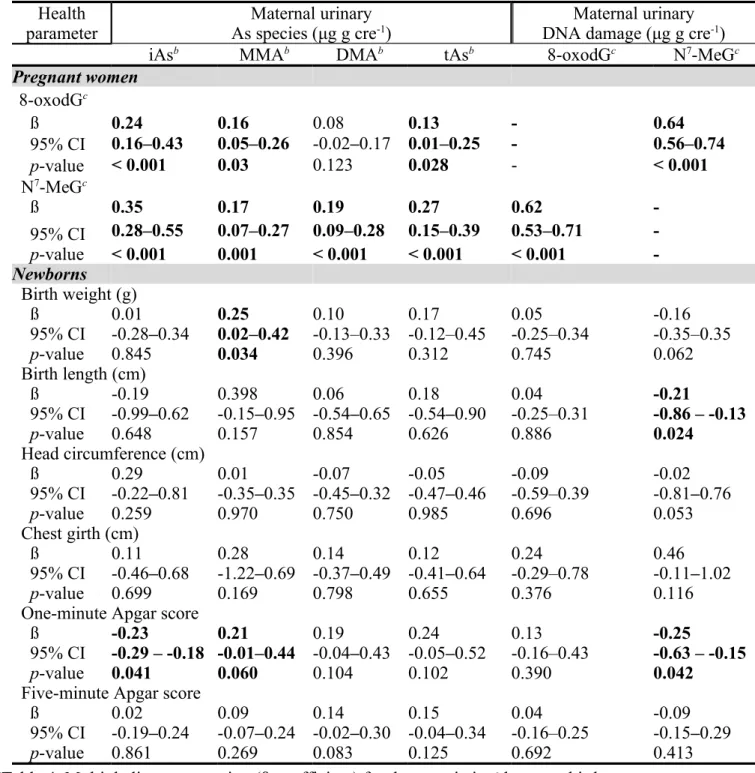
Regression analyses identified positive associations between the maternal urinary level of iAs, MMA tAs, and the DNA damage biomarkers 8-oxodG and N7-MeG 267 268 269 270 271 272 273 274 275 276 277 278 279 280 281 282 283 284 285 286
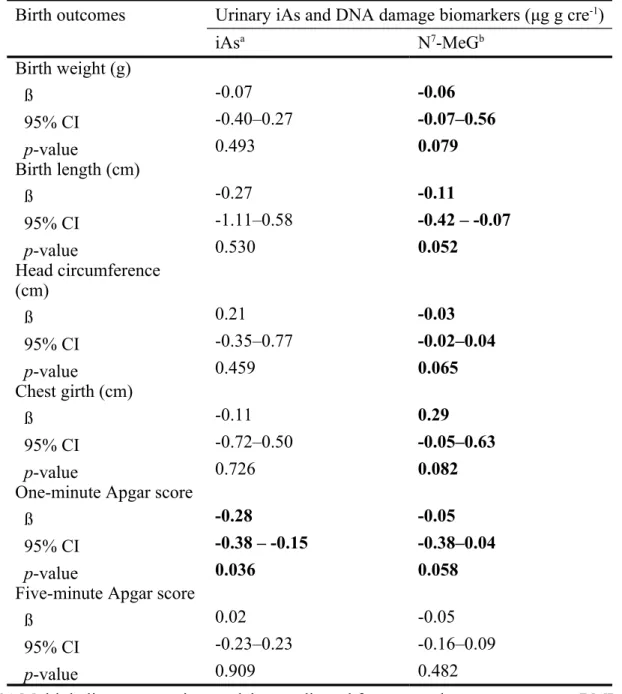
(Table 4). Maternal iAs levels had negative associations with 1-min Apgar scores (β-coefficient = -0.23, 95% CI: -0.29 – -0.18, p = 0.041). MMA had positive associations with the newborn birth weight (β = 0.25, 95% CI: -0.02–0.42, p = 0.034), and a marginally significant positive association with 1-min Apgar scores (β = 0.21, 95% CI: 0.01–0.44, p = 0.06). In addition, the DMA and tAs were not significantly associated with the 1-min Apgar score. The maternal urinary N7-MeG levels had negative associations with the birth length (β = -0.21, 95% CI: -0.86 – -0.13, p = 0.024) and 1-min Apgar score (β = -0.25, 95% CI: -0.63 – -0.15, p = 0.042). To determine whether or not the estimated effects of maternal iAs exposure on newborn health status was via methylated DNA damage, we performed a multivariable adjusted regression analysis to estimate the association between maternal iAs exposure and newborn health outcomes, controlling for N7-MeG and potential confounders (Table 5). The associations between maternal iAs levels and 1-min Apgar scores remained significant after adjusting for N7-MeG.
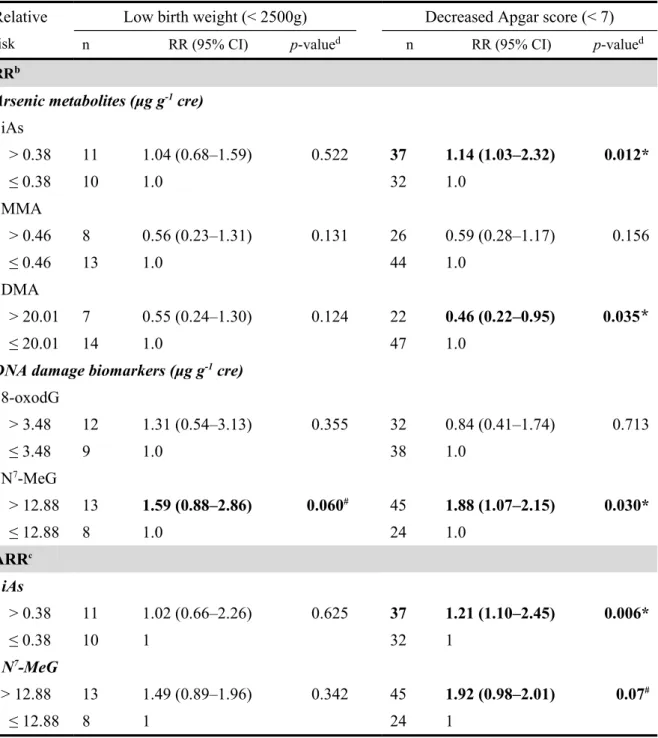
Cox’s proportional hazard model demonstrated that the maternal iAs level over the median was associated with the risk of decreased Apgar scores (RR = 1.14, 95% CI: 1.03 – 2.32, p = 0.012; Table 6). Supplemental Figure S1 showed that the increase in iAs greater than the median of 0.79 µg/g creatinine was associated with 1-min Apgar 287 288 289 290 291 292 293 294 295 296 297 298 299 300 301 302 303 304 305
score decreasing from an average of 9 to 7. The relative risks for decreased Apgar scores was significantly increased (OR = 1.88, 95% CI: 1.07–2.15, p = 0.03) for pregnant women with urinary N7-MeG levels over the median. Relative risks for decreased Apgar scores associated with maternal N7-MeG levels were borderline significant (RR = 1.92, 95% CI: 0.98–2.01, p = 0.07) after adjusting for iAs and other potential confounders. [“Borderline” significance really does not qualify as
significance.]
Discussion
This is the first study to simultaneously assess the effects from maternal arsenic exposure and maternal oxidative and methylated DNA damage on the health status of newborns. The concentrations of urinary tAs in this study were significantly lower than previous studies conducted in Bangladesh (median urinary tAs, 717.5 μg g-1 cre) [26] and Chile (median urinary tAs, 40.4 μg g-1 cre) [27]. Adverse birth outcomes and decreased 1-min Apgar scores were associated with increased maternal levels of iAs and N7-MeG in the general population.
We observed a significantly increased relative risk of low Apgar scores associated with maternal urinary iAs levels after adjusting for N7-MeG. The critical mechanism 306 307 308 309 310 311 312 313 314 315 316 317 318 319 320 321 322 323 324 325
underlying prenatal arsenic exposure is still not clear. Disrupted placentation [13] and endocrine disturbance [14] have been reported for arsenic-related adverse pregnancy outcomes. Animals treated with high doses of arsenic have reported severe early effects, such as neural tube effects [28]; however, the levels of arsenic exposure relevant to humans await further investigation. DNA damage was reported to be induced by iAs, as shown by increased concentrations of the biomarkers of oxidized DNA adducts (8-oxodG) in the brains of mice [29] and in the urine of women in the early stages of pregnancy [17]. In the present study, urinary 8-oxodG andN7-MeG levels were significantly associated with concentrations of maternal urinary arsenic species. N7-MeG was significantly associated with decreased birth length and 1-min Apgar scores after adjustment for maternal age, pre-pregnant BMI, mode of delivery, gestational age, and newborn sex. Thus, N7-MeG appeared to be a more sensitive biomarker than 8-oxodG for maternal DNA damage related to newborn adverse outcomes. This suggests that maternal iAs might cause both DNA damage and adverse newborn health independent of the DNA damage.
We first reported that the association between iAs and N7-MeG. N7-MeG has been established as a marker of human exposure to methylating agents and smoking [30]. The induction of N7-MeG is believed to occur via the direct toxicity of arsenic on 326 327 328 329 330 331 332 333 334 335 336 337 338 339 340 341 342 343 344
enzyme activities, such as DNA repair enzymes. It has been shown that low concentrations of iAs are able to inhibit the expression and activity of poly(ADP-ribose) polymerase (PARP) enzymes [31], the enzymes responsible for base excision repair pathways, which increase unrepaired DNA lesions [32]. Urinary N7-MeG is derived from transfer RNA (tRNA) turnover [33]. The current association between arsenic exposure and increased urinary N7-MeG levels might be due to upregulation of alternative repair pathways of methylated DNA damage, such as base excision repair, resulting in the formation of N7-MeG. A previous report indicated that a variety of methylated purines and pyrimidines are found in tRNA, thus degradation of tRNA might result in the release of all minor methylated bases [34]. A recent in vivo study showed that arsenic exposure induces tRNA modification in Saccharomyces
cerevisiae, and may subsequently increase cellular levels of N7-MeG [35]. An improper alteration in tRNA modification may lead to disorders in embryonic development, cell proliferation, and differentiation in mice [36], and developmental abnormalities in Caenorhabditis elegans [37].
DNA methylation is an important mechanism of fetal programming during fetal development [2,10]. Long-term exposure to arsenic in utero has been associated with changes in DNA methylation, which may have severe consequences for the
345 346 347 348 349 350 351 352 353 354 355 356 357 358 359 360 361 362 363
development of fetal health effects [10]. Urinary N7-MeG could be used as a biomarker for the alteration of DNA methylation due to arsenic [38]. It has been shown that high arsenic exposure in pregnant mice significantly reduces DNA methylation in offspring [39]. We suggest that iAs might induce adverse birth outcomes. Further evaluation is needed in a larger sample to understand whether or not prenatal low iAs exposure results in altering DNA methylation in newborns.
Maternal urinary DMA was not significantly associated with maternal 8-oxodG nor were 1-min Apgar scores. This might result from organic arsenic as a source of DMA and tAs: A large population study showed that seafood intake was a major
determinant of increased urine concentrations of DMA and total arsenic [41]. Current study area residents in Taiwan regularly consume seafood and fish from the
surrounded Pacific Ocean [42]. These foods might contain substantial amounts of arsenosugars or arsenolipids, which could metabolized as DMA [42].
The main strengths of this study include a study design that allows findings on the longitudinal capture of biomarkers for inorganic arsenic exposure to relate to birth outcomes, monitoring biomarkers of oxidative damage, and sufficient sample size. In addition, none of the study subjects smoked cigarettes, which otherwise would have been a major confounder because smoking is associated with several adverse
364 365 366 367 368 369 370 371 372 373 374 375 376 377 378 379 380 381 382 383
outcomes of pregnancy, including LBW [40] and increased N7-MeG levels [30]. The current study was limited by the lack of paternal data, thus early contributions from the male complement due to arsenic-induced damage cannot be evaluated and warrant further studies. Furthermore, iAs has a short half-life and the efficiency of inorganic arsenic methylation to DMA was increasing since the 1st trimester of pregnancy [43]. [Is this rewrite accurate?] We only measured urinary arsenic species once during the third trimester, which likely introduced a substantial degree of exposure measurement misclassification towards null hypothesis.
In this study, there were no significant differences in the association of birth outcomes with maternal iAs between sexes; we combined data from female and male newborns to increase the statistical power. Future work might recruit more subjects to further verify the sex difference. We assessed arsenic and biomarkers of DNA damage using the same spot urine and thus temporality cannot be evaluated. However, we do not think the converse is likely to occur (i.e., greater oxidation/methylation metabolism increases arsenic elimination).
Conclusions
This is the first study to report significant associations between arsenic-induced N7 -384 385 386 387 388 389 390 391 392 393 394 395 396 397 398 399 400 401 402 403
MeG levels of pregnant women and an increased risk of adverse birth outcomes in newborns. These findings strongly emphasize that maternal N7-MeG may be a sensitive and effective biomarker for newborn health, particularly after early-life arsenic exposure. Further studies are necessary to understand the potential health effects of arsenic-related DNA methylation or tRNA modifications in newborns.
Funding
Financial support received from the National Science Council, Taiwan, is gratefully acknowledged (grants no.: NSC98-2314-B-400-001-MY3). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. [Please note that your target journal requests that the funding information not be provided in the manuscript itself, but in the forms submitted with the
manuscript.]
Acknowledgments
We are greatly indebted to the clinics of the Department of Pediatrics and Department of Obstetrics and Gynecology, Chung-Shan Medical University Hospital, especially for the assistance of Dr. Jia-Yuh Chen, Dr. Long-Yau Lin, Dr. Pen-Hua Su, and Dr. Chin-Yi Lin. We appreciate the earlier participation of Mr. Yun-Siang Liu and Dr. 404 405 406 407 408 409 410 411 412 413 414 415 416 417 418 419 420 421 422 423
Po-Chin Huang at the National Health Research Institutes, Miaoli, Taiwan, including subject recruitment and specimen processing.
424 425
References
1. Doctor BA, O’Riordan MA, Kirchner HL, Shah D, Hack M (2001) Perinatal correlates and neonatal outcomes of small for gestational age infants born at term gestation. Am J Obstet Gynecol 185: 652–659.
2. Valdez R, Athens MA, Thompson GH, Bradshaw BS, Stern MP (1994) Birth weight and adult health outcomes in a biethnic population in the USA. Diabetologia 37: 624–631.
3. Kajantie E, Osmond C, Barker DJP, Forsén T, Phillips DIW, et al. (2005) Size at birth as a predictor of mortality in adulthood: a follow-up of 350 000 person-years. Int J Epidemiol 34: 655–663.
4. Casey BM, McIntire DD, Leveno KJ (2001) The continuing value of the Apgar score for the assessment of newborn infants. New Engl J Med 344: 467–471. 5. Saenger P, Czernichow P, Hughes I, Reiter EO (2007) Small for gestational age:
short stature and beyond. Endocr Rev 28: 219–251.
6. Odd DE, Rasmussen F, Gunnell D, Lewis G, Whitelaw A (2007) A cohort study of low Apgar scores and cognitive outcomes. Arch Dis Child Fetal Neonatal Ed 93: F115–F120.
7. Concha G, Vogler G, Lezcano D, Nermell B, Vahter M (1998) Exposure to inorganic arsenic metabolites during early human development. Toxicol Sci 44: 185–190. 426 427 428 429 430 431 432 433 434 435 436 437 438 439 440 441 442 443 444 445
8. Rahman A, Vahter M, Smith AH, Nermell B, Yunus M, et al. (2009) Arsenic exposure during pregnancy and size at birth: a prospective cohort study in Bangladesh. Am J Epidemiol 169: 304–312.
9. Huyck KL, Kile ML, Mahiuddin G, Quamruzzaman Q, Rahman M, et al. (2007) Maternal arsenic exposure associated with low birth weight in Bangladesh. J Occup Environ Med 49: 1097–1104.
10. Yang CY, Chuang HY, Ho CK, Wu TN, Wu MTF (2003) Arsenic in drinking water and adverse pregnancy outcome in an arseniasis-endemic area in
Northeastern Taiwan. Epidemiology 14: S127–S127.
11. Myers SL, Lobdell DT, Liu Z, Xia Y, Ren H, et al. (2010) Maternal drinking water arsenic exposure and perinatal outcomes in inner Mongolia, China. J Epidemiol Community Health 64: 325–329.
12. Vahter M (2009) Effects of arsenic on maternal and fetal health. Annu Rev Nutr 29: 381–399.
13. He WJ, Greenwell RJ, Brooks DM, Calderon-Garciduenas L, Beall HD, et al. (2007) Arsenic exposure in pregnant mice disrupts placental vasculogenesis and causes spontaneous abortion. Toxicol Sci 99: 244–253.
14. Davey JC, Nomikos AP, Wungjiranirun M, Sherman JR, Ingram L, et al. (2008) Arsenic as an endocrine disruptor: Arsenic disrupts retinoic acid receptor- and thyroid hormone receptor-mediated gene regulation and thyroid hormone-446 447 448 449 450 451 452 453 454 455 456 457 458 459 460 461 462 463 464 465
mediated amphibian tail metamorphosis. Environ Health Perspect 116: 165– 172.
15. Vijayaraghavan M, Wanibuchi H, Karim R, Yamamoto S, Masuda C, et al. (2001) Dimethylarsinic acid induces 8-hydroxy-2′-deoxyguanosine formation in the kidney of NCI-Black-Reiter rats. Cancer Lett 165: 11–17.
16. Yamanaka K, Mizol M, Kato K, Hasegawa A, Nakano M, et al. (2001) Oral administration of dimethylarsinic acid, a main metabolite of inorganic arsenic, in mice promotes skin tumorigenesis initiated by dimethylbenz(a)anthracene with or without ultraviolet B as a promoter. Biol Pharm Bull 24: 510–514. 17. Engstrom KS, Vahter M, Johansson G, Lindh CH, Teichert F, et al. (2010)
Chronic exposure to cadmium and arsenic strongly influences concentrations of 8-oxo-7,8-dihydro-2′-deoxyguanosine in urine. Free Radic Biol Med 48: 1211-1217.
18. Ahmed S, Mahabbat-e Khoda S, Rekha RS, Gardner RM, Ameer SS, et al. (2011) Arsenic-associated oxidative stress, inflammation, and immune disruption in human placenta and cord blood. Environ Health Perspect 119: 258–264.
19. Chiang SY, Huang TH, Uang SN, Wu HDI, Wei YC, et al. (2005) Analysis of 7-methylguanine using isotope dilution and gas chromatography/electron-capture negative chemical ionization mass spectrometry. Rapid Commun Mass 466 467 468 469 470 471 472 473 474 475 476 477 478 479 480 481 482 483 484 485
Spectrom 19: 1915–1920.
20. Rydberg B, Lindahl T (1982) Nonenzymatic methylation of DNA by the intracellular methyl group donor S-adenosyl-L-methionine is a potentially mutagenic reaction. EMBO J 1: 211–216.
21. Wang SL, Lin CY, Guo YLL, Lin LY, Chou WL, et al. (2004) Infant exposure to polychlorinated dibenzo-p-dioxins, dibenzofurans and biphenyls (PCDD/Fs, PCBs)—correlation between prenatal and postnatal exposure. Chemosphere 54: 1459–1473.
22. Chou WC, Chuang CY, Huang PC, Wang CJ, Chen HY, Chuang YD, et al. (2012) Arsenic exposure in pregnancy increases the risk of adverse birth outcomes of newborn in Taiwan. In: Ng JC, Noller BN, Naidu R, Bundschuh J, editors. Proceedings of the 4th International Congress: Arsenic in the
Environment, 2012. Cairns, Australia. pp. 157–158.
23. Ritsema R, Dukan L, Navarro TRI, van Leeuwen W, Oliveira N, et al. (1998) Speciation of arsenic compounds in urine by LC-ICP MS. Appl Organometal Chem 12: 591–599.
24. Chao MR, Wang CJ, Wu MT, Pan CH, Kuo CY, et al. (2008) Repeated
measurements of urinary methylated/oxidative DNA lesions, acute toxicity, and mutagenicity in coke oven workers. Cancer Epidemiol Biomarkers Prev 17: 3381–3389. 486 487 488 489 490 491 492 493 494 495 496 497 498 499 500 501 502 503 504 505
25. Baskett TF (2000) Virginia Apgar and the newborn Apgar score. Resuscitation 47: 215–217.
26. Hall M, Gamble M, Slavkovich V, Liu X, Levy D, et al. (2007) Determinants of arsenic metabolism: blood arsenic metabolites, plasma folate, cobalamin, and homocysteine concentrations in maternal-newborn pairs. Environ Health Perspect 115: 1503–1509.
27. Christian WJ, Hopenhayn C, Centeno JA, Todorov T (2006) Distribution of urinary selenium and arsenic among pregnant women exposed to arsenic in drinking water. Environ Res 100: 115–122.
28. Hill DS, Wlodarczyk BJ, Finnell RH (2008) Reproductive consequences of oral arsenate exposure during pregnancy in a mouse model. Birth Defects Res B Dev Reprod Toxicol 83: 40–47.
29. Piao F, Ma N, Hiraku Y, Murata M, Oikawa S, et al. (2005) Oxidative DNA damage in relation to neurotoxicity in the brain of mice exposed to arsenic at environmentally relevant levels. J Occup Health 47: 445–449.
30. Lin IH, Chao MR, Hu CW, Ho ML, Huang JY, et al. (2009) Modification of urinary N7-methylguanine excretion in smokers by glutathione-S-transferase M1 polymorphism. Toxicology 260: 1–6.
31. Walter I, Schwerdtle T, Thuy C, Parsons JL, Dianov GL, et al. (2007) Impact of arsenite and its methylated metabolites on PARP-1 activity, PARP-1 gene 506 507 508 509 510 511 512 513 514 515 516 517 518 519 520 521 522 523 524 525
expression and poly(ADP-ribosyl)ation in cultured human cells. DNA Repair (Amst) 6: 61–70.
32. Qin XJ, Liu W, Li YN, Sun X, Hai CX, et al. (2012) Poly(ADP-ribose) polymerase-1 inhibition by arsenite promotes the survival of cells with unrepaired DNA lesions induced by UV Exposure. Toxicol Sci 127: 120–129. 33. Shuker DEG, Farmer PB (1992) Relevance of urinary DNA adducts as markers
of carcinogen exposure. Chem Res Toxicol 5: 450–460.
34. Mandel LR, Srinivasan PR, Borek E (1966) Origin of urinary methylated purines. Nature 209: 586–588.
35. Chan CTY, Dyavaiah M, DeMott MS, Taghizadeh K, Dedon PC, et al. (2010) A quantitative systems approach reveals dynamic control of tRNA modifications during cellular stress. PLoS Genet 6: e1001247.
36. Tuorto F, Liebers R, Musch T, Schaefer M, Hofmann S, et al. (2012) RNA cytosine methylation by Dnmt2 and NSun2 promotes tRNA stability and protein synthesis. Nat Struct Mol Biol 19: 900–905.
37. Chen CC, Tuck S, Bystrom AS (2009) Defects in tRNA modification associated with neurological and developmental dysfunctions in Caenorhabditis elegans elongator mutants. PLoS Genet 5: e1000561.
38. Stillwell WG, Xu HX, Adkins JA, Wishnok JS, Tannenbaum SR (1989) Analysis of methylated and oxidized purines in urine by capillary gas-526 527 528 529 530 531 532 533 534 535 536 537 538 539 540 541 542 543 544 545
chromatography mass-spectrometry. Chem Res Toxicol 2: 94–99. 39. Xie YX, Liu J, Benbrahim-Tallaa L, Ward JM, Logsdon D, et al. (2007)
Aberrant DNA methylation and gene expression in livers of newborn mice transplacentally exposed to a hepatocarcinogenic dose of inorganic arsenic. Toxicology 236: 7–15.
40. Bjerg A, Hedman L, Perzanowski M, Lundbäck B, Rönmark E (2011) A strong synergism of low birth weight and prenatal smoking on asthma in
schoolchildren. Pediatrics 127: E905–E912.
41. Navas-Acien A, Francesconi KA, Silbergeld EK, Guallar E (2011) Seafood intake and urine concentrations of total arsenic, dimethylarsinate and arsenobetaine in the US population. Environ Res 111: 110–8.
42. Lee MM, Pan WH, Yu SL, Huang PC. (1992) Foods predictive of nutrient intake in Chinese diet in Taiwan: I. Total calories, protein, fat and fatty acids. Int J Epidemiol 21: 922–928.
43. Gardner RM, Nermell B, Kippler M, Grandér M, Li L, Ekström EC, et al. (2011) Arsenic methylation efficiency increases during the first trimester of pregnancy independent of folate status. Reprod Toxicol 31: 210–218. 546 547 548 549 550 551 552 553 554 555 556 557 558 559 560 561 562
Table 1. Characteristics of mothers and their newborns by newborn sex in central Taiwan during 2000–2001 (n=299)
Characteristics All (n=299)a Male (n=151)a Female
(n=148)a p-valueb Pregnant women Age (years) 28.3 ± 4.2 28.1 ± 4.0 28.0 ± 4.8 0.772 BMI (Kg/m2) 25.6 ± 3.9 25.6 ± 4.4 25.1 ± 4.0 0.832 Urinary creatinine (mg/dL) 78.2 ± 48.5 74.9 ± 52.3 80.7 ± 46.6 0.732 Parity 0.693 Primiparous 159 (53) 90 (59) 69 (47) Multiparous 140 (47) 61 (41) 79 (53) Maternal Education 0.482 ≤ high school 132 (44) 61 (41) 71 (48)
high school + 2years 117 (39) 60 (40) 57 (39)
≥ high school + 3 years 50 (17) 30 (19) 20 (13)
Alcohol consumption 0.783
Yes 5 (1) 2 (1) 3 (1)
No 294 (99) 149 (99) 145 (99)
Newborns
Gestational age (weeks) 39 ± 2.8 39 ± 1.5 39 ± 1.8 0.290
Birth length (cm) 51 ± 2.6 51.5 ± 2.3 50.7 ± 2.7 0.005 Head circumference (cm) 34.5 ± 18.5 35.6 ± 25.1 33.2 ± 1.5 0.261 Chest girth (cm) 32.7 ± 1.8 32.9 ± 1.8 32.5 ± 1.8 0.120 Mode of delivery Normal spontaneous 98 (33) 45 (30) 44 (30) 0.534 Vacuum extraction 103 (34) 55 (36) 58 (39) 0.356 Cesarean section 98 (33) 51 (34) 46 (31) 0.289 Birth weight (g) 3085 ± 466 3170 ± 425 2985 ± 493 0.001 < 2,500 21 (7) 8 (5) 13 (9) 0.019 ≥ 2,500 278 (93) 143 (95) 135 (91)
One-minute Apgar score 8.3 ± 1.0 8.2 ± 0.91 8.3 ± 1.15 0.664
< 7 69 (23) 40 (26) 29 (20 ) 0.153
≥ 7 230 (77) 111 (74) 119 (80)
Five-minute Apgar score 9.8 ± 0.8 9.6 ± 0.5 9.7 ± 1.1 0.546
< 7 4 (1) 0 (0) 4 (3) 0.001
≥ 7 295 (99) 151 (100) 144 (97)
aPresented as the mean ± SD or number (percentage)
bp-value for difference between male and female newborns using t-test for continuous
variables and χ2 or Fisher’s exact test for categorical variables. The p-value was bolded when < 0.1. 563 564 565 566 567 568 569
Table 2. Distribution of creatinine-adjusted concentrations of urinary arsenic species (iAs, MMA, and DMA) and urinary DNA damage biomarkers (8-oxodG and N7-MeG) for pregnant women in the present study versus two others with established arsenic-related effects (n=299)
< LOD Percentileb
Exposure variablesa (n) Min 5th 25th 50th 75th 95th Max
As metabolites (μg g cre-1) As3+ 14 0.0 2 0.06 0.16 0.30 0.66 1.77 12.17 As5+ 20 0.0 2 0.05 0.11 0.21 0.49 2.95 16.52 MMA 10 0.0 5 0.07 0.18 0.46 2.03 5.82 43.89 DMA 12 0.1 2 1.43 7.48 20.01 32.30 69.94 131.5 iAs (ΣAs3+, As5+) - 0.0 5 0.18 0.38 0.79 1.49 3.96 18.00 tAs (ΣiAs, MMA and DMA) - 0.2
1
2.80 8.21 22.26 36.72 83.00 137.5 DNA damage biomarkers
8-oxodG (μg g cre-1) 0 0.2 4 1.59 2.67 3.48 4.84 8.56 16.94 N7-MeG (mg g cre-1) 0 0.2 1 6.47 10.28 12.88 19.50 27.57 76.49
aAbbreviations: iAs represents the sum of As3+ and As5+; MMA: methylarsonic acid; DMA: dimethylarsinic acid; AsB: arsenobetaine; tAs: the sum of iAs, MMA, and DMA; 8-oxodG: 8-oxo-7,8-dihydro-2′-deoxyguanosine; N7-MeG: N7-methylguanine.
bThis study. Taiwanese pregnant women in third trimester (n=299). cBangladesh pregnant women in first trimester (n=101) [21]. dChilean pregnant women in first trimester (n=93) [22]. 570 571 572 573 574 575 576 577 578 579 580
Table 3. Pearson correlations between maternal inorganic arsenic and its metabolites levels, DNA damage in pregnant women, newborn health status, and other factors
aAll urinary arsenic species in pregnant women were adjusted by creatinine and log-transformed.
bPearson correlation coefficient; #p < 0.10; *p < 0.05; **p < 0.01.The p-value was bolded when < 0.1.
cUrinary 8-oxodG and N7-MeG in pregnant women were both adjusted by creatinine and natural log-transformed. Health parameter Maternal urinary As species (μg g cre-1)a Maternal urinaryDNA damages(μg g cre -1)c
iAsb MMAb DMAb tAsb 8-oxodG N7-MeG
Maternal urinary DNA damagec
8-OHdG 0.24** 0.16** 0.13* 0.17** 1.00
N7-MeG 0.35** 0.19** 0.23** 027** 0.62** 1.00
Pregnant women
Maternal age (years) 0.06 0.07 0.13# 0.12# 0.16* 0.04 Pre-pregnant BMI
(Kg/m2) 0.05 -0.02 0.12# 0.15* -0.05 -0.01
Maternal education -0.03 -0.09 -0.05 -0.09 -0.06 -0.06
Newborns
Sex 0.04 -0.08 0.04 0.06 -0.05 -0.04
Gestational age (weeks) -0.04 0.06 0.07 0.06 0.07 -0.02 Mode of delivery 0.08 -0.07 -0.06 -0.05 -0.08 -0.12
Birth weight (g) 0.03 0.13 0.09 0.12 0.04 0.09
Birth length (cm) -0.03 0.09 0.03 0.05 -0.001 -0.01 Head circumference (cm) 0.09 0.01 0.02 0.05 0.02 -0.08
Chest girth (cm) 0.04 0.10 0.05 0.07 0.04 0.11
One-minute Apgar score -0.13# 0.15* 0.11 0.10 0.06 -0.18# Five-minute Apgar score -0.01 0.07 0.10 0.09 0.01 0.06 581 582 583 584 585 586 587 588 589
Health
parameter As species (μg g creMaternal urinary-1) DNA damage (μg g creMaternal urinary -1)
iAsb MMAb DMAb tAsb 8-oxodGc N7-MeGc
Pregnant women 8-oxodGc ß 0.24 0.16 0.08 0.13 - 0.64 95% CI 0.16–0.43 0.05–0.26 -0.02–0.17 0.01–0.25 - 0.56–0.74 p-value < 0.001 0.03 0.123 0.028 - < 0.001 N7-MeGc ß 0.35 0.17 0.19 0.27 0.62 -95% CI 0.28–0.55 0.07–0.27 0.09–0.28 0.15–0.39 0.53–0.71 -p-value < 0.001 0.001 < 0.001 < 0.001 < 0.001 -Newborns Birth weight (g) ß 0.01 0.25 0.10 0.17 0.05 -0.16 95% CI -0.28–0.34 0.02–0.42 -0.13–0.33 -0.12–0.45 -0.25–0.34 -0.35–0.35 p-value 0.845 0.034 0.396 0.312 0.745 0.062 Birth length (cm) ß -0.19 0.398 0.06 0.18 0.04 -0.21 95% CI -0.99–0.62 -0.15–0.95 -0.54–0.65 -0.54–0.90 -0.25–0.31 -0.86 – -0.13 p-value 0.648 0.157 0.854 0.626 0.886 0.024 Head circumference (cm) ß 0.29 0.01 -0.07 -0.05 -0.09 -0.02 95% CI -0.22–0.81 -0.35–0.35 -0.45–0.32 -0.47–0.46 -0.59–0.39 -0.81–0.76 p-value 0.259 0.970 0.750 0.985 0.696 0.053 Chest girth (cm) ß 0.11 0.28 0.14 0.12 0.24 0.46 95% CI -0.46–0.68 -1.22–0.69 -0.37–0.49 -0.41–0.64 -0.29–0.78 -0.11–1.02 p-value 0.699 0.169 0.798 0.655 0.376 0.116
One-minute Apgar score
ß -0.23 0.21 0.19 0.24 0.13 -0.25
95% CI -0.29 – -0.18 -0.01–0.44 -0.04–0.43 -0.05–0.52 -0.16–0.43 -0.63 – -0.15
p-value 0.041 0.060 0.104 0.102 0.390 0.042
Five-minute Apgar score
ß 0.02 0.09 0.14 0.15 0.04 -0.09
95% CI -0.19–0.24 -0.07–0.24 -0.02–0.30 -0.04–0.34 -0.16–0.25 -0.15–0.29
p-value 0.861 0.269 0.083 0.125 0.692 0.413
Table 4. Multiple linear regression (ß-coefficient) for the associationa between birth outcomes with maternal urinary arsenic metabolitesb and DNA damagec biomarkers (n=299)
aMultiple linear regression model was adjusted for maternal age, pre-pregnant BMI, mode of delivery, gestational age, and newborn sex; ß, regression coefficient; 95% CI, 95%
confidence interval. The p-value was bolded when < 0.1.
bAll maternal urinary As species were adjusted by creatinine and log-transformed.
cUrinary 8-oxodG and N7-MeG in pregnant women were both adjusted by creatinine and 590 591 592 593 594 595 596
natural log-transformed. 597
Table 5. Multiple linear associations (ß-coefficient) of birth outcomes with maternal urinary inorganic concentrations and DNA damage biomarkers after further mutual adjustment for each other.
Birth outcomes Urinary iAs and DNA damage biomarkers (μg g cre-1)
iAsa N7-MeGb Birth weight (g) ß -0.07 -0.06 95% CI -0.40–0.27 -0.07–0.56 p-value 0.493 0.079 Birth length (cm) ß -0.27 -0.11 95% CI -1.11–0.58 -0.42 – -0.07 p-value 0.530 0.052 Head circumference (cm) ß 0.21 -0.03 95% CI -0.35–0.77 -0.02–0.04 p-value 0.459 0.065 Chest girth (cm) ß -0.11 0.29 95% CI -0.72–0.50 -0.05–0.63 p-value 0.726 0.082
One-minute Apgar score
ß -0.28 -0.05
95% CI -0.38 – -0.15 -0.38–0.04
p-value 0.036 0.058
Five-minute Apgar score
ß 0.02 -0.05
95% CI -0.23–0.23 -0.16–0.09
p-value 0.909 0.482
aMultiple linear regression model was adjusted for maternal age, pre-pregnant BMI, mode of delivery, gestational age, and newborn sex, and further adjusted for N7-MeG. The p-value was bolded when < 0.1.
bMultiple linear regression model was adjusted for maternal age, pre-pregnant BMI, gestational age, and newborn sex, and further adjusted for iAs.
598 599 600 601 602 603 604 605
Table 6. Relative risks (RR)a and 95% confidence interval (95% CI) for low birth weight and decreased one-minute Apgar score in relation to maternal urinary arsenic and DNA
damage biomarker levels (n=299) Relative
risk
Low birth weight (< 2500g) Decreased Apgar score (< 7)
n RR (95% CI) p-valued n RR (95% CI) p-valued
RRb
Arsenic metabolites (μg g-1 cre)
iAs > 0.38 11 1.04 (0.68–1.59) 0.522 37 1.14 (1.03–2.32) 0.012* ≤ 0.38 10 1.0 32 1.0 MMA > 0.46 8 0.56 (0.23–1.31) 0.131 26 0.59 (0.28–1.17) 0.156 ≤ 0.46 13 1.0 44 1.0 DMA > 20.01 7 0.55 (0.24–1.30) 0.124 22 0.46 (0.22–0.95) 0.035* ≤ 20.01 14 1.0 47 1.0
DNA damage biomarkers (μg g-1 cre)
8-oxodG > 3.48 12 1.31 (0.54–3.13) 0.355 32 0.84 (0.41–1.74) 0.713 ≤ 3.48 9 1.0 38 1.0 N7-MeG > 12.88 13 1.59 (0.88–2.86) 0.060# 45 1.88 (1.07–2.15) 0.030* ≤ 12.88 8 1.0 24 1.0 ARRc iAs > 0.38 11 1.02 (0.66–2.26) 0.625 37 1.21 (1.10–2.45) 0.006* ≤ 0.38 10 1 32 1 N7-MeG > 12.88 13 1.49 (0.89–1.96) 0.342 45 1.92 (0.98–2.01) 0.07# ≤ 12.88 8 1 24 1
aThe continuous variables were transformed into a two-level scale using medians, which represented the high or low levels arsenic/DNA damage biomarkers exposure, to calculate relative risks (RR).
bAdjusted for potential confounders (maternal age, mode of delivery, pre-pregnant BMI, 606 607 608 609 610 611 612
gestational age, and newborn sex).
cAdjusted for iAs or N7-MeG and potential confounders.
dCox’s proportional hazards model: #p < 0.10; *p < 0.05 for RR significance above 1. p-value was bolded when less than 0.1.
613 614 615 616
Figure 1. Subject recruitment and follow-up scheme for final analyses. [Please note that your target journal suggests both a figure title of less than 15 words as well as a figure legend describing the key message of the figure.]
Supplemental Figure S1. The newborn one-minute Apgar scores in relation to maternal urinary inorganic concentration. Upper panel: By log-transformed iAs concentrations; Lower panel: By the median level.
617 618 619 620 621 622 623